Full Length Research Paper

ABSTRACT
Sexually transmitted infections pose a public health crisis globally and in low and middle-income countries, and substance use has been linked to an increased risk of engaging in risky sexual behaviors among youths. This work aims to explore the relationship between substance use and risky sexual behaviors among school-based youths in Liberia. An 86-question survey was developed to collect information about substance use and sexual behaviors. The survey was validated using qualitative data obtained from focus groups of Liberian youths. 400 students were sampled with a mean age of 18.15 ±2.14 years. Students who use alcohol were 2.4 times more likely to have multiple sexual partners (OR=2.38, CI= 1.06–5.32, p=0.035), 11 times more likely to engage in unwanted sexual activity (OR=10.86, CI=1.36–86.96, p=0.025); marijuana use increased the risk of multiple unintended pregnancies (OR=5.49, CI= 1.37–22.03, p=0.016); users of heroin had 4 times the odds of engaging in unwanted sexual activity (OR=4.18, CI= 1.07-16.37, p=0.039). Substance use increases the risk of engaging in risky sexual behaviors among youths in Liberia. Intervention programs that target individual, community, and societal level determinants are needed to tackle risky sexual behaviors in this population.
Key words: Risky sexual behaviors, substance use, Liberia, youths, adolescents, sexually transmitted infections (STIs).
INTRODUCTION
Risky sexual behaviors, unintended pregnancy, and sexual violence are common among youths in Sub-Saharan Africa (Doyle et al., 2012; Kebede et al., 2005; Tolera et al., 2019). Risky sexual behaviors, defined as activities that put people at increased risk for Sexually Transmitted Infections (STIs), include: having unprotected sexual intercourse; having multiple sexual partners over one’s lifetime; having intercourse with a casual partner; sexual initiation at a young age; sexual intercourse with commercial sex workers; bartering sex for money, goods or other favors; engaging in sexual activity under the influence of alcohol/drugs; and sexual violence (Madise et al., 2007; Perera and Abeysena, 2018).
Adolescence is a time of developmental, physiological, and behavioral changes, and is characterized by increased autonomy, peer influence, risk-taking behaviors such as initiation of sex, and alcohol/drug use (Doyle et al., 2012; Tapert et al., 2001). Adolescents are more likely to have multiple sexual partners, engage in unprotected intercourse, and choose high-risk partners compared to adults (Tapert et al., 2001). The study of adolescent sexual behavior is important as approximately 60% of youths worldwide are currently infected with STIs, including HIV (Da Ros and da Silva Schmitt, 2008). STIs continue to pose a public health crisis globally and in low and middle-income countries (LMICs) (Ritchwood et al., 2015). Although youths make up about 25% of the sexually active population; they comprise 50% of the population with newly acquired STIs. In LMICs, STIs are amongst the top ten diseases reported by both young adult males and females, and the second most commonly reported disease among young adult females (Da Ros and da Silva Schmitt, 2008).
Earlier studies conducted in Liberia among in-school youths and young adults have found high rates of risky sexual behaviors. In one study conducted in 2008, 78% of youths were found to be sexually active (Quiterio et al., 2013). Of those who were sexually active, 24.9% reported having sex for money and 20.9% had never used a condom (Quiterio et al., 2013). Males were also found to be more likely to have sex, have multiple sexual partners, and initiate sex early (Quiterio et al., 2013). Another study among youths in Liberia found 34% of their sample had their sexual debut at less than 15 years of age (defined as early sexual debut), and 21% of those who were sexually active had multiple sexual partners (Kennedy et al., 2012). Furthermore, 26% of sexually active youths had never used a condom, 11% had got pregnant or got someone pregnant one or more times, and 11% reported sexual assault (Kennedy et al., 2012). Among 1,119 young women aged 14- 25 years surveyed in Montserrado County in Liberia, 72% reported engaging in transactional sex. Of these women, 67% had early sexual debut, 91% had multiple sexual partners, and 61% had at least one pregnancy (Okigbo et al., 2014). Youths in post-conflict Liberia face daily challenges that put them at increased risk of risky sexual behaviors as a result of the effects of the civil war on the country’s infrastructure, education, and healthcare (Okigbo et al., 2014).
Substance use has been linked to an increased risk of engaging in risky sexual behaviors among youths. Studies report increased rates of early age of sexual intercourse, having multiple sexual partners, and lower rates of condom use among youths who use substances compared to those who do not (Connell et al., 2009; Madkour et al., 2010; Tucker et al., 2012; Vasilenko and Lanza, 2014). Among youths in Liberia, very few studies have been conducted to explore the relationship between risky sexual behaviors and substance use. One such study did not find any association between alcohol use and transactional sex (Okigbo et al., 2014)while another study found an association between alcohol use and engaging in sex and having multiple sexual partners - but no other substances were explored (Quiterio et al., 2013). Use of substances other than alcohol among youths has been found to be associated with risky sexual behaviors including the use of marijuana (Andrade et al., 2013; Grossman et al., 2004), cocaine (Castrucci and Martin, 2002; Tolou-Shams et al., 2010), and other drugs including stimulants and methamphetamines (Castrucci and Martin, 2002; Kebede et al., 2005; Tolera et al., 2019). This study aims to explore the relationship between the use of various substances and risky sexual behaviors among school-based youths in Liberia and to identify other risk factors that may be associated with risky sexual behaviors in this population.
METHODOLOGY
Study design
An 86-question survey was developed by the research team using several sources including the CDC 2017 State and Local Youth Risk Behavior Survey, the 2016 Indiana College Substance Use Survey, the WHO 2013 Global School-Based Student Health Survey, the 2011 European School Survey Project on Alcohol and Other Drugs, a paper on Risk Factors and Consequences of Substance Use among Youths in Post Conflict Liberia (Lippitt, 2013), and the original 2008 pilot survey (Harris et al., 2012). The survey was validated using qualitative data obtained from focus group discussion conducted at two secondary schools in the capital of Liberia, Monrovia, to identify the local terminology used by Liberian youths to describe common substances and sexual behaviors. The revised survey, containing the list of local terminologies in parenthesis, was then administered in English to students from eight secondary schools in a classroom setting.
Data collection
The sampling frame included co-educational secondary schools in central and greater Monrovia. Recruitment letters were mailed to a total of 55 eligible schools; of the schools that responded expressing interest in participating in the study, ten schools were randomly selected for inclusion. Of the ten schools included in the study, two schools were randomly selected to participate in phase 1 of the study, while the remaining eight schools participated in phase 2. For phase 1, students participated in focus group discussions to provide feedback on the study survey. For phase 2, 50 students were randomly selected from each participating school, totaling 400 students across all eight schools. Study staff included a total of 10 research assistants (two research assistants per school), affiliated with the A.M. Dogliotti Medical College at the University of Liberia, who received training on study procedures including obtaining consent, facilitating focus group discussions, administering surveys, and entering data. All data collection occurred during the month of October 2018.
