Full Length Research Paper

ABSTRACT
Although infant and young child feeding practices play an important role in reducing early childhood morbidity and mortality, very large proportions of women do not practice optimal breastfeeding and complementary feeding for their children in Ethiopia. Till date, none has addressed the supply and demand side factors that influence infant and young child feeding practices (IYCFP). This work aims to assess supply and demand side factors that influence infant and young child feeding. A community based cross sectional study was employed involving quantitative and qualitative methods among sampled mothers with children under 24 months in Gibe District Southern Ethiopia. Qualitative data were collected through in-depth interviews and focus group discussion, and analyzed through a thematic analysis approach. Quantitative data were entered into Epi-data 3.1 and then exported to SPSS 21. Bivariate and multivariate logistic regression was used. Prevalence of inappropriate infant and young child feeding practice was 67.9%. Being government employee of husband [AOR = 4; 95%CI: 1.65, 10.04], lower income status [AOR = 3.1;95%CI:1.36, 7.07], not attending ANC (AOR = 2.03 (1.22, 3.36)], child age 0 - 5 months [AOR = 2.4;95%CI:1.02, 5.72], negative attitude of mothers towards IYCFP [AOR = 2.35 (1.44, 3.84)] and number of children 3-4 [AOR = 1.99;95%CI:1.08, 3.64] were predictors of inappropriate IYCFP. There is high prevalence of inappropriate infant and young child feeding practice in the study area. Interventional initiatives should focus on improving socio-economic status, and access to information, education and communication for improvement of IYCFP.
Key words: Infant and young child feeding practice, supply side factors, demand side factors, Ethiopia.
INTRODUCTION
Infant and young child feeding is the exclusive breast-feeding of children <6 months of age, early initiation of breastfeeding, non- use of bottle feeding, minimum meal frequency, minimum dietary diversity, timely introduction of solid, semi-solid and soft foods in 6-8 month-old and breastfeeding. Indicators for infant and young child feeding practice (IYCFP) utilized in this study on the basis of literature review on World Health Organization (WHO) IYCF indicators includes; initiating breastfeeding (BF) within one hour of delivery, exclusive (BF) for the first six months, introduction of solid, semi-solid and soft foods in 6-8 months of age, minimum dietary diversity, minimum meal frequency and continued breastfeeding for 2 years (WHO/UNICEF, 2016)
The cornerstone of care for childhood development is Infant and young chibreastfeedingld feeding. The first two years of life provides a critical window of opportunity for ensuring children’s appropriate growth and development of children from generation to generation through optimal feeding. Any damage caused during infancy and young age can lead to impaired cognitive development, compromised educational achievement, low economic productivity and malnutrition since the first two years of a child’s life is the most vital for establishing healthy growth. Once growth faltering occurs in this age, there is little opportunity for catch-up growth (WHO/UNICEF/USAID/FANTA/IFPRI, 2014a; WHO/UNICEF/USAID/FANTA/IFPRI, 2014b)
WHO and UNICEF’s recommendations for optimal IYCF are early initiation of breastfeeding within one hour of birth, exclusive breastfeeding for six months and nutritionally adequate and safe complementary feeding starting from the age of six months with continued breastfeeding up to two years of age or beyond. WHO also has developed indicators (eight core and nine optional) to assess infant and young child feeding practices (WHO/UNICEF, 2016; WHO/UNICEF/USAID/FANTA/IFPRI, 2014b; Kramer, 2002)
Worldwide, IYCF associated problems in 2015, 156 million children under 5 were estimated to be stunted, 50 million were estimated to be wasted, and 42 million were overweight. About 43% of infants 0–6 months old are exclusively breastfed. Few children receive nutritionally adequate and safe complementary foods; in many countries less than a fourth of infants 6–23 months of age meet the criteria of dietary diversity and feeding frequency that are appropriate for their age (PAHO/WHO, 2001; WHO/UNICEF, 2016). Over 800 000 children's lives could be saved every year among children under 5 years, if all children 0-23 months were optimally breastfed. Breastfeeding improves intelligence quotient (IQ), school attendance, and is associated with higher income in adult life. Improving child development and reducing health costs through breastfeeding result in economic gains for individual families as well as at the national level (WHO/UNICEF, 2016; Bank, 2016). Directly or indirectly, malnutrition has been responsible for 60% of deaths annually among children under five. Well over two-thirds of these deaths, which are often associated with inappropriate feeding practices, occur during the first year of life. Because poor feeding practices are a major threat to social and economic development, they are among the most serious obstacles to attaining and main-taining health that face this age group (WHO/UNICEF, 2016; Kimani-Murage, 2011).
