Full Length Research Paper

ABSTRACT
Globally, palliative care is an urgent humanitarian need for patients with cancer and other chronic disease. Currently, it is estimated that only one in ten people who need palliative care receive it. Therefore, this study is aimed to identify barriers preventing people from using the service. Institutional based qualitative case study was conducted among twenty- seven purposively selected health care providers. Two focus group discussions and fifteen individual interviewed were conducted from 1st April to 3oth June 2017. Ethical clearance was obtained from the university ethical review board. Atlas ti 7 was used to assist deductive analysis. A total of 27 health care providers from two public hospitals and one local nongovernmental organization were included in this study; fourteen of them were health professionals and thirteen were peer educators; of which 20 (74.07%) were females and 7(25.93%) were males. Unavailability of drug, un-conducive working environment, patient-related problems and lack of recourse are identified as barrier to provide palliative care. Numerous barriers exist on the healthcare providers’ side, for the provision of palliative care for patients with chronic disease. Additional research is required to explore barriers in a patient side.
Key words: Palliative care, Jimma, barriers, health care providers, peer educators, qualitative.
Abbreviation: ACS, American Cancer Society; AIDS, Acquired Immuno Deficiency Syndrome; ART, Anti Retro viral Therapy; BSC, Bachelor of Science; FGD, Focus Group Discussion; HIV, Human Immuno Deficiency Virus; HRW, Human rights watch; IDI, In depth Interview; MSC, Master of Science; NCD, Non-communicable Disease; OSSHD, Organization for Social Service Health and Development; RA, Research Assistant; WHO, World Health Organization.
INTRODUCTION
Palliative care is an organized care which is provided to patients and their families going through a progressive, chronic, life threatening disease to relieve the symptoms of the disease by incorporating psychosocial and spiritual care, and it is essential to the management of all patients with non-communicable, communicable diseases, injuries and trauma (Meier, 2014; Steedman et al., 2014).
Globally, palliative care is an urgent humanitarian need for patients with cancer and other chronic disease and is required in countries where a high proportion of patients in advanced stages of disease and little chance of cure (Elshamy, 2015). The global burden of cancer is expected to grow to 21.6 million new cancer cases by 2030, and from this, 13 million cancer deaths is due to the growth and aging of the population (American Cancer Society (ACS), 2018). Worldwide, non-communicable disease is responsible for 71% (41 million) of the 57 million deaths; similarly, in Ethiopia, 39% of deaths are dueto non-communicable disease (Global Health Estimates, 2016; WHO, 2018). An overall prevalence of chronic disease in Jimma town was 8.9% (Martin, 2012). High rates of death and disease, particularly in developing countries, are a reflection of insufficient NCD premature death minimizing interventions (WHO, 2014).
Currently in Sub Saharan Africa, palliative care provision remains inadequate and available to less than 5% (Eve, 2013). It is estimated that one in 10 people who need palliative care are currently receiving it; and only 2% of terminally ill patients having access to opioids to manage pain and 80% of the global need for palliative care is in low- and middle- income countries (Human Right Watch, 2011; WPCA, 2014). As ageing population increases, it results in living longer with more comorbidities, which obligates the health systems to focus on palliative care service in order to improve quality of life and decrease the negative impacts in the last days of life the patient (Morin, 2017). Several studies in different country showed that palliative care programs could improve patient outcomes, including symptom control and quality of life and caregiver outcomes, such as reduced stress and dysfunctional grief (Pippa, 2017; El-Jawahri, 2017; Kelly, 2018). Despite its effectiveness and strong recommendations for broad application, palliative care remains underutilized and only a small proportion of patient are getting the services so, the aim of this study is to explore the barriers preventing from using the service.
MATERIALS AND METHODS
Study area
The study was conducted in Jimma town, which is one of the towns in the Oromiya region located 352 km from Addis Ababa (the capital city). Currently, three health care settings, namely Jimma university medical center, Shenen Gibe hospital and Organization for social service health and development provide palliative care collaboratively by the health professionals and peer educators in the town.
Study design and period
Institutional based qualitative case study design was employed from 1st April to 30th June 2017.
