ABSTRACT
This research was conducted in the Federal Capital Territory (FCT), Abuja of Nigeria and aimed at discovering areas of support needs required by TB patients from Treatment Supporters (TS), from the perspectives of TB patients, as compared to what the managers of TB program consider as ideal support. Here, qualitative design using Focus Group Discussions (FGDs), In-depth Interview (IDI) and Key Informant Interview (KII) were used. From the study, TB patients expressed their support needs while on treatment as follows: (1) monitoring and supervision of daily drug in-take, (2) motivational support to take the drugs as expected, (3) provision of support for feeding (when there is no food or means of eating), and (4) support for provision of transportation cost to visit TB clinic when the need arises. The study thus revealed that left on their own, TB patients may not be committed to taking their drugs and complete their treatment regimen, if any of these supports is lacking while on treatment. Patients with Treatment Supporters who were offered these supports, tend to complete their treatment regimen and not likely to default.
Key words: Tuberculosis, TB patients, supports needs.
Tuberculosis (TB) remains a major global health problem, responsible for ill health among millions of people each year. TB ranks as the second leading cause of death from an infectious disease worldwide, following Human Immunodeficiency Virus (Global TB Report, 2014). Apart from this, TB was responsible for 1.5 million people’s deaths (1.1 million HIV-negative and 0.4 million HIV-positive) (Global TB Report, 2015). Nigeria is one of the six countries (India, Indonesia, China, Nigeria, Pakistan and South Africa) accounting for 60% of new TB cases and progress in TB control globally depends equally on major advancement in TB prevention and care (Global TB Report, 2016). An important mandate of Community Tuberculosis Care (CTBC) program in Nigeria is demand creation for TB services through health education, social mobilization and awareness via trained individuals and Community Based Organizations (CBOs) involved in TB control at the community level. This is expected to translate into early TB detection, referral and treatment, also aimed to improve community support to TB patients through implementation of Treatment Supporters’ concept and other community support structures which also include TB clubs in schools.
WHO-recommended Directly Observed Treatment Short-course (DOTS) requires patients taking their drugs under daily observation of a healthcare professional (World Health Organization, 2001). DOTS ensures better patient adherence though it places a high burden of care on both providers and patients, leading to increased work load and patients having to walk long distances daily to receive their medication, which often results in high level default in treatment due to transportation costs.
Although it may be argued that tests and drugs are free for TB patients and therefore all other expenses should be left for patients to bear, reality shows that some patients cannot afford these other costs. This category of individuals constitutes a larger proportion of Nigerian population. Therefore, ignoring the socio-economic aspect of TB treatment has grave implications for disease control and development (World Bank Report on Poverty in Nigeria, 2014). The socioeconomic context of providing care and services for TB patients cannot be neglected especially in poor and developing countries.
For example, in the last (2013) National Demographic Health Survey (NDHS) conducted in the country, findings from household possessions indicated that; “in both urban and rural areas, only a small percentage of households possess a means of transport. Rural households are slightly more likely than urban households to own a motorcycle or scooter (34% versus 27%) or a bicycle (23% versus 13%), only 9% of households own a car or truck” (National Population Commission (NPC) [Nigeria] and ICF International, 2014).
While the DOTS approach has been in place and seems to have lessened the burden of care on patients, adherence to TB treatment still leaves much to be desired especially in a tenuous health system lacking in adequate human resources for health and infrastructures. As a result of this indisputable factor, the introduction of treatment support in TB therapy is meant to complement efforts and the effectiveness of this strategy has also engaged scholars’ attention. Review of literature on patients’ understanding of treatment support shows clearly the importance of patients’ social networks in facilitating effective treatment support for TB. Findings from studies underscore the need for a patient-centered approach to TB treatment as a veritable approach for disease treatment, cure and control.
In this respect, four factors are key; proximity to patient, emotional support, moral authority of the treatment supporter and the demonstrated confidence exhumed (Nachega et al., 2006). Proximity to the patient would enable the Treatment Supporter witness in-take of drugs by patient; obtain inventory of drugs to ensure availability as and when necessary. In providing emotional support, patients would expect a treatment supporter to demonstrate compassion, exhibit willingness to listen to the patient’s concerns, fears, etc. and have the moral authority to command the patient’s respect or influence his/her decisions (Nachega et al., 2006). The `social capital´ provided by a trusted patient-nominated treatment supporter (e.g. material and emotional support, health care utilization, etc.), may have contributed to saving lives, regardless of the DOTS component of intervention (Nachega et al., 2010).
