Full Length Research Paper

ABSTRACT
On July 5, 2016, Amibera District Health office was alerted of excess of malaria cases in two villages. Within July 5 to 17, 2016 malaria outbreak and associations factors were investigated. A malaria case is when a person with fever or fever with headache is confirmed either microscopically to have Plasmodium parasites or by Rapid Diagnostic Test (RDT) to detect the malaria antigens. In the last five years malaria data were reviewed from 2011 to 2015 at the district level. Cases were identified by using line list and house to house active case search was done on a daily basis. Unmatched case-control study was conducted in 1:1 ratio conveniently selected cases (117) and community controls (117). The control was the neighbor of those who have not developed symptoms of malaria in the last three months. Data were collected through a structured interview administered questionnaire, entered into Epi-info version7 and analyzed using SPSS version 20. A total of 415 confirmed malaria cases with no death was identified. The predominant species was Plasmodium Falciparum accounting for 95.5%. The median age was 27 years (ranges 2- 63 years). The highest age specific attack rate was above 15 years (63.7/1000 populations). Poor insecticide treated bed net utilization, absence of indoor residual spray, sleeping outside of their homes at nights and presence of stagnant water were factors associated with the disease contraction. In this study the current malaria outbreak was higher in magnitude than that of three years ago.
Key words: Amibera, malaria, outbreak, Plasmodium Falciparum.
INTRODUCTION
In Ethiopia, malaria transmission is generally seasonal and highly unstable because of the variations in topography, climate and rainfall patterns (Daddi and Abebe, 2012).Hence, large scale outbreak frequently occurs particularly in epidemic prone areas of the country. Generally outbreak occurs in places where there is low and unstable malaria transmission, and where people have low or no immunity(Daddi and Abebe, 2012; Policy, 2013).
Other triggering factors like unusual local weather phenomena and activities resulting in environmental modifications that increase vector population increase vulnerability of population to famine and malnutrition, and interruptions of anti-malarial measures which have kept malaria under control. However, there could be outbreak in high transmission areas if there is deterioration of health system, interruption of anti-malarial measures or migration of non-immune individuals (WHO, 2015; World Health Assembly, 2016).
Many localized but severe outbreaks of malaria occurred in Amhara and SNNP Regional States, leading to widespread epidemic malaria in highland and highland fringe areas (up to 2,500 m) in 2003 (Gemechu et al., 2015; Hurissa, 2015). Conventionally, in areas of high-endemicity, prevalence of malaria infection is known to peak at an early age with an increase up to the age of 5 years; followed by a sharp fall in age groups of 10-15 years and continuing on a slow decline with increasing age (Kevin and Baird, 2010; World Health Assembly, 2016).
Afar’s geography and climate influence (seasonal) outbreaks of malaria epidemics. Peculiarities of this region (lowlands and seasonal heavy rainfall) lead to a high prevalence of mosquito breeding sites. The Afar Region is characterized by the lowland areas (≤1500 m altitude) with hot or warm climate. Malaria transmission in the region is generally seasonal and highly unstable due to variations in topography and rainfall patterns. Malaria transmission in the region is perennial due to the availability of large perennial river bodies and hot climate favoring the transmission throughout the year, with seasonal peak extending from August to December (AMREF, 2011; Daddi and Abebe, 2012).
The region is also prone to natural disasters such as droughts and floods and these have in the past contributed to increased malaria transmission, particularly along the banks of Awash River. Since the last decade, flooding of Awash River is on the increase, creating ideal conditions for vector breeding (AMREF, 2011). Plasmodium Falciparum (about 65%) and Plasmodium vivax (about 35%) are the two dominant malaria parasites prevailing in the region (Alemu, 2015; WHO, 2015)
There was a normal trend of malaria cases in Amibera District during the last five years. On the last week of June/2016 Werer health center of Amibera district reported an unusual increased number of malaria cases from Werer and Badhamo village. The aim of this investigation was to identify risk factors associated with this outbreak. The study ained to describe the magnitude of morbidity and mortality due to malaria outbreak and investigate factors associated with an occurrence of malaria outbreak in Amibera, Ethiopia, 5-17 July/2016.
