ABSTRACT
The current study has been undertaken by studying the data from the hospital registers at the Kasugu District Hospital, Malawi. The malaria cases of 2014 were chosen for the study. They typically represent disease distribution based on the ages and genders of the patients. The data suggest that the cure rates among patients under age 5 and above do not have any significant difference, contrary to the commonly anticipated outcome that the older children should have better developed immune systems and should have higher cure rates. A notable point is there are huge dichotomies between genders in terms of the reported registered cases, the cure and mortality rates. The gender differentiation in the reporting and management of malaria is understood under the contemporary socio-cultural beliefs and economic realities of the Malawian society. This analysis has been carried out from a qualitative perspective, but with an attempt to identify a pattern from a year's length of statistical data.
Key words: Malaria epidemiology, malaria cases, mortality, case fatality rates.
There have been a number of epidemiological studies on the prevalence of tropical diseases in sub-Saharan Africa (Carneiro et al., 2010; Fenwick et al., 2009; Cairns et al., 2015; Ceesay et al., 2015; Hotez and , Kamath 2009; et
Talisuna al., 2015). There seems to be a universal agreement that much of medical maladies can be attributed to socio economic realities and the inevitable domino effects. Among all, malaria as a disease that poses a pre-eminent danger to the world population with mortality rate at 42% globally since 2000 and 49% in the African region (World Malaria Report 2013). Malawi has been consistently regarded as one of the most prone to the wide scale prevalence of malaria perhaps only after Congo, Nigeria and Uganda. While it is obviously possible to attribute this to the poor economic state of the country because insufficient funding can stifle the preventive measure programs, geographical factors such as climate and topography cannot be discounted or overlooked.
The current study has been undertaken by a group of students from various US universities and high schools who joined together under the auspices of the Science, Technology, Engineering, Mathematics Research Institute (STEMRI) Fairfax, Virginia, USA and worked in collaboration with the authorities at Kasungu District Hospital (KDH), Malawi. By this, the hospital data were made available for analysis in order to understand and recognize any patterns in the incidence of diseases in this district as a geographical sample of the country.
Malawi is a land locked country bounded by Mozambique, Zambia, and Tanzania. Lake Malawi, formerly known as Lake Nyasa, is a part of the country's eastern border and is a major water body. Kasungu District Hospital (KDH), where this study was conducted, is a public hospital in Kasungu, a town in the central region of Malawi.
A number of studies of malaria under the patronage of World Health Organization (WHO) have been undertaken e.g. in the aspects of the current world burden, control and epidemiology (Bell et al., 2005; Socrates, 2015; Olliaro et al., 2011). There are enormous literature resources to understand the clinical, socio-economic and political aspects of this disease. These studies, though valuable, in informing the scholars and general public and even in influencing global policies towards the manage-ment of diseases, are still far from being controversial. There are reports claiming tendencies by various agencies, mostly government, to artificially inflate or underplay the statistical figures for other vested motives (Rothmyer, 2011).
This is unfortunate and therefore can, in some cases, cast suspicious statistical data that cannot be taken on their face value, though a perception on the general trend can still be accomplished. In order to have a hands-on approach to handle the most authentic figures right from the hospital registers, this study has been undertaken so that an analysis can be presented.
Thus, this study was focused on the registered cases of malaria in a representative year (2014) in KDH, Malawi. The year of focus- 2014 for this study has been selected because it is the most recent during the “study period” for which data are available. It should be borne in mind that the year is not special in respect of any event-climatic or geopolitical.
Therefore, it can be safely regarded as an average representative year for the report of diseases and treatments in the hospital.
The objective is to make cognizance of any pattern that can be detected in the data so that there can be related to various factors- socioeconomics, gender mindsets, local belief systems.
The hospital patients' records were made available for this study. Thus, the patients’ distribution for malaria in respect of genders, age groups, treatment outcomes and times of the year were collected and arranged. The data collection and analysis focused on the most recent available in complete form, that is the year 2014.