In a qualitative study of patients’ understanding of treatment support in Nepal, respondents reported that the TB treatment burden was high, particularly in terms of difficulties with social and psychological aspects of undergoing treatment. They identified three main areas for support during treatment, namely: relevant information for them and their families about their disease, its treatment, potential side-effects and what they should do if side-effects arise; approachable and supportive healthcare staff with whom patients feel comfortable discussing (often non-medical) problems that arise during treatment; and some flexibility in treatment to allow essential elements of patients' lives (Christopher and Newell, 2009). Having such support systems is beneficial in helping patients follow a physician's recommendations and a strong social support will help patients stick to their medical regimen by reminding them among other things to keep their medical appointments and take their medicines (John Hopkins Centre to Eliminate Cardiovascular Health Disparity, 2015).
The mandate of TB control in Nigeria is vested on the National TB and Leprosy Control Programme (NTBLCP). The trend of the annual TB case notifications of all forms of TB in the country shows an unimpressive drift, though TB treatment success rate remain progressively consistent. The result of the first National TB Prevalence survey (2012), indicated that TB prevalence level in Nigeria for 2012 is estimated at 323 (95% CI: 239-406) per 100,000; indicating a higher level of TB prevalence in the country, than previously estimated by the World Health Organization (WHO) (The First National TB-Prevalence Survey in Nigeria, 2012).
In order to improve on treatment supporters’ concept implementation in Nigeria, the Association for Reproductive and Family Health (ARFH), a Principal Recipient of the Global Fund Grant, conducted an Operations research using qualitative research methodology on patients’ understanding of treatment supporter concept in Nigeria’s Federal Capital Territory (FCT). The objective of this study was to identify and document patients' support needs during TB treatment from TB patients’ perspectives, in order to inform the development of appropriate support and supervision strategies that accurately and appropriately meet patients’ needs.
Study area
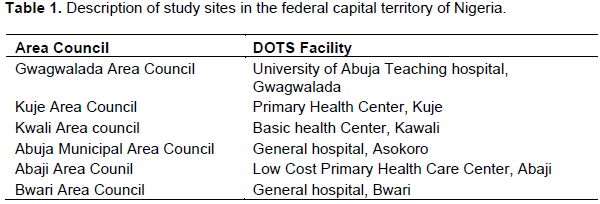
The study area is the Federal Capital Territory [FCT]; fondly referred to as Abuja, is the capital city of Nigeria. It is located at the geographic center of Nigeria and is bordered by Niger, Kaduna, Nasarawa and Kogi states. It occupies a land area of about 7,315 km2 (2,824 square miles). It was initially sparsely populated (1,406,239 population) as at the last census in 2006, which was nationally estimated at 140,431,790” (National Population Commission, Nigeria (2006). Currently, FCT is now the most rapidly expanding settlement in Nigeria with an annual growth rate of 9.3%. There are six area councils in the FCT namely; Abaji, Gwagwalada, Kuje, Bwari, Kwali and Abuja Municipal Area Council (AMAC). The major ethnic groups are Gwari, Hausa and Fulani.
Study design
As shown in Table 1, one public health facility providing TB services was purposively selected in each of the area council due to their patronage by members of the community. The research methodology is qualitative. Key Informant Interviews (KII) and Focus Group Discussions (FGDs) techniques were adopted. The suitability of the choice of methodology was based on the naturalistic and descriptive nature of qualitative research (Crosby et al., 2006); which is helpful to provide the information that addresses the specific objectives of the study. More importantly, the purpose of qualitative research is to understand social life and to disclose reality exactly as it is (Sotirios, 2003).
Study population and sampling
Owning to the specific objective and nature of the study, the sampling methodology for the selection of participants was purposive. Data was collected from three categories of respondents, namely; Treatment Supporters, health care workers providing health care services to TB patients in DOTS centers and TB patients on treatment. While Treatment Supporters and health care workers were interviewed through KII technique, TB patients participated in FGDs.