Sampling technique and participant selection procedures
A criterion-based purposive sampling was used. Any health care providers who had experience in caring for patients with chronic life-threatening disease were selected as a study participant. For in-depth interview, health professionals and four focused group discussions peer groups were selected. Health care providers assisted participant selection.
Data collection procedure and tools
Data were collected by the principal investigator and assisted by two research assistant (RA) having BSC degree and MSC degree and experience in qualitative research data collection after taking one day training by using semi-structured interview guides containing open-ended questions after commented by an expert. Fifteen in-depth face to face interview, two focused group discussion was conducted, and probing question was used. Voice recorders and field-notes were used to capture the information.
Data analysis
The data were analyzed with thematic analysis, using both an inductive and deductive coding approach. All data were transcribed verbatim and translated into English by the Principal investigator and RA. The transcripts were read and reread to gain familiarity with the data and were checked against the recordings to confirm or correct any errors and exported directly into Atlas.ti7.1. The process was supported by the analytic memoing during the coding phases. Category and subcategories are developed into themes for each participant and across different participant. Forty primary codes are identified and then the codes are examined for similarities and merged. Finally, it was expressed in four main categories.
Operational definition
Provision of palliative care - an institution that provide at least two components (physical care, social care, psychological care, spiritual care and practical care) of palliative care considered as they provide the services.
Trustworthiness
Respondents with different educational status and professional background were selected for the interview and discussion, regular debriefing meetings and review of data collection forms were held daily. Iterative questioning to get in-depth information, peer scrutiny of the research by colleagues, peers and academics and feedback from the presentation were welcomed. The interviews and discussion were transcribed into word, in the language of respondent by the principal investigator and research assistant then translated into English language for analysis. Member check was done. In addition, a narrative thick description was conducted. Qualitative research experts were consulted during data collection, analysis, and report writing. First interviews, then focused group discussions were conducted.
Ethical considerations
Ethical clearance and approval to conduct the research were obtained from the university institutional review board and cooperation letter is sent to respective health institution management. Anonymity was kept. All typed records were kept on password- protected computer and backup drive. All interviews and discussion were recorded after obtaining the participants’ permission. When the participants did not want the audios of the interview recorded, notes were taken and analyzed along with other data. Written consent was obtained from all participants after orientation.
FINDINGS
Participants’ characteristics
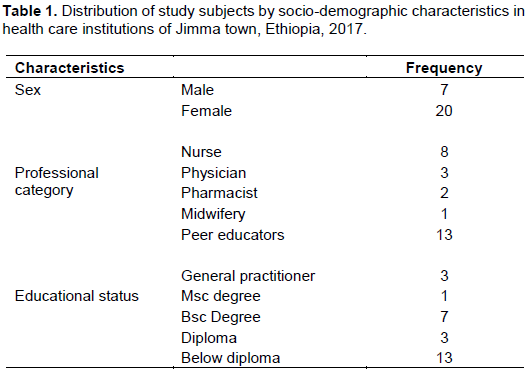
Twenty-seven health care providers from two public hospitals and one local nongovernmental organization; 14 (51.85%) of them are health professionals and 13 are peer educators (48.14%) participated in this study among those 20 (74.07%) were females and 7(25.93%) were males. Eleven (40.7%) of them has educational status above Bachelor of Science degree (Table 1).
Barriers to provide palliative care
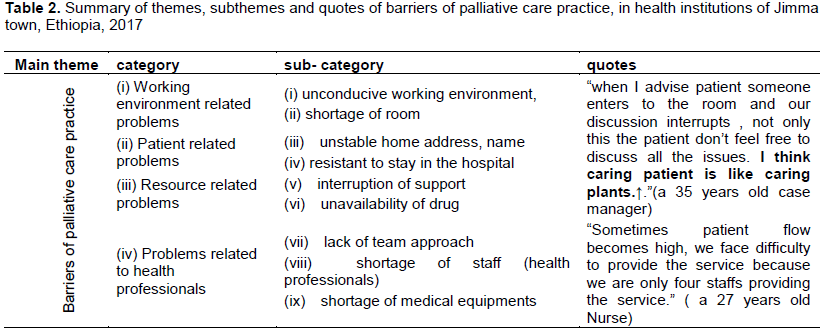
The result of this study indicated that the study participants have an awareness of palliative care and provide it by calling “comfort care”. The service is provided for HIV/AIDS positive and cancer patients in structured manner, but for other patients pain management has given due focus in all health institution. The result of this study identified the following barriers while provision of palliative care (Table 2).