MATERIALS AND METHODS
The malaria outbreak investigation was conducted in Werer and Badhamo village of Amibera district from July 5 to 17th/2016. Amibera is bordered on the south by Awash Fentale, on the west by the Awash River which separates it from Dulecha to the southwest then on the northwest by the Administrative Zone 5, on the north by Buromodaytu district, and on the east by the Oromia Region. The mean monthly temperature of the district was between 19 and 34°C, implying tropical temperature condition. The mean annual rainfall of the district is about 560 mm (AMREF, 2011).
Malaria was defined and identified as acute febrile illness with blood smear positive for malaria in Amibera district during this outbreak. We reviewed the previous five years (2011-2015) data of malaria from Amibera district health office and health facility to set epidemic threshold level and compare with similar week of this year (2016). The number of malaria cases was collected from health facilities on daily and weekly basis. Magnitude of outbreak was described by person, place and time. Slide positivity rate was calculated as those positive for malaria among total examined. Attack rates were calculated by person and place. An epidemic curve was constructed.
During analytical epidemiology, an un-matched case-control study was conducted to identify risk factors associated with malaria outbreak. A community control was selected for recently (not more than two weeks before interview) confirmed malaria case patients in 1:1 ratio basis. Controls were defined as having no malaria signs and symptoms for the last three months. A standard checklist was used to assess risk factors, including sleeping and staying area during the night, use of insecticide bed net, indoor residual spray, and presence of stagnant water or any other mosquito breeding area.
Regarding sampling method and sample size determination, the cases and control were recruited by convenience sampling method irrespective of the variables. Sample size determination was with a ratio of 1: 1 cases and control. The assumption taken from a previous study indicates that the proportion of controls exposed was 50% for a power of 80% with odds ratio (OR) of 2.2. The sample sizes which were conveniently taken from each group can be determined by the Epi-info version 7.2.1. Proposed sample size, therefore, 117 cases and 117 controls needed for the study was 234.
In the laboratory, laboratory technicians conducted thick and thin smears with a 100 × oil immersion microscopy at three health centers. Additionally, Rapid Diagnostic Test (RDT) was also used in this health center whenever they faced shortage of some reagents and during interruption of electric power. Health extension workers also used RDT to identify confirmed malaria cases at health post and community level during outbreak investigation case searching.
Data were collected in the presence of potential mosquito breeding sites. Selected case-patients and controls were interviewed about the presence of mosquito breeding sites in their compound and near home within 500 meters or less than it. In addition, availability of uncovered plastic water container, old tires and broken glasses in the home or outside the home were also critically assessed.
Quantitative data were collected using standardized face to face interviewer administered questionnaire that addressed socio-demographic characteristics, clinical manifestation, potential exposures, discussion with relevant bodies (task force), review of weekly integrated disease surveillance and response at different levels (District Health office and Health facilities), visiting of the affected village and interview of community members (patients) about knowledge of malaria transmission and control measure. Both RDT and Microscopic laboratory diagnoses were performed. Epi Info version 7.3.1 and SPSS version 20 were used to analyze the associated risk factors. The significance of risk factors for the outbreak was determined through bivariate and multivariate analysis by calculating Adjusted Odds Ratio and 95% Confidence Interval.
To ensure quality, the standardized questionnaire adopted was in English and translated into Afar local language, by experts. We reviewed and revised the questionnaire to ensure internal validity. We pre-tested it on 5% of the sample size. Data collectors and supervisors were trained for three days on the data collection tools and process of data collection. To ensure completeness, 5% of the collected data were checked and the investigators monitored the overall quality of data collection. We used line list for describing malaria cases in terms of time, place and person.
Case definitions
1. Community case definition: Any person with fever OR fever with headache, back pain, chills, rigor, sweating, muscle pain, nausea and vomiting OR suspected case confirmed by RDT.