In each of the six Area Councils, two (2) FGDs (1 male, 1 female groups) were conducted among TB patients. These FGDs participants were identified and selected from DOTS facility’s TB Central register where TB patients’ were registered after diagnosis of TB. Participants who were selected for participation in the FGDs have been on treatment for not less than two months preceding the study. Fifteen (15) Treatment Supporters (TS) were identified from facilities’ records, and were interviewed as key informants across the six study sites. Lastly, in-depth interview was conducted with one (1) DOTS staff in each of the six facilities, where the FGDs were conducted.
Ethical approval for the study was granted by Federal Ministry of Health and Department of Public Health, National Health Research Ethics Committee. Consent from the management of the selected health facilities was obtained and participants were recruited into the study based on Informed consent.
Data management and analysis
Data generated was recorded on a Digital recording device with the consent of the participants and transcribed verbatim. Data content was analyzed in a rigorous manner guided by the objectives and themes from the discussion guides used for each category of the participants. Also, social, economic, cultural and political contexts in which the study was conducted, was considered in the interpretation of the findings. No qualitative data analysis software was used.
Data generated from this study revealed general low level of awareness and knowledge about TB among Treatment Supporters, health care workers and TB patients in DOTS centers and TB patients. The overwhelming majority of respondents lack accurate knowledge about the causes of TB. Although few described TB as a communicable or airborne disease, in most groups discussion conducted, patients described the modes of TB transmission as; sharing food, cigarettes and cutleries with an infected person. This widespread ignorance about TB is also a reflection of people’s beliefs in the communities. Most patients admitted that they never knew they had the disease until they were enrolled for treatment in a DOTS facility. This finding corroborated the result from the Knowledge, Attitude and Practice (KAP) survey conducted in six states selected from each of the six geo-political zones of the country in 2012. Survey results revealed that only 27% of respondents surveyed knew the cause of TB (National TB Knowledge, Attitude and Practice (KAP) survey, 2012). This is a slight increase over the baseline figure of 19.5% (p<0.05), conducted in 2008 Survey.
Apart from this, there were also several misconceptions about TB which point towards ignorance and lack of adequate knowledge about the disease. This is dangerous and may fuel stigma and discrimination. As a result, those with TB symptoms may be tempted to avoid taking measures that will reveal their identity, and regrettably, may prevent them from seeking treatment at appropriate place. The reported delays in seeking TB therapy from appropriate facilities may not be unconnected with ignorance about the disease. Furthermore, where availability of TB treatment services is obtainable, due to lack of knowledge about the disease, TB symptoms are mistaken for other ailments such as malaria, typhoid and ordinary cough and consequently, many potential TB cases may be missed.
Based on experiences shared across the 12 FGDs, the period of TB treatment is a trying one that requires every support that TB patients could receive to adhere to treatment regimen. The period is characterized by several challenges, including difficulties in swallowing some of the drugs, considered to be too big in size, associated with nausea, vomiting, uneasiness and loss of appetite, especially during the 2-month intensive phase of TB treatment. However, these unfavorable experiences in TB patients’ perspective, begin to subside even as initial TB symptoms weakens due to treatment effect and also coupled with effective treatment support from patient’s family members, treatment supporters and the DOTS facility health worker.
Analysis of data revealed four elements that reflected patients’ perception of TB treatment support, namely: monitoring and supervision of drug administration, provision of emotional support, provision of support in feeding and provision of support in transportation.
Findings clearly reinforced the type of support required by TB patients as outlined under the following sub-headings.
Monitoring and supervision of drug administration
As part of the strategy to ensure adherence to treatment, patients initiating treatment are requested to bring someone who they trust and respect that could supervise and monitor their treatment. Interviews with DOTS staff in all the six Area Councils show that patients are given the opportunity to choose who they would like to be their Treatment Supporter. This was confirmed from the findings of the interviews conducted among TB patients and Treatment Supporters. Therefore, most of the people who act as Treatment Supporters were either related to the patient or friends of the patient family.
The quotations below were from DOTS staff description of a Treatment Supporter to a TB patient;
We need somebody who is close to you who can be with you at all time… somebody that will support your treatment, to help you to make sure you’re taking the drug at the time you should take it, and also to help you so that you will eat, small at frequent intervals so that you’ll be able to recover what you have lost (body weight). Female DOTS Staff, Gwagwalada.