Problems related with the working environment
Most participants mentioned that, the environment where the service provided should be comfortable as much as possible but, lack of privacy while providing the service exposes the patient to have an unnecessary effect on the disease prognosis. A 27 years old male Nurse interviewee said that “The room is not comfortable, better to stay in a corner, (...) privacy not kept for a patient, you are unable to discuss freely with them, and patient don’t feel free”.
Additionally, the participants mentioned that the importance of palliative care unit is to provide the service freely in order to have the desired outcome on patient life and also to discuss confidently with the patient to attain his need. A 35 years old female key informant said “When I advise patient someone enters the room and our discussion is interrupted because we don’t have a separate room for palliative care…the patient doesn’t feel free to discuss all the issues”.
However, few participants reported that even if there is no room for palliative care, the available area should be conducive for the patients to discuss freely and to provide the service, as well as the staff relationship should be friendly while providing palliative care. Regarding this, a 31-year-old female diploma nurse interviewee said that “The working environment is comfortable and the staffs are willing to share what they know”
Problems related to patient
FGD discussants mentioned that they have their own clients in the community; these clients already disclosed themselves and use the service but, some of the clients vanish after using the service. They search for those patients in collaboration with health extension workers; due to health extension workers busy schedule, they go to patients home alone. Even if they search the whole day, they do not get them, because patients conceal themselves by frequently changing their name and address due to fear of stigmatization and discrimination.
“When the patient defaults treatment we will find them in the community; since the patients change their name and address…You stay all day searching for her, but she is there, when you ask her, she says“ such kind of woman does not live here”.
While other discussant describe unwillingness of patients to use the service.
“Some patient throw stone on us, untie their dog, when we go to their homse”.
Several respondents described that the patient’s family are un-willing to initiate palliative care, by hoping for a miracle or consideration of treatments futile for the patient. Increased possibility of death combined with denial on the part of patient’s family serve as an important barrier to receive and initiate palliative care.
Regarding this 28 years old male general practitioner interviewee said that
“…. if they (the attendant) know the patient is diagnosed with chronic disease, they hesitate to initiate palliative care discussions and interventions.”
Unavailability of drug
As reported by health care providers, patients with life-limiting conditions frequently have multiple symptoms as a result access to pain medication is one component of palliative care but inaccessibility and unaffordable to the medication make it difficult to manage pain symptom.
A male oncology nurse interviewee said that “…there is financial problem… the drugs are expensive, some patients unable to pay…patients are suffering due to pain”.
A female oncology Nurse interviewee said that “… Last year we faced a challenge to manage pain… currently there is shortage of pain medication… due to diclofenac is contraindicated in children less than twelve year, … we provide morphine by decreasing the dose.”
A 32 years old male pharmacist interviewee supported the idea and said that “…currently morphine is a preferred drug for severe pain management, but for pediatrics, the suspension form is not currently available in our hospital.”
Resource related problems
Continuous support for the palliative care patients in material or in-kind has a temporarily means to resolve their illness, by decreasing psychological burden being economically weak.
As described by study participants, sometimes there is an interruption of material supports provided by the nongovernmental organization for patients who need palliative care.
A 34 years old male manager interviewee said that “When supports are interrupted, we face difficulty; actually everyone should be economically independent but little support is needed for those who are critically sick.”
The FGD discussants also mentioned the negative impact of economic support on the acceptance of care by the patients.
“Due to interruption of support provided by the organization, when we go to patients home, they (patient) say “why did you come without material support”.
Problem related to health care providers
According to the analysis, most participants mentioned that all health care providers are responsible to provide palliative care and the essentiality different discipline in
solving different problems of the patient and to appeal for a better solution.
A 30 years old male general practitioner interviewee said that “Sometimes things become very complicated, (...)when the patient caught by chronic disease, it is related with almost all system so, I have to discuss with other medical staffs to provide medical service.”
