Full Length Research Paper

ABSTRACT
Vaccine preventable diseases are the major global health problem which contributes to morbidity and mortality of less than 5 years child population. But, the immunization coverage worldwide is below the target. Therefore, the study was aimed at immunization coverage of 12 to 23 months old children in Areka Town, Sothern Ethiopia. A community based cross-sectional study conducted from 10th March to 19th June 19, 2016 in Areka Town, Sothern Ethiopia. Data on 173 children aged 12 to 23 months from 173 households selected using a systematic random sampling. Analysis was conducted using SPSS version 20. The result presented in the all tables and figures. The study showed that, 130(75.4%) fully vaccinated and 93(53.6%) vaccinated during immunization campaigns. The sources of information for 39(22.5%) were radio and television. 22(12.9%) missed vaccine appointment day and 13(7.7%) interrupted vaccine program. Of the vaccinated children, 166(96.2%) vaccinated for Bacillus Calmette–Guérin (BCG), 138(80%) vaccinated for oral polio vaccine (OPV) 0, 172 (99.2%) OPV1, Penta1 and PCV1, 165(95.4%) vaccinated for OPV2, Penta2 and PCV2, 161(92.9%) vaccinated for OPV3, Penta3 and PCV3, and 158(91.5%) vaccinated for measles. The dropout rate from BCG to measles was 4.7%.Therefore, continuous support and health education at the community level is recommended.
Key words: Immunization, Areka, children, oral polio vaccine (OPV), Bacillus Calmette–Guérin (BCG).
INTRODUCTION
The extended program on immunization (EPI) was launched to reduce morbidity and mortality, promote national self-reliance and deliver immunization services against six major childhood diseases (Lakew et al., 2015). Immunization is a highly effective, cheap and essential components of every child survival programs in the world (Mbengue et al., 2017; Ekouevi et al., 2018). Vaccine preventable diseases are the major global health problem which contributes for morbidity and mortality of less than 5 years child population (Mbengue et al., 2017).
According to prevalence of vaccine preventable diseases in each country and economic status of that nation, every country set their own immunization program (Mbengue et al., 2017). The Ethiopian health policy has given emphases to prevent and control major communicable diseases. It was integrated to general health services as essential component of primary health care. The program goal remained largely unrealized with low and fluctuating coverage for many years (Ekouevi et al., 2018). The services are given at static level in health setup, and outreach program and national immunization days (Mbengue et al., 2017).
According to the guidelines developed by the World Health Organization, children are considered to have received all basic vaccinations when they have received a vaccination against tuberculosis, three doses pentavalent, polio vaccines, HBV vaccine and a vaccination against measles (Restrepo-Méndez et al., 2016). Various countries have specific strategies for reaching targeted coverage implementation of new approaches called reaching every district and sustainable outreach. The immunization coverage worldwide is below the target (Mutua et al., 2016; Hu et al., 2015). In Ethiopia, the routine immunization coverage has not reached targeted figures and planned objectives. Insufficient health personnel, lack of adequate health facilities, transportation shortage, high defaulter rate from schedule, missed opportunity, in adequate supplies are among major health problems identified as a cause or factors for low immunization coverage in Ethiopia and many countries (Negussie et al., 2016; Kassahun et al.,2015; Legesse et al., 2015).
Despite improvements world over in vaccine coverage in the last ten years, still there is regional and local disparities due to factors such as limited resources; competing health priorities; poor management of health systems and inadequate monitoring and supervision (Crocker-Buque et al., 2017). Therefore, community awareness creation programs, delivering health education, taking feedback from the mothers and involving the community members in the service delivery may enhance the service utilization (Mutua et al., 2016). Furthermore, continuous training of the health professionals is essential (Kiptoo et al., 2015, Adokiya, et al., 2017). The study was aimed at immunization coverage of 12-23 months old children in Areka Town, Sothern Ethiopia.
MATERIALS AND METHODS
Study design and area
A community based cross-sectional study was conducted from 10th March to 19th June, 2016. All households with 12 to 23 months of age children in Areka town were the source population. Selected households in with 12 to 23 months of age children were the study population. All households with 12 to 23 months of age children who stayed for more than 6 months were included. Parents or care givers who were mentally challenged and chronically sick were excluded.
Sample size determination and sampling technique
The sample size was determined using a formula for estimation of single population proportion with the following assumptions: 76% proportion ( Kassahun et al., 2015), Z a/2 is the Z value at 95% Confidence level (1.96) and 0.05 margin of error (d). Adding 10% for the non-response rate the final sample size was 301. A systematic random sampling method was used. The first household was selected by lottery method. Data were collected from every 8th households.
