Full Length Research Paper

ABSTRACT
The integrated approach is the new recommendation of the World Health Organization (WHO) for the control of neglected tropical diseases. The goal of this cross-sectional study was to implement this approach in 4 municipalities with a high prevalence of leprosy in Benin from September 2019 to August 2020. Mobile medical consultations were organized in these municipalities following the mobilization and sensitization of the populations. In the 4 municipalities, 6416 people were examined. The mean age was (27.3 ±19.8) years. Women represented 52.7% of people examined. Among the 6416 people examined, 1230 (19.2%) had skin conditions. The most common skin conditions were pityriasis versicolor (421 cases; 34.2%); eczema (203 cases; 16.5%); ringworm (159 cases; 12.9%); pruritus sine materia (81 cases; 6.6%); acne (62 cases; 5.0%); epidermophytia (37 cases; 3.0%); achromic nevus (35 cases; 2.8%); keloids (28 cases; 2.3%); chronic ulcers (27 cases; 2.2%) and depigmentation stigmata (24 cases; 2.0%). 8 new leprosy cases (0.7%) were detected. This study proves the efficiency of the integrated approach in the control of neglected tropical diseases (NTDs) with cutaneous manifestations in Benin.
Key words: Neglected tropical disease, leprosy, skin disease, integration, disease control, Benin.
INTRODUCTION
The skin is the most visible structural element both for patients and caregivers who examine them. Any skin condition is noticeable and will have an effect on the personal and social well-being of the patient. The skin is therefore an important point of intervention for both diagnostic and therapeutic procedures (OMS, 2018a).
Many neglected tropical diseases (NTDs) affect the skin, causing considerable disability, stigma and exacerbation of poverty (Engelman et al., 2016). NTDs cause changes in the skin, with symptoms ranging from pruritus to changes in colour, feeling or appearance (OMS, 2018a). In addition, NTDs with cutaneous manifestations are co-endemic in many countries, districts and communities (Amazigo, 2008; Alvar et al., 2012; van de Sande, 2013; Mitjà et al., 2014; WHO, 2014; Mitjà et al., 2015; Yotsu et al., 2015; WHO, 2016). These cutaneous NTDs are responsible for the loss of a large number of disability-adjusted life years (DALY) (WHO, 2010).
Integrating efforts to control cutaneous NTDs can facilitate progress in understanding and controlling this diverse group of diseases (Engelman et al., 2016). Indeed, examination of the skin offers the opportunity to screen individuals in communities or children in schools to identify multiple conditions in a single visit. This common approach for controlling these skin diseases justifies the integrated delivery of health care interventions to both increase cost-effectiveness and expand coverage (Mitjà et al., 2017).
In Benin, two programmes have been involved in the control of NTDs. The National Program for the Control of Neglected Tropical Diseases (PNLMTN) is engaged in the treatment of NTDs in general, whereas the National Program for the Control of Leprosy and Buruli Ulcers (PNLLUB) addresses only cutaneous NTDs including Buruli ulcers, leprosy and yaws. Despite the efforts of these programmes, NTDs in general and those with cutaneous manifestations in particular persist. Many challenges remain for these programmes, especially PNLLUB, in achieving the control of Buruli ulcers and yaws, the elimination of leprosy and the management and/or intensive care of the other cutaneous NTDs. The purpose of this study was to implement integrated approach for the control of NTDs with cutaneous manifestations in the municipalities of Djidja, Ouinhi, Zagnanado and Kétou in Benin.