Despite reduction of under nutrition being one to achieve SDGs goal, it continues to be a great public health concern in many developing countries, particularly in sub Saharan Africa (Department, 2014). Over 1/3 of under-five mortality is caused by malnutrition related to inadequate complementary feeding (Department, 2014; Kibebew, 2012). In general, poor complementary feeding practices means that many children continue to be vulnerable to irreversible outcomes of stunting, poor cognitive development, and significantly increased risk of infectious diseases leading to gastroenteritis, diarrhea and acute respiratory infection (Ministry of Human Resource Development DoWaCD, 2004). Nationally, 10 percent of Ethiopian children are wasted, and 3 percent are severely wasted and 44 percent of children under age five are stunted, and 21 percent of children are severely stunted (Jones, 2014; Bahl et al., 2015).
From EDHS (2016), about 58% of children less than 6 months old are exclusively breastfed but complementary foods are not introduced timely for all children. Only about half of children receive complementary foods at 6-9 months. Overall, only 4 percent of 6-23 months children are fed appropriately, based on the recommended IYCF practices. It is also documented that poor infant feeding practice which is poor breastfeeding and poor complementary feeding contributes to 24% of infant deaths (Jones, 2014; International CoEaI, 2011; Tamiru et al., 2013).
Composite variables of infant and young child feeding index based on key indicators identified by WHO are not studied in Ethiopia; there is limitation of studies that address the supply and demand side factors that influence the infant and young child feeding practices and associated factors in the study area. Therefore the study will fill the gap and provide clear findings regarding the magnitude of IYCF practices in Gibe District among infants less than 24 months of age.
MATERIALS AND METHODS
Study setting and sampling procedure
The study was conducted in eight kebeles in Gibe District, Hadiya Zone, SNNPR, Ethiopia from March 13th to April 13th 2017. The 8 kebeles were randomly selected from the 22 kebeles in the district. A community based cross sectional study was employed involving quantitative and qualitative methods. The sample size was estimated using a single population proportion formula based on a study from northern Ethiopia (Kedir, 2016) that showed estimated proportion of children that achieved adequate/minimum dietary diversity is 22.2%.The following assumptions was used at 95% confidence level, 80% power of the test and 5% margin of error. In addition 10% non-respondent rate was added and since the sampling technique was multi stage sampling, design effect of 1.5 was used. The total sample size was determined to be 434. First, the sample size was proportionally allocated to each kebele based on total number of mothers with 0-24 months child. Study participants were selected by systematic random sampling techniques. Lists of children < 24 months old were prepared by Health Extension Works (HEWs) from family registration book and used as a sampling frame. For the qualitative part data were collected using FGD guide and in-depth interview guide. The participants for the in-depth interview were key informants who were selected purposively based on the assumption that they have more prior information on the issues. Interviews with HEWs, health professionals, Traditional Birth Attendant (TBA), religious leaders, breastfeeding mothers, and grandmothers were carried out inde-pendently. Key personnel such as OPD heads and health center administrators were involved in in- depth interview while FGD was used for respondents who were not included in quantitative study.
Questionnaire was validated by the World Health Organization (WHO) and different literature and adapted to include context-specific factors (WHO/UNICEF/USAID/FANTA/IFPRI, 2014b; Kramer, 2002; DHS-Yemen National Health and Demographic Survey 2013). Data were collected using a structured questionnaire, administered in-person by 8 nurse midwives who had experience in data collection. Socio-demographic characteristics, mothers’ knowledge and attitude towards IYCF, maternal and child health status, mother’s health service utilization, mothers’ obstetrics history, breast-feeding practices, complementary feeding practices, maternal health service use characteristics, support and source of information for IYCF practices parts were collected. The questionnaire was prepared in English, translated to Hadiyyisa, and back-translated to English separately by two individuals to ensure consistency. Collected data were checked for consistency and completeness. Incomplete questionnaires were returned to interviewers for completion.