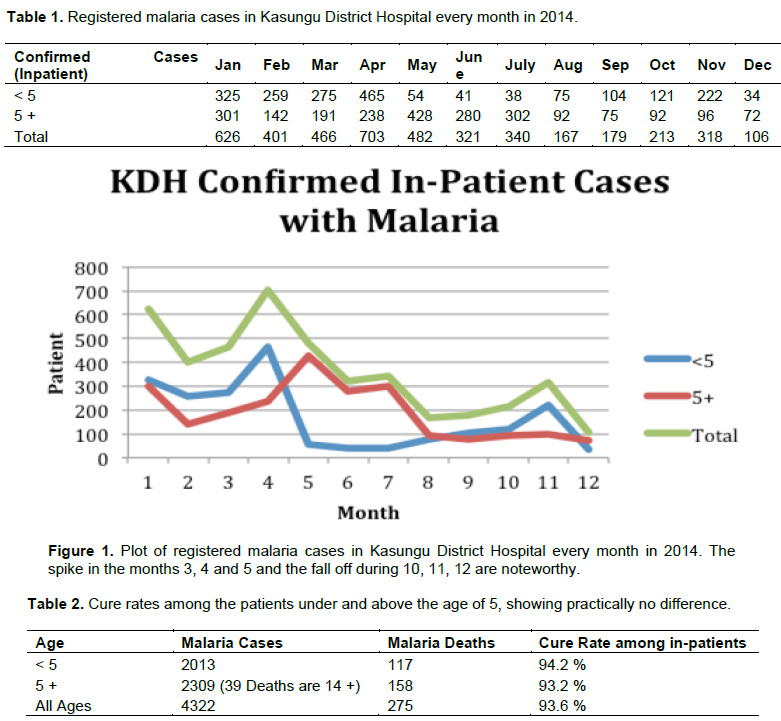
In 2014, a total number of 4322 malaria cases were registered as hospital in-patients comprising 2013 patients under the age of 5 and 2309 patients above 5. These cases have been registered on a monthly basis as presented in Table 1.
It is clear that there is a spike in registered cases during the months of March, April and May (Figure 1). This trend is noticed in the other years too (not shown here as it is outside the scope of this paper). Out of these cases, the reported mortality was 117 for under age 5 and 158 for over 5, accounting for 94.2 and 93.2% cure rates, as shown in Table 2.
It appears that the difference in the cure rates between both the under 5 and above 5 age groups is miniscule, indicating that lower immunity under the age 5 has very little bearing on the overall curability figures. This data is different from many findings in the literature where more than 75% mortality share is on the under 5 age group.
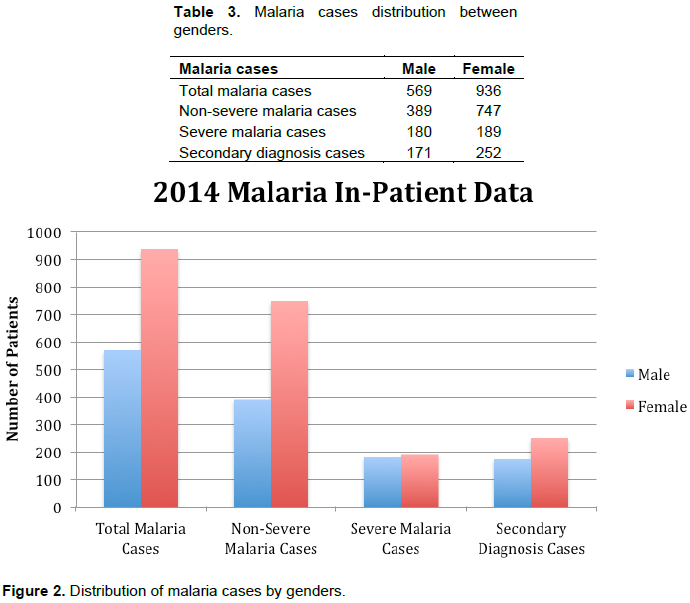
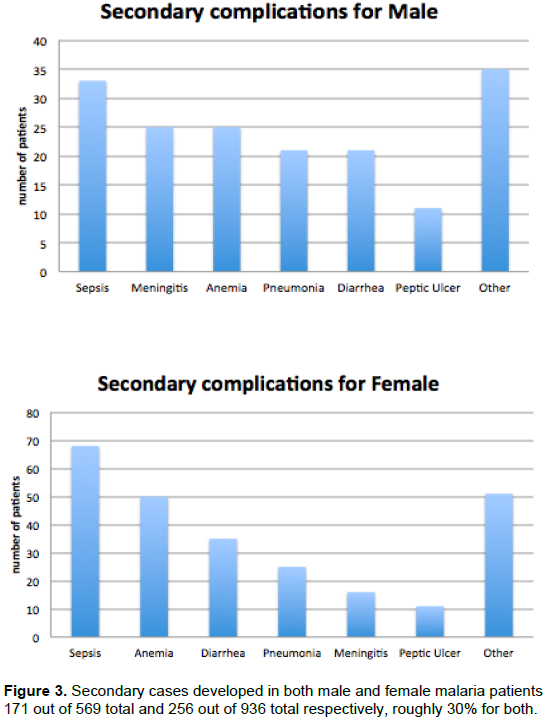
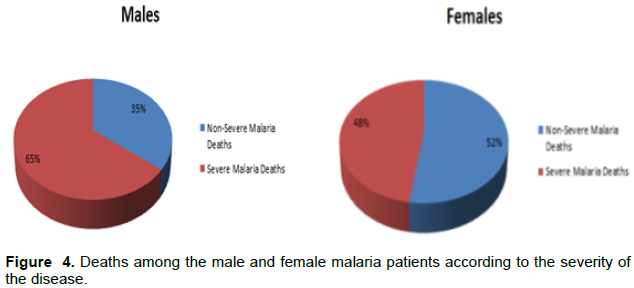
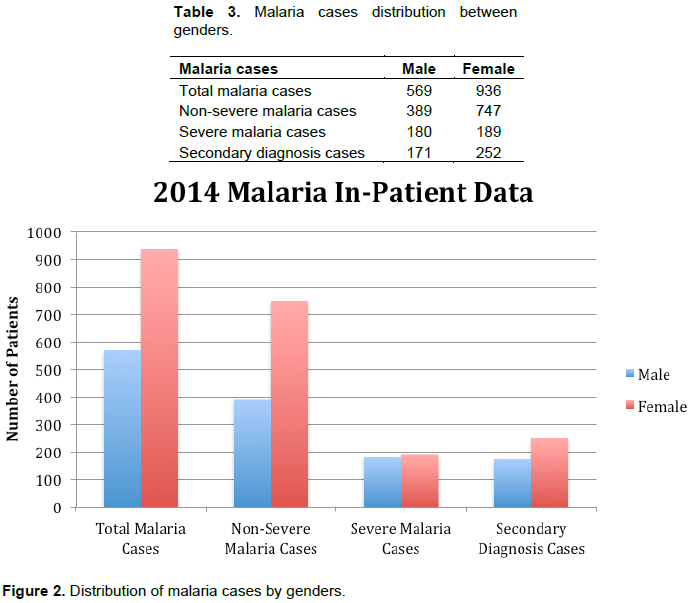
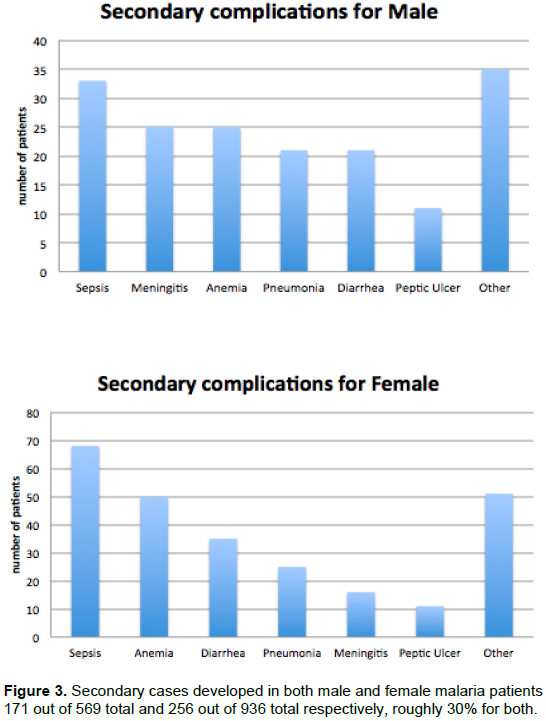
However, in the age group above 14, there are some perceptible differences between the genders (Table 3). In 2014, there were 569 males and 936 females. Among the males, 389 were afflicted with non-severe malaria and the rest 171 were severe cases. Among the females, 747 accounted for the non-severe and 189 as severe cases. It is clear from Figure 2 that in spite of a significantly smaller number of registered cases for the males, the numbers of severe cases for both genders are roughly the same. One obvious inference is that there is a tendency by the male patients to register as in-patients when the affliction has degenerated to an advanced stage. It was also noted that both male and female patients were affected with secondary complications, as noted in Figure 3. As expected, anemia as secondary complication had a more visible presence in females than in males, diarrhea, peptic ulcer, meningitis and pneumonia being other associated complications. As for the mortality rates among the males and females, a significant difference exists. Whereas death occurred in 65% of the severe malaria male cases among males, it was 48% in female (Figure 4).