Similarly a 26 years old male pharmacist interviewee said that “…Every health service is provided in a team if
one of the team member is missing, the service would not be adequate."
Even the participants agree on the essentiality of multidisciplinary/team approach in the provision of palliative care, but absence of bringing diverse disciplinary points of view together while providing palliative care service challenged them to provide the service.
A 27 years old male Bsc nurse interviewee said that “During training, we thought palliative care is provided in a team but it is practically different; the physician order
medication and leaves the patient (...) comes and asses again (..) Writes order and go.”
The participants also described disproportion between patients to health care provider ratio while providing palliative care for the patient as a challenge.
Regarding this a 48 years old key informant said that “Sometimes patient flow increases, during that time (...) we cannot provide the palliative care for patients, because of shortage of health professionals.”
DISCUSSION
Palliative care has been on for about a decade. It is not yet known as routine care and this study focus mostly on outpatient department and very little on inpatient unit. Besides, staff shortage makes the service inaccessible. This finding similar with that of a study done in five European country (Jasper van, 2014). This leads to decrease in the quality of life of the patient (Ernst, 2014).
One of the important aspects of palliative care is the availability and possibility of utilizing medical resources and financial support. In this study, social support is provided by the nongovernmental organization and the eligible patient is determined by the health professionals and referred to. However, most of the patients do not get the support timely, as a result, they are severely ill and go to missionaries; the missionaries help the patients for a while and let them go after offering immediate support. Since, the support is very limited, the patients suffer economically and discontinue the medication and finally, they either die or go to second-line drugs, which are very expensive, and with many side effects. This finding is similar with a study done in United Kingdom (Clare, 2011).
In order to increase the quality of life and to decrease frustration due to fragmented and disjointed care for patients with life-limiting illness the service should have continuity. This is associated with the option of further home care or/and collaboration with other units. In this study, service inaccessibility and interruption challenge people to use other services, this is in line with the study done in England (Nathan C. et al. 2014).
To have mutual trust between the patient and the healthcare providers, the service should be provided in both setting either by one health care institution or by having network with other organization who provide similar service in the community. In this study, palliative care is provided separately in both setting and the service are not as recommended by world health organization (Stjernsward J., 2007).
Effective pain control and health sectors capacity to use anti-pain drugs efficiently is the foundation of palliative care. It is best achieved through a holistic approach in-order to address psychological, social, spiritual and physical needs of a patient and their family. The result of this study indicated that problem related to prescription and supply of anti-pain drugs are identified as barrier in contrast with the finding of a qualitative study conducted in Canada, England, Germany, and United State.
This study and others have observed obstacles that health professionals perceive as preventing the provision of palliative care. The results of this study point out that work environment related problem and patient-related factors are significant and they encounter these when they perform their duty; which is similar with study conducted in United Kingdom (Clare G., et al. 2011).
Non-disclosure is an important public health problem that affects individuals’ access to treatment and care (Bezabhe WM., 2014). In this study, the peer educators mostly see this issue during palliative care provision in the community. Some of them provide palliative care only in the community, while others provide in both the community and healthcare institution; in both settings, interrelated obstacles were identified.
The hospital environment, which encompasses the physical surroundings and the social interactions with hospital staff, can impact on the quality of palliative care experienced by patients (Robinson J., et al. 2015). When the end of life makes its inevitable appearance, patients should be able to expect reliable, humane and effective care giving. In this study, unconducive working environment and lack of palliative care unit are identified as a barrier, which have an impact on quality of life of the patient.
CONCLUSIONS
Various barriers exist in the provision of palliative care, which has a negative impact on quality of life of the patients, resulting from healthcare providers’ side. Additional research is required to explore barriers arising from patients’ side.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The research was funded by the Ministry of Education, in collaboration with Wolaita Sodo University.
