ABSTRACT
This study is a direct hands-on epidemiological sampling of a hospital data of registered patients for tuberculosis (TB) in the Kasungu District Hospital of Malawi. The data for the year 2013 and 2014 were chosen as the latest but random sample to analyze whether the data fit in and follow the broad pattern of the country at the national level and also at the global level. The data represent convoluted results of genuine TB diagnosis and latency, but impacted by the socio-cultural mindset to obtaining health care in general. Incidences of human immunodeficiency virus (HIV) run in close parallel to TB as the former precariously enhance the vulnerability from TB infection to the disease stage.
Key words: Tuberculosis (TB), Malawi, human immunodeficiency virus (HIV).
Tuberculosis (TB) is a disease caused mainly by bacteria (Mycobacterium tuberculosis) in majority of cases followed by other similar microbes such as Mycobacterium bovis (Liu et al., 2015; Chatterjee and Pramanik, 2015; Wobudeya et al., 2015). It is a disease that has rather a ubiquitous presence by affecting almost 1/3 of the world population in latent form (Castilla et al., 2009). The TB microbes infect many people before visible symptoms are discovered when the disease is fully evident. Also, when a person develops active TB (disease), the symptoms (cough, fever, night sweats, etc.) are initially so mild that they procrastinate medical care and thus it results in transmission of the bacteria to others. A TB patient can infect up to 10 to 15 other people through close contact over the course of a year and therefore, is a ferociously contagious disease (Kehn-Hall et al., 2011). TB had the dubious distinction of being the largest single cause of death in industrialized countries in the mid-nineteenth century (Wobudeya et al., 2015). However, the TB mortality declined dramatically because of efficient disease management including treatment by chemotherapy and improving social circumstances. In a significant way, the World Health Organization (WHO) has taken multipronged approaches of the disease prevention and management so that post 2015, in the following twenty years, the world will be free of TB (Global Tuberculosis Report, 2015; Yoko et al., 2015).
Like many diseases, TB is an opportunistic disease and socio-economic factors play pre-eminent roles in deciding the national statistics with regard to this disease (John et al., 2007). The sub-Saharan African nations make interesting case studies for building a perspective in terms of occurrences of TB and the management of the disease.
The current study comprises of a direct look at the Hospital registration data of reported cases of TB in Kasungu District Hospital of Malawi. The access to the data was provided to the researchers of STEM Research Institute, Fairfax, VA, USA, who, along with the hospital authorities, undertook an analysis of one year of reported cases.
Thus, the cases have been organized on the basis of gender, age and time of the year as well as the patients’ human immunodeficiency virus (HIV) status. The focus year is 2014, though some data of 2013 are included when comparison was warranted. The years were chosen simply to have the latest data at the time of the study.
Data were obtained directly from the registers of the Kasungu District Hospital of Malawi. Hospital records included every TB case and admitted patient, type of TB, category of TB, and treatment outcome. Death could be due to any cause during anti-tuberculosis treatment. For patients that died during their stay at the hospital, the age, sex, and day of death were recorded.
Patients that tested smear positive were treated for six months at the hospital and would be identified as cured if they tested smear negative after the entire duration of the treatment period. Relapse was defined as completing the six-month treatment for the previous TB, contracting TB again, and testing smear positive. No treatment
outcome was a result of no information being available.