Data analysis
Data were analyzed using SPSS 20. Bivariate and multivariate logistic regression analyses were used to determine the association between independent and dependent variable. Variables with p<0.25 in bivariate analysis were entered into a multivariate logistic regression model. Odds ratio with 95% confidence were computed to identify the presence and strength of associations at p<0.05 level of significance. Final model was checked using the Hosmer–Lemeshow goodness of fit test. Cofounders, interaction and multi-collinearity were checked to minimize bias. Qualitative data were analyzed manually using thematic analysis.
Ethics statement
Study protocol was approved by the Institutional Research Review Board of Jimma University’s, Institute of Health Science and Community Services Ethical Review Committee. Permission was obtained from Hadiya Zone Health Department, Gibe District Health Office and participating kebele. Informed verbal consent was obtained from participants prior to enrollment in the study. Participation in the study was voluntary and participants were informed of the right to withdraw from the study. Data collection was conducted confidentially and data were de-identified, de-linked and stored in a secure location.
RESULTS
Socio-demographic characteristics
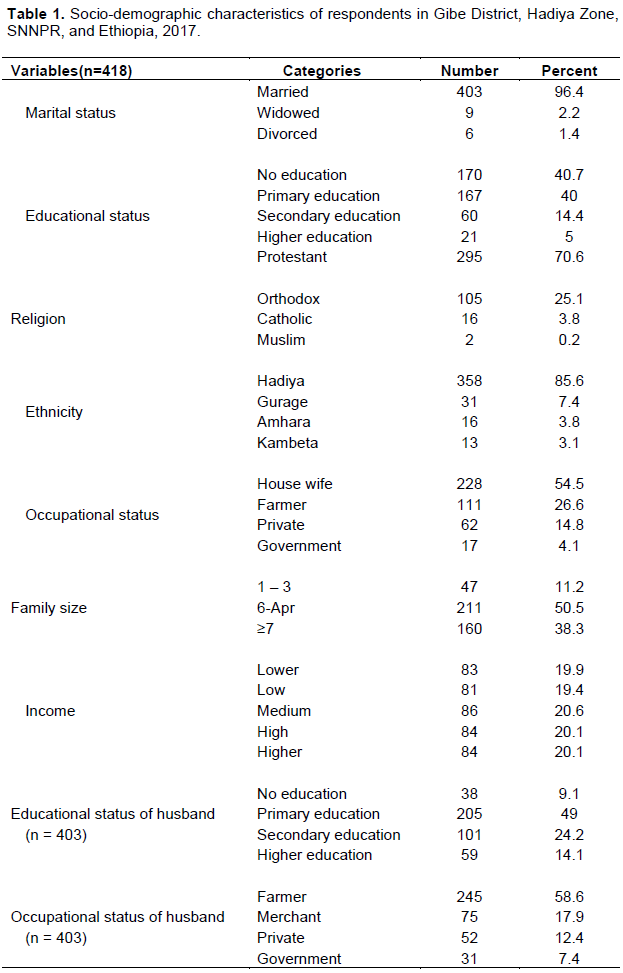
A total 418 of mothers and caregivers of children less than 24 months were included in the study with response rate of 96.3%. The mean age of the mothers was 30.72 years (SD±6.4) and ranges from 19 to 47 years. More than half 228(54.5%) of the mothers were housewives, and 111(26.6%), farmers. Regarding mothers’ educational status, 170(40.7%) of the mothers did not have formal education and 167(40.0%), primary education. Most of the respondents were Hadiya by ethnicity (85.6%), Protestant by religion (70.6%). More than half 211 (50.5%) of the households had a family size of four to six and the median family size was six. Regarding wealth index one to five (20.6%) of the respondents were in 3rd quartiles (Table 1). Regarding husbands’ education level, 205(49.0%) and 101(24.2%) of them had primary education and secondary education respectively, whereas 245(58.6%) were farmers by occupation.
Child characteristics
More than half 219(52.4%) of the children were females and more than one-third 138 (33.0%) of them were 6-11 months old. More than two in five (65.8%) of the children were second to fourth in birth order. About one-third of the children (75.8%)’s birth intervals between youngest child (index child) and their immediate older were less than 24 months (Table 2).