Phase 1: Survey validation
In order to conduct the rapid validation of the survey, the study staff held a focus group discussion at two secondary schools to receive students’ feedback on the format and content of the developed survey. Each school had 1 focus group consisting of 9-10 male and female secondary students. Each focus group was led by two research assistants using a semi-structured discussion guide in a private area of the school during school hours. Before beginning each session, research assistants provided instructions to students that participation was voluntary, all responses shared would remain anonymous, and there would be no repercussions for their responses. All students provided written consent to participate in the focus group discussions; students under the age of 18 years provided written assent and permission signed by their parent or guardian prior to participation in the study. Research assistants then asked students to review the developed survey before taking part in a focus group discussion regarding students’ thoughts on the survey. Research assistants remained present in the classroom for the entire session, which lasted approximately for 60 min. One research assistant facilitated the group discussion while the other took written notes and audio recorded the session. Upon focus group completion, the research assistants’ notes and audio recordings were reviewed by the study research team and used to revise the survey prior to phase 2.
Phase 2: Survey distribution
In phase 2 of the study, the revised survey was administered by two research assistants per school to a total of eight schools. Research assistants provided instructions to students and reinforced that the survey was anonymous and voluntary and that there would be no repercussions to their responses. Surveys were then distributed to students with both research assistants and a school representative present in the classrooms. Once the consenting process was complete, data were collected on demographics including age, sex, grade, living arrangements, family SES relative to others, history of being a child soldier, county/city of origin, ethnicity, languages spoken, and religion. The survey also asked questions about the lifetime and current prevalence of substance use (including alcohol, tobacco, marijuana, heroin, cocaine, and other drugs), as well as risk factors for substance use (including the role of peers and sexual behaviors).Study data were entered and managed using the REDCap electronic data capture tool hosted at Boston University (Boston University, CTSI 1UL1TR001430).
Measures
Risky sexual behaviors were measured using 16 questions that covered 11 risky sexual behaviors: early sexual debut; unwanted sexual activity; number of sexual partners; sexual assault; number of unintended pregnancies; sex for money, drugs or grades; sex with relatives; use of birth control; and use of substances before sex. Early sexual debut was defined as the initiation of sex at or less than the age of 15 years. The question was, “How old were you when you were sexually active (did man or woman business) for the first time? Circle one” with answer choices ranging from 11 to 18 years and above. Unwanted sexual activity was defined as engaging in unwanted sexual activity as a result of the use of alcohol and/or other drugs. A question for the use of birth control allowed more than one option to be checked (options included the use of condoms, pills, injectables, others and none). Questions about peer approval about sex, being encouraged by parents to engage in sex, social norms about the age of sexual initiation, knowledge of safe sex, and access to condoms were also asked.
Statistical analysis
Data were analyzed using SAS version 9.4 (SAS Institute, 2012).
Age was categorized into two groups – younger than 18 years, and 18 years and older. Risky sexual behaviors were stratified by gender and Pearson Chi-square tests were used to determine gender differences in risky sexual behaviors. Bivariate analyses were done using Pearson Chi-square test to test the association between any risky sexual behavior and substance use, and using a simple logistic regression model with risky sexual behavior as the dependent variable and use of substances as predictor variables. Finally, a multiple logistic regression analysis was conducted with a model adjusting for age, sex, family socioeconomic status, and other determinants of risky sexual behaviors (such as access to condoms, safe sex knowledge, parental approval of sex, peer approval of sex, and school type). For all of the tests, statistical significance was set at alpha of 0.05. Odds ratios and 95% confidence intervals are reported for all statistically significant variables.
Ethical approval
Ethical approval for the study was done by the University of Liberia-Pacific Institute for Research and Evaluation Institutional Review Board (UL-PIRE IRB) and the Boston University Medical Campus Institutional Review Board (BUMC IRB). Approval of the study was also received from the Liberian Ministry of Health and Social Welfare, and the Ministry of Education.
RESULTS
Demographic characteristics
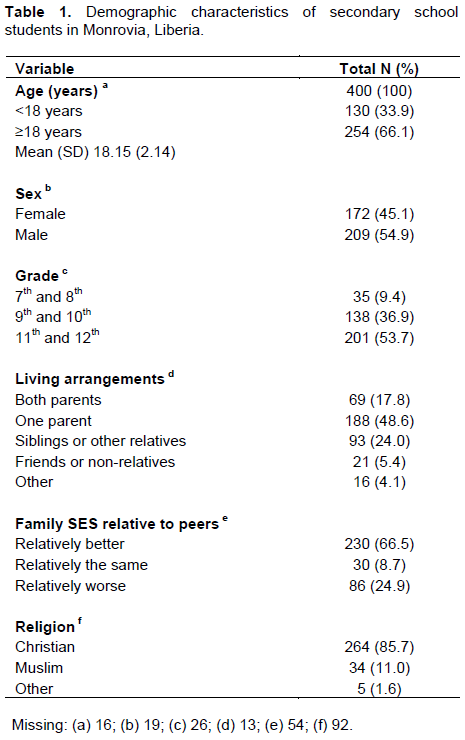
A total of 400 students were sampled with age ranging between 12 and 23 years, and a mean of 18.15 ±2.14 years. Of these students, 209 (54.9%) were males, 254 (66.2%) were aged 18 years and above, and 299 (74.8%) were from private high schools. Demographic characteristics of the study sample are presented in Table 1.
Risky sexual behaviors
Of the 400 students in the sample, 58% (n=222) were sexually active, and of these, 64.4% were males. Of those who were sexually active: 34.1% (n=74) initiated sex at age 15 years and below, 38.6% (n=83) had 2 – 5 sexual partners, 22.8% (n=49) had 6 or more sexual partners, 28.8% (n=64) reported using no form of birth control, 24% (n=49) had at least one unintended pregnancy, and 25.1% (n=53) reported experiencing sexual assault, 19.6% (n=42) reported using substances before sex, 16.6% (n=35) engaged in unwanted sexual activity as a result of using substances, 14.8% (n=31) had had sex for money, 8.2% (n=17) had sex in exchange for drugs, 6.8% (n=14) had exchanged sex for grades, and 18.6% (n=39) had sex with an older relative or adult (Table 2).