The person should be close, either they are living in the same household or it’s a walking distance or they are living in the same complex or living in the same community. Male DOTS Staff, Kuje.
These characteristics put an enormous burden of care on treatment supporter who is expected to ensure that the patient takes his/her drug regularly and on schedule; and monitors the level of drug usage to ensure constant availability even when the patient is incapacitated. Interestingly, TB patients themselves acknowledged the need for someone to encourage or persuade them to adhere to the treatment regimen, especially when some measure of relief sets in. Some of the patients reported that they were discouraged from discontinuing treatment by their Treatment Supporters. The comments below corroborate the ideal Treatment Supporter’s responsibility to a TB patient.
When it is time to take my medicine, even when am sleeping, my husband will wake me up. Female TB Patient, Kuje
The drugs are with me. That is the normal thing I do. I collect the drugs and I give it to the patient. l give him a cup of water and she swallows them in my presence. Male Treatment Supporter, Gwagwalada
As for me, honestly there is nothing they have not done for me, my Treatment Supporter is trying his best, because if I can call him that my medicine is almost finished; before you know it, he comes to get another blister for me…most of the time, he comes on Saturdays, when he’s supposed to be resting or doing other things and be normally care for me and ask how I am doing, whether the situation is getting better or not. Male TB Patient, Kwali
He helps me a lot to the extent that if my drugs is to finish tomorrow, he would call me to remind me saying: ‘someone has called from Asokoro Hospital to remind you that your drugs will finish tomorrow, please come before you finish the one with you’. Male TB Patient, Asokoro
In order to obtain their perception about treatment support, Treatment Supporters and DOTS staffs were asked to describe what it entails to provide such a support and how effective it has been. From the point of view of DOTS staff, having a Treatment Supporter is essential for adherence. Left on their own, patients may not be committed to taking their drugs according to the treatment regimen. But with a treatment supporter, they are encouraged, persuaded and reminded of the un-wholesome consequences for missing their drugs. This support enables them to adhere to the treatment regimen. Supporting a patient at times requires collecting the drugs on behalf of the patient when he/she is not able to make it to the DOTS centre. In some cases, the Treatment Supporter may have to be called unplanned to attend to patients. This suggests that a Treatment Supporter must have the quality of providing care though may not be a trained health worker.
The following statements corroborate this finding:
If the patient didn’t see me, he will say they should go call me and immediately they will call me. If they call me, whatever the support he needed by that time I will just give. Female Treatment Supporter, Kwali
Giving support to the patient means I have to talk with her on how she takes her drugs, I have to be around most of the times to look over her, to watch over her. I have to tell her the time she is supposed to come for her checkup, that’s after 2 months, 5 months and 6 months, I’m always there to take care of her. Then I tell her a way to prevent her family members from getting the disease. Female Treatment Supporter, Gwagwalada
Apart from monitoring and supporting patients to take their drugs, the Treatment Supporter also gives emotional support to reinforce his/her efforts. Patients, from the point of view of Treatment Supporters, need to be encouraged and spoken to in comforting words to enable them complete their treatment.
If I want to take TB drugs, I will just pretend and hide the drugs, but thank God that my Treatment Supporter will see it and complain and that is why I will now take the drugs. Male TB Patient, Abaji
Yes, my Treatment Supporter use to remind me through my telephone… Male TB Patient, Asokoro
Providing emotional support
Most TB patients considered taking their drugs as drudgery, complaining bitterly about the size of the drugs which they considered too big to swallow. Therefore, they need a lot of emotional support in form of encouragement, persuasions and reassurance of quick recovery to adhere to treatment.
Patients cherished and value motivations received from their Treatment Supporters, DOTS staff and members of their immediate families. Regarding motivations from health care workers, patients believed that dispensing drugs and managing them clinically is not enough; the disposition of the health care worker to patients is as important as the drugs being administered. That is, effectiveness of TB therapy begins with the attitude of health care workers they interact with in the first place. While respondents were full of appreciation for some DOTS staff for their care and support during treatment, they castigated other health care workers, especially nurses in secondary level facilities, for their unfriendly attitude to them.
