Full Length Research Paper

ABSTRACT
Comorbidity of diabetes mellitus and hypertension is common, with both diseases and their treatment being able to cause liver function abnormalities, which can lead to liver failure. This study aims to access the effect of drugs used in the management of these diseases on liver function. A cross-sectional study will be conducted, followed by a case-control design. Ethical clearance will be obtained from the Faculty of Health Sciences Institutional Review Board and administrative authorization from the various hospital directorates. The sampling procedure adopted will be consecutive and shall include all consenting patients aged 21 years and above, treated for hypertension, diabetes mellitus, or both. Pregnant women, patients with liver disease, viral hepatitis, as well as those on known hepatotoxic drugs will be excluded. Clinical, lifestyle, anthropometric data as well as venous blood samples will be collected and analyzed for liver enzymes (aspartate transaminase, alanine transaminase, and gamma glutamyl transferase) total or conjugated bilirubin, hepatitis B surface antigen and hepatitis C virus antibodies. Student T-test will be used to compare means and chi-square to test for proportion. Associated factors will also be determined using odds ratios. A p-value of <0.05 will be considered significant. The prevalence of liver function abnormalities shall be determined. Determinants of liver function abnormalities shall also be identified.
Key words: Liver function tests, diabetes mellitus, hypertension, treatment, liver failure.
INTRODUCTION
Diabetes mellitus (DM), also known as diabetes, is a group of metabolic disorders characterized by persistently high blood sugar levels caused by defects in insulin secretion, insulin action, or both (Shaw et al., 2010; American Diabetes Association, 2014). In 2010, the global prevalence of diabetes among adults (aged 20–79 years) was 6.4 percent, affecting 285 million adults, and is expected to rise to 7.7 percent, affecting 439 million adults, by 2030 (Shaw et al., 2010). Hypertension (defined as a blood pressure ≥140/90 mmHg) is an extremely common comorbid condition in diabetes, affecting ∼20-60% of patients with diabetes, depending on obesity, ethnicity and age (Delacroix et al., 2014). In Africa, the prevalence of hypertension can be as high as 40% in some countries (van de Vijver et al., 2013) while in Cameroon, it spans from 5.7% in rural settings through 21.9% in semi-urban to 47.5% in urban milieu (Arrey et al., 2016).
Diabetes and hypertension are common conditions. Type 2 diabetes mellitus is becoming more common as are the associated co-morbidities such as Hypertension. As a result, a diabetic patient must take multiple medications at the same time to slow the progression of the disease and to reduce the risk of drug interactions, and failure to monitor the liver may have an impact on the patient's quality of life (Amin and Suksomboon, 2014). There are numerous anti-diabetic and anti-hypertensive medications available, and many people with these two diseases are advised to take more than one type of medication. Drug-drug interactions are a common cause of adverse drug effects, which can be avoided if they are reported on time (Carter, 2002). Drug-drug interaction is defined as any alteration in the pharmacokinetics or pharmacodynamics, produced by different substances, other drug treatments, dietary factors and habits such as alcohol drinking and smoking. These interactions can affect the anti-hypertensive drugs, altering their therapeutic efficacy, and causing toxic effects of hepatotoxicity (Jáuregui-Garrido and Jáuregui-Lobera, 2012).
Drug metabolism is an important process for the removal of unwanted substances from the body. Certain drugs used have a direct or indirect action on the liver or are simply metabolized by it. The liver is a vital organ in drug metabolism that plays an important role in the regulation of most homeostatic processes in the body. Both phase I (mainly CYP450s) and phase II (mainly UGTs) enzymes play a significant role in drug metabolism. Although metabolites in general, are expected to be inactive and nontoxic, certain metabolites can cause hepatotoxicity (Almazroo et al., 2017).