MATERIALS AND METHODS
Study framework
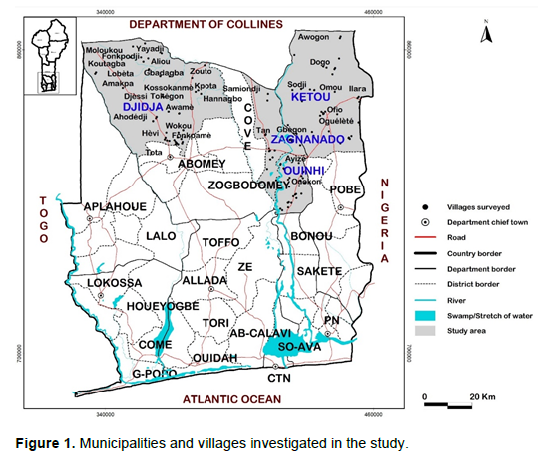
The study was conducted in 96 villages of the municipalities of Djidja, Ouinhi, Zagnanado (in the department of Zou) and Kétou (in the department of Plateau) in Benin (Figure 1). These municipalities were selected according to the endemicity of leprosy (PNLLUB, 2019). The estimated populations of these municipalities were respectively 146,681, 70,507, 65,377 and 186,834 inhabitants for Djidja, Ouinhi, Zagnanado and Kétou (INSAE, 2016).
Study design and population
This is a cross-sectional study carried out from September 2019 to August 2020. It was conducted on the populations of the municipalities of Djidja, Ouinhi, Zagnanado and Kétou.
Participants
A non-probabilistic method in conjunction with a convenience-based choice technique was used in this study. Thus, any person who was at least 1 year old, available and who gave consent after being informed, was included in the study. For participants under 18 years old, the consent of parents or guardians has been requested.
Data collection
Social mobilization was carried out in the 96 villages by community health volunteers, local elected officials and town criers. Information sessions on skin diseases, especially leprosy, were organized for the participants. Thus, the purpose and benefits of the study were presented each time at the start of consultations in the villages where the study was conducted. The consultations were done in public places, sometimes in schools, in rooms well-lit by daylight while respecting the patients’ privacy. Two teams were formed, each composed a leprosy specialist/dermatologist, a local health worker and a data collection agent. When a person, after being informed of the objectives of the study, agrees to participate, he/she is examined by a leprosy specialist/dermatologist. This latter looked for the cardinal signs of leprosy and for symptoms of Buruli ulcers (BU) and yaws on the participant's body. In addition, the leprosy specialist/dermatologist looked for signs of other dermatoses (OMS, 2018b). The leprosy specialists/dermatologists were helped by local health workers and data collectors who were responsible for providing out dermatological drugs and filling out data collection forms. Thus, the sociodemographic information and data on the characteristics of the skin conditions were collected. Leprosy screening was carried out by leprosy specialists/dermatologists according to the WHO clinical criteria. The leprosy patients were clinically diagnosed according to the WHO clinical definitions. The patients were classified as paucibacillary (≤ 5 lesions) or multibacillary (> 5 lesions or with nerve enlargement) according to the WHO classification (Géniaux, 2010; OMS, 2016). All leprosy new cases detected were systematically placed on multidrug therapy (MDT). After receiving the first supervised dose of MDT, these patients were referred to the municipality’s Leprosy Nursing Supervisor and the most accessible responsible health worker. These patients benefited the disability prevention counselling sessions too. Some were given shea butter for the care of scars and the prevention of dry skin. The contacts of new leprosy cases were systematically examined too. In addition, the non-leprosy patients were carefully assessed by the leprosy specialists/ dermatologists to determine the type of dermatosis and the appropriate treatment. An appropriate treatment was given to each type of dermatosis diagnosed. The necessary inputs for bandages and dressings were also made available to patients with chronic ulcers. These patients were then referred to the nearest BU treatment centres.
Variables
The variable of interest was the skin condition diagnosed through the presence of clinical signs. The sociodemographic informations such as age and gender were recorded for each person examined.
Data processing and statistical analysis
The data collected in the field were recorded using Microsoft Excel 2016 and analysed with IBM SPSS 25. Proportions were calculated for the different skin conditions detected and for the other qualitative variable (gender). The mean and standard deviation were determined for the quantitative variable (age).
Ethical aspects
This study was authorized by the National Ethics Committee for Health Research (CNERS) of the Ministry of Health Benin (ethical authorization N°21/MS/DC/SGM/DRFMT/CNERS/SA). Informed consent was obtained from each participant before any data collection.
