Full Length Research Paper

ABSTRACT
Research suggests that inappropriate approaches to information dissemination can negatively affect containment of an outbreak, including Ebola, norovirus, SARS, influenza, and now Coronavirus. The objective of this study was to examine how COVID-19 information disseminated to the public was perceived by Californians during the beginning of the COVID-19 outbreak. A cross sectional study of 207 California residents was conducted to determine perceptions regarding the dissemination of COVID-19 information. A Kruskal Wallis test was conducted using SPSS 27 to examine potential differences in groups regarding access to information. Also, Chi-square analysis was conducted to determine Californian’s perceived reliability of the information presented to them early in the outbreak. A difference was found between the use of social media and online sources, the news, and word of mouth in relation to accuracy of information (p=0.05) and trustworthiness of information (p=0.05). There is also a statistical significance for sufficiency of information, timeliness of information, and trustworthiness of information compared to reliability of information (p<0.001). Of the 66% of participants who said COVID-19 related information provided during the start of the outbreak was unreliable, 75% of them reported that the information was also insufficient, 84% said it was untimely and untrustworthy. The majority of Californians were dissatisfied with how information was presented during the beginning of the COVID-19 pandemic. Not providing accurate, timely, trustworthy, and sufficient information during an outbreak result in knowledge gaps, riskier behaviors, and in the case of California, may have potentially increased cases of COVID-19.
Key words: COVID-19, health information, California, trend study, epidemiology.
INTRODUCTION
What is already known on this subject?
Before this study was conducted, there was and still limited information and knowledge about the public’s perceptions of COVID-19 related information given out at the start of the pandemic. Therefore, this study is novel and needed because it helps us garner more knowledge on how COVID-19 related information was perceived by those receiving it. Thus, it helps health professionals to control inaccurate information by means that allows for correct information to be presented in a timely, trustworthy, accurate, and sufficient manner during any pandemic.
At the end of 2019, severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) emerged and quickly spread globally. However, coronaviruses have been around for some time. As early as 2003, SARS coronavirus (SARS-CoV-1) was identified and believed to be a zoonotic virus that originated in bat populations in China (WHO, 2020). Initial confirmed human cases of coronavirus disease 2019 (COVID-19) were reported in Wuhan, China in December 2019 (WHO, 2020). Quickly after, the spread rose to pandemic levels. Over the next few months, countries took precautions beginning with ceasing travel, mandating quarantine orders, requiring face masks, and emphasizing social distancing practices. Some countries that followed similar ordinances managed to contain or lower the cases of incidence in their area. Countries that did not make safety restrictions mandatory or who took longer to close their borders, reported higher numbers of active cases. Restrictions included wearing face masks, avoiding large gatherings, wearing disposable gloves, or washing hands frequently, and practicing social distancing to avoid droplets from those who cough or sneeze (Agarwal et al., 2020).
What does this study add?
As a result of this study, we learned that giving consistent accurate information about Covid-19 from start would have helped reduce the spread of the virus. The faster a plan of action that targets misinformation is given to the public during pandemics, the faster trust can be built, which will allow more people to access accurate information from credible sources.
In the U.S. between December 2019 and March 2020, hospitals began to have an influx of patients with symptoms that included: shortness of breath, cough, fever, pneumonia, sore throat and even loss of taste and smell (Agarwal et al., 2020). Treatment was nonexistent to minimal, so symptoms were primarily maintained to the best of hospitals’ abilities and diagnosis was often confused as Influenza (flu) cases (CDC, 2019). In early March, states including California and New York began suggesting to their residents to stay at home and socially distance. When these suggestions were not followed, governors, including California’s Gavin Newsom, issued stay at home orders and curfews in mid-March (Office of Governor, 2020). All the while, new cases and COVID-19 related deaths in the United States continued to rise, particularly in population-dense states such as California. COVID-19 was being compared to Influenza due to the similarity of symptoms but eventually was categorized as a separate illness (WHO, 2019). During initial outbreak
months, it was also diminished to not being a deadly virus since it had the lowest overall death rate compared to more prevalent diseases such as influenza, Ebola, and severe acute respiratory syndrome. However, health officials emphasized the risks of COVID-19 due to the rate at which transmission was spreading, which was observed to be higher than the rate of transmission for the flu. Consequently, the U.S. healthcare system was faced with overwhelmed hospitals, shortages of available beds, limitation of personal protective equipment (PPE), closing of businesses, increase in unemployment rate, and the rise to number one in terms of number of infected cases globally (Mareiniss, 2020; Blustein et al., 2020).