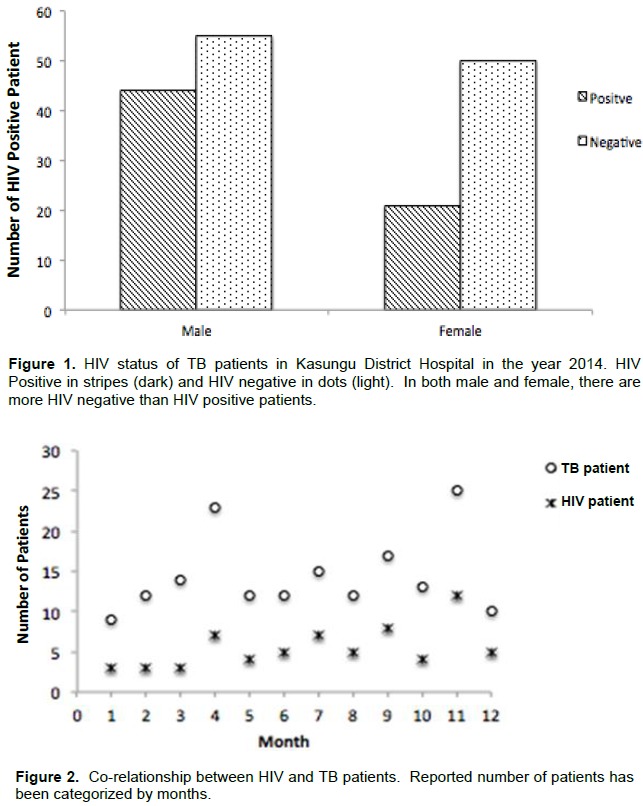
In the year 2014, there were 234 male and 164 female patients over the age of 5 and only 5 male and 1 female minor with age ≤ 5 years, as listed in Table 1. Of the patients over 5 years, 5 males died of the disease.
It is a common phenomenon to see co-affliction of TB and HIV because the HIV positive status increases the vulnerability of a person to TB infection. Figure 1 shows the HIV status of the TB patients. There were 45 HIV positive vs. 56 HIV negative in males, while 21 and 50, respectively among females. These figures translate to 18.8% of the total male patients testing HIV positive vs. 23.4% male patients testing HIV negative in 2014 and 12.7% female patients testing HIV positive vs. 30.3% female patients testing HIV negative. Figure 2 shows the total numbers of TB patients as they vary from month to month. It may be noted that except for larger number of patients in April and November and concomitantly more HIV positive cases, the number of patients average between 13 and 14 per month with roughly 40% of them detected HIV positive among both males and females.
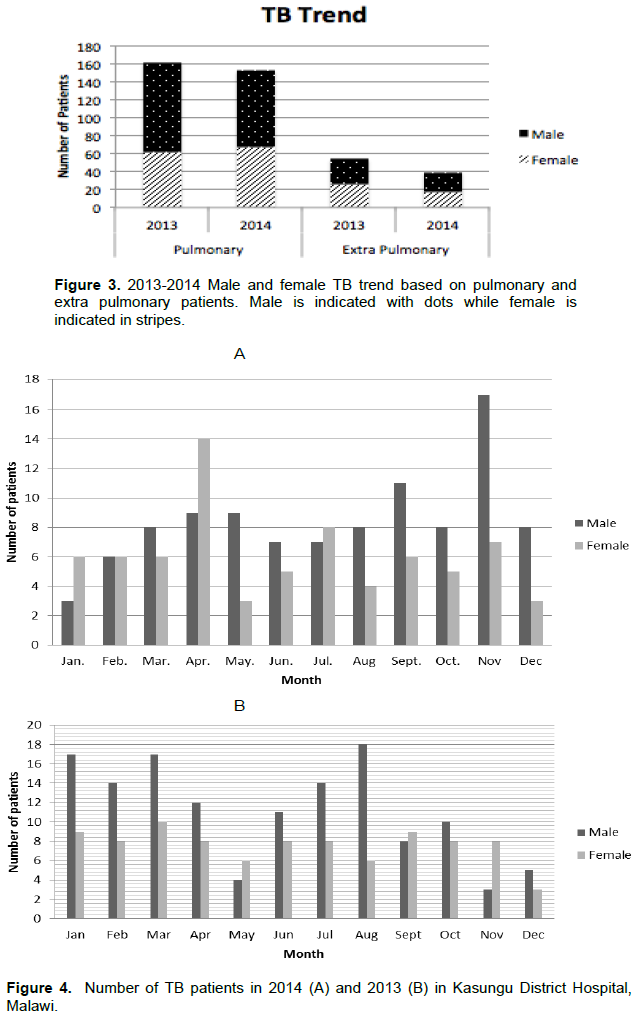
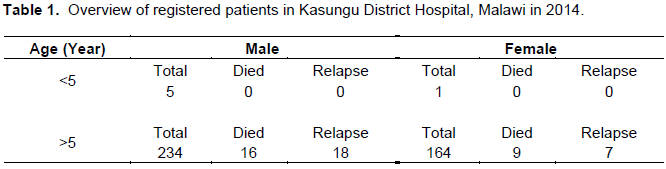
It is apparent that there was a decrease in the total number of TB cases in the year 2014 compared to the previous year (Figure 3). In order to comment on whether there is a general trend of the year-to-year decrease on the total number of cases, multi-year data analysis is necessary, which is beyond the scope of this short study. However, the decrease of total number of TB patients is an encouraging sign. Figure 4 shows month-to-month variations in both 2014 and 2013 of the total TB patients for either gender and irrespective of their HIV status. It appears that there is no clear tendency of a particular time of the year spiking on the number of TB patients.