Hepatotoxicity is the injury or liver damage caused by exposure to drugs; it is an adverse drug reaction that may be uncommon but serious. Hepatic injury can be classified into hepatocellular, cholestatic and mixed, caused by an increase in alanine aminotransferase and alkaline phosphatase than the upper limit of normal (Dara and Kaplowitz, 2020). Recent epidemiological studies suggested that patients with diabetes are twice as likely to suffer hepatic failure compared to patients who have not diabetes. Increased incidences of hepatotoxicity have been observed in patients with diabetes receiving drug therapies (De-Boer et al., 2017). Drug?induced liver injury (DILI) is an increasingly recognized clinical problem encompassing over 50% of cases of acute liver failure in the United States (Paniagua et al., 2018). Drug-induced liver injury is responsible for 5% of all hospital admissions and 50% of all acute liver failures. A higher incidence was found in Spain in 2005, with 34.2 per 1000000 inhabitants per year, and 16.6 per 1000000 inhabitants per year being serious life-threatening episodes (Alempijevic et al., 2017).
A major limitation in DILI diagnosis and prediction is the current lack of specific biomarkers. Despite the refined usage of traditional liver biomarkers in DILI, reliable disease outcome predictions are still difficult to make. These limitations have driven the growing interest in developing new more sensitive and specific DILI biomarkers (microRNAs (miRNA), mechanistic biomarkers HMGB-1, Cytokeratin-18 and microRNAs (miRNA), mechanistic biomarkers HMGB-1 and Cytokeratin-18), which can improve early DILI prediction, diagnosis, and course of action (Robles-Díaz et al., 2016). The most important cause of liver dysfunction is drug-induced liver injury (DILI) which can lead to a wide spectrum of symptoms ranging from mild non-specific symptoms like asymptomatic transaminitis, acute hepatitis, chronic hepatitis, cholestasis, and liver failure (Bashir et al., 2020).
Concomitant drugs are associated with an increased risk of drug interactions. The study recommends that continuous medical education of healthcare workers on drug interactions should be initiated and done continuously (Khandeparkar and Rataboli, 2017). Managing the liver disease is an important component of the care of people living with diabetes and hypertension. However, there are few structures limited study that has so far evaluated the burden of drug combination on treatment on the advent of liver injury in our country. An assessment of the associated factors would help weigh benefits against risk before the prescription. Finally, these outcomes could help establish a baseline record which could serve as a monitoring rod indicating whether we are improving on the safety or regressing. In this study, we seek to: (i) Identify patient under antihypertensive, antidiabetic, and both treatments presenting with liver abnormality. (ii) To assess the liver abnormality profile associated with respective therapy in a case-control approach. (iii) To identify the risk factors associated with abnormal liver function tests in all groups. (iv) Determine the predictive abnormal liver function test among patients under antihypertensive and anti-diabetic or both treatments. (v) Determine the effect of drug combinations associated with abnormal liver function among patients under antihypertensive and antidiabetic or both treatments.
MATERIALS AND METHODS
Study design
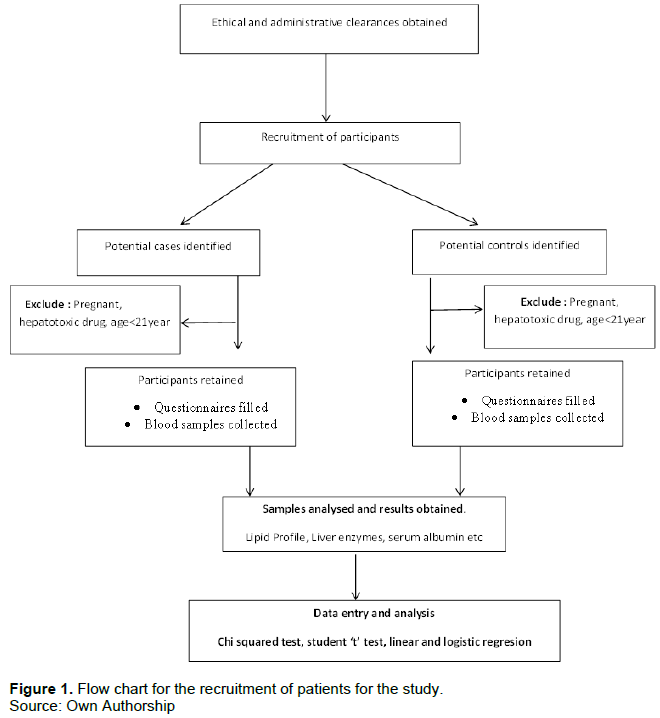
A cross-sectional study will be conducted, followed by a case-control design. Patients with hypertension and diabetes or both comorbidities who have been receiving treatment for at least 5 years shall be recruited for the cross-sectional design to determine the prevalence of liver injury. Among these patients, those presently with liver abnormality shall be included as cases and their counterparts without the liver abnormality as the control group in the case-control study to determine the determinants of liver function abnormality (figure 1).