After their interface with the DOTS provider, the next source of care for most respondents was their immediate family members. Responses from TB patients revealed that their family members have been supportive and this has aided their quick recovery. They enumerated the receipt of material, financial and emotional support received; some specifically mentioned the invaluable emotional support provided by their close relatives such as from parents, spouses and siblings. Effective support received by some patients from their family links, may have informed the pattern of participants views as stated in the statements stated below:
Whenever I am seating lonely and quiet, my husband usually comes to me and asks: ‘why am I seating quiet, am I alright? And whenever my drugs are finished, he goes and gets them for me and he advises me to take the drugs. Female TB Patient, Kwali
Ever since I started this cough, I have not done anything by myself. My aunt is the one cooking for me. She is the one doing everything for me. She takes me out sometimes, and then if she sees that I am not happy, she talks with me to make me happy”. Male TB Patient, Bwari
For me it was very traumatic to start taking drugs I have not been used to… but I got so many encouragements, people around me, my pastor’s wife, she had such experience herself, they tried to tell me that it will stop, …though even here they told me that when I started taking my drugs it will stop. And probably to be frank, if not for their own encouragement and everything, I would have stopped; because this is my last month, I wouldn’t have taken it this far, I would have stopped, but they encouraged me that I had to complete the period of medication”. Female TB Patient, Asokoro
Feeding support
According to TB patients, appetite for food increases with the in-take of TB drugs. Unfortunately, for some, having to factor in the additional expenses on food in addition to other burden of care is a big challenge. In a situation where the patient could ill-afford the extra demand for food; socio-economic support is needed at that stage. Inability to meet demands for food creates a disincentive to continue with the use of the drugs. Some would not like to take the drugs fearing that it would lead to an increased appetite for food which they could not afford.
Treatment Supporters and DOTS staff reported that in such cases, there is need for intervention to either provide money to buy food or seek for assistance from willing members of the community to cover the gap. A DOTS staff reported how she had to promise a patient supply of food before she was convinced to take her drugs.
When you take this medicine, it makes you eat, and sometimes is hard for me to get money to buy. Sometimes, food is available in the house but no money to buy other ingredients”. Female TB Patients, Bwari
The support I provided is that, even sometimes I have to give patients money. Some patient will come here, they have not eaten, they don’t have money for transport and they don’t have anything to eat, so many times I give money to patients to go and eat. One time, a patient almost nearly collapsed in my office. I asked him; what is the problem? He said he has not eaten since morning. Female DOTS Staff, Gwagwalada.
Provision of money for TB patients transportation to and from DOTS facility
Interviews conducted with some DOTS staff provided some insights into patients’ challenges with transportation. Although TB medication is free, the burden of transportation cost to and from the DOTS facility for drug resupply and follow up appointments on a weekly basis is a challenge for some patients. It was found that those who live far away from DOTS facilities are more likely to complain about transportation cost.
Those Patients, who were not able to afford the transportation cost to and from the facility, have to rely on the generosity of DOTS staff and Treatment Supporters, from time to time during the period of their treatment. The following quotations supported this finding:
The only thing is that, there are occasions when I will not have money for transportation; so I have to walk down to collect drugs because I don’t want to miss the date of my scheduled appointment. So, I normally undergo difficulty in trekking down to this facility and back home. Female TB Patients, Bwari My difficulty is getting transportation to get to this place (DOTS centre). I will go and meet my brother to tell him that I am supposed to go and take drugs then he will find me some money for transportation. Male TB Patient, Asokoro
The challenge of meeting transportation cost for routine visit to TB treatment centre by TB patient for their drug refill, has given rise to drug re-supply in advance, to minimize the frequency of visits to the health facility. This development was due to the low economic class to which majority of the TB patients belong. If real DOTS is to be practiced, TB patients will have to visit DOTS site on a daily and regular basis; but the Treatment Supporter will have to provide a bail-out for the attendant transport costs.
Treatment support and defaulting in TB treatment
Interviews with Treatment Supporters and DOTS staff provided opportunity to explore the different factors that may be responsible for defaulting TB treatment. The findings revealed different factors that could be responsible for defaulting in TB treatment. Interestingly, they include: long duration of treatment, lack of close supervision and monitoring, difficulties involved in swallowing of drugs which are considered to be too big in size by some TB patients, and inability to meet financial burden required for obtaining TB treatment, which are connected with feeding and transportation costs to and from DOTS centers.