Maternal health services use characteristics
A total of 265(63.4%) mothers attended antenatal care. Most of the mothers (35.5%) had antenatal care follow up at least once during their last pregnancy. Only 20.8% attended three-four focused ANC as recommended and during ANC follow up one-third (76.4%) of mothers did not receive information about IYCFP. Majority 396 (94.7%) of the mothers had spontaneous vaginal delivery. With respect to delivery assist, only 144 (34.4%) mothers gave birth by the assistance of skilled health professionals, 270 (64.6%) gave birth at home and 35.4% of the mothers gave birth to their index child at a health institution. Most 296 (70.8%) of mothers did not have PNC. Many of them (38.5%) had three-four children. Most 369 (88.3%) of the mothers were multi-porous with mean of 4.2 live births and the mean of the total number of children they had was 3.96 (Table 3).

Breastfeeding practices
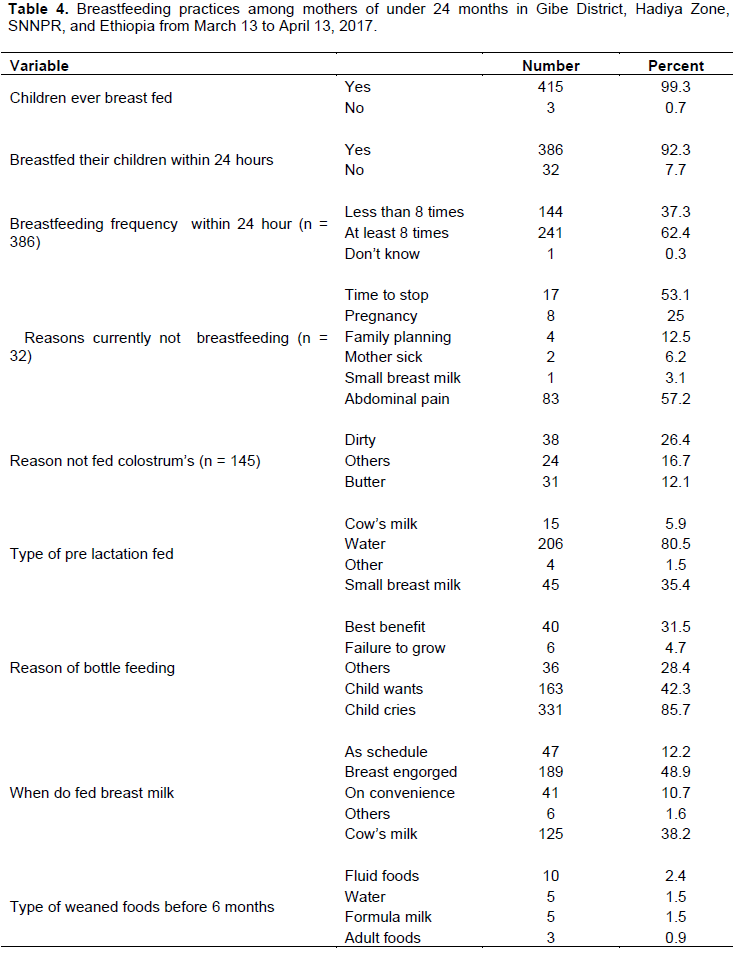
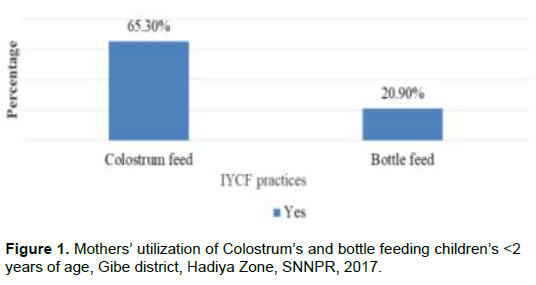
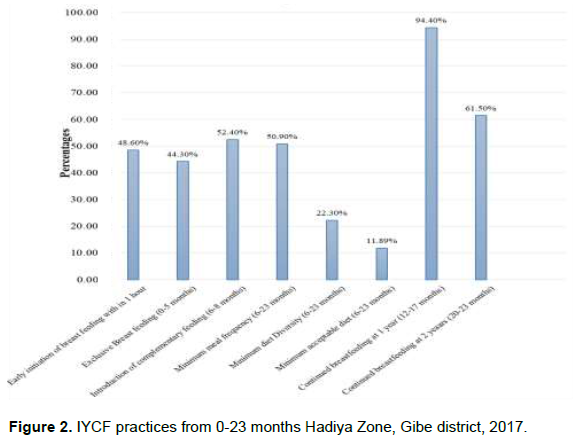
Almost all the mothers 415 (99.3%) had ever breastfed their children. Among the mothers who are currently breastfeeding, 386 (92.3%) breast-fed their children within 24 h preceding the survey. Among mothers who were not breastfeeding their children currently, more than half (53.1%) reported that they stopped breast- feeding because it was time to stop (Table 4). Slightly less than half of the mothers 203 (48.6%) initiated breast- feeding within the first hour of delivery. Two-thirds 273 (65.3%) of the mothers gave colostrum to their infants. Over all exclusive breastfeeding for age groups (0-5 months) was 185(44.30%). The study also showed that 207 (49.5%) mothers provided pre lacteal foods for their babies. More than half 331 (79.1%) of the mothers did not feed their children using bottle. Nearly 8.9% of the total bottles fed infants were put on the bottle at an age less than a month and 12% of them between 3-4 months (Figure 1).