Study setting
We will carry out a hospital-based study carried out in the Internal medicine Departments of the Douala General (DGH) and Laquintinie Hospitals. These departments have resident Endocrinologists, Cardiologists, and Nephrologist, amongst others, who follow up and manage persons with hypertension and diabetes. All the experts mentioned above are reasons why these centers are suitable sites for the study to be carried out.
Sample size determination for the cross-sectional study
The sample size was determined using the formula for sample size calculation.
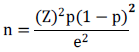
Where n= sample size,
Z= = 1.96 (standard normal value at 95% confidence level)
p= 50% (to the best of our knowledge, as of the time of elaboration of this protocol, no study evaluating liver function abnormalities in a patient with hypertension and diabetes on treatment had been done. As such we use the estimated prevalence of 50%)
e= precision of the event of interest = 0.05. Thus:

A minimum of 385 participants will be recruited for a cross-sectional study.
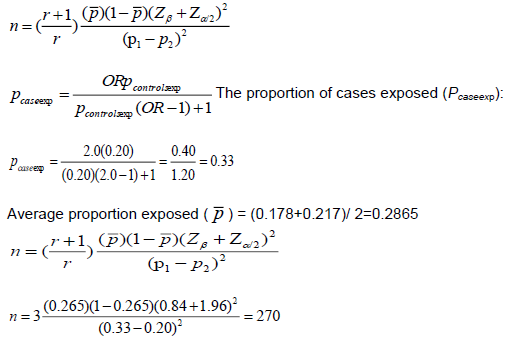
Sample size determination for the case-control study
The sample size shall be calculated assuming that:
80% as the power, Zb=0.84
At a 0.05 significance level, Za=1.96
r =ratio of controls to cases (2:1)
OR= assuming an odds ratio of 0.5
The proportion exposed in the control group is 21.7% (Pcontrolexp) following a study done on the prevalence of liver function abnormalities in patients with T2D.
Sampling method
We shall carry out a sequential study; a cross-sectional then a case-control study. A consecutive sampling method will be used to recruit subjects. Samples shall be obtained from each hospital in proportion to the number of patients treated in each center, that is, probability proportionate to size. We shall define diabetes as a patient with fasting whole blood glucose level > 126 mg/dl, a previous diagnosis of diabetes mellitus, or a patient on anti-diabetic medication and Hypertension: as a patient with Systolic Blood Pressure ≥ 140 mmHg and/or a diastolic Blood Pressure ≥ 90 mmHg, or a previous diagnosis of hypertension or on long-term antihypertensive medications. We shall define liver injury as patient with abnormal liver function test.
Study procedures
Ethical approval will be obtained from the Institutional review board of the Faculty of Health Sciences, University of Buea (2018_864_098_SG_IRB_FSH) followed by administrative authorization from the Regional Delegation of Public Health for the Littoral Region, as well as the Directorate of the Douala General, Laquintinie Hospitals, and Bonassama district Hospitals. We will then proceed to pre-test our data collection instruments. Following ethical and administrative approvals, we shall proceed to host a one-day training seminar for our research assistants at the Bonassama district hospital. The training manual shall contain the following topics: basic concepts on the research topic, ethics in medical research, informed consent and its common pitfalls, challenges and how to recruit participants, how to administer the questionnaire, how to use and enter data.
Training of research assistants
This training will be done by lectures followed by question and answer sessions. At the end of the training workshop, we shall proceed to pre-test the questionnaire to ensure its validity, reliability as well as ensure that it responds to all specific objectives. We shall then proceed to recruit our participants. We shall explain the study in detail to patients presently at the Internal medicine service of the Douala General and Laquintinie Hospitals for follow-up of hypertension and diabetes comorbidities and treatment naïve hypertension or diabetes patients.