Data collection tools and techniques
A structured questionnaire was used to collect data from the respondents. Three data collectors and one supervisor were used. Training was provided for the data collectors and the supervisor for two days. The session of the training was the objective of the study, meaning of each question and interview techniques. In addition, the role of data collector and the supervisor was covered.
Ethics statement and data quality assurance
Each respondent was informed about the objective of the study and was assured of confidentiality. Each respondent briefly informed about having the right to stop the interview at any time they want. Pretesting was conducted using 5% of the total sample. Training and supervison were provided for the data collectors and the supervisors. Each questionnaire was coded and completeness of filled questionnaire was checked.
Data processing and analysis
Data first were checked for completeness, and then each completed questionnaire was assigned a unique code. Subsequently, the data was entered using EpiData 3.1. The generated data were then exported to SPSS version 20. Finally the results were summarized and presented in texts, tables, and graphs.
Operational definition
Full vaccination
A child who takes all vaccine and full dose according EPI schedule by age of 12 month.
On vaccination process
A child who already started vaccination and still on vaccination process according to EPI schedule but not complete or default vaccination.
RESULTS
Socio-demographic characteristics
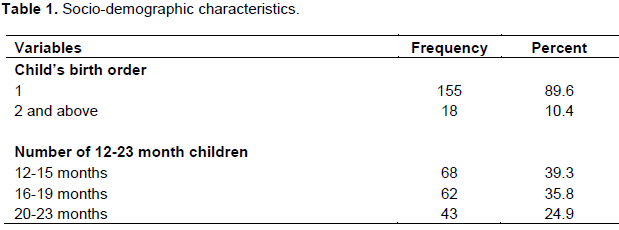
One hundred fifty five (89.6%) were the first child and 68(39.3%) were 12 to 15 months old age (Table 1).
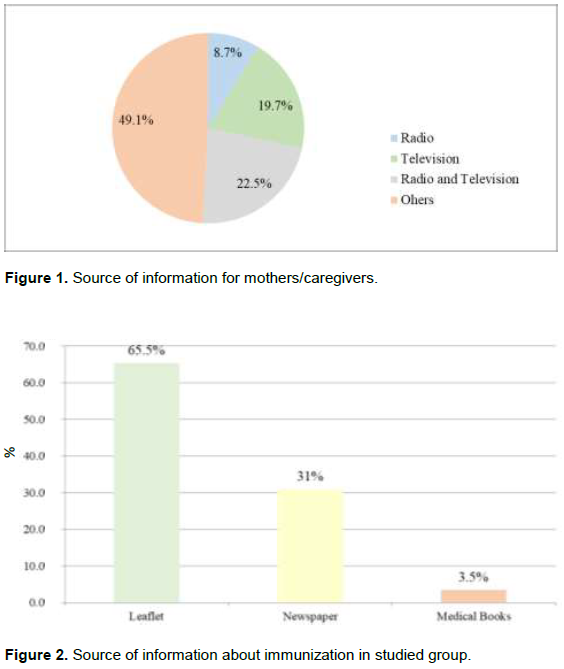
Source of information
The source of information for 15(8.7%), 34(19.7%), 39(22.5%) and 85(49.1%) were radio, television; both radio and television and others source of information, respectively. Regarding the written source of information, 113(65.5%), 54(31%) and 6(3.5%) had information from leaflet, newspaper and medical books, respectively (Figures 1 and 2).
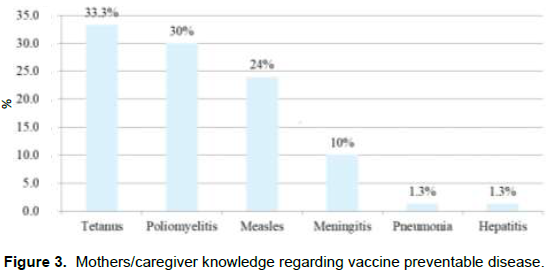
Knowledge of the vaccine preventable diseases
Fifty eight (33.3%), 52(30%), 42(24%), 17(10%), 2(1.3%) and 2(1.3%) of the respondents knows that tetanus, poliomyelitis, measles, meningitis, pneumonia and hepatitis are vaccine preventable diseases (Figure 3).