Between December 2019 and February 2020, information about COVID-19 spread on social media and news outlets was changing daily. Misinformation was spread through these means. Although sources like the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) are readily available with up-to-date information for the public, members of the public continue to trust unreliable sources. On March 21, 2020, over 27% of YouTube’s top 150 videos about coronavirus, had non-factual information and over 62 million views (Li et al., 2020). Facebook and Twitter faced similar issues, having over 600 posts about false cures, anti-vaccination concerns, or conspiracy theories (BBC, 2020). These posts were not immediately flagged for including potentially illegitimate information and were accessed by thousands (BBC, 2020). At times, these sources disguised themselves as credible sources yet lacked true credible references. This led health officials to quickly develop informative counter posts and to provide legitimate sources of information. However, remaining knowledge gaps allowed for the emergence of conspiracy theories that resulted in further distrust and public misinformation (BBC, 2020).
Coronavirus disease 2019 (COVID-19) is not the first disease in which misinformation contributed to increased infection rates and prevalence of disease. During outbreaks, misleading information given to the public by inappropriate sources can cause people to resist appropriate and correct information. This stems not only from misinformation but also fear, lack of a secure plan, and lack of resources needed to support local health official responses. Effects of misinformation need to be better examined and trends tracked to determine potential correlations and reoccurring problems that can be addressed prior to future outbreaks. Examining how different countries handle outbreaks can help us understand practices that work and those that do not. Gathering a better understanding of people’s perceptions regarding outbreaks can help inform improvement strategies within the public health system, especially as it pertains to information dissemination and use of reliable sources.
Previous pandemic outbreaks have demonstrated that information about a disease and delayed transparency of
information to the public affect the time of containment. Research on diseases such as Ebola, influenza, SARS, and norovirus have all demonstrated how information during outbreaks can exacerbate infectious disease outbreaks and instill fear on the public through unreliable information from various sources (Brainard and Hunter, 2020; Sell et al., 2020). In some cases, misinformation can instill fear in people and contribute to distrust in the government, public health, and medical professionals. For instance, the COVID-19 pandemic led to widespread misinformation particularly among Americans, thereby, creating distrust in health professionals (McKay et al., 2020). The timing and source of information can either help decrease disease spread or lead to wider spread of the virus (Olaimat et al., 2020).
Public health officials have found that information gaps are recurring problems that affect pandemics and other serious health-related topics such as cancer self-screening, tobacco use, and obesity risks (Dower, 2013). These information gaps include delayed or incorrect information as well as mistrust in those who deliver health information (Dower, 2013). Investigating factors that contribute to how people access information as well as their perceptions about the information presented to them, allows us to understand common disconnections between the public and health officials. There have been consistent challenges with keeping the public informed to make the best health decisions for themselves. The goal of this study was to examine California residents’ perceptions of information disseminated during the COVID-19 pandemic while also assessing their perceptions of information accuracy. This understanding will help public health professionals address the issues and may be applicable to other areas in public health that face similar information gap challenges.
Research questions
This study examined two questions, which are “what factors contribute to how California residents access information related to COVID-19? And what perceptions did California residents have about the information presented to them at the start of the COVID-19 outbreak?