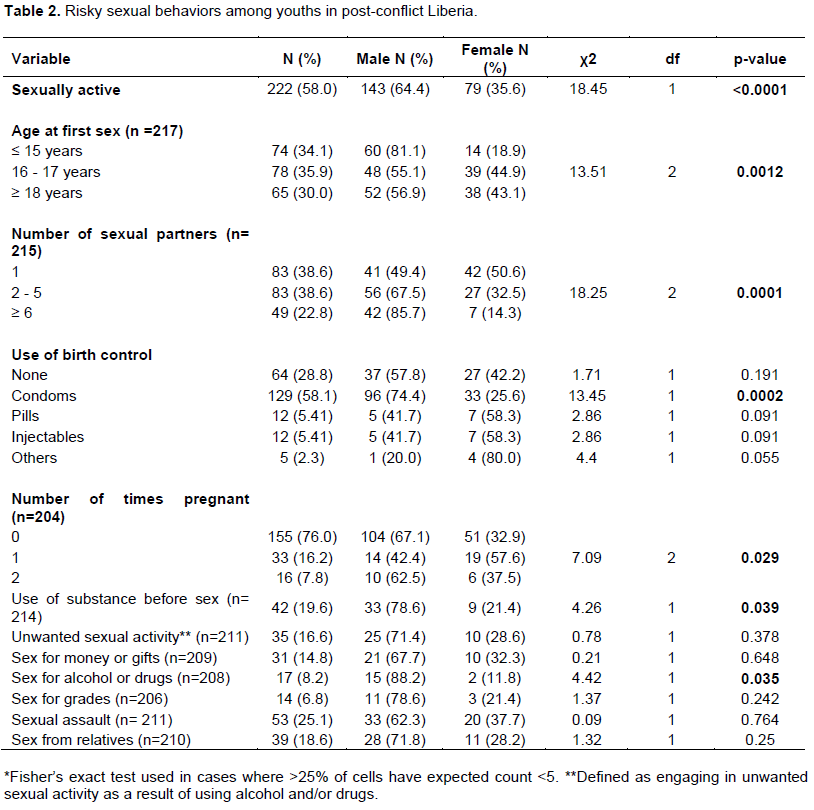
Compared to females, males were more likely to: have multiple sexual partners (χ2=18.25, df=2, p=0.0001), use substances before sex (χ2=4.26, df=1, p=0.039), engage in sexual activities for drugs (χ2=4.42, df=1, p=0.035), initiate sexual activity at a younger age (χ2=13.51, df=2, p=0.0012), and use condoms (χ2=13.45, df=1, p=0.0002). There was a non-linear association observed between gender and unintended pregnancies (χ2=7.09, df=2, p=0.029) with more females (57.6%) reporting one unintended pregnancy compared to males (42.4%). However, more males reported two or more unintended pregnancies (62.5%) compared to females (37.5%). The only association found between age and risky sexual behaviors was related to having multiple sexual partners. Students 18 years and older were more likely to have multiple sexual partners compared to those younger than 18 years (χ2=11.12, df=2, p=0.004).
Substance use and risky sexual behaviors
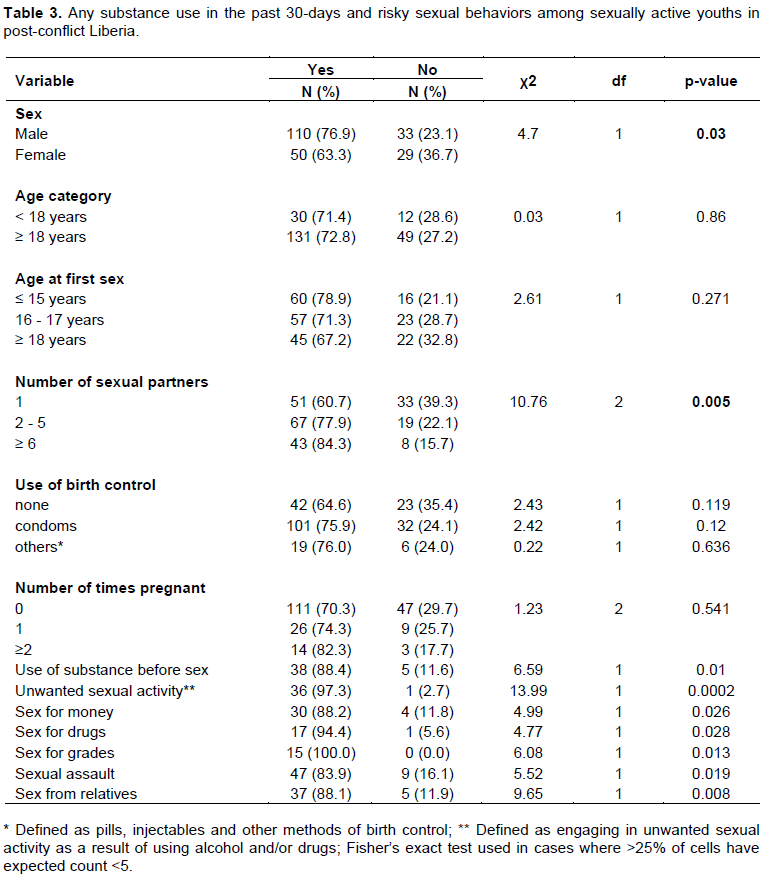
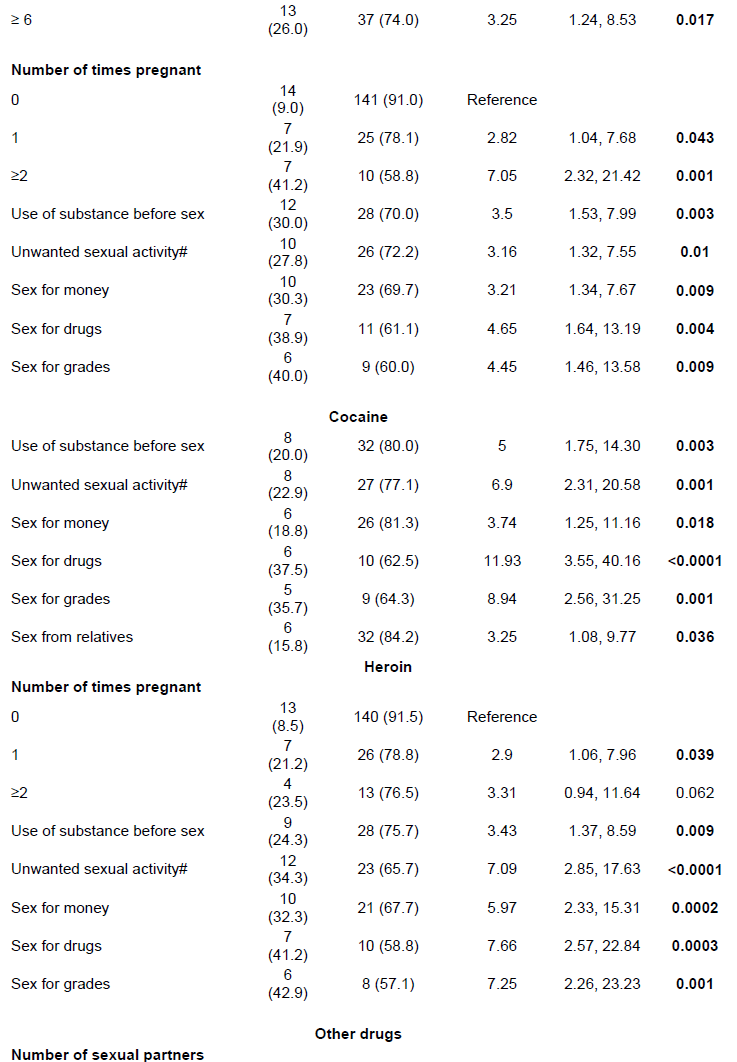
Among those students who were sexually active, risky sexual behaviors were associated with the use of any substances in the past 30 days in the bivariate analysis - except for age of sexual debut, unintended pregnancy and use of birth control (Table 3). When each substance was examined (Table 4), use of alcohol, tobacco, marijuana, cocaine, heroin alcohol use was associated with: having multiple sexual partners, using substances before sex, engaging in unwanted sexual activity, and sex with relatives. Use of tobacco was associated with having 6 or more sexual partners, having 2 unintended pregnancies, use of substances before sex, having unwanted sexual activity, having sex for money, having sex in exchange for drugs, having sex in exchange for grades, experiencing sexual assault, and having sex with relatives. Marijuana use was associated with: having 6 or more sexual partners, having one or more unintended pregnancies, use of substances before sex, having unwanted sexual activity, having sex for money, having sex in exchange for drugs, and having sex in exchange for grades. Cocaine use was associated with: use of substances before sex, having unwanted sexual activity, having sex for money, having sex in exchange for drugs, having sex in exchange for grades, and having sex with relatives. Use of heroin was associated with: having 2 or more unintended pregnancies, use of substances before sex, having unwanted sexual activity, having sex for money, having sex in exchange for drugs, and having sex in exchange for grades. The use of other drugs wasassociated with: having 6 or more sexual partners, use of substances before sex, having unwanted sexual activity, having sex in exchange for drugs, experiencing sexual assault, and having sex from relatives.