2. Standard case definition: Any person with fever or fever with headache, rigor, back pain, chills, sweats, myalgia, nausea, and vomiting diagnosed clinically as malaria.
3. Suspected: Patient with fever or history of fever in the last 48 hours and lives in malaria endemic areas or has a history of travel within the past 30 days to malaria-endemic areas.
4. Probable: Any person with fever and one or more of major sign such as headache, rigor, back pain, chills, sweats, myalgia, nausea, and vomiting diagnosed clinically as malaria.
5. Confirmed: Any suspected case that is confirmed by microscopy or RDT for plasmodium parasites.
Inclusion criteria
1. Cases: Any residents of Werer and Badhamo village, who had symptoms of malaria and agreed to participate
2. Controls: Any residents of Werer and Badhamo village during the study who was a neighbor to a case and who did not develop signs and symptoms of malaria and agreed to participate.
3. Exclusion criteria
4. Cases: Those who refused to participate
5. Control: Those who refused to participate and did not fulfill inclusion criteria
Ethical consideration
All participants were informed about the objective of the study, confidentiality of the participant was assured and informed consent was sought from and given by the participants, with the knowledge they were free to withdraw at any time. Ethical clearance was obtained from the institutional review board of Mekelle University, College of health sciences and the support letter was written from Afar regional health bureau to Amibera district health office.
RESULTS AND DISCUSSION
Descriptive epidemiology by person
This study revealed that, among a total of 431 suspected malaria cases, 198 (45.9%), 233(54.1%) were males and female respectively. Fever and headache were the two predominant clinical manifestations. Sweating and Diarrhea were less frequent, being present in approximately one quarter of the cases (Table 1).
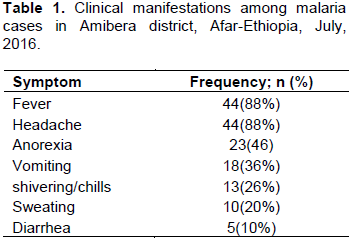
The median age of suspected malaria cases was 27 years old (range- 2 to 63 year).The most affected age group was >=15 years (63.6%) followed by 5-14 age groups (27.2%) and <=4 years age group (8.2%) of all notified suspected malaria cases (Table 2).
The highest and lowest positivity rate was reported in the age group above 15 years (100%) and less than 4 years (78.5%) respectively (Table 3).
Among the total suspected malaria cases (431), 423 (98.1%) of them were examined by RDT/Microscopy and 8 (1.9%) were treated clinically. Of the total positive cases, Plasmodium Falciparum accounts for 404/423(95.5%) followed by P. Vivax 11/423 (4.5%). For the screened 415 febrile cases, RDT result comes out with 98.1% positivity rate. As the national guideline the outbreak threshold is 50% positive; these results confirmed the outbreak (Table 4).
The overall attack rate was 36.7 per 1000popn with a case fatality ratio of zero. Age group above 15 years was the most affected with an AR of 63.7 per 1000popn followed by age group 5-14 years which accounts for 11.4 per 1000 population (Table 5).
Descriptive epidemiology by place
Among the total suspected malaria cases, 349/423 (82.5%) were from Werer village and 74/423 (17.5%) were from Badhamo village, Amibera district. The most dominant species responsible for this outbreak were P. Falciparum followed by Plasmodium Vivax. Positivity rate was high in Werer village (82.5%) as compared to Badhamo village (17.5%)
The populations in Werer village were more affected by malaria outbreak followed by Badhamo village with an attack rate of 31 and 11 per 1000 population, respectively (Table 6).