METHODOLOGY
Study design
This was a cross-sectional study, which assessed individuals’ perception of information provided during the outbreak of COVID-19 from December 2019 to April 2020. A survey was created that includes demographic questions to help understand the population being studied as well as perceptive questions. The online survey was shared with colleagues, friends, school mates, family members, people on social media (through Facebook, Instagram, and Twitter), and was posted on Reddit.com under the subreddit posts of r/Coronavirus, r/takemysurvey, and r/samplesize. Anyone over the age of 18 was encouraged to fill out the survey and assured that responses were anonymous and voluntary. This research focused specifically on Californians’ views on a health-related issue and helped us determine and identify population perspectives. Survey questions incorporated into the study included the respondents’ perception on whether information presented to them in relation to COVID-19 was timely, sufficient, efficient, accurate, and trustworthy. Other questions determined the study population’s first sources of pandemic related information. Before data collection began, approval from California Baptist University’s Institutional Review Board (IRB) was obtained. Furthermore, informed consent was stated in the beginning of the survey and had to be acknowledged by all participants before they could proceed with the survey. If an individual did not consent to be in the study, the survey ended immediately, and they were not able to proceed with filling out any portion of the survey. The consent form highlighted that participation was completely voluntary and ending participation in the survey may be done by the participant at any time throughout the survey. Qualtrics was used to collect responses and no identifying information was gathered from the participants.
Study participants
Participants aged eighteen and older were recruited through online and word of mouth. The study’s sample focused on California residents over the age of eighteen who observed how information from COVID-19 was presented. Anyone outside of California, under the age of eighteen years old was excluded from the study. This allowed for an understanding from online cohort users’ perspectives across different platforms where large amounts of COVID-19 information were presented during the beginning of the pandemic. Non-random convenience sampling was utilized; this sampling technique did have potential issues of bias including population misrepresentation. However, convenience sampling provides a fair deal of benefits as well. Examining a pre-existing group is cheap, efficient, and allows for simple implementation (Jager et al., 2017). Disqualification from the study was categorized for respondents that did not complete demographic questions including age and specific questions relating to information access, which were needed for analysis.
Measures
The variables of interest for this study included dependent and independent variables. The dependent variable was source of information (the outcome). The independent variables were perceived timeliness, sufficiency, accuracy, and trustworthiness of information (predictors). These variables were analyzed as individual’s perceptions. Demographic questions included age, sex, ethnicity, and education.
Instruments/data collection
A COVID-19 questionnaire was created to control questions asked and avoid researcher bias. Questions that were asked were specific to the source of information (where individuals get information from), perceived timeliness (information received right away), efficiency (information being effective in the best possible way), sufficiency (information being enough to understand the situation), accuracy (information had reliable facts), and trustworthiness (information had credible sources). Centralizing the questions around specific information allows for an understanding of the group of interest’s interpretations and response to each question. This questionnaire included questions for each variable. These questions were written as:
(1) With regards to how information got out to the public about COVID-19, do you agree or disagree that the information was generally sufficient?
(2) With regards to how information got out to the public about COVID-19, do you agree or disagree that the information was generally accurate?
(3) With regards to how information got out to the public about COVID-19, do you agree or disagree that the information was generally timely?
(4) With regards to how information got out to the public about COVID-19, do you agree or disagree that the information was generally trustworthy?
Answer choices for the listed perception questions within the questionnaire included strongly agree, agree, somewhat agree, neither agree nor disagree, somewhat disagree, disagree, and strongly disagree.
Questions populated from the questionnaire included both demographic and perception-based questions regarding COVID-19. Demographic variables included age, gender, education, and ethnicity. Demographic questions were used to understand factors that contribute to how people access information related to COVID-19. Age group, gender, education level, and ethnicity were the factors explored. Behavioral variables including formal and informal gatherings, CDC or WHO guidelines, covering of mouth when sneezing, use of hand sanitizer, social distancing, self-quarantining, and proper hygiene were also assessed. These variables were analyzed through grouping analysis to understand frequencies of use from the start of the pandemic. An anonymous survey link was posted across different social media platforms and Reddit. This link directed participants to the Qualtrics questionnaire where their identity remained private. Participants first read the consent form at the beginning of the questionnaire and acknowledged their right to end the survey at any time and consenting that they are at least 18 years old. Remaining questions focused on their experience with COVID-19 from the months of December 2019 to April 2020.