This will be done to the patients in a language that they understand. If the patient does not understand French, English, or Pidgin English an interpreter would be solicited to translate. The patient or their representative will be required to sign a consent form, a copy of which shall be given to them.
Administration of a questionnaire
After obtaining informed consent, a brief history, review of the patient's file, and physical examination will be done to ensure the patient fits all inclusion criteria and has no exclusion criteria as well fill the questionnaire. Those that fulfill any of the exclusion criteria will be dropped from the study. The physical examination will involve blood pressure and anthropometric measurements like weight, height, and waist circumference. All the information obtained will be entered into a predesigned questionnaire. The questionnaire is divided into the following sections:
(i) Socio-demographic data: Date of birth, gender, marital status, and level of education
(ii) History taking: Smoking, alcohol use, hypertension, diabetes, gouty arthritis, malignancy, Cerebrovascular accident, HIV, HBsAg, HCV antibodies status, diabetes mellitus, and current drugs.
(iii) Physical examination: weight, height, waist circumference, and blood pressure.
Anthropometric measurement
Anthropometric measurements (weight, height, waist circumference, and blood pressure) shall be obtained using standard protocols and techniques. After removal of shoes and heavy clothing; height will be measured using a stadiometer, the weight will be measured using a calibrated bathroom scale and waist circumference will be determined using a measuring tape. Body mass index (BMI) will be calculated using the Quetelet’s formula. Waist circumference will be measured midway between the lower costal margin and the iliac crest to the nearest centimeter.
Arterial blood pressure
Arterial blood pressure will be measured using an automated sphygmomanometer after sitting for at least 15 min. Blood pressure measurements will be taken according to the Joint National Committee VII criteria (JNC VII). Three readings will be taken at 5 min intervals. The mean of the three measurements will be recorded.
Laboratory investigations
We shall also determine the patient’s laboratory baseline biochemical indicators. Five milliliters of venous blood will be collected from each patient into a dry vacutainer test tube following Standard Operating Procedures. The sample will be transported in a biohazard flask at 4°C for testing at the Laquintinie hospital and Douala general hospital. All blood samples will be refrigerated and stored at -20°C at the end of the analysis until two years after completion of studies. The transaminases (ALAT, ASAT, ?GT), bilirubin T, and C) were analyzed using an auto-analyzer and hepatitis B virus surface antigen, serum anti–hepatitis C virus antibody will be analyzed using Enzyme Linked Immunosorbent Assay on ErbaLisascan II automated microplate reader. Serum level of total bilirubin >10 g/dl, and direct bilirubin >4 g/dl was considered as abnormal. The level of ALT >33 U/L and AST >31 U/L for females and ALT >40 U/L and AST >37 U/L for males were classified as abnormal. Fasting blood sugar (FBS) was >110 mg/dl. Anthropometric measurement (weight, height) was measured according to WHO guidelines by trained nurses. Body mass index (BMI) was calculated as weight divided by height squared (kg/ m2) and classified as underweight (BMI < 18.5 kg/m2), normal weight (18.5-24.9 kg/m2), overweight (BMI = 25-29.9 kg/m2) and obese (BMI ≥ 30 kg/m2). Blood pressure was taken by qualified personnel using a sphygmomanometer and stethoscope. Systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg or current use of blood pressure-lowering medication was used to define hypertension. Laboratory quality control will be done regularly to verify inter- and intra-assay reproducibility.
Data management
All questionnaires and data entry forms will be cross-checked daily to ensure completeness and consistency. All questionnaires will be kept in a safe cupboard. Data will be entered and analyzed in Epi Info version 7.2.2. Copy of raw data alongside all analysis will be stored in a dedicated account on Google drive.
DATA ANALYSIS
Data will be entered and analyzed in Epi Info version 7.2.2. Categorical variables; Sex, level of education, and clinical factors such as comorbidities, and treatment regimens will be summarized using frequencies and percentages. Continuous variables such as age, Serum albumin, transaminases, and lipid profile will be summarized using means, standard deviations, medians, and interquartile range where necessary. Group comparisons for categorical variables will be done using the chi-squared test (or Fisher’s exact test where appropriate) while the independent samples t-test, will be used for comparing group means for continuous variables.
Logistic regression will be done to identify associated factors.