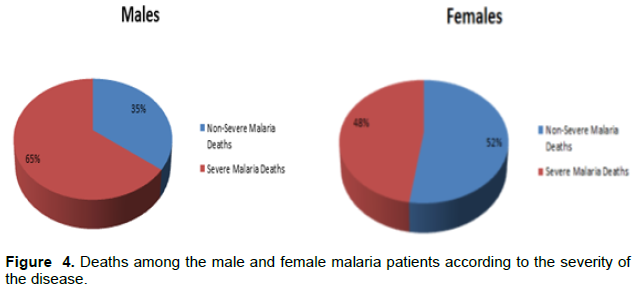
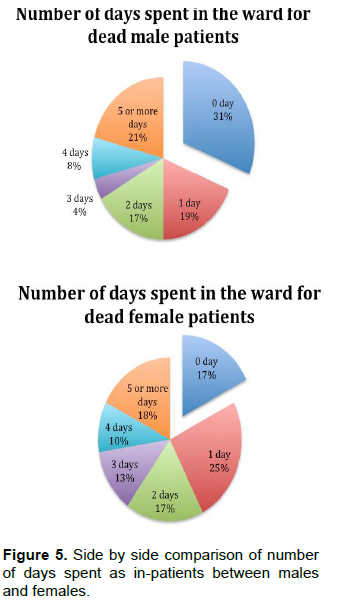
This signifies that the severe cases in males were more acute than in case of females. There was also a noteworthy difference between the in-patient residence times for male and female patients as shown in Figure 5. 17% of the male patients and 31% females registered as in-patients were discharged on the same day of admission. Also, 25% of the females spent an average of one day whereas only 19% males did so. The residence time beyond 1 day did not show much difference between males and females. It appears that the tendency of the male to need a hospital care requiring an average of one day is low either due to psychological or economic factors or both.
In general, men report to the hospital when the case assumes a severity when it may prima facie require more than a day’s care.
The hospital record of KDH for malaria patients for 2014 as a representative year presents a very interesting case in the general perspective of disease occurrence and management. There are interesting features in respect of the number of malaria cases occurring in terms of age and gender distribution.
At the outset, the general rise in registered cases in the months of March, April and May (Figure 1) is consistent with the climatic conditions in the southern hemisphere where high heat and rain fall rate would aid the mosquito breeding resulting in malaria proneness. Transmission of the disease depends on climatic conditions that affect the number and survival of mosquitoes- rainfall, temperature and humidity. Therefore, it is conceivable that there is a considerable decrease in the dry months of October, November and a part of December.
Among the reported cases in terms of age, as shown in Table 2, the cure rates of patients under 5 and above 5 are almost identical at 94.2 and 93.2% respectively. This is an unusual exception from the general trend where the mortalities among the under 5 children is overwhelmingly large according to many reports (Ladeia-Andrade et al., 2009; Artavanis-Tsakonas et al., 2003; Nyirenda et al., 2015). Worldwide, usually the children under five are one of most vulnerable groups. This is also inconsistent with a focused study on Malawian children done by Dembo (2012). There were an estimated 584 000 malaria deaths around the world in 2013, of which approximately 78% were in children under five years of age.