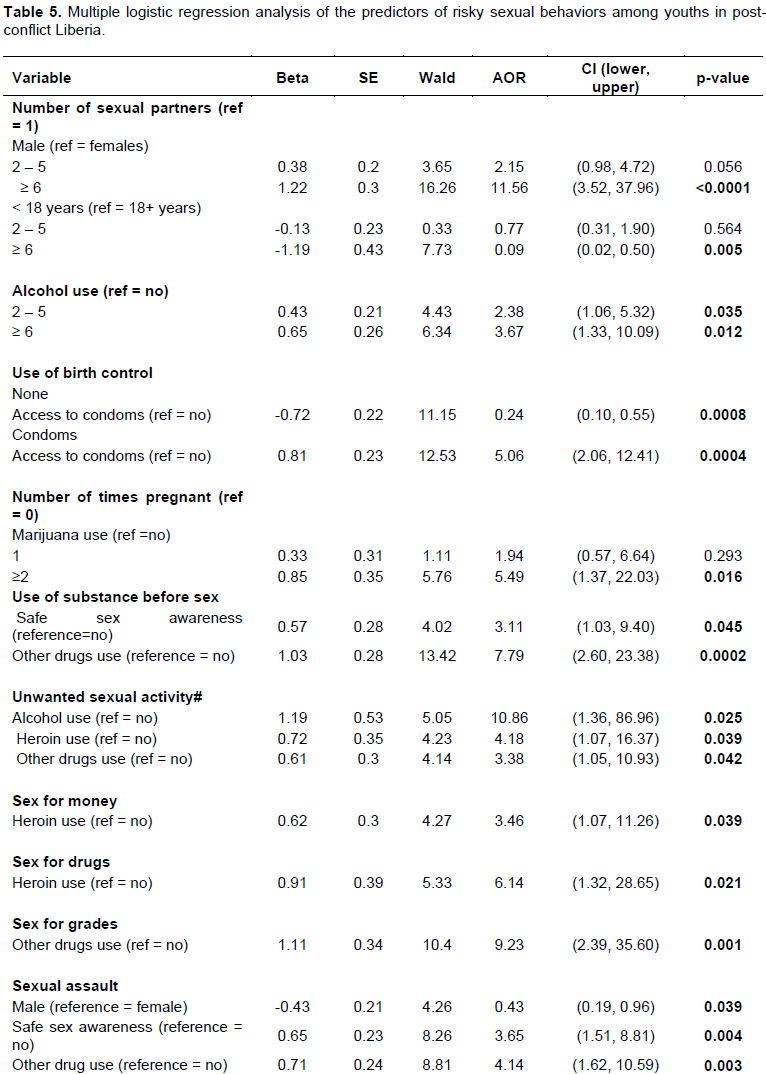
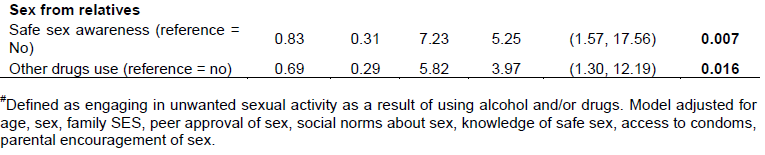
Independent predictors of risky sexual behaviors
In the final multivariable logistic regression model (Table 5), students who use alcohol were 2.4 times more likely to have 2-5 sexual partners (OR=2.38, CI= 1.06–5.32, p=0.035), 3.7 times more likely to have 6 or more sexual partners (OR=3.67, CI= 1.33–10.09, p=0.012), and 11 times more likely to engage in unwanted sexual activity (OR=10.86, CI= 1.36–86.96, p=0.025) compared to those who do not drink alcohol. Marijuana use increased the risk of multiple unintended pregnancies (OR=5.49, CI= 1.37-22.03, p=0.016). Those who use heroin have 4 times the odds of engaging in unwanted sexual activity (OR=4.18, CI= 1.07-16.37, p=0.039), 3 times the odds of having sex for money (OR=3.46, CI= 1.07-11.26, p=0.039), and 6 times the odds of having sex for drugs (OR=6.14, CI= 1.32-28.65, p=0.021). Those who were using other drugs were more likely to use substances before sex (OR=7.79, CI= 2.60-23.38, p=0.0002), engage in unwanted sexual activity (OR=3.38, CI= 1.05-10.93, p=0.042), exchange sex for grades (OR=9.23, CI= 2.39-35.60, p=0.001), experience sexual assault (OR=4.14, CI=1.62-10.59, p=0.003), and engage in sexual activities with relatives (OR=3.97, CI= 1.30-12.19, p=0.016).Being male, having knowledge of safe sex, and having access to condoms were also independent predictors of engaging in risky sexual behaviors. Males were 12 times more likely to have 6 or more sexual partners compared to females (OR=11.56, CI= 3.52-37.96, p<0.0001) and were 60% less likely to be victims of sexual assault (OR=0.43, CI= 0.19-0.96, p=0.039). Having access to condoms increased the odds of using a condom (OR=5.06, CI= 2.06–12.41, p=0.0004) and decreased the odds of not using any form of birth control (OR=0.24, CI= 0.10–0.55, p=0.0008). Having knowledge of safe sex increased the risk of using substances before sex (OR=3.11, CI= 1.03–9.40, p=0.045), having sex with relatives (OR=3.97, CI= 1.30–12.19, p=0.016), and having experienced sexual assault (OR=3.65, CI= 1.51–8.81, p=0.004).