Quantitative research establishes general laws of behavior across different contexts and tests theories to support or reject them (McLeod, 2019). These results can be useful for further investigation into understanding how perception with outbreaks is perceived, specifically COVID-19. Due to coronavirus, conducting interviews or in person surveys is not the optimal method of sampling because of restrictions of social distancing implemented during the time of the study. Instead, to acquire participants, a survey was created and published online by highly trafficked websites that are viewed by millions of people and used to represent an online based population. Facebook, Instagram, Twitter, and Reddit were used to recruit participants. These platforms were selected to try to reach different platforms that handle information in different ways. Facebook is a social media platform with 2.7 billion users (Clement, 2020a). Instagram has over 1 billion registered users (Clement, 2020b). Twitter is a social media platform with over four-hundred-forty million monthly users (Lin, 2020a). Reddit is a public online website that is accessed by over four-hundred million people worldwide (Lin, 2020b).
Data analysis
Analysis was conducted using the latest Statistical Program for the Social Sciences (SPSS) software version 27. Frequency distributions were used to analyze demographic factors including age groups, gender, ethnicity, and education levels. Grouping method analysis was used for demographic and behavioral variables. Kruskal-Wallis test was used for each variable to examine the dependent variable of source of information against each independent variable of sufficiency, timeliness, accuracy, and trustworthiness. A Pearson chi-square test was performed and
reported a two-sided p-value based on a Chi-square distribution with two degrees of freedom. Chi-square test was used to assess participants’ perception of reliability of information in relation to access to information. Interpretation of the results was observed based on overall responses to each question. These techniques were selected due to the data’s non-normal distribution.
Patient and public involvement
How, were the development of the research question and outcome measures informed by patients’ priorities, experiences, and preferences? The questionnaire was piloted tested with a small group of young and seasoned professionals in public health. A second pilot test was conducted with a group of 18 and above college students in California.
How did you involve patients in the design of this study? Patients were not directly involved in the design of this study; however, every day people were solicitated to provide feedback on the questionnaire.
Were patients involved in the recruitment to and conduct of the study? No, patients were not involved in the recruitment to and conduct of the study.
How will the results be disseminated to study participants? The results of the study were presented at the university to a group of faculty and will be made available to all individuals in the study once the manuscript is accepted and published.
For randomized controlled trials, was the burden of the intervention assessed by patients themselves? This is not applicable to this study.
Patient advisers should also be thanked in the contributorship statement/acknowledgments.
If patients and/or the public were not involved, please state this. Patients and public were not involved in advising role for this study.
RESULTS
Characteristics of the study sample
The survey generated a total of 222 responses of those who lived in California. Fifteen responses had substantial missing data, thereby, they were excluded from analysis. The remaining 207 responses were analyzed. Table 1 displays the characteristics of participants. Among the 207 respondents approximately 65% were female (n=135). Participants were all over the age of 18. By age groups, about 48% of respondents were between the ages of 18-29 years (n=100), 21% were between 30-39 years old (n=44), 11% were between 40-49 years old (n=24), 10% were between 50-59 years old (n=20), and 8% were over the age of 60 years old. In terms of education, respondents who had a University-Undergraduate Degree were approximately 47% of the participants (n=98) and 34% (n=49) of respondents had at least a University-Graduate Degree. About 36% were of White, Non-Hispanic Origin (n=74), 30% of participants were of Hispanic or Latino origin (n=62), and18% were of Asian, Asian-American or Pacific Islander Origin (n=37).