Most of them stated that “Every infant should be provided with “Tenadam “before starting breastfeeding, because it protects the infant from the “evil eyes “of other people.” Almost all stated that “we provide “tenadam” with water for infants for two basic reasons: the “tenadam” cleans their mouth and stomach and we give water because the breast milk is salty, thus, the baby will be thirsty.”
Most mothers breast-feed when the child cries 332 (86.0%). For the frequency of breast-feeding for those mothers who were currently breastfeeding, 241(62.4%) of them reported that they breastfeed at least 8 times per day. The proportion of children aged 6 - 23 months who were predominantly breastfed was 183 (56.8%). For types of additional foods introduced before 6 months, 125 (38.2%) of them introduced cow milk and 10 (2.4%) fluid foods (Table 4). Out of 125 mothers who had children age 12 - 17 months, almost all [118 (94.4%)] of them continued to breastfeed their children until the end of the first year. However, among 65 children aged 18 – 23 months, 40 (61.5%) mothers continued to breastfeed until the end of two years.
Complementary feeding practices
Mothers practice of complementary feeding assessed in this study included: the practice of timely initiation of liquids, semi-solids and soft foods, dietary diversity, minimum meal frequency and use of bottle with teat to feed children semi-solids and liquids. The mean age for introduction of solid, semi-solid and soft foods was 5.6 (SD ± 0.9) months. A total of 172 (52.4%) mothers introduced complementary food by 6–8 months, 167(50.9%) received the recommended minimum meal frequency, 73 (22.3 %) received the recommended minimum dietary diversity and only 39 (11.89%) received the recommended minimum acceptable diet and 216(65.8%) did not meet the requirement (Figure 2).
Optional breast-feeding indicators and core IYCF indicators
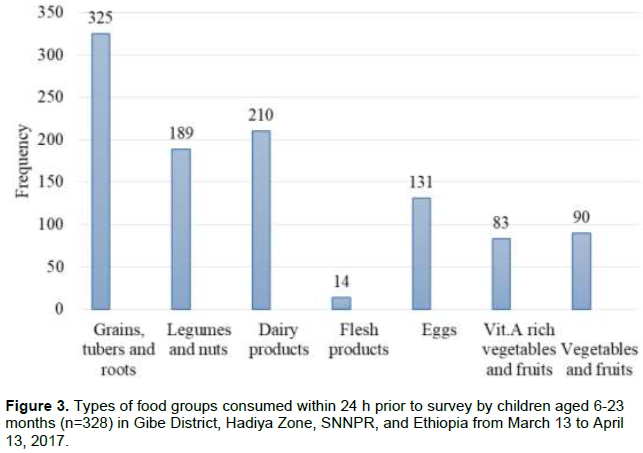
The primarily food source (99.1%) of children aged 6 - 23 months were grains, tubers and roots, followed by dairy products (64.0%); whereas very smallest number (4.3%) of children were provided with flesh products (Figure 3). Most of the mothers stated that “Even if it is available, we don’t give meat to children below the age of five years. If children start to eat meat at earlier ages, they will share with adults and want to eat more. We get meat once a year during Mesikel holiday.” Vegetables and fruits are not common in children’s diet. Almost all responded that “If children get a variety of fruits like mango and, papaya and if they also get cow milk and breast milk, they will be healthy.” “We are not giving them any fruit...therefore most of them are not strong and healthy.” …”In this area it’s cold and there is hunger.’’ Garlic and herbs like rue were reported given for treatment of abdominal cramp.