Presentation and reporting of results
Data collection is ongoing and statistical results shall be presented using frequency distribution tables. Quantitative variables such as alkaline phosphate (ALP), alpha-fetoprotein, transaminases (ALAT, ASAT, ?GT), total and conjugated bilirubin will be summarized as mean and standard deviation where appropriate.
What is already known on this topic?
(i) Anti-hypertensive medications can cause idiosyncratic drug-induced liver injury.
(ii) Anti-diabetic medications can cause idiosyncratic drug-induced liver injury.
What this study adds
(i) The prevalence of liver abnormality in hypertension and diabetic co-morbid population on treatment for over 5 years.
(ii) The combination of antihypertensive and antidiabetic drugs potentiates liver enzyme abnormalities.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors appreciate the contribution by all staff of the Faculty of Health Sciences towards improving the quality of this work. The input of all Ph.D. students in the faculty has been great.
REFERENCES
|
Alempijevic T, Zec S, Milosavljevic T. (2017) Drug-induced liver injury: Do we know everything?. World journal of hepatology 9(10):491-502. doi: 10.4254/wjh.v9.i10.491. PMID: 28443154; PMCID: PMC5387361. |
|
|
Almazroo OA, Miah MK, Venkataramanan R (2017). Drug metabolism in the liver. Clinics in liver disease 21(1):1-20. |
|
|
American Diabetes Association (2014). Diagnosis and classification of diabetes mellitus. Diabetes care 37(Supplement_1):S81-S90. |
|
|
Amin M, Suksomboon N (2014). Pharmacotherapy of type 2 diabetes mellitus: an update on drug-drug interactions. Drug safety 37(11):903-919. |
|
|
Arrey WT, Dimala CA, Atashili J, Mbuagbaw J, Monekosso GL (2016). Hypertension, an emerging problem in rural Cameroon: prevalence, risk factors, and control. International Journal of Hypertension, 2016. |
|
|
Bashir A, Sarwal P, Mehta D (2020). Liver Toxicity. In: StatPearls. Treasure Island (FL). Stat Pearls. Accessed 22 May 2020. |
|
|
Carter B. (2002). The extent of potential antihypertensive drug interactions in a Medicaid population. American Journal of hypertension 15(11):953-957. |
|
|
Dara L, Kaplowitz N (2020). Drug?Induced Liver Injury. In: Arias IM, Alter HJ, Boyer JL, Cohen DE, Shafritz DA, Thorgeirsson SS et al., editors. The Liver. Wiley pp. 701-713. |
|
|
De Boer IH, Bangalore S, Benetos A, Davis AM, Michos ED, Muntner P, Bakris G. (2017). Diabetes and hypertension: a position statement by the American Diabetes Association. Diabetes care 40(9):1273-1284. |
|
|
Delacroix S, Chokka RG, Worthley SG (2014). Hypertension: Pathophysiology and treatment. J Neurol Neurophysiol 5(6):1-8. |
|
|
Jáuregui-Garrido B, Jáuregui-Lobera I (2012). Interacciones entre fármacos antihipertensivos y alimentos. Nutrición Hospitalaria 27(6):1866-1875. |
|
|
Khandeparkar A, Rataboli P (2017). A study of harmful drug-drug interactions due to polypharmacy in hospitalized patients in Goa Medical College. Perspectives in clinical research 8(4):180. |
|
|
Paniagua AC, Amariles P (2018). Hepatotoxicity by Drugs. In: Mahlangu N, editor. Pharmacokinetics and Adverse Effects of Drugs - Mechanisms and Risks Factors. InTech. |
|
|
Robles-Díaz M, Medina-Caliz I, Stephens C, Andrade RJ, Lucena MI (2016). Biomarkers in DILI: one more step forward. Frontiers in pharmacology 7:267. |
|
|
Shaw JE, Sicree RA, Zimmet PZ (2010). Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes research and clinical practice 87(1):4-14. |
|
|
van de Vijver S, Akinyi H, Oti S, Olajide A, Agyemang C, Aboderin I, Kyobutungi C (2014). Status report on hypertension in Africa-Consultative review for the 6th Session of the African Union Conference of Ministers of Health on NCD's. Pan African Medical Journal 16(1). |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