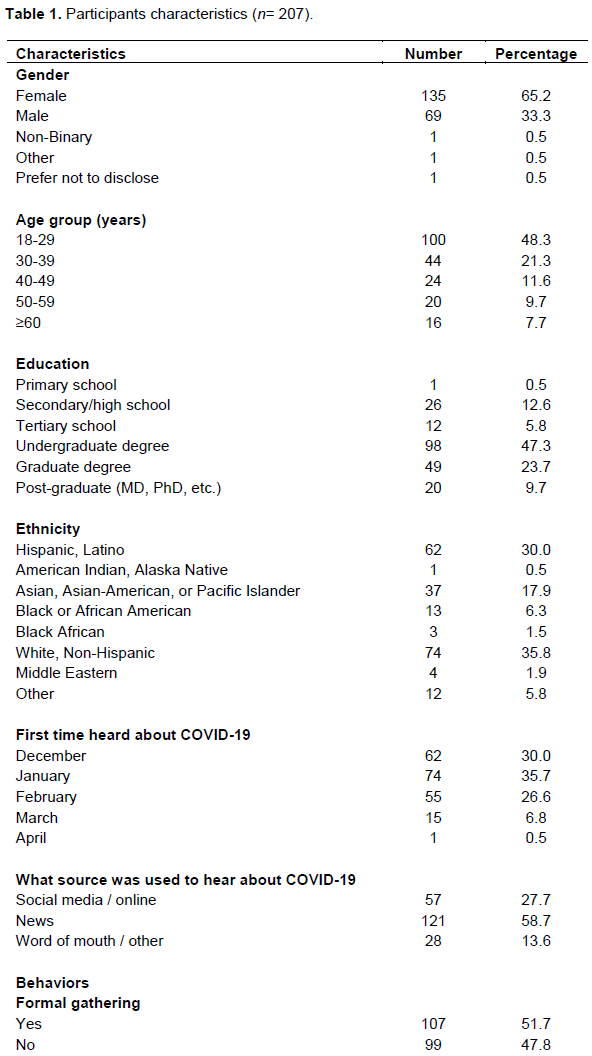
Between December 2019 and April 2020, approximately 36% of respondents stated they first heard about COVID-19 in January 2020 (n=74). While 30% first heard about COVID-19 in December 2019 (n=62) and approximately 27% first heard about COVID-19 in February 2020 (n=55). The most popular source used to obtain COVID-19 information was the news at approximately 59% (n=121) followed by social media at approximately 17% of responses (n=34).
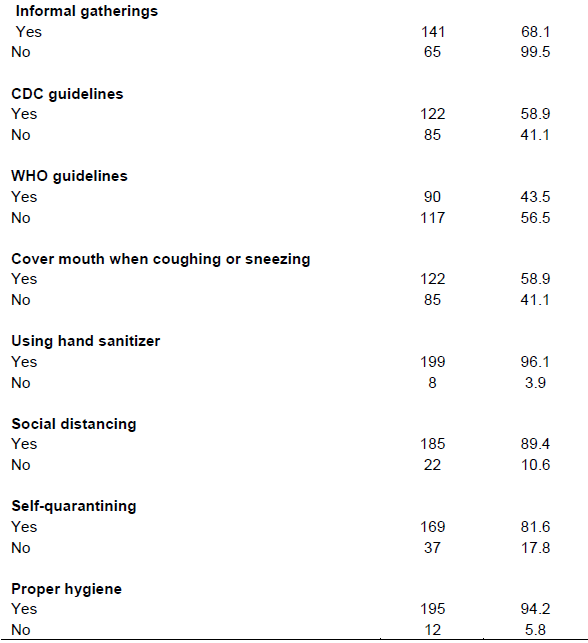
Preventative behavioral observations of participants during the outbreak included observation of practices with hygiene, referencing guidelines, and practicing suggested measures such as social distancing. Approximately 52% of respondents reported that they attended formal gatherings (n =107) and approximately 68% of respondents attended informal gatherings (n=141) during the pandemic. Of those who followed guidelines, 56% reported following CDC guidelines (n=122) while 44% reported following WHO guidelines (n=90). In terms of hygiene, about 59% of residents (n=122) reported covering their mouth when coughing or sneezing (n=122) and approximately 96% reported using hand sanitizer (n=199) during the pandemic. Majority (94%) of respondents (n=195) reported practicing proper hygiene including washing hands, covering when coughing and sneezing, and not touching their face to prevent contracting COVID-19 (Table 1).