The incidence of diseases on the sub-Saharan Africa has been a subject of intense studies and analysis both from epidemiological perspective as well as from a socio-economic context (Bell et al., 2015; Peter et al., 2013; Christine et al., 2011). The burden of TB in sub-Saharan is enormous. Continuing poverty and other socio-political realities in the continent have largely inhibited progress in implementing effective TB control measures, both indigenous and internationally sponsored. Needless to mention, TB is closely related to lifestyles of poverty, overcrowded conditions, drug addiction, and malnutrition. This disease spreads quickly among undernourished populations. But aside from this, the link between TB and the acquired immune deficiency syndrome (HIV/AIDS) is the one that exacerbates the problem most. People who are latently infected with M. tuberculosis, about one-third of the inhabitants of sub-Saharan Africa, are at hugely greater risk of developing active TB if they are also immunologically weakened by HIV positive status (Scheele et al., 2002).
Malawi happens to be one of the least developing countries in the world. The economy is heavily based on agriculture, with a largely rural population, low life expectancy and high infant mortality. The country faces challenges in education, health care and environmental protection. However, the country has several programs running with international aid and the outlook has been improving over the years. The scene of disease management including TB also shows some optimistic outcomes.
The hospital data from the Kasungu District Hospital in the survey year 2014 shows that there are more male patients afflicted with the disease than females, though the case mortality in case of females is higher. This is likely because there was a higher percentage of smear positive among all female TB patients compared to all male TB patients. The total number of patients has decreased from 2013. The percentage of infant patients (under 5 years) is less than 1% in both genders and the case fatality rate is nearly nil. The overall trend of the TB incidence and management seems consistent with the national trend. The data from Table 1 suggests high cure rate or at least low death rate. But it should be borne in mind that according to one study, about 40% of TB deaths in Malawi occurs in the first two months of treatment (Harries et al., 2001; Kang’ombe et al., 2004). There is also evidence that high mortality amongst patients occurs months or years after TB treatment. A TB report by Nyirenda (2006) has collected the data from 1997 and 2002. A comparison of the current hospital data with the report suggests that the trends have remained intact in that the male patients outnumber females in both HIV positive and negative patients.
Although, the reported low incidence among children is an encouraging finding, it also has to be noted that the diagnosis through regular procedure such as smear-positive tests are not very effective in children. Additionally, this study is limited to only cases that were registered and treated in the district hospital. It should also be recognized that the NTP uses passive case finding, that is, patients present to health facilities for TB diagnosis, which is the most inexpensive and easiest way of databasing. Therefore, it is understandable that because of the latency of the disease or other cultural or socio-economic constraints, these statistics could be highly underestimated.
According to the WHO, the year 2015 is a watershed moment in the battle against tuberculosis (TB) since WHO set up the Millennium Development Goals (MDGs) at the start of the millennium to tackle deadly disease. The slogan has been from Stop TB Strategy to the End TB Strategy. Both Kenya and Malawi have reported decreases in tuberculosis incidence among both HIV-infected and uninfected people (Yuen et al., 2014; Kanyerere et al., 2014). WHO established a global TB monitoring system and accordingly, 20 annual rounds of data collection have been completed. Overall, the global trend shows an immense optimism that TB can be completely eradicated in specified time frame earmarked by the organization. Thus, this study report would potentially testify, at a later time analysis of the country profile of Malawi, as being a credible component of a set of studies by various agencies.
The authors have not declared any conflict of interests.
REFERENCES
|
Bell LCK, Breen RM, Robert F, Noursadeghi M, Lipman M (2015). Paradoxical reactions and immune reconstitution inflammatory syndrome in tuberculosis. Int. J. Infect. Dis. 32:39-45.