RESULTS
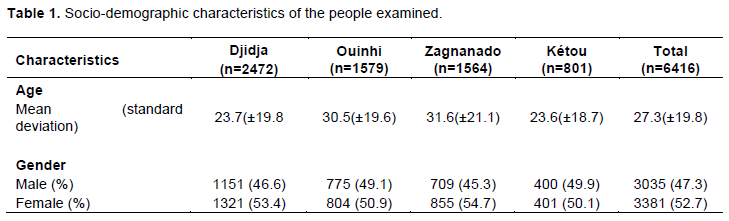
The study mobilized 9,941 people. A total of 6416 (64.5%) had given their consent to be examined. The mean age was (27.3 ±19.8) years and the women represented 52.7% (Table 1). The reasons that 3,525 people did not participate in the study included lack of consent, refusal to be examined and to wait.
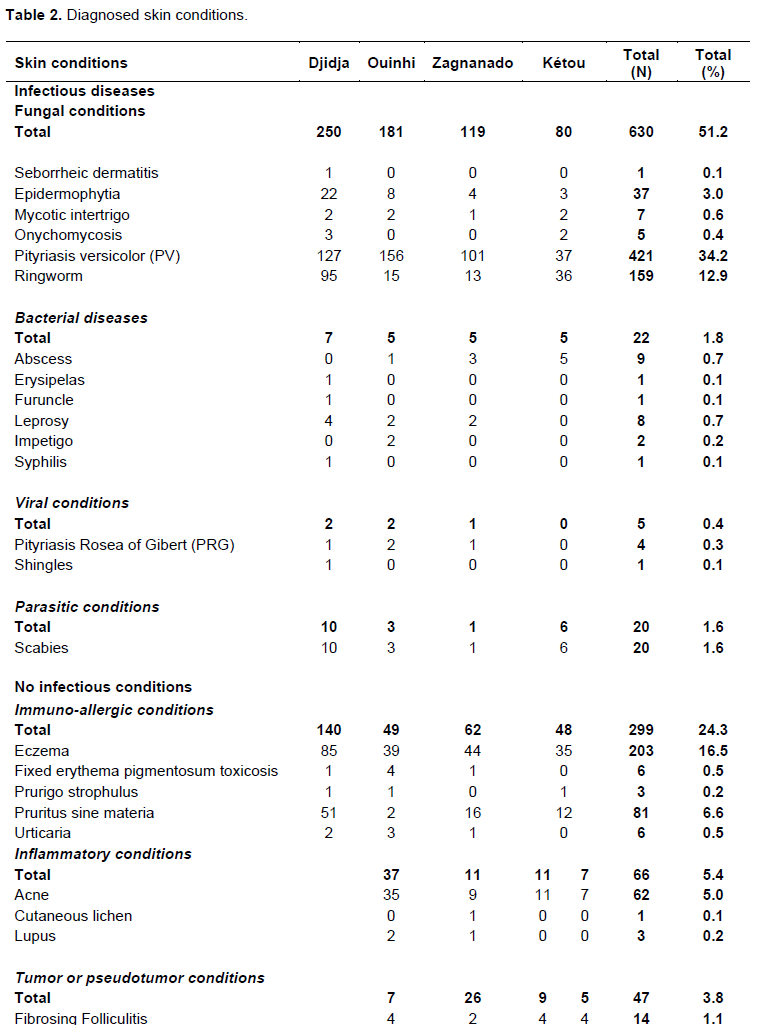
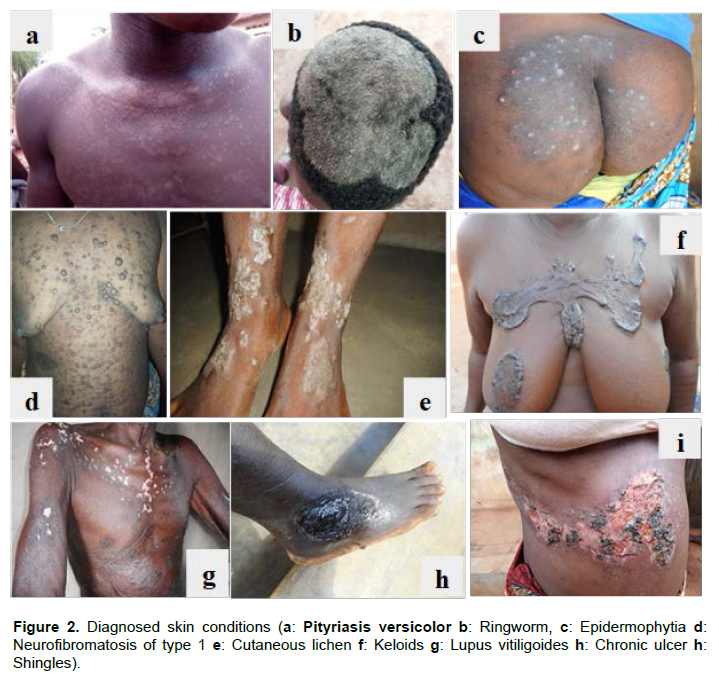
Of the 6416 participants examined, 1230 (19.2%) had at least one skin condition (502 people in Djidja, 322 in Ouinhi, 241 in Zagnanado and 165 in Kétou). The most common skin conditions were pityriasis versicolor (421 cases; 34.2%); eczema (203 cases; 16.5%); ringworm (159 cases; 12.9%); pruritus sine materia (81 cases; 6.6%); acne (62 cases; 5.0%); epidermophytia (37 cases; 3.0%); achromic nevus (35 cases; 2.8%); keloids (28 cases; 2.3%); chronic ulcers (27 cases; 2.2%) and depigmentation stigmata (24 cases; 2.0%) (Table 2). Some of these conditions are presented in Figure 2a to i.

Among the 6416 persons examined, 8 new leprosy cases were detected. Of these patients, 4 were from the municipality of Djidja, 2 were from the municipality of Ouinhi and 2 were from the municipality of Zagnanado. Of these cases, 4 were multibacillary, 4 were paucibacillary and none of them had any disability. One was a paediatric paucibacillary case (14 years old). These cases systematically received the first supervised dose of multidrug therapy (MDT) and were referred to the most accessible municipality’s Leprosy Nursing Supervisor and the responsible health worker.
DISCUSSION
Using integrated approach of screening for skin diseases, this study confirmed the endemicity of leprosy in the municipalities of Djidja, Ouinhi, Zagnanado and Kétou in Benin and helped to detect and treat many other skin diseases. The mean age of the participants was (27.3 ± 19.8) years with a predominance of women. These results reflected the situation at the national level where women predominate in the Beninese population (INSAE, 2016). These findings corroborate the results of one study that showed that women and children are the most vulnerable and most affected by neglected tropical diseases (Hotez et al., 2007). Our results were also consistent with those of a study conducted on sex and age adjusted prevalence estimates of five chronic inflammatory skin diseases in France where it was found a strong representation of the female gender (Richard et al., 2018). A similarity was observed in a study carried out on the prevalence of skin diseases in an outpatient dermatology clinic in Turkey (Bilgili et al., 2013). On the other hand, our results were inconsistent with those obtained in a study of 3673 patients attending a medical camp in Kumble, India, which revealed a predominance of the male sex (Rao and Kumar, 2003). This difference in results may be related to the target population, sample size, and screening technique. Our study focused on mobile consultations whereas this study involved consultations in a hospital. This could mean that the mobile strategy improves accessibility for women and reduces gender-based inequities.