In high transmission areas, only partial immunity to the disease is acquired during childhood. In such settings, the majority of malarial disease, and particularly severe disease with rapid progression to death, occurs in young children without acquired immunity. Severe anemia, hypoglycemia and cerebral malaria are features of severe malaria more commonly seen in children than in adults. In the hospital data, this observation, however, is not supported. Though this may require a more comprehensive multi-year data analysis, this may also have some connotation with the child’s welfare and malaria prevention program that Malawi and the Kasungu District administration have implemented. Programs such as universal distribution of insecticide treated mosquito nets, community case management of childhood illnesses including malaria as well as improvements in case management and improvements in early diagnosis have borne out results. Also, most current strategies for interventions often target children under five years of age, making the efficacy of the programs more visible and perhaps shifting the vulnerabilities to an older age group in a statistical sense. This has been supported by a simulation study done by a research group in Swiss Tropical and Public Health Institute (Pemberton-Ross et al., 2015).
The most noteworthy of the statistics is in the gender gap that exists in the reporting and management of the disease. As seen in Figure 2 and Table 2, the female patients far outnumber the male-936 against 569. However, the number of severe malaria cases among the male and female are essentially same at 180 and 189 for male and female respectively. This implies that the percentage of male patients afflicted with a severity of the disease is much higher which may also imply that the males have a tendency to report as registered in-patients only at a later stage of severity. This is a social trend that is in keeping with the general ethos where males are regarded as the fenders for the families who would be procrastinate being registered as in-patients since it would keep them away from homes, as it potentially would jeopardize the family’s economic structure. This is an interesting finding and it would be curious to explore a trend in the general socio-economic divide across African nations and even globally. Whereas the reluctance in male patients to register as in-patients arises from genuine economic concerns, there are also reports of cultural stubbornness routed in a certain degree of superstition. One such practice is that even if there is a provision of distributing mosquito nets, the male members in many cases desist from using them because of a conjectured fear that this practice reduces male virility. This fear may not necessarily arise from superstition, but rather deep distrust that exists in certain pockets on the Government preventive programs where the public fear that the Government has other motivations in stealth mode.
The case study for malaria at KDH for the year 2014 is being treated as a typical representative study with no extraneous factors in terms of climatic or political event prejudicing the results. Moreover, this analysis has been made by resorting to the data straight from the hospital register. It is conceivable that the general rise in education and economic level in this largely agrarian and rural population will also amend many social and cultural habits that will contribute towards the total eradication of this serious disease. However, it will be hard to extra-polate a prediction by analyzing some trends in few years’ data. Yet, this study is an important addition to the literature of data and figures that establish a trend as to how the disease is being managed at present.
CONCLUSION AND RECOMMENDATION
The data analyzed under this study is a snap shot in time albeit of a year’s length. Thus, it is sufficient data to notice a general trend in respect of gender and age distribution. The little difference in the cure and mortality rates between age groups under and above 5 is particularly noteworthy. The differences in the registrations and treatment outcome between genders are also highly noticeable which are attributed to the reasons of socioeconomics and traditions.
However, it is recommended that a larger multi-year data analysis needs to be undertaken to validate or nullify the aforementioned conclusions, because such a study will bear greater statistical significance.
The authors have not declared any conflict of interests.
The authors acknowledge the STEM Research Institute for the institutional grant (SRI-06-2015) that permitted this medical project and the cooperation of the authorities of Kasungu District Hospital that allowed access to the Hospital registration data.
REFERENCES
|
Artavanis-Tsakonas K, Tongren JE, Riley EM (2003). The war between the malaria parasite and the immune system: immunity, immunoregulation and immunopathology. Clin. Exp. Immunol. 133:145-152.
Crossref
|
|
|
|
Bell DR, Jorgensen P, Christophel EM, Palmer KL (2005). Malaria risk: Estimation of the malaria burden. Nature (London, United Kingdom) 437(7056):E3-E4.