DISCUSSION
This study examined the relationship between substance use and risky sexual behaviors among youth in Liberia. The findings from this study show that most school-based Liberian youths are sexually active (58% with a higher prevalence of sexually active male students than female) and those risky sexual behaviors are prevalent among Liberian youths. In the study sample, 1 in 4 youths reported sexual assault, about 3 in 10 youth had sex at 15 years or younger. In addition, 1 in 5 reported substance use before sex, 1 in 6 had unwanted sex as a result of substance use, and between 6.8 and 18.6% had transactional sex for money, grades or drugs.
In an earlier study among youths in Liberia, the proportion of youths who were sexually active was higher than that reported in the current study (78 vs. 58%) (Quiterio et al., 2013). This difference may be due to the higher average age of study participants in the 2008 study compared to those in the current study. In Sub-Saharan Africa, a trend towards less risky sexual behaviors has been reported (Doyle et al., 2012). Changes in technology, increasing use of social media by youths, and an increase in education about STIs and HIV in schools have led to a decline in the prevalence of sexual activity among youths (Ethier et al., 2018). Although the civil war in Liberia damaged the education and healthcare systems, there have been attempts to revitalize school-based social services and formulate adolescent sexual health policies (Kennedy et al., 2012).
The reduced prevalence of sexually active youths in this study may be the result of such interventions.
Similar to this study, another study conducted among 802 adolescents in Liberia found the proportion of those who initiated sex at ages 15 years and younger was 34% (Kennedy et al., 2012). While the prevalence of sexual activity appears to be reducing, the prevalence of early initiation of sex appears static. Substance use, lack of parental supervision, encouragement by parents to engage in transactional sex, and socioeconomic difficulties have all been cited as reasons for the persistence of early initiation of sexual activity (Gizaw et al., 2014; Kassa et al., 2015; Mazengia and Worku, 2009; Rudatsikira et al., 2007). Early sexual debut is associated with increased risk of STIs including HIV (Shrestha et al., 2016; Stöckl et al., 2013), having multiple sexual partners (Shrestha et al., 2016; Son et al., 2016; Yaya and Bishwajit, 2018)and engaging in other risky sexual behaviors (Baumgartner et al., 2009; Okigbo et al., 2014; Shrestha et al., 2016).
In a sample of young females in Liberia, 70% of those who were sexually active had traded sex for material benefits (Okigbo et al., 2014). In this study, the prevalence among females was much lower (14.8%) which may be due to the sampling methods that were restricted to in-school youths. This may have impacted the prevalence of risky sexual behaviors reported in this study because out-of-school youths have a higher prevalence of risky sexual behaviors compared to in-school youths (Ndyanabangi et al.,2004). However, the prevalence of sexual activity among females was higher than those previously reported by Atwood et al. in a sample of in-school youths in Liberia (Atwood et al., 2012). Transactional sex increases the risk of STIs and HIV because it often involves age and power differentials, a reduction in the capacity of youth (usually female) to negotiate condom use, and often involves substance use (Atwood et al., 2012). Transactional sex also increases the likelihood of sexual assault and violence (Atwood et al., 2011; Okigbo et al., 2014). In the current study, there were no gender differences found in engagement in transactional sex similar to an earlier study by Quiterio et al. (Quiterio et al., 2013)among youths in Liberia. Other studies found that females are usually more likely to engage in transactional sex and, in some instances, are encouraged to engage in transactional sex by their parents in order to contribute to the family’s income (Atwood et al., 2011; Okigbo et al., 2014; Tolera et al., 2019). A significant proportion of adolescent boys have also been found to engage in transactional sex (Adjei and Saewyc, 2017; Moore and Biddlecom, 2007).
In the current study, 1 in 4 youths had experienced sexual violence, which is similar to prevalence rates reported among youths in Ethiopia (Tolera et al., 2019). However, this rate is higher than those reported in two studies conducted among 8th graders (ages 12 – 23 years) in public schools in South Africa where the prevalence of sexual violence was 9.5 and 3.9% respectively (De Vries et al., 2014; Pöllänen et al., 2018). Similar to other studies (Atwood et al., 2012; Tolera et al., 2019), our study found that females were more likely to experience sexual violence compared to males. However, in two studies among youth in South-Africa, the prevalence of sexual violence was found to be higher in males compared to females (De Vries et al., 2014; Pöllänen et al., 2018). This suggests that it is possible that sexual violence is common in males but due to the lack of focus on sexual violence in males, it has largely gone underreported. Similar to transactional sex, it may be that males are suffering in silence, especially given the culture of masculinity in many African countries where men are not allowed to complain or show any signs of weakness (Adjei and Saewyc, 2017).
The study found that 58% of sexually active youths reported condom use, while 28.8% reported no form of contraception use. The rate of condom use in this study is higher than earlier studies conducted in Liberia (Kennedy et al., 2012; Okigbo et al., 2014; Quiterio et al., 2013), Ethiopia (Kebede et al., 2005; Tolera et al., 2019), Ghana, Uganda, Malawi, and Burkina-Faso (Madise et al., 2007). In a review of risky sexual behaviors of countries in Sub-Saharan Africa, the average rate of condom use was found to be below 50% (Doyle et al., 2012). Though encouraging, this result should be interpreted with caution as this study was carried out in the capital city of Monrovia, and it has been shown that condom use is lower in rural areas (Doyle et al., 2012; Madise et al., 2007). Youths who reported having access to condoms in this study were more likely to use a condom. Making condoms accessible is an effective strategy in increasing condom use and promoting positive sexual behaviors among youths (Wang et al., 2018). However, other studies have noted that condom access is not the only factor that predicts condom use among in-school adolescents; lack of accurate information about condoms and misinformation can also contribute to low condom use among youths (Atwood et al., 2011; Tolera et al., 2019), as well as negative attitudes towards condom use (Ndyanabangi et al., 2004). As reported in other studies (Kennedy et al., 2012), males were more likely to use condoms in our study and were more likely to demonstrate self-efficacy in the purchase and correct usage of condoms (Meekers and Klein, 2002). Females are usually disadvantaged in negotiating condom use, especially considering potential age and power differentials involved (Atwood et al., 2011; Moore and Biddlecom, 2007; Okigbo et al., 2014).
Risky sexual behaviors were found to be associated with substance use in this study. The use of alcohol, marijuana, heroin, and other drugs increased the risk of engaging in risky sexual behaviors. Although cocaine and tobacco use were associated with risky sexual behaviors in the bivariate analysis, they were no longer statistically significant in the multivariable analysis. Alcohol use in youths has been found to be associated with having multiple sexual partners (Doku, 2012; Oppong et al., 2014; Quiterio et al., 2013), engaging in transactional sex (Okigbo et al., 2014; Oppong et al., 2014), and having unprotected sex (Kebede et al., 2005; Oppong et al., 2014). In contrast, other studies have reported no association between alcohol use in youths and risky sexual behaviors (Espinoza et al., 2019; Tolera et al., 2019). Alcohol consumption decreases inhibitions, affects rational thinking and decision making, and increases risk-taking behaviors. These effects may be amplified in youths (Kebede et al., 2005; Ritchwood et al., 2015).