Research question one
From the Kruskal Wallis analysis (Table 2), source of information was used to differentiate Californian’s perception of information provided during the start of the pandemic. Median change was analyzed to find differences between the groups. Three groups were compared: groups who accessed information through the news, through social media and online sources, and those who received COVID-19 information through word of mouth and other sources. These groups were observed in terms of sufficiency, accuracy, timeliness, and trustworthiness of information received. The Kruskal Wallis test for accuracy of information showed a statistically significant difference between the outcome (source of information) of the three groups (news, social media/online, and word of mouth/others) (c2 (2) = 6.03, p= 0.05) with a mean rank of 117.35 for social media and online sources, 98.08 for news, and 94.88 for word of mouth and other sources. For trustworthiness, the analysis showed a statistically significant difference between the outcome (source of information) of the three groups (news, social media/online, and word of mouth/others) (c2 (2) = 5.80, p = 0.05) with a mean rank of 116.67 for social media and online sources, 95.56 for news, and 106.68 for word of mouth and other sources. For sufficiency and timeliness of information, no significant differences (c2 (2) = 3.22, p=.20) (c2 (2) = 5.40, p=.07), respectively, were found among the three categories of participants (news, social media/online, and word of mouth/others).

Research question two
From the Chi-square analysis (Table 3), variables sufficiency, timeliness, and trustworthiness of information were compared to information reliability to understand participants’ perceptions. All variables had a p-value of less than 0.001. A majority (66%) of participants believed that COVID-19 related information provided at the start of the outbreak was unreliable compared with 34% of people who believed the information was reliable. From the participants who believed the information was unreliable, 75% found the information to be insufficient, 84% reported the information to be untimely, and another 84% found the information to be untrustworthy. About 19% of the participants who found the information provided during the start of COVID-19 to be unreliable also said the information was sufficient. Of the 34% who found the information to be reliable, 75% reported the information was sufficient, 46% said the information was timely, while approximately 44% said the information was not timely. The majority (79%) of participants found the information to be both reliable and trustworthy.

DISCUSSION
Research on previous outbreaks has demonstrated that incorrect information presented to the public potentially contributes to delayed containment (Perscheid et al., 2018). A common challenge with information presented during outbreaks include the lack of reliable information needed to close information gaps related to the disease along with associated preventative measures. Our study’s findings demonstrate that COVID-19 faced similar recurring challenges.
Kruskal Wallis analysis resulted in a significant p-value for accuracy and source of information. There is a difference in perceptions between people who access information through social media and other online sources, people who access information through the news, and those who access information through word of mouth. A majority of Californians reported the information they accessed at the beginning of the COVID-19 outbreak was not accurate across information sources.
Similarly, previous studies have found that people’s perceptions for sources vary, whereas people expressed that information from online sources were considered more accurate and reliable than information from public health officials (Malecki et al., 2020). There was also a significant difference for trustworthiness of information between those who accessed information through social media, news, and word of mouth. This indicates a difference between the three types of source of information. A majority of responses reported that COVID-19-related information presented to them at the beginning of the outbreak was mostly untrustworthy. This difference may be due to the fact that different sources of information are perceived to provide different levels of reliable information. However, another study found that social media, the news, and an official source observed, all had about the same number of links and information related to COVID-19 that led to low credibility (Yang et al., 2020). The variables sufficiency and timeliness were not significant in our analysis, but this is a small sample of the population and potential differences among our sample cannot be ruled out. Although our analysis did not show a significant difference between groups for these variables, a majority of participants agreed that the information across all sources were not sufficient nor timely. This suggests that Californians on average held a negative perception around COVID-19 information at the beginning of the outbreak, indicating a flaw in how information was distributed to the public. This is contradictory to the findings by Narayana et al. (2020), in their study on the knowledge, perception, and practices of the general public in India regarding COVID-19 pandemic. The authors found that participants displayed accurate knowledge and positive perceptions toward COVID-19, which shows the importance of information dissemination, one that is managed efficiently, to control the release of correct information about outbreaks to the public. It also shows that proper communication and release of accurate information regarding outbreaks at the start of an outbreak is vital to containment and garnering public trust. Thereby, having proper measures in place for communicating information about an outbreak early on is likely to help reduce the spread of the disease (McKinney et al., 2020).