Descriptive epidemiology by time
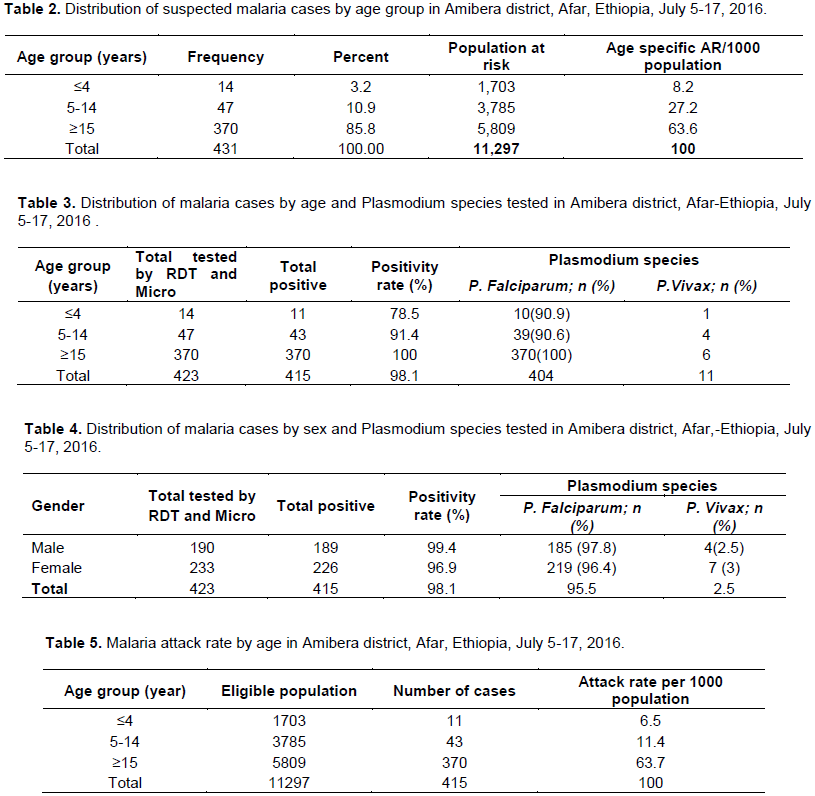
In both assessed villages, malaria outbreak was verified by comparing the current year data with a third quartile method (2nd largest number) during the previous 5 years (2011-2015). It was shown that the current case trend line crossed the threshold levels in both villages (Figure 1), peaked in second week and started to decline after the fourth week of July 2016 (WHO week 26 to 29/2016).
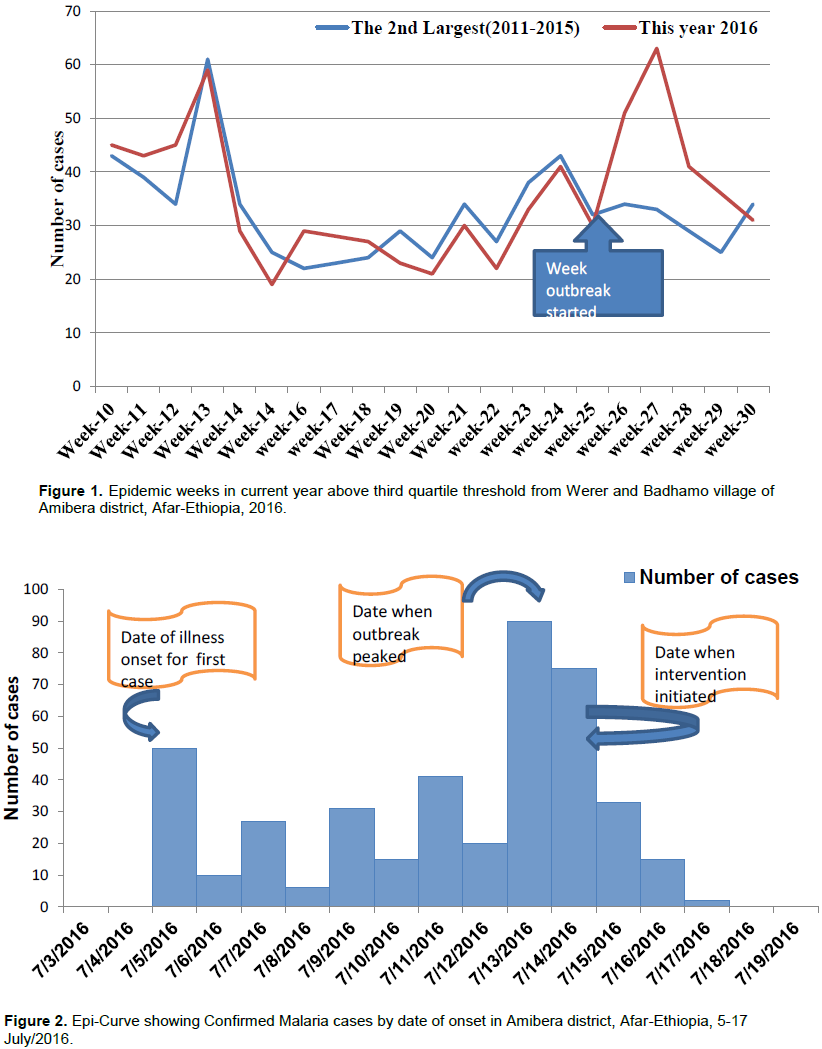
Epic curve showed that, district health office departed to the outbreak area lately, a week after the outbreak started. The epi-curve showed the outbreak was a propagated one with multiple peaks with a possibility of person to person transmission (Figure 2).The weeks when the epidemic started were on March 6, 2016. However, the district health department was notified on July 5, 2016. The peak numbers of malaria patients were on 13th to 14th July, 2016. The proportion of P. Falciparum infections was higher than that of P. viva.
Epidemic preparedness and response
None of the district’s health facility that we visited had an epidemic preparedness plan or an epidemic preparedness committee in place prior to the outbreak. There was no functional radio system for communication. They had to travel almost 15 km by foot or bicycle to communicate with the health district. There were no epidemic management