Similarly, marijuana use in youths has been reported to increase the risk of unintended pregnancies (Cavazos-Rehg et al., 2011; Jonas et al., 2016), multiple sexual partners (Doku, 2012; Oppong Asante et al., 2014)and transactional sex (Oppong et al., 2014). Like alcohol, marijuana use also decreases inhibitions and increases risk-taking behaviors (Espinoza et al., 2019). In a study among eighth-graders in South Africa, Palen et al. (2006) found that marijuana use increases the risk of casual sex; however, there was no association with condom use. The authors concluded that in designing interventions, the message should be framed to reflect the link between substance use and casual sex, and how that may increase the risk of STIs and unintended pregnancies. This message may increase consistent condom usage among youths (Palen et al., 2006).
Similar to previous studies among youths in Ghana and the United States (Doku, 2012; Espinoza et al., 2019; Tapert et al., 2001), youths who reported heroin use had an increased risk of engaging in unwanted sexual activity and transactional sex compared to youths who did not use heroin. Those who use other drugs (including drugs such as tramadol, diazepam, amphetamines, and other stimulants) were also more likely to engage in risky sexual behaviors, including having unwanted sexual activity and transactional sex. Studies among youths in Ghana and Ethiopia have reported associations between risky sexual behaviors and the use of stimulants (such as khat), diazepam, and hallucinogens (Doku, 2012; Kebede et al., 2005; Tolera et al., 2019).
The risk of engaging in risky sexual behaviors is said to be higher in youths who use alcohol alone or in combination with other substances. Among high-risk youths, those who used marijuana but not alcohol had less risk of engaging in risky sexual behaviors than youths who used alcohol alone or in combination with other substances (Gillman et al., 2018). Therefore, interventions to reduce substance use in the context of risky sexual behaviors may be more effective when alcohol consumption is targeted either alone or in combination with other substances (Gillman et al., 2018). This is important because, among youths who use substances, alcohol is the most common substance consumed (Quiterio et al., 2013; Tolera et al., 2019). Although in the final regression analysis, tobacco and cocaine use were not associated with risky sexual behaviors in this study, associations between tobacco use and risky sexual behaviors have been reported among youth in Ghana (Doku, 2012; Oppong et al., 2014), Scotland (Jackson et al., 2012), and the United States (Espinoza et al., 2019).
Our study identified an association between substance use and risky sexual behaviors among youths in Liberia, a country recovering from decades of conflict. Although this relationship is not causal, the co-occurrence of substance use and risky sexual behaviors in youths can produce a synergistic effect to cause adverse health consequences (Jackson et al., 2012). It is, therefore, necessary to develop effective intervention programs to address substance use and risky sexual behaviors among this population. Effective intervention will address the determinants of these behaviors at multiple levels – individual, community, and societal/policy. Interventions targeted at the individual level may be delivered in a school setting and should consist of educational programs targeted at both substance use and risky sexual behaviors with context regarding their interactive effects. Additionally, interventions should aim to increase self-efficacy in condom acquisition and correct use. Ideally, these educational components should be targeted before the initiation of sexual activity (before the age of 15 years). However, it should be noted that knowledge of safe sex is not enough to prevent youths from engaging in risky sexual behaviors. In our study, those with knowledge about safe sex were more likely to engage in risky sexual behaviors, including transactional sex and non-use of condoms. Therefore, educational programs must be paired with other interventions to formulate a comprehensive intervention to tackle risky sexual behaviors in youths. School-based interventions have been shown to be effective in reducing risky sexual behaviors among adolescents. In South Africa, Jemmott et al. (2010)conducted a school-based intervention program among 1,057 sixth grade students, consisting of one-hour sessions that included interactive exercises, games, brainstorming, role-playing, and group discussions. They reported a reduction in unprotected vaginal intercourse, vaginal intercourse and multiple sexual partners among students who received the intervention compared to controls (Jemmott et al., 2010).
Future interventions should also include community-based programs that address the location and affordability of condoms to make condoms more accessible. School clinics are ideal locations for making condoms available and can be paired with safe sex education. Previous research has found that parental support for condoms has been declining and that perceived parental approval for condom use is associated with increased condom use (Doyle et al., 2012). Therefore, interventions to address risky sexual behaviors among youths must also target the parents. In addition, studies reveal that parents sometimes encourage and pressure female children to engage intransactional sex, which should also be a target for intervention in reducing risky sexual behaviors (Atwood et al., 2011; Okigbo et al., 2014).
On the society/policy level, the fundamental needs of the population must be addressed, such as poverty, unemployment, and trauma. Interventions to address risky sexual behaviors among youths, especially transactional sex, have often failed because the drivers of these behaviors are economic (Atwood et al., 2012; Okigbo et al., 2014). School policies should be enacted and enforced to prevent the exploitation of students by teachers for grades. Though not highlighted in this study, students in high school have reported being coerced by teachers to have sex in exchange for better grades (Atwood et al., 2011; Tolera et al., 2019). To stop male teachers from sexually harassing female students in South Africa, the National Department of Education introduced an amendment to the Employment of Educators
Act that requires provincial departments of education to dismiss any educator found guilty of having a sexual relationship with a learner of the school where he or she is employed. The South African Council for Educators (SACE) Act also makes provision for the removal from the register of any educator found guilty of a breach of the code of professional ethics (Prinsloo, 2006). According to Prinsloo, the following recommendations may be put in place to prevent exploitation of students by teachers: 1) developing a school culture in which values and human rights are protected, promoted and fulfilled; 2) equipping the learners with the necessary skills to be able to assert themselves in cases of emotional and sexual harassment, victimization, intimidation, hate speech and all forms of sexism; 3) creating an awareness of the definition and different forms of sexual harassment; 4) developing a standard of conduct among gender groups; 5) creating a climate of trust in which stereotyping is avoided; 6) encouraging female learners to talk to educators who are trusted about any incident of sexual harassment or sexual abuse; and 7) creating a safe school environment conducive to effective teaching and learning (Prinsloo, 2006). In addition to policies, school personnel training has also been shown to be an effective intervention program to reduce the exploitation of students by teachers. (Schwandt and Underwood, 2016)
This study has several limitations that must be considered in interpreting the findings. First, it was conducted among selected schools in Monrovia, which is an urban area. Our findings may not be generalizable to youths in rural areas and to out-of-school youth. Indeed, studies have found that compared to in-school youths, out-of-school youths have a much higher prevalence of risky sexual behaviors and less opportunity for safe sex education (Ndyanabangi et al., 2004; Oppong Asante et al., 2014). Second, the study utilized a self-report survey that may be subject to social desirability bias. Also, several of the variables contained missing data which may affect the overall effect of the associations detected in this study. Third, this study did not take into account psychiatric morbidity in assessing both the prevalence of substance use and the increased risk of engaging in risky sexual behaviors. Among youths, it has been shown that among risky sexual behaviors, substance use and psychological distress are interconnected (Caminis et al., 2007; Page and hall,2009).