An important inference that was drawn from these findings is a correlation between treatment support and defaulting in TB treatment. Meaning that, where the elements of treatment support mentioned above are lacking, poor adherence to medication is a likely consequence leading to treatment default.
As soon as patients begin to feel better after two months of treatment (the intensive phase), they feel they are well enough and don’t have to continue taking their drugs. At this stage, the intention to default begins to set in, however with persuasions and threats from their Treatment Supporters and DOTS staff, patients are encouraged to persevere to complete their treatment.
In order to reduce the incidence of defaulting by patients, Treatment Supporters and DOTS staffs were asked to share strategies they have devised and adopted. The main strategies mentioned are; close supervision and monitoring of drugs intake, as well as taking of inventory of TB drugs with patients. However, for a more effective supervision, some believed that managers of TB programs need to introduce home visits by DOTS staff. The justification being that, patients need to be followed up, encouraged or persuaded to continue and complete treatment.
Effectiveness of treatment support
Going by opinions and views from TB patients on their experiences during their TB therapy, it can be safely asserted that the treatment support they received from members of their immediate family, Treatment Supporters and DOTS personnel, have been largely effective.
However, treatment support seems to be more effective where TB patient have maximum emotional and physical support from members of their family. This underscores the importance of selecting a family member as Treatment Supporter at the initiation of TB treatment. Although, this study did not explore preference between types of Treatment Supporters, a similar finding has been documented in a study on impact of treatment supporters in Pakistan (Soomro et al., 2012).
RECOMMENDATIONS AND IMPLICATIONS FOR TB PROGRAM DESIGN
In the light of the above inferences drawn from views and opinions of majority of respondents, an effective treatment support is required for the patients to adhere strictly to treatment regimen for treatment success to be achieved.
Experiences shared by TB patients revealed that the treatment support they received from family members, their Treatment Supporters and the DOTS facility personnel has been effective. Most patients acknowledged that their ability to sustain the treatment until the present study was largely due to the quality of treatment support they got.
This study highlights the importance of patient-centered approach to TB treatment and underscored the TB patients’ need for someone who can provide assistance for patients’ drug in-take, and the needed emotional and material support. From the data generated from this study, TB patients’ understanding of treatment support was mainly for:
1) Close monitoring of TB patients to ensure adherence to taking of drugs.
2) Provision of emotional support in terms of providing encouragement, persuasions and reassuring the patient of his/her ability to complete treatment and get cured.
3) Provision of food to meet up with increase in appetite engendered by drug taking.
4) Provision of assistance in transportation to and from DOTS facilities for routine visits to collect drugs and for subsequent follow up visits.
Based on the findings from this study, the following are being recommended to further enhance the control of TB in Nigeria and in other African countries.
Need for public enlightenment on TB
In the light of general lack of awareness and knowledge about TB, even as acknowledged by the three categories of respondents, there is need for comprehensive public enlightenment on diseases’ cause, symptoms, means of transmission and preventions measures. While designing public enlightenment activities, it would be suggested that behavior change communication strategies specifically targeted at the individual, family, community and policy makers be designed.
An integral part of communication strategy should be community mobilization. It is expected that through this, members of the community would be sensitized to complement government efforts and development partners in providing treatment support for TB patients, especially concerning their emotional, material and financial needs as highlighted in this paper.
Motivation
Findings from this study revealed the need to motivate TB patients, Treatment Supporters and DOTS staff. Evidence abounds to show that indigent patients may not be able to meet with the financial needs for transportation and feeding required during the period of treatment. In the light of this, some form of incentives needs to be put in place to motivate these individuals to ensure effective treatment support of TB patients.
Creation of more DOTS facilities
The findings from the study imply that some patients live far away from DOTS facilities and as a result, visiting the DOTS center for TB drug re-supply and follow up becomes a burden. The DOTS staff from Abaji and Gwagwalada Area councils confirmed this challenge. Therefore, more DOTS facilities would need to be created especially in communities where the prevalence of TB appears to be high. By so doing, accessibility to DOTS facility would be facilitated for TB patients and other presumptive TB cases that are yet to be detected.