Our results showed that among the participants, 19.2% had skin conditions. This prevalence is higher than the one reported in one study conducted in an Indian village, which reported a prevalence of 11.16% (Rao and Kumar 2003). This result was also higher than the one obtained in Côte d'Ivoire, which reported a prevalence of 15.0% (Koffi et al., 2020). On the other hand, this proportion was much lower than the 64.5% reported in a study conducted in Munich (Tizek et al., 2019). Our prevalence is also lower than the one obtained in a community-based clinical skin examination of 400 subjects in 4 villages in Cameroon and one other obtained in literature review study where the overall prevalence of school children with skin disease was 34.6 and 42.0% in two Ghanaian studies, 45.8% in Gabon and 26.7% in Rwanda (Bissek et al., 2012; Hogewoning et al., 2013). The difference in results could be explained by the diversity of targets, sample size and screening technique.
In the present study, the most common skin conditions were pityriasis versicolor (34.2%); eczema, ringworm, pruritus sine materia, acne, epidermophytia, achromic nevus, keloids, chronic ulcers and depigmentation stigmata. All skin conditions cases received appropriate treatment using dermatological drugs. These results are similar to those reported at Nepal, Yucatan (Mexico) and Laos (Walker et al., 2008; Paek et al., 2012; Wootton et al., 2018). Among the participants, 8 new leprosy cases were detected representing 0.7% of skin conditions (4 cases of multibacillary and 4 cases of paucibacillary form). This percentage was slightly higher than the 0.3% reported one study conducted in the district of Lalo in Benin (Barogui et al., 2018). The number of leprosy cases detected in our study is higher than that reported in a study conducted in a regional hospital center in Burkina Faso who found 5 leprosy cases (Korsaga et al., 2018).
However, our percentage was lower than that reported in a study conducted in Côte d'Ivoire (Koffi et al., 2020). The divergence in the results may be due to the difference in study populations and sample sizes.
Our study also resulted in the early detection of 8 cases of leprosy, including a 14-year-old girl. This paediatric patient reflects recent transmission of leprosy in the study communities and thus represents a warning sign to increase epidemiological surveillance of leprosy and to further promote active screening during mobile consultations in these communities. These leprosy patients, fortunately diagnosed without visible deformities, were administered MDT to ensure proper healing due to the implementation of the integrated approach.
Despite the results in this study, it has several limitations. One limitation is the use of the reasoned choice technique (non-probability method), which prevents us from generalizing our results to a larger population. Another limitation is the absence of an established dermatologist in the screening team. This limitation is related to the scarcity of dermatologists in Benin (about 15). Nevertheless, skin conditions diagnosed in the field were assessed by dermatologists to minimize nomenclature bias. Another limitation of our study is the organization of community-based fairground consultations that may constitute a barrier to participation in the study for some individuals with ugly lesions may be ashamed to show themselves in public (Sermrittirong et al., 2015; Hofstraat and van Brakel, 2016). Finally, the exclusively community-based clinic in the present study could result in many children, especially school children, being missed during screening. It would then be important to use the integrated approach by combining community and school surveys. This was done by researchers in Cameroon who successfully combined community and school-based surveys for the detection of Buruli ulcer and yaws (Boock et al., 2017).
CONCLUSION
The integrated approach in the control of neglected tropical diseases with cutaneous manifestations was effective in the leprosy-endemic municipalities of Djidja, Ouinhi, Zagnanado and Kétou in Benin. The success of this implementation was possible due to the availability and involvement of community health volunteers, health agents and local elected officials and to the receptivity of beneficiary communities. This success is also due to the technical and institutional support of the two programmes in charge of the control in Benin: the PNLLUB and the PNLMTN. According to the importance of this approach, it would be necessary to extend this type of study to other leprosy and Buruli ulcer endemic municipalities in Benin.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors appreciate the National Program for the Control of Leprosy and Buruli Ulcer of Benin (PNLLUB) and the National Program for the Control of Neglected Tropical Diseases (PNLMTN) for their administrative and technical support in conducting this study and also thank the Raoul Follereau Foundation (http://www.raoulfollereau.org), the ANESVAD Foundation (http://www.anesvad.org/fr) and the World Health Organization (https://www.who.int/fr) for their support in the control of leprosy and Buruli ulcers in Benin.