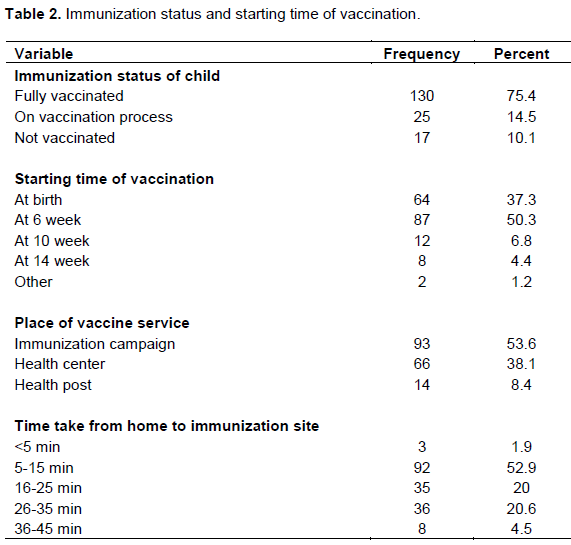
Immunization status
One hundred thirty (75.4%) of the children were completely vaccinated and 87(50.3%) of the children were vaccinated starting from 6 week. Ninety three (53.6%) of the respondent children get immunization service during immunization campaign. For the 92(52.9%) respondents, it took 5 to 15 min to go to the immunization site (Table 2).
Immunization schedule adherence
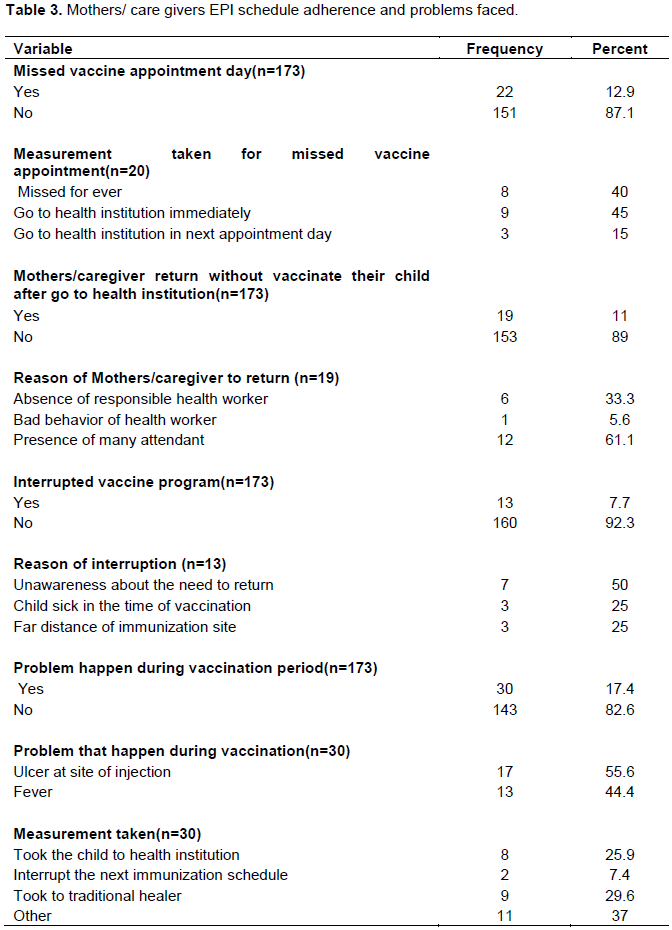
Twenty two (12.9%) of the children missed appointment day. Nine (45%) of the respondents took the child to the health institution immediately when they remember that they miss the appointment. Nineteen (11%) returned due home without using the service. Twelve (61.1%) of them returned home due to the presence of many attendants. 13 (50%) of respondent had interrupted vaccine program due to unawareness about the need to return the next dose. Thirty (17.4%) of the respondents reported that the children vaccinated had a problem during the vaccination period and 17(55.6%) experienced ulcer at the site of children to the health institution for treatment (Table 3).
Types of immunization
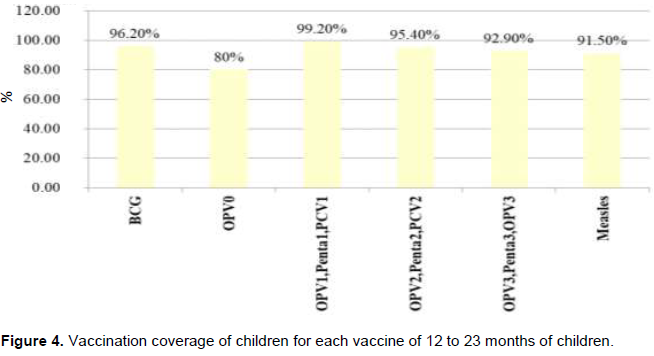
Of the vaccinated children 166(96.2%) vaccinated for BCG, 138(80%) vaccinated for opv0, 129 172(99.2%) OPV1, Penta1 and PCV1, 165(95.4%) vaccinated for OPV2, Penta2 and PCV2, 161(92.9%) vaccinated for OPV3, Penta3 and PCV3, and 158(91.5%) vaccinated for Measles (Figure 4).