Interpersonal communication skills
Most TB patients found DOTS facility personnel friendly and supportive. Some of them believe that the healing process begins from interactions with a friendly DOTS staff. Therefore, nurses and other frontline health workers need to be trained on interpersonal communication especially concerning to dealing with TB patients. It would also be suggested that behavior change communication materials be designed specifically for health care workers.
It is strongly believed that implementation of aforementioned measures would also stem the tide of defaulting in TB treatment.
Although TB drugs are free in Nigeria and Treatment Supporters are being engaged to support TB treatment, TB patients’ support needs should be part of the design of Community TB care.
Findings from this study revealed that the TB treatment burden is borne between DOTS staff, Treatment Supporter and patients. Although the study shares almost the same objectives with similar studies reviewed, it has revealed the importance and effectiveness of a patient-nominated Treatment Supporter and patient-centered approach to TB therapy.
As acknowledged by the three categories of respondents for this study; TB patients, Treatment Supporters and DOTS staff, the period of TB therapy is a demanding one for TB patients. More so, for those who belong to lower socio-economic class. Thus, it is difficult for the majority of TB patients to cope with financial demands of therapy. The burden is worse for patients taking into consideration the stigma and discrimination they have to contend with in an environment of limited or no knowledge about the disease.
Information gathered from the three categories of respondents, especially Treatment Supporters and DOTS staff, revealed that where the four elements of treatment support mentioned above are lacking, patients are likely to contemplate and to ultimately default on treatment. Some patients acknowledged that if not for the effective treatment support they received, they would have defaulted on treatment. The implications of this finding is that, left on their own, TB patients may not be committed to taking their drugs and complete their treatment regimen, if any of the supports highlighted in this study is lacking when needed. Patients with Treatment Supporters who offer these supports tend to complete their treatment regimen and not likely to default.
The authors have not declared any conflict of interests.
REFERENCES
|
Christopher PL, Newell JN (2009). Improving Tuberculosis care in low income countries – a qualitative study of patients' understanding of "patient support" in Nepal.
View
|
|
|
|
Crosby RA, DiClemente RI, Salazar LF (2006). Research Methods in Health Promotion. Jossey –Bass, San Francisco.
|
|
|
|
Global TB Report, 2014.
|
|
|
|
Global TB Report, 2015.
|
|
|
|
Global TB report, 2016.
|
|
|
|
John Hopkins Centre to Eliminate Cardiovascular Health Disparity (2015). Family and Social Support. Retrieved on July 12th, 2015.
View
|
|
|
|
Nachega JB, Knowlton AR, Deluca A, Schoeman JH, Watkinson L, Efron A, Chaisson RE, Maartens G (2006). A qualitative study on Treatment supporter to improve adherence to antiretroviral therapy in HIV-infected South African adults.
View
|
|
|
|
Nachega JB, Richard E, Chaisson RG, Anne E, Mohammad AC, Malathi R, Chelsea M, Hennie S, Amy RK, Gary M (2010). Randomized Controlled Trial of Trained Patient-Nominated Treatment Supporters Providing Partial Directly Observed Antiretroviral Therapy.
View
|
|
|
|
National Population Commission, Nigeria (2006). Nigerian 2006 Census Report, retrieved on February 1st, 2017.
View
|
|
|
|
National Population Commission (NPC) [Nigeria] and ICF International (2014). Nigeria Demographic and Health Survey 2013. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International.
|
|
|
|
National TB Knowledge (2012). Attitude and Practice (KAP) survey Federal Ministry of Health, Nigeria.
|
|
|
|
Soomro MH, Ejaz Q, Khan MA, Mokve O (2012). Treatment Supporters and their impact on Treatment Outcomes in Routine Tuberculosis Program Conditions in Rawalpindi, Pakistan.
View
|
|
|
|
Sotirios S (2003). Social Research, 2nd edition, Macmillan Publishers Ltd, Australia.
|
|
|
|
The First National TB-Prevalence Survey in Nigeria (2012). Federal Ministry of Health, Nigeria.
|
|
|
|
World Bank Report on Poverty in Nigeria (2014).
|
|
|
|
World Health Organization (2001). The five elements of DOTS.
|