CONCLUSION
This study found that risky sexual behaviors are quite common among youths in Liberia and that substance use among youth increases the risk of engaging in risky sexual behaviors. These behaviors put them at increased risk of STIs including HIV, unintended pregnancies and sexual violence. Intervention programs that target individual, community, and societal level determinants are needed to tackle risky sexual behaviors in this population. Educational programs for youths should start early (before the initiation of sexual activity and consequent school drop-out), provide accurate information about the risk associated with risky sexual behaviors, discuss the link between substance use and risky sexual behaviors, provide accurate information about condom use, and promote self-efficacy to obtain and use condoms. Community-based interventions should promote parental support for condom use, and parental disapproval of transactional sex and other risky sexual behaviors. Policy interventions should focus on tackling poverty and unemployment, and enacting and enforcing policies to prevent sexual exploitation of youths.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors are grateful for the following local research assistants from the A.M. Dogliotti College of Medicine at the University of Liberia who carried out data collection for the study: Wilbur TS Harris, Emmanuel D Lah, Clarice Dixon, Terry Juty Socro, Emmanuel Flomo, Matthew Kolleh, Theophilus Sieka, James T Helb Jr, Harriet N Yangian, and Kodjo N Tehoungue and also appreciate the support of the Liberia Ministry of Health and the Liberia Ministry of Education. This work was supported by the National Institute of Mental Health under Grant Number K01MH100428.
REFERENCES
|
Adjei JK, Saewyc EM (2017). Boys are not exempt: Sexual exploitation of adolescents in sub-Saharan Africa. Child Abuse and Neglect 65:14-23. |
|
|
Andrade LF, Carroll KM, Petry NM (2013). Marijuana use is associated with risky sexual behaviors in treatment-seeking polysubstance abusers. The American Journal of Drug and Alcohol Abuse 39(4):266-271. |
|
|
Atwood KA, Kennedy SB, Barbu EM, Nagbe W, Seekey W, Sirleaf P, Sosu F (2011). Transactional sex among youths in post-conflict Liberia. Journal of Health, Population and Nutrition 29(2):113-122. |
|
|
Atwood KA, Kennedy SB, Shamblen S, Taylor CH, Quaqua M, Bee EM, Dennis B (2012). Reducing sexual risk taking behaviors among adolescents who engage in transactional sex in post-conflict Liberia. Vulnerable Children and Youth Studies, 7(1):55-65. |
|
|
Baumgartner JN, Geary CW, Tucker H, Wedderburn M (2009). The Influence of Early Sexual Debut and Sexual Violence on Adolescent Pregnancy: A Matched Case-Control Study in Jamaica. International Perspectives on Sexual and Reproductive Health 35(1):21-28. |
|
|
Caminis A, Henrich C, Ruchkin V, Schwab-Stone M, Martin A (2007). Psychosocial predictors of sexual initiation and high-risk sexual behaviors in early adolescence. Child and Adolescent Psychiatry and Mental Health, 1(1):14. |
|
|
Castrucci BC, Martin SL (2002). The Association Between Substance Use and Risky Sexual Behaviors Among Incarcerated Adolescents. Maternal and Child Health Journal 6(1):43-47. |
|
|
Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, Schootman M, Cottler LB, Bierut LJ (2011). Substance Use and the Risk for Sexual Intercourse With and Without a History of Teenage Pregnancy Among Adolescent Females. Journal of Studies on Alcohol and Drugs 72(2):194-198. |
|
|
Connell CM, Gilreath TD, Hansen NB (2009). A multiprocess latent class analysis of the co-occurrence of substance use and sexual risk behavior among adolescents. Journal of Studies on Alcohol and Drugs 70(6):943-951. |
|
|
Da Ros CT, da Silva Schmitt C (2008). Global epidemiology of sexually transmitted diseases. Asian Journal of Andrology 10(1):110-114. |
|
|
De Vries H, Eggers SM, Jinabhai C, Meyer-Weitz A, Sathiparsad R, Taylor M (2014). Adolescents' Beliefs About Forced Sex in KwaZulu-Natal, South Africa. Archives of Sexual Behavior 43(6):1087-1095. |
|
|
Doku D (2012). Substance use and risky sexual behaviours among sexually experienced Ghanaian youth. BMC Public Health 12(1):571. |
|
|
Doyle AM, Mavedzenge SN, Plummer ML, Ross DA (2012). The sexual behaviour of adolescents in subâ€Saharan Africa: patterns and trends from national surveys. Tropical Medicine and International Health 17(7):796-807. |
|
|
Espinoza L, Richardson JL, Ferguson K, Chou CP, Baezconde-Garbanati L, Stacy AW (2019). Adolescent Substance Use and Sensation-Seeking on Sexual Behaviors Among Young Adults from Continuation High Schools. Substance Use and Misuse, pp. 1-11. |
|
|
Ethier KA, Kann L, McManus T (2018). Sexual Intercourse Among High School Students - 29 States and United States Overall, 2005-2015. MMWR. Morbidity and Mortality Weekly Report 66(5152):1393-1397. |
|
|
Gillman AS, Yeater EA, Feldstein Ewing SW, Kong AS, Bryan AD (2018). Risky Sex in High-Risk Adolescents: Associations with Alcohol Use, Marijuana Use, and Co-Occurring Use. AIDS and Behavior, 22(4):1352-1362. |
|
|
Gizaw A, Jara D, Ketema K (2014). Risky sexual practice and associated factors among high school adolescent in Addis Ababa, Ethiopia, 2014. Family Medicine and Medical Science Research 3(141):2. |
|
|
Grossman M, Kaestner R, Markowitz S (2004). Get high and get stupid: The effect of alcohol and marijuana use on teen sexual behavior. Review of Economics of the Household 2(4):413-441. |
|
|
Harris BL, Levey EJ, Borba CPC, Gray DA, Carney JR, Henderson DC (2012). Substance use behaviors of secondary school students in post-conflict Liberia: a pilot study. International Journal of Culture and Mental Health 5(3):190-201. |
|
|
Jackson C, Sweeting H, Haw S (2012). Clustering of substance use and sexual risk behaviour in adolescence: analysis of two cohort studies. BMJ Open 2(1):e000661. |
|
|
Jemmott JB, Jemmott LS, O'Leary A, Ngwane Z, Icard LD, Bellamy SL, Makiwane MB (2010). School-Based Randomized Controlled Trial of an HIV/STD Risk-Reduction Intervention for South African Adolescents. JAMA Pediatrics 164(10):923-929. |
|
|
Jonas K, Crutzen R, van den Borne B, Sewpaul R, Reddy P (2016). Teenage pregnancy rates and associations with other health risk behaviours: a three-wave cross-sectional study among South African school-going adolescents. Reproductive Health 13(1):50. |
|
|