DISCUSSION
The study showed that 75.4% children of 12 to 23 months of age were fully vaccinated. This finding is comparable to a finding from a study conducted in Tamil Nadu in which 76% of children were fully vaccinated (Murugesan et al., 2017) and in Kenya which reported that 76.6% were fully vaccinated (Maina et al., 2013). On the other hand this finding is lower than a report from a study conducted in India which showed that 80.7% (Chaudhari et al., 2016) were fully vaccinated. It is also lower than a finding from a study done in Rims, Ranchi (87.3%) (Vidyasagar et al., 2017). This difference could be reacted to a difference in the level of intervention done to address the issue of immunization coverage in the study areas.
Furthermore, the finding is higher than a report from studies done in in Allahabad district 31% (Masood et al., 2011), 57% India (Shrivastwa et al., 2015), 65.4% Zimbabwe (Mukungwa et al., 2015) and hosanna 30.51% (Ayano et al., 2015). This might be due to the fact that in the study area immunization is currently delivered in the form of community outreach program which is supported by the health extension workers. Therefore, access to the service increased. In addition, health education is delivered to the community through the community based training programs.
In this study the overall drop out was 4.7%. This finding is comparable to a finding from a study conducted in Debre markos town, Amhara Regional State, Ethiopia which reported the overall dropout was 5% (Gualu et al., 2017). The finding is lower from a report from a study conducted in Bareilly District 37.3% (Joshi et al., 2011). This might be related to the difference in the delivery of the service in the two study areas. There might be a difference in the interventions applied to the increase the access to the immunization service. The difference in year at which the studies conducted might also contribute to the difference. Currently, due to increased provision of information and advancement of community engagement in the health care, the community is more likely to use the service.
In this study, among children aged 12 to 23 months 10.1% were not vaccinated. This is lower than a finding from a study conducted in Jigjiga District, Somali National Regional State, Ethiopia which reported that 25.4% of children were not vaccinated at all (Mohamud et al., 2014). The discrepancy might be due to a difference in study setting. The vaccination coverage is different in the study areas. According to a national report, in Somalia the vaccination coverage is only 22%. As compared to other vaccines coverage, the BCG vaccine was high. Accordingly, 96.2% were vaccinated for BCG. This could be due to the fact that it is administered at the time of delivery inside the health institution. There is a decrease in the vaccination coverage from BCG to measles in which only 91.54% children were vaccinated for measles. This could be due to lack of intention to use the service, far distance of health facilities and lack of continuous encouragement.
CONCLUSION
Only half of the children’s were fully vaccinated and majority was vaccinated during immunization campaign. The main written source of information for the mothers or caregivers was leaflets. Continuous support and health education should be provided at the community level. At individual level, frequent follow-up of a change in attitude and knowledge is essential. Especially the health promotion should focus on the returning of children for another dose of vaccination. Furthermore, health institutions should work to improve the quality of vaccination care.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adokiya MN, Baguune B, Ndago JA (2017). Evaluation of immunization coverage and its associated factors among children 12–23 months of age in Techiman Municipality, Ghana, 2016. Archives of Public Health 75(28). |
|
|
Ayano B (2015). Factors Affecting Fully Immunization Status of Children Aged 12- 23. |
|
|
Chaudhari CC, Gunjana G, Kelkar VS, Patel DA, Saiyed SM, Thakor N (2016). Immunization status of 12-23 months children in urban slums of Ahmedabad city, Gujarat, India: a cross sectional study. International Journal of Advances in Medicine 3(4):816-9. |
|
|
Crocker-Buque T, Mindra G, Duncan R, Mounier-Jack S (2017). Immunization, urbanization and slums – a systematic review of factors and interventions. BMC Public Health 17(556). |
|
|