The analysis of Chi square results compared Californians’ perceptions of the reliability of information to sufficiency, timeliness, and trustworthiness of information. Reliable information was highly statistically significant with sufficiency, timeliness, and trustworthiness of information. The majority of participants stated that information provided during the outbreak was neither reliable nor sufficient. This is in agreement with another study on perception where a little more than half of the respondents in the study had an accurate perception towards COVID-19 based on information they had found from various sources (Narayana et al., 2020). Narayana et al. (2020) went on to state that correct perception of COVID-19-related information was not an acceptable margin and that sensitization of myths and false information for the public is essential. Unreliable information, including myths and conspiracy theories can become harmful to the public. For timeliness it was reported that a majority (84%) of respondents found the information was both unreliable and untimely. This suggests that Californians had a negative perspective on information related to COVID-19 across all platforms of sources. The same is true for trustworthiness, in which a majority of respondents who believed the information was unreliable also stated that it was not trustworthy. Indicating an association between the doubt Californians had in the information presented to them during the beginning of COVID-19 across all information sources. It was observed that Californians felt the information about COVID-19 given to them was not trustworthy while Narayana et al. (2020), found that more than 50% of the general public in India knew correct information during the beginning of the pandemic, for each fact about COVID-19.
A study on whether people can distinguish fake news, found that although every country suffers widespread misinformation (e.g. conspiracy theories were popular in the United Kingdom while health related misinformation were common in the United States), on average, ten percent of participants were likely to believe the fake news while 30% are likely to know someone who believe it (Tadepalli, 2020). Another major issue determined in this study was that algorithms used by social media were amplifying posts with false information across platforms such as Facebook and Twitter, thereby increasing exposure (Tadepalli, 2020). Presenting the public with accurate information and building public trust in said information are two equally important components of educating populations regarding emerging pandemics.
CONCLUSION
Regardless of source, Californians consistently perceived information given at the beginning of the COVID-19 pandemic to be unreliable in terms of accuracy, trustworthiness, timeliness, and sufficiency. To assist in controlling the spread of COVID-19, it is essential that the public receiving information deem each of the aforementioned characteristics to be reliable. One such way this can be accomplished is by addressing any trending, yet inaccurate information through the use of social media platform flagging, whereas key words trigger alert warning users of potentially untrustworthy information. In order to ensure that public trust can be built quickly during pandemics, action plans targeting the spread of misinformation must be implemented early on, such that the public has access to accurate and reliable information from credible sources before inaccurate information is widely disseminated.
Strengths and limitations of this study
This is an innovative study because no other studies have been done in this area and the study focuses on how information is perceived to be disseminated during a pandemic, therefore can help public health professionals under better approaches to disseminate information to the public in the future. Another strength of this study includes the use of online surveys, which draws in younger participants who are technically savvy and future of public health. However, the use of online surveys, which exclude those who may not be technologically savvy can also be a weakness.