REFERENCES
|
Alvar J, Vélez ID, Bern C, Herrero M, Desjeux P, Cano J, Jannin J, den Boer M, WHO Leishmaniasis Control Team (2012). Leishmaniasis worldwide and global estimates of its incidence. PloS one 7(5):e35671. |
|
|
Amazigo U (2008). The African programme for onchocerciasis control (APOC). Annals of Tropical Medicine and Parasitology 102(sup1):19-22. |
|
|
Barogui YT, Diez G, Anagonou E, Johnson RC, Gomido IC, Amoukpo H, Bachirou ZS, Houezo JG, Saizonou R, Sopoh GE (2018). Integrated approach in the control and management of skin neglected tropical diseases in Lalo, Benin. PLoS Neglected Tropical Diseases 12(6):e0006584. |
|
|
Bilgili ME, Yildiz H, Sarici G (2013). Prevalence of skin diseases in a dermatology outpatient clinic in Turkey. A cross-sectional, retrospective study. Journal of Dermatological Case Reports 7(4):108 |
|
|
Bissek A-CZ-K, Tabah EN, Kouotou E, Sini V, Yepnjio FN, Nditanchou R, Nchufor RN, Defo D, Dema F, Fonsah JY, Njamnshi AK, Muna WF (2012). The spectrum of skin diseases in a rural setting in Cameroon (sub-Saharan Africa). BMC Dermatology 12(1):7 |
|
|
Boock AU, Awah PK, Mou F, Nichter M (2017). Yaws resurgence in Bankim, Cameroon: The relative effectiveness of different means of detection in rural communities. PLoS neglected tropical diseases 11(5):e0005557. |
|
|
Engelman D, Fuller LC, Solomon AW, McCarthy JS, Hay RJ, Lammie PJ, Steer AC (2016). Opportunities for integrated control of neglected tropical diseases that affect the skin. Trends in Parasitology 32(11):843-854 |
|
|
Géniaux M (2010). Lèpre ou pas lèpre?? Bulletin de l'ALLF 25:26-27 |
|
|
Hofstraat K, van Brakel WH (2016). Social stigma towards neglected tropical diseases: a systematic review. International Health 8(suppl_1):i53-i70. |
|
|
Hogewoning A, Amoah A, Bavinck JNB, Boakye D, Yazdanbakhsh M, Adegnika A, De Smedt S, Fonteyne Y, Willemze R, Lavrijsen A (2013). Skin diseases among schoolchildren in Ghana, Gabon, and Rwanda. International Journal of Dermatology 52(5):589-600. |
|
|
Hotez PJ, Molyneux DH, Fenwick A, Kumaresan J, Sachs SE, Sachs JD, Savioli L (2007). Control of neglected tropical diseases. New England Journal of Medicine 357(10):1018-1027. |
|
|
INSAE (2016). Effectifs de la population des villages et Quartiers de ville du Bénin (RGPH4). Ministère du Plan et du Développement, Cotonou, Bénin. |
|
|
Koffi AP, Yao TAK, Barogui YT, Diez G, Djakeaux S, Zahiri MH, Sopoh GE, Santos S, Asiedu KB, Johnson RC (2020). Integrated approach in the control and management of skin neglected tropical diseases in three health districts of Côte d'Ivoire. BMC Public Health 20:1-9. |
|
|
Korsaga N, Ilboudo L, Bado B, Andonaba J-B, Barro F, Niamba P, Traoré A (2018). Profil épidémiologique, clinique et thérapeutique des dermatoses observées dans un centre hospitalier régional (CHR) du Burkina Faso. Elsevier pp. S243-S244. |
|
|
Mitjà O, Lukehart SA, Pokowas G, Moses P, Kapa A, Godornes C, Robson J, Cherian S, Houinei W, Kazadi W (2014). Haemophilus ducreyi as a cause of skin ulcers in children from a yaws-endemic area of Papua New Guinea: a prospective cohort study. The Lancet Global Health 2(4):e235-e241. |
|
|
Mitjà O, Marks M, Bertran L, Kollie K, Argaw D, Fahal AH, Fitzpatrick C, Fuller LC, Garcia Izquierdo B, Hay R (2017). Integrated control and management of neglected tropical skin diseases. PLoS Neglected Tropical Diseases 11(1):e0005136. |