Crossref
|
|
|
|
Castilla J, Palmera R, Navascues A, Abeti M, Guillermo A, Irisarri F, Jimenez MS, Garcia CM, Barricarte A (2009). Population-based contact investigation of a cluster of tuberculosis cases in a small village. Epidemiol. Infect. 137(10):1426-1435.
Crossref
|
|
|
|
|
Chatterjee D, PramanikArun K (2015). Pathophysiology Tuberculosis in the African continent: A comprehensive review. Pathophysiology 22(1):73-83.
Crossref
|
|
|
|
|
Christine U, Daniels KR, Matthew LJ, Christopher R (2011). The environmental and social influences of HIV/AIDS in sub-Saharan Africa: a focus on rural communities. Int. J. Environ. Res. Pub. Health 8(7):2967-2979.
|
|
|
|
|
Global Tuberculosis Report (2015). World Health Organization. ISBN 978 92 4 156505 9.
|
|
|
|
|
Harries AD, Hargreaves N, Gausi F, Kwanjana J, Salaniponi F (2001). High early death rate in tuberculosis patients in Malawi. Int. J. Tuberc. Lung Dis. 5:1000-1005.
|
|
|
|
|
John MA, Menezes CN, Chita G, Sanne I, Grobusch MP (2007). High tuberculosis and HIV coinfection rate. Emerg. Infect. Dis. 13:795-796.
Crossref
|
|
|
|
|
Kang'ombe CT, Harries AD, Ito K, Clark T, Nyirenda TE, Aldis W, Salaniponi FML (2004). Long term outcome in patients registered with tuberculosis in Zomba, Malawi. Int. J. Tuberc. Lung Dis. 8:829-836.
|
|
|
|
|
Kanyerere H, Mganga A, Harries AD, Tayler-Smith K, Jahn A, Chimbwandira FM, Mpunga J (2014). Decline in national tuberculosis notifications with national scale-up of antiretroviral therapy in Malawi. Pub. Health Action 4:113-115.
Crossref
|
|
|
|
|
Kehn-Hall K, Boshoff HI, Kashanchi F, Dowd CS (2011). Design, synthesis, and biological evaluation of novel Mtb-specific Dxr inhibitors as potential antitubercular agents, San Jose, Geraldine; Abstracts of Papers, 242nd ACS National Meeting and Exposition, Denver, CO, United States, August 28-September 1, 2011.
|
|
|
|
|
Liu EM, Abel D, Paul S, Donna S, David L, Nan C, Guerino S, Christopher R, Hertzmark E, Fawzi WW (2015). Tuberculosis incidence rate and risk factors among HIV-infected adults with access to antiretroviral therapy. AIDS (London, United Kingdom). 29(11):1391-1399.
Crossref
|
|
|
|
|
Nyirenda T (2006). Epidemiology of Tuberculosis in Malawi, Book Chapter. Malawi Med. J. 18(3):147-159.
|
|
|
|
|
Peter J, Gwenan M, Lawn Stephen D, Corbett, Elizabeth L, Richard G (2013). Predicting the long-term impact of antiretroviral therapy scale-up on population incidence of tuberculosis. PLoS One 8(9):e75466.
Crossref
|
|
|
|
|
Scheele P, Dolin V, Pathania MC (2002). Global Burden on Tuberculosis: Estimated Incidence, Prevalence, Mortality by Country. Bull. World Health Organ. 80(6).
|
|
|
|
|
Wobudeya E, Deus L, Irene R, Lubega FMugabe, Moorine S, Philippa M (2015). Epidemiology of tuberculosis in children in Kampala district, Uganda, 2009–2010; a retrospective cross-sectional study. BMC Pub. Health 15:967.
|
|
|
|
|
Yoko VL, Ulla KG, Anna V (2015). Costs to Health Services and the Patient of Treating Tuberculosis: A Systematic Literature Review. Pharm. Econ. 33:939-955.
Crossref
|
|
|
|
|
Yuen CM, Weyenga HO, Kim AA, Malika T, Muttai H, Katana A, De Cock KM (2014). Comparison of trends in tuberculosis incidence among adults living with HIV and adults without HIV-Kenya, PLoS One 9(5):e99880.
Crossref
|
|