This survey focused on three of the most common forms of acquiring information: social media, news, and word of mouth. By acquiring participants from sources like reddit we can identify the perception of those who directly used these sources often. With the use of reddit comes potential bias from nonrandomization; however, this becomes less limiting due to reddit being one of the top ten most used websites in the world (Lin, 2020). Another limitation of this study is the use of online surveys, which exclude those who may not be technologically savvy but include those who monitor specific sites, hashtags, and forums where the link was posted. Internal validity is threatened due to outside concurrent events. Although people may be opinionated about concurrent events, our survey focused specifically on coronavirus related events and information.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Agarwal KM, Mohapatra S, Sharma P, Sharma S, Bhatia D, Mishra A (2020). Study and Overview of the Novel Coronavirus Disease (COVID-19). Sensors International, 100037. |
|
|
BBC (2020). Social media firms fail to act on Covid-19 fake news. |
|
|
Blustein DL, Duffy R, Ferreira JA, Cohen-Scali V, Cinamon RG, Allan BA (2020). Unemployment in the time of COVID-19: A research agenda. Journal of Vocational Behavior 119(2020):103436. |
|
|
Brainard J, Hunter PR (2020). Misinformation making a disease outbreak worse: outcomes compared for influenza, monkeypox, and norovirus. Simulation 96(4):365-374. |
|
|
CDC (2019). Symptoms of Coronavirus. |
|
|
Clement J (2020a). Facebook worldwide 2020. |
|
|
Clement J (2020b). Instagram: age distribution of global audiences 2020. |
|
|
Dower C (2013). Among different populations across the United States, substantial disparities in health and health care persist. Health Affairs. |
|
|
Jager J, Putnick DL, Bornstein MH (2017). More than just convenient: The scientific merits of homogeneous convenience samples. Monographs of the Society for Research in Child Development 82(2):13-30. |
|
|
Li H, Bailey A, Huynh D, Chan J (2020). YouTube as a source of information on COVID-19: a pandemic of misinformation? BMJ Global Health 5(5):e002604 |
|
|
Lin Y (2020a). 10 Reddit Statistics You Should Know in 2020 [Infographic]. |
|
|
Lin Y (2020b). 10 Twitter Statistics Every Marketer Should Know in 2020 [Infographic]. Oberlo. |
|
|
Malecki K, Keating JA, Safdar N (2020). Crisis communication and public perception of COVID-19 risk in the era of social media. Clinical Infectious Diseases. |
|
|
Mareiniss DP (2020). The impending storm: COVID-19, pandemics and our overwhelmed emergency departments. The American Journal of Emergency Medicine 38(6):1293-1294. |
|
|
McKay D, Heisler M, Mishori R, Catton H, Kloiber O (2020). Attacks against health-care personnel must stop, especially as the world fights COVID-19. The Lancet 395(10239):1743-1745. |
|
|
McKinney O, Sturz D, Mukaire P, Brown L, Toki H, Druten EV (2020). Effectiveness of the medical response teams to the 2014 Ebola outbreak: African immigrants' perceptions. Journal of Public Health and Epidemiology 12(4):349-356 |
|
|
McLeod SA (2019). Qualitative vs. quantitative research. Simply Psychology. |
|
|
Narayana G, Pradeepkumar B, Ramaiah JD, Jayasree T, Yadav DL, Kumar BK (2020). Knowledge, perception, and practices towards COVID-19 pandemic among general public of India: A cross-sectional online survey. Current Medicine Research and Practice 10(4):153-159. |
|
|
Office of Governor Gavin Newsom (2020). Governor Gavin Newsom Issues Stay at Home Order. |
|
|
Olaimat AN, Aolymat I, Shahbaz HM, Holley RA (2020). Knowledge and Information Sources About COVID-19 Among University Students in Jordan: A Cross-Sectional Study. Front. Public Health 8:254. |
|
|
Perscheid C, Benzler J, Hermann C, Janke M, Moyer D, Laedtke T, Adeoye O, Denecke K, Kirchner G, Beermann S, Schwarz N, Tom-Aba D, Krause G (2018). Ebola outbreak containment: real-time task and resource coordination with SORMAS. Frontiers in ICT 5(7). |
|
|
Sell TK., Hosangadi D, Trotochaud M (2020). Misinformation and the US Ebola communication crisis: analyzing the veracity and content of social media messages related to a fear-inducing infectious disease outbreak. BMC Public Health 20(1):1-10. |
|
|
Tadepalli A (2020). In the Age of Information, Can We Weed Out the Fake News? Cal Alumni Association. |
|
|
World Health Organization (WHO) (2019). Ebola health update - North Kivu/Ituri. DRC, 2018-2020. |
|
|
World Health Organization (WHO) (2020). Coronavirus disease 2019 (COVID-19) Situation Report - 94. |
|
|
Yang KC, Torres-Lugo C, Menczer F (2020). Prevalence of low-credibility information on twitter during the covid-19 outbreak. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