|
|
Mitjà O, Marks M, Konan DJ, Ayelo G, Gonzalez-Beiras C, Boua B, Houinei W, Kobara Y, Tabah EN, Nsiire A (2015). Global epidemiology of yaws: a systematic review. The Lancet Global Health 3(6):e324-e331. |
|
|
OMS (2018a). Intégrer les maladies tropicales négligées dans l'action pour la santé mondiale et le développement: quatrième rapport de l'OMS sur les maladies tropicales négligées. |
|
|
OMS (2018b). Comment reconnaître les maladies tropicales négligées selon les altérations de la peau. Guide de formation à l'usage du personnel sanitaire de première lignes. |
|
|
OMS (2016). Stratégie mondiale de lutte contre la lèpre 2016-2020?: parvenir plus rapidement à un monde exempt de la lèpre?: manuel opérationnel. |
|
|
Paek SY, Koriakos A, Saxton?Daniels S, Pandya AG (2012). Skin diseases in rural Yucatan, Mexico. International Journal of Dermatology 51(7):823-828. |
|
|
PNLLUB (2019). Rapport de monitoring lèpre. Ministère de la Santé, Cotonou, Bénin. |
|
|
Rao G, Kumar S (2003). Pattern of skin diseases in an Indian village. Indian Journal of Medical Sciences 57(3):108-110. |
|
|
Richard M, Corgibet F, Beylot?Barry M, Barbaud A, Bodemer C, Chaussade V, D'Incan M, Joly P, Leccia M, Meurant J (2018). Sex?and age?adjusted prevalence estimates of five chronic inflammatory skin diseases in France: results of the «OBJECTIFS PEAU» study. Journal of the European Academy of Dermatology and Venereology 32(11):1967-1971. |
|
|
Sermrittirong S, Van Brakel WH, Kraipui N, Traithip S, Bunders-Aelen J (2015). Comparing the perception of community members towards leprosy and tuberculosis stigmatization. Leprosy Review 86(1):54-61. |
|
|
Tizek L, Schielein M, Seifert F, Biedermann T, Böhner A, Zink A (2019). Skin diseases are more common than we think: screening results of an unreferred population at the Munich Oktoberfest. Journal of the European Academy of Dermatology and Venereology 33(7):1421-1428. |
|
|
van de Sande WW (2013). Global burden of human mycetoma: a systematic review and meta-analysis. PLoS Negl Trop Dis 7(11):e2550. |
|
|
Walker S, Shah M, Hubbard V, Pradhan H, Ghimire M (2008). Skin disease is common in rural Nepal: results of a point prevalence study. British Journal of Dermatology 158(2):334-338. |
|
|
World Health Organization (WHO) (2014) Global programme to eliminate lymphatic filariasis: progress report, 2013. Weekly Epidemiological Record= Relevé épidémiologique hebdomadaire 89(38):409-418 |
|
|
World Health Organization (WHO) (2016) Accelerating towards a leprosy-free world. Global Leprosy Strategy 2016-2020. India |
|
|
World Health Organization (WHO) (2010). Working to overcome the global impact of neglected tropical diseases: first WHO report on neglected tropical diseases. World Health Organization. |
|
|
Wootton C, Bell S, Philavanh A, Phommachack K, Soukavong M, Kidoikhammouan S, Walker S, Mayxay M (2018). Assessing skin disease and associated health-related quality of life in a rural Lao community. BMC Dermatology 18(1):1-10 |
|
|
Yotsu RR, Murase C, Sugawara M, Suzuki K, Nakanaga K, Ishii N, Asiedu K (2015). Revisiting buruli ulcer. The Journal of Dermatology 42(11):1033-1041 |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