Kassa GM, Tsegay G, Abebe N, Bogale W, Tadesse T, Amare D, Alem G (2015). Early Sexual Initiation and Associated Factors among Debre Markos University Students, North West Ethiopia. Science Journal of Clinical Medicine 4(5):80. |
|
|
Kebede D, Alem A, Mitike G, Enquselassie F, Berhane F, Abebe Y, Gebremichael T (2005). Khat and alcohol use and risky sex behaviour among in-school and out-of-school youth in Ethiopia. BMC Public Health 5(1):109. |
|
|
Kennedy SB, Atwood KA, Harris AO, Taylor CH, Gobeh ME, Quaqua M, Warlonfa M (2012). HIV/STD Risk Behaviors Among In-School Adolescents in Post-conflict Liberia. Journal of the Association of Nurses in AIDS Care, 23(4):350-360. |
|
|
Lippitt MW (2013). Risk factors and consequences of substance use among youth in post-conflict Liberia: A qualitative study. Yale Universi. Retrieved from https://elischolar.library.yale.edu/ysphtdl/1175/ |
|
|
Madise N, Zulu E, Ciera J (2007). Is poverty a driver for risky sexual behaviour? Evidence from national surveys of adolescents in four African countries. African Journal of Reproductive Health 11(3):83-98. |
|
|
Madkour AS, Farhat T, Halpern CT, Godeau E, Gabhainn SN (2010). Early adolescent sexual initiation as a problem behavior: a comparative study of five nations. Journal of Adolescent Health 47(4):389-398. |
|
|
Mazengia F, Worku A (2009). Age at sexual initiation and factors associated with it among youths in North East Ethiopia. Ethiopian Journal of Health Development 23(2). |
|
|
Meekers D, Klein M (2002). Understanding Gender Differences in Condom Use Self-Efficacy among Youth in Urban Cameroon. AIDS Education and Prevention 14(1):62-72. |
|
|
Moore AM, Biddlecom A (2007). Transactional sex among adolescents in sub-Saharan Africa amid the HIV epidemic. [Unpublished] 2007. Presented at the Population Association of America 2007 …. |
|
|
Ndyanabangi B, Kipp W, Diesfeld HJ (2004). Reproductive Health Behaviour among In-School and Out-of-School Youth in Kabarole District, Uganda. African Journal of Reproductive Health / La Revue Africaine de La Santé Reproductive 8(3):55-67. |
|
|
Okigbo CC, McCarraher DR, Chen M, Pack A (2014). Risk factors for transactional sex among young females in post-conflict Liberia. African Journal of Reproductive Health 18(3):133-141. |
|
|
Oppong Asante K, Meyer-Weitz A, Petersen I (2014). Substance use and risky sexual behaviours among street connected children and youth in Accra, Ghana. Substance Abuse Treatment, Prevention, and Policy 9(1):45. |
|
|
Page RM, Hall CP (2009). Psychosocial Distress and Alcohol Use as Factors in Adolescent Sexual Behavior Among Sub-Saharan African Adolescents. Journal of School Health 79(8):369-379. |
|
|
Palen LA, Smith EA, Flisher AJ, Caldwell LL, Mpofu E (2006). Substance Use and Sexual Risk Behavior among South African Eighth Grade Students. Journal of Adolescent Health 39(5):761-763. |
|
|
Perera UAP, Abeysena C (2018). Prevalence and associated factors of risky sexual behaviors among undergraduate students in state universities of Western Province in Sri Lanka: a descriptive cross sectional study. Reproductive Health 15(1):105. |
|
|
Pöllänen K, de Vries H, Mathews C, Schneider F, de Vries PJ (2018). Beliefs About Sexual Intimate Partner Violence Perpetration Among Adolescents in South Africa. Journal of Interpersonal Violence. |
|
|
Prinsloo S (2006). Sexual harassment and violence in South African schools. South African Journal of Education 26(2):305-318. |
|
|
Quiterio N, Harris BL, Borba CPC, Henderson DC (2013). Substance use and sexual risk behaviours amongst in-school youth and young adults living in Liberia. African Journal of Drug and Alcohol Studies 12(2). |
|
|
Ritchwood TD, Ford H, DeCoster J, Sutton M, Lochman JE (2015). Risky sexual behavior and substance use among adolescents: A meta-analysis. Children and Youth Services Review 52:74-88. |
|
|
Rudatsikira E, Ogwell AE, Siziya S, Muula AS (2007). Prevalence of sexual intercourse among school-going adolescents in Coast Province, Kenya. Tanzania Journal of Health Research 9(3):159-165. |
|
|
SAS Institute. (2012). SAS versión 9.4. SAS Institute Inc. |
|
|
Schwandt HM, Underwood C (2016). Engaging school personnel in making schools safe for girls in Botswana, Malawi, and Mozambique. International Journal of Educational Development 46:53-58. |
|
|
Shrestha R, Karki P, Copenhaver M (2016). Early Sexual Debut: A Risk Factor for STIs/HIV Acquisition Among a Nationally Representative Sample of Adults in Nepal. Journal of Community Health 41(1):70-77. |
|
|
Son DT, Oh J, Heo J, Huy N, Van Minh H Van, Choi S, Hoat LN (2016). Early sexual initiation and multiple sexual partners among Vietnamese women: analysis from the Multiple Indicator Cluster Survey, 2011. Global Health Action 9(1):29575. |
|
|
Stöckl H, Kalra N, Jacobi J, Watts C (2013). Is Early Sexual Debut a Risk Factor for HIV Infection Among Women in Sub-Saharan Africa? A Systematic Review. American Journal of Reproductive Immunology 69(s1):27-40. |
|
|
Tapert SF, Aarons GA, Sedlar GR, Brown SA (2001). Adolescent substance use and sexual risk-taking behavior. Journal of Adolescent Health 28(3):181-189. |
|
|
Tolera FH, Eshetu G, Abebe M, Zalalem KB (2019). Risky sexual behaviors and associated factors among high and preparatory school youth, East Wollega, Ethiopia, 2017: A cross-sectional study design. Journal of Public Health and Epidemiology 11(1):1-12. |
|
|
Tolou-Shams M, Ewing SWF, Tarantino N, Brown LK (2010). Crack and cocaine use among adolescents in psychiatric treatment: associations with HIV risk. Journal of Child and Adolescent Substance Abuse 19(2):122-134. |
|
|
Tucker JS, Ryan GW, Golinelli D, Ewing B, Wenzel SL, Kennedy DP, Zhou A (2012). Substance use and other risk factors for unprotected sex: Results from an event-based study of homeless youth. AIDS and Behavior 16(6):1699-1707. |
|
|
Vasilenko SA, Lanza ST (2014). Predictors of multiple sexual partners from adolescence through young adulthood. Journal of Adolescent Health 55(4):491-497. |
|
|
Wang T, Lurie M, Govindasamy D, Mathews C (2018). The Effects of School-Based Condom Availability Programs (CAPs) on Condom Acquisition, Use and Sexual Behavior: A Systematic Review. AIDS and Behavior 22(1):308-320. |
|
|
Yaya S, Bishwajit G (2018). Age at First Sexual Intercourse and Multiple Sexual Partnerships among Women in Nigeria: A Cross-Sectional Analysis. Frontiers in Medicine. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