Ekouevi DK, Gbeasor-Komlanvi FA, Yaya I, Zida-Compaore WI, Boko A, Sewu E, Lacle A, Ndibu N, Toke Y, Landoh DE (2018). Incomplete immunization among children aged 12–23 months in Togo: a multilevel analysis of individual and contextual factors. BMC Public Health 18(952). |
|
|
Gualu T, Dilie A (2017).Vaccination Coverage and Associated Factors among Children Aged 12–23 Months in Debre Markos Town, Amhara Regional State, Ethiopia. Advances in Public Health. |
|
|
Hu Y, Luo S, Tang X, Lou L, Chen Y, Guo J (2015). Comparative assessment of immunization coverage of migrant children between national immunization program vaccines and non-national immunization program vaccines in East China. Human Vaccines and Immunotherapeutics 11(3):761-768. |
|
|
Joshi HS, Gupta R, Singh A, Mahajan V (2011). Assessment of Immunization Status of Children between 12-23 Months in Bareilly District Nepal Journal of Epidemiology 1(2):47-50. |
|
|
Kassahun MB, Biks GA, Teferra AS (2015). Level of immunization coverage and associated factors among children aged 12–23 months in Lay Armachiho District, North Gondar Zone, Northwest Ethiopia: a community based cross sectional study. BMC Research Notes 8(239). |
|
|
Kiptoo E, Esilaba M, Kobia G, Ngure R (2015). Factors Influencing Low Immunization Coverage Among Children Between 12 - 23 Months in East Pokot, Baringo Country, Kenya. International Journal of Vaccines and Vaccination 1(2):00012. |
|
|
Lakew Y, Bekele A, Biadgilign S (2015). Factors influencing full immunization coverage among 12–23 months of age children in Ethiopia: evidence from the national demographic and health survey in 2011. BMC Public Health 15 (728). |
|
|
Legesse E, Dechasa W (2015). An assessment of child immunization coverage and its determinants in Sinana District, Southeast Ethiopia BMC Pediatrics 15(31). |
|
|
Maina LC, Karanja S, Kombich J (2013). Immunization coverage and its determinants among children aged 12 - 23 months in a peri-urban area of Kenya. Pan African Medical Journal 4(3). |
|
|
Masood A, Dwivedi S, Singh G, Hassan MA, Singh A (2011). Assessment of immunization status of children between 12-23 months in allahabad district. National Journal of Community Medicine 2(3):346-348. |
|
|
Mbengue MAS, Mboup A, Ly ID, Faye A, Camara FBN, Thiam M, Ndiaye BP, Dieye TN, Mboup S (2017). Vaccination coverage and immunization timeliness among children aged 12-23 months in Senegal: a Kaplan-Meier and Cox regression analysis approach. The Pan African Medical Journal 27(8). |
|
|
Mbengue MASM, Sarr M, Faye A, Badiane O, Camara FBN, Mboup S, Dieye TN (2017). Determinants of complete immunization among Senegalese children aged 12–23 months: evidence from the demographic and health survey. BMC Public Health 17(630). |
|
|
Mohamud AN, Feleke A, Worku W, Kifle M, Sharma HR (2014). Immunization coverage of 12–23 months old children and associated factors in Jigjiga District, Somali National Regional State, Ethiopia. BMC Public Health 14(865). |
|
|
Mukungwa T (2015). Factors Associated with full Immunization Coverage amongst children aged 12 – 23 months in Zimbabwe. African Population Studies 29(2):1761-1774. |
|
|
Murugesan D, Ramasubramanian R (2017). A study on immunization coverage of 12-23 months children in urban areas of Kanchipuram district, Tamil Nadu. International Journal of Community Medicine And Public Health 4(11):4096-4100. |
|
|
Mutua MK, Murage EK, Ngomi N, Ravn H, Mwaniki P, Echoka E (2016). Fully immunized child: coverage, timing and sequencing of routine immunization in an urban poor settlement in Nairobi, Kenya. Tropical Medicine and Health 44(13). |
|
|
Negussie A, Kassahun W, Assegid S, Hagan AK (2016). Factors associated with incomplete childhood immunization in Arbegona district, southern Ethiopia: a case – control study. BMC Public Health 16(27). |
|
|
Restrepo-Méndez MC, Barros AJD, Wong KLM, Johnson HL, Pariyo G, França GVA, Wehrmeister FC, Victora CG (2016). Inequalities in full immunization coverage: trends in low- and middle income countries. Bull World Health Organ 94:794-805. |
|
|
Shrivastwa N, Gillespie BW, Kolenic GE, Lepkowski JM, Boulton ML (2015). Predictors of Vaccination in India for Children Aged 12-36 Months. American Journal of Preventive Medicine 49(64):435-444. |
|
|
Vidyasagar KA (2017). Evaluation of Immunization Coverage among Children between 12-23 Months of Age, Attending Immunization Centre at Rims, Ranchi: A Cross Sectional Study. Journal of Medical and Dental Science Research 4(4):1-4. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