Crossref
|
|
|
|
|
Cairns ME, Milligan PJ, Walker PG T, Okell LC, Griffin JT, Garske T, Ghani AC, Asante KP, Owusu-Agyei S, Diallo D, Cisse B, Greenwood BM, Chandramohan D, Diallo D, Dicko A, Cisse B (2015). Seasonality in malaria transmission: implications for case-management with long-acting artemisinin combination therapy in sub-Saharan Africa. Malar. J. 14(1):321
Crossref
|
|
|
|
|
Carneiro I, Roca-Feltrer A, Griffin JT, Smith L, Tanner M, Schellenberg JA, Greenwood B, Schellenberg D (2010). Age-patterns of malaria vary with severity, transmission intensity and seasonality in sub-Saharan Africa: a systematic review and pooled analysis. PLoS One 5(2).
Crossref
|
|
|
|
|
Ceesay SJ, Koivogui L, Nahum A, Taal MA, Okebe J, Affara M; Kaman LE, Bohissou F; Agbowai C, Tolno BG, Amambua-Ngwa A, Bangoura NF, Ahounou D, Muhammad AK, Duparc S, Hamed K, Ubben D, Bojang K, Achan J, D'Alessandro U (2015). Malaria Prevalence among Young Infants in Different Transmission Settings, Africa. Emerg. Infect. Dis. 21(7):114-1121.
Crossref
|
|
|
|
|
Dembo E (2012). Community health workers' perceptions of barriers to utilisation of malaria interventions in Lilongwe, Malawi: A qualitative study. Malar. World J. 3:11.
|
|
|
|
|
Fenwick A, Zhang Y, Stoever K (2009). Control of the Neglected Tropical Diseases in sub-Saharan Africa: the unmet needs. Int. Health 1(1):61-70.
Crossref
|
|
|
|
|
Hotez PJ, Kamath A (2009). Neglected tropical diseases in sub-saharan Africa: review of their prevalence, distribution, and disease burden. PLoS one 3(8):e412.
Crossref
|
|
|
|
|
Ladeia-Andrade S, Ferreira, MU, de Carvalho ME, Curado I, Coura JR (2009). Age-Dependent Acquisition of Protective Immunity to Malaria in Riverine Populations of the Amazon Basin of Brazil. The Am. Soc. Trop. Med. Hyg. 80(3):452-459.
|
|
|
|
|
Nyirenda TS, Molyneux ME, Kenefeck R, Walker LSK, MacLennan CA, Heyderman RS, Mandal WL (2015). T-Regulatory Cells and Inflammatory and Inhibitory Cytokines in Malawian Children Residing in an Area of High and an Area of Low Malaria Transmission During Acute Uncomplicated Malaria and in Convalescence. J. Pediatr. Infect. Dis. Soc. 4(3):232-241.
Crossref
|
|
|
|
|
Olliaro P, Djimde A, Dorsey G, Karema C, Martensson A, Ndiaye JL, Sirima SB, Vaillant M, Zwang J (2011). Hematologic parameters in pediatric uncomplicated Plasmodium falciparum malaria in sub-Saharan Africa. The Am. J. Trop. Med. Hyg. 85(4):619-25.
Crossref
|
|
|
|
|
Pemberton-Ross P, Smith TA, Hode EM, Kay K, Penny MA (2015). Age-shifting in malaria incidence as a result of induced immunological deficit: a simulation study. Malar. J. 14:287.
Crossref
|
|
|
|
|
Rothmyer K (2011). Hiding the Real Africa. Columbia Journalism Review. Available at:
View
|
|
|
|
|
Socrates L (2015). Re-imagining the control of malaria in tropical Africa during the early years of the World Health Organization. Malar. J. 14:178.
Crossref
|
|
|
|
|
Talisuna AO, Noor AM, Okui AP, Snow RW (2015). The past, present and future use of epidemiological intelligence to plan malaria vector control and parasite prevention in Uganda. Malar. J. 14:158.
Crossref
|
|
|
|
|
World Health Organization (2013). Fact-Sheet on the World Malaria Report. Available at:
View.
|
|