funds available in the country prior to the occurrence of the epidemic. No chemical was available in all the health districts that we visited. The public health surveillance system is run by one person in Amibera health facility. The system was not evaluated prior to the occurrence of the epidemic.
Risk factor analysis
In order to asses associated factors, 117 malaria case-patients and 117 community control were selected conveniently and interviewed from Werer and Badhamo village of the Amibera district. Of 117 case-patients and 117 controls, 87(73.2%) and 73(62.4%) were females for case-patients and controls respectively. The multivariable binary logistic regression analysis showed that, persons not using insecticide treated bed nets (every night) were 3.52 times more likely to be exposed to malaria parasite than those who use insecticide treated bed nets (every night) with (AOR=3.52 (3.33, 4.12) (Table 7).
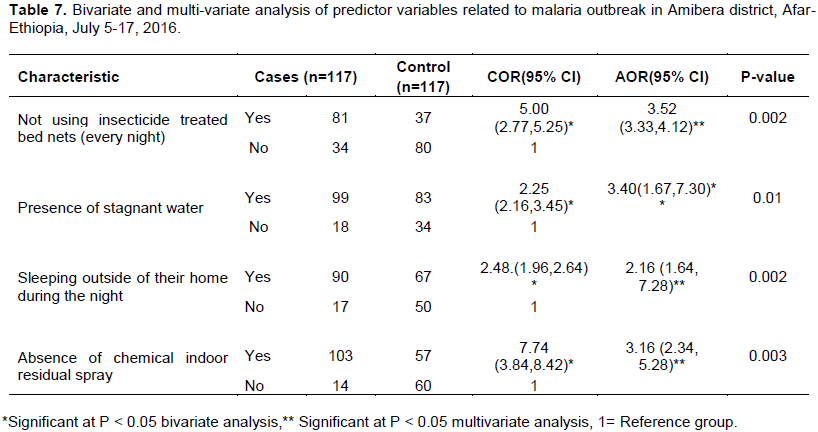
In addition, persons who live in an area where there is stagnant water were 3.4 times more likely to be exposed to malaria parasite than those who do not live in an area with stagnant water (AOR=3.40(1.67,7.30). Moreover, sleeping outside at nights and absence of chemical indoor residual spray were risk factors for the occurrence of the outbreak and statistically significant with an AOR of 2.16 (1.64-7.28), 3.16 (2.34, 5. 28) respectively (Table 7).