REFERENCES
|
American Cancer Society (ACS) (2018). Global cancer facts and figure. |
|
|
Bezabhe WM, Chalmers L, Bereznicki LR, Peterson GM, Bimirew MA, Kassie DM (2014). Barriers and Facilitators of Adherence to Antiretroviral Drug Therapy and Retention in Care among adult HIV-Positive Patients A Qualitative Study from Ethiopia. PLoS ONE 9(5):e97353. |
|
|
Clare G, Cobb M, Gott M, Ingleton C (2011). Barriers to providing palliative care for older people in acute hospitals. Age and Ageing 40:233-8. |
|
|
El-Jawahri A, Temel JS, Greer JA, Pirl WF, Park ER, Jackson VA Rinaldi SP (2017). Effects of Early Integrated Palliative Care on Caregivers of Patients with Lung and Gastrointestinal Cancer: A Randomized Clinical Trial 22(12):1528-1534. |
|
|
Elshamy K ((2015). Current Status of Palliative Care Nursing in Egypt: Clinical Implementation, Education and Research. Journal of Palliative Care and Medicine S5:005. |
|
|
Ernst KF, Hall DE, Schmid KK, Seever G, Lavedan P, Lynch TG, Johanning JM (2014). Surgical Palliative Care Consultations Over Time in relation to System wide Frailty Screening. JAMA surgery 149 (11):1121-1126. |
|
|
Eve N, Powell RA, Kariuki H, Harding R, Luyirika E, Mangi-Powell F (2013). Palliative care research in eastern Africa. European Journal of Palliative Care 20(6):300-304. |
|
|
Global Health Estimates (2016). Deaths by Cause, Age, Sex, by Country and by Region, 2000-2016. Geneva: World Health Organization. |
|
|
Human rights watch (HRW) (2011). Global State of Pain Treatment: Access to Palliative Care as a Human Right. Human rights watch. |
|
|
Jasper van RP, Vernooij-Dassen M, Brouwer F, Meiland F, Iliffe S, Davies N, Vissers K (2014). Improving the organization of palliative care: identification of barriers and facilitators in five European countries. BMC 16(10):9. |
|
|
Kelly B (2018). Early palliative care provides important benefits for family care givers of patients with cancer [news release]. Alexandria, VA: American Society of Clinical Oncology 2016. Accessed 24 November 2018 |
|
|
Martin P (2012). Chronic non-communicable diseases in Ethiopia-a hidden burden. Ethiopian journal of health sciences 22(Spec Iss):1-2. |
|
|
Meier DE (2014). Palliative Care Facts and Stats: Palliative Care Frequently Asked Questions. New York City: Center to Advance Palliative Care. |
|
|
Morin L, Aubry R, Frova L, MacLeod R, Wilson DM, Loucka M, Teno J (2017). Estimating the need for palliative care at the population level: a cross-national study in 12 countries. Palliative medicine 31(6):526-536. |
|
|
Nathan D, Maio L, Vedavanam K, Manthorpe J, Vernooij DM, Iliffe S, IMPACT Research Team (2014). Barriers to the provision of highâ€quality palliative care for people with dementia in E ngland: a qualitative study of professionals' experiences. Health and social care in the community 22(4):386-394. |
|
|
Pippa H (2017). Barriers to Access to Palliative care Pain and Symptom Management/Palliative Care Program SAGE Palliative Care: Research and Treatment review paper pp. 1-6. |
|
|
Robinson J, Gott M, Gardiner C, Ingleton C (2015). The impact of the environment on patient experiences of hospital admissions in palliative care. BMJ supportive and palliative care, bmjspcare-2015. |
|
|
Steedman MR, Hughes-Hallett T, Knaul FM, Knuth A, Shamieh O, Darzi A (2014). Innovation can improve and expand aspects of end-of-life care in low-and middle-income countries. Health Affairs 33(9):1612-1619. |
|
|
Stjernsward J (2007). Palliative care: the public health strategy. Journal of public health policy 28(1):42-55. |
|
|
World Health Organization (WHO) (2014). Global status Report on Noncommunicable Diseases Attaining the Nine Global Noncommunicable Diseases Targets; A Shared Responsibility. |
|
|
World Health Organization (WHO) (2018). World health organization, Non communicable disease(NCD) country profiles. |
|
|
Worldwide Palliative Care Alliance (WPCA) (2014). WHO Global Atlas of Palliative Care at the End of Life. World Health Organization. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