Environmental assessment
Thirty-three households from each affected village were arbitrarily selected and visited to search for new malaria cases and observe the status of insecticide treated bed nets utilization during night time. All households had at least one insecticide treated bed nets in their house, but, only 36.3% (12) of the households hanged it in their ceiling directly to the bedding while the rest were put underneath the beds and other places in the house. However, 17/33(51%) of the places visited, household nets were damaged. About 14/33(42%) do not use their nets at all while of those who reportedly use their nets, about 23/33(69.6%) use their nets irregularly.
Public health interventions
A total of 137 (7%) households with 106 unit structures was sprayed with Propoxur and Bendiocarb chemical in Werer village. Abate chemical was sprayed as anti-larval on stagnant water with an estimated area of 46 m2. A total of 18 volunteered people participated in this activity. Communities were mobilized and taught on prevention and control measures of malaria disease. Health professionals were mobilized and assigned to the affected village for active case search and early case management in the community.
These case-control studies confirmed existence of malaria outbreaks based upon believable five years of the 2nd largest number as a threshold to compare with 2016 on a weekly basis including laboratory diagnosed malaria data.
Malaria outbreak appreciated at the end of the week of June/2016 when it started to cross the threshold. The health facility had weekly malaria outbreak monitoring chart for early detection of an outbreak, but they were not reported to the district health office when the number of cases crossed the threshold. It was an exaggerated seasonal increase precipitated by interruption of vector control intervention. There were multiple potential mosquitoes breeding sites difficult for environmental management (Shalako Rivers) which surrounds the affected village and maybe the probable source of the outbreak.
Malaria outbreak in affected village was related to the national outbreak scenario; actually the outbreak occurred at different period depending on the weather condition of the region, but overall it is believed to have started in April, and lasted until the end of December. Many region of Ethiopia began reporting an abnormally increased number of malaria cases(Alemu, 2015; AMREF, 2008).
This study revealed that, the high proportion of Plasmodium falciparum cases shows difference as compared to the nationally registered proportion of Plasmodium falciparum and P. vivax which is 60 and 40%, respectively (Daddi and Abebe, 2012). This variation may be linked to high sensitivity of the malaria rapid diagnostic test. Since clients who get cured from malaria have also the chance to be positive for malaria if tested by the RDT within 14 days of treatment; this may increase the positivity rate falsely when clients visit health facility within 14 days of treatment. This is consistence with the case-study report from Oromia region (Alemu, 2015; AMREF, 2008).
In this study, the malaria outbreak lasted for two weeks (July 5-17/ 2016) due to inadequate vector control intervention in affected village. Heavy rain fall in affected village in mid-June was significantly attributed to the stagnant water bodies, and unusual temperature in affected village may also favore mosquito breeding site which is consistence with literature (Tarekegn, 2013).
Moreover, Amibera District is a place where agro-industry is under way both by private and government organization. Many unknown number of migrants come to work from different parts of the country; a lot of quarry works holding water bodies are suitable for mosquito breeding.
The results of analytical epidemiological study showed that, unusual heavy rainfall followed by high temperature is considered as one of the confirmed causes of malaria outbreak which agrees with the study from northeastern Ethiopia (Alemu, 2015; AMREF, 2008, 2011)
Besides this, using of bed net every night is associated with malaria parasite exposure and absence of timely chemical indoor residual spraying was associated with higher risk of febrile illness which is consistence with the study from Amhara Regional States (Workineh et al., 2015).
In addition, Stagnant water surrounding affected village and their compound was one of the dominant risk factor for malaria outbreak, which is consistent with previous reports in the literature (Alemu, 2015; AMREF, 2008; WHO, 2015); and study from Sri Lanka and India indicated that people living closer to vector breeding sites were at higher risk for malaria parasite exposure than those living farther away (Kiszewski and Teklehaimanot 2014).
This outbreak scenario has clearly showed that, in order to prevent and control malaria infection the sustainable implementation of vector control intervention through well organized malaria related strategies and programmes is crucial. Inter-sectoral collaboration and control interventions are prerequisites for malaria control and elimination.
Limitation of the study
Mosquito breeding sites were visited in the village but observation of mosquito larva was not conducted due to lack of expert.
CONCLUSION
The malaria outbreak current situation is high in magnitude than three years ago. Inability to analze and interprete the surveillance data at the district level delayed the outbreak investigation. This late notification of the outbreak shows that there is weak monitoring of malaria trends at district. This study revealed that, the attack rate was highest among above 15 years age groups (63.7 per 1000 of population) compared to the other age groups with sex difference. Sleeping outside of their homes during night, presence of stagnant water, absence of chemical indoor residual spray and poor utilization of insecticide treated bed net were attributed for this outbreak.
RECOMMENDATIONS
To prevent subsequent malaria outbreaks in the village it is recommended that Afar regional health bureau, Amibera district health office, District health facility and other sectors be interested in malaria prevention:
1. Since most of the village of the district are malarious area, insecticide treated bed net should be distributed for
all households and utilization of bed net should be monitored and optimized.
2. Timely indoor residual spraying operations have to be planned as per required standard (twice per year) and applied before rainy season with appropriate chemical.
3. Trends of malaria cases should be monitored on weekly basis at all levels. This could help for early detection of malaria outbreak.
4. Community mobilization on disruption of potential mosquitoes breeding site.
5. It needs further study to evaluate validity and reliability of rapid diagnostic tests to avoid false positivity rate.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors are grateful to Mr. Aweke, Miss Etaferyiman, and Amibera District Health Office for their support and cooperation; Mr. Wuiso Ahmad - UNICEF Regional Representative and Mr. Musa Mohammad for their leadership roles during all stages of the outbreak investigation; and the Ethiopian Field Epidemiology Training Programme for financial support.
REFERENCES
|
African Medical and Research Foundation (AMREF) (2011). Report on malaria baseline survey in two woredas of zone 5 in afar region, northeast ethiopia Lancet, 371:1-55. |
|
|
African Medical and Research Foundation (AMREF) (2008). Report on malaria baseline survey in two woredas of zone 5 in afar region, northeast ethiopia Lancet, 371:1-55. |
|
|
Alemu HD (2015). Malaria outbreak investigation in seba boru and melka soda woredas, guji and borena zones, oromia, Ethiopia. American Journal of Health Research. pp. 1-45. |
|
|
Daddi J, and Abebe A (2012). Analysis of malaria surveillance data. . BioMed Central pp. 1-14. |
|
|
Gemechu B, Ayele B, Adamu A, Zegeye H (2015). A malaria outbreak in ameya woreda, south-west shoa, oromia, Ethiopia.American Journal of Health Research, 3(3):125-129. |
|
|
Hurissa D (2015). Malaria outbreak investigation in seba boru and melka soda woredas, guji and borena zones, oromia. Ethiopia American Journal of Health Research, 3:1-45. |
|
|
Kevin J, Baird M (2010). Epidemiological measures of risk of malaria. SPRINGER 5:1-20. |
|
|
Kiszewski AE, Teklehaimanot A (2014). A review of the clinical and epidemiologic burdens of epidemic malaria. American Journal of Tropical Medicine and Hygiene, 71:128-135. |
|
|
Policy USGH (2013). The global malaria epidemic. The Kaiser Family Foundation. |
|
|
Tarekegn A (2013). Guidelines for malaria epidemic prevention and control in ethiopia. American Journal of Health Research, 3:1-30. |
|
|
Workineh KA, Andualem TM, Gize YA (2015). Assessment of control measures and trends of malaria in burie-zuria district, west gojjam zone, amhara region, north west ethiopia. Hindawi, pp. 1-5. |
|
|
World Health Assembly (2016). Global technical strategy for malaria 2016-2030. Retrieved from |
|
|
World Health Organization (WHO) (2015). Eliminating malaria Retrieved from |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