Most of them stated that “Children start eating egg after 1 year. It predisposes the child to diarrhea and vomiting if given before this age.” “We do not give cabbage to children less than two years old; it will cause worms in their stomach.” “We don’t give meat to children below 5 years because they can not chew and swallow meat at this age. I will give roasted meat after the age of 5 years”.
Health extension workers (HEWs) have different opinions on feeding a variety of foods to children. HEWs have concerns about the availability of certain grains, fruits, and overall income to feed variety of food to children. “Families cannot afford them. They can only make the porridge from what they have. It is hard because of poverty” (Hadaye, HP). “I think mothers can do this if they are advised. If they are aware of this and if they can sell what they have at home to buy other foods, they can do it. It does not require much time and money, and it is easy if the different grains are available at home” (Ratesh, HEW at HPA).
The role of health workers, opinion leaders, traditional communicators, NGOs and grandmothers in supporting mothers to adequately feed their infants has been highly valued in the area. In addition, increased workload of women, maternal illness or death after delivery, breast milk insufficiency and the involvement of grandmothers, husbands, friends and other family members play an influential role in the early introduction of complementary foods to infants. Also, mothers’ socio-economic status, culture and tradition have been found to have an influence on early introduction of complementary foods. This study presents an analysis and summary of the data collected during the course of the explorative research conducted in the study area.
Knowledge and attitude of mothers towards IYCFP
Out of the total of 418, 339 (81.1%) respondents had sufficient knowledge about IYCFPs. Out of 418 respondents 189 (45.2%) had positive attitude towards IYCFP.
Infant and young children feeding practice status
Indicators used to construct comprehensive infant and young child feeding practices to classify into appropriate and inappropriate feeding were: exclusive breastfeeding, timely initiation of breastfeeding, bottle feeding, timely introduction of solid, semi-solid and soft foods, minimum food diversification, minimum meal frequency and continued breastfeeding. Based on the above indicators of IYCFPs, 284 (67.9%)[95% CI; 63.6-72.5] of under 24 months children were fed inappropriately (Figure 4).

Source of drinking water
Almost more than half of mothers get drinking water from well 312(74.6%), but only 11.5% of mothers use by boiling; majority of them use simply by storing. Most of the mothers 52.3% >1h walk to get maternal and child health services at health institutions.
Support and source of information for IYCF
This study assessed the support mothers received for IYCF practices and the findings are depicted as; key person supporting through words of praise, providing reassurance and opportunity to discuss IYCF. About more than a third (73.7%) of the mothers cited the child’s father and Health worker (14.6%) as key persons who supported BF through praising them for their efforts. The mother-in-law provided the least (4.1%) words of praise to mothers in support of IYCF.
Slightly less than half 137 (32.8%) of the mothers cited health workers as the persons who provide reassurance on mothers’ practice of breastfeeding. Own mother accounted for 4 (1.0%), child’s father 237 (56.7%), mother in law 39 (9.3%), friend 1(0 .2%) and 33 (8.8%) of the mothers had no one to reassure them of breastfeeding. About less than half 176(42.1%) of the mothers cited health workers as the persons who gave them opportunity to discuss IYCF practices, 26 (6.2%) their own mother, 132(31.6%) their child’s father, 84(20.1%) mother-in-law as shown in Table 5. These findings indicated that the health workers and the child’s father were key persons offering the mothers IYCF support.

Majority 289 (69.1%) of the mothers had not received IYCF information while 129(30.9%) of the mothers had received IYCF information. The mothers stated that the IYCF information was received from mass media (all Radio and television stations 48(11.5%), magazines 4(1%), books 5(1.2%), health professionals 196(46.9%) and others; 12 (2.9%) of the mother had received IYCF information.
Factors associated with infant and young child feeding practice status
In bivariate logistic regression, occupation, mother educational status, husband occupation, husbands’ educational status, family size, socio economic status, ANC visit, IYCF information, place of delivery, birth attendant, PNC, number of children, age of child, birth order and attitude of mothers toward IYCFP were significantly associated with IYCFP at (P < 0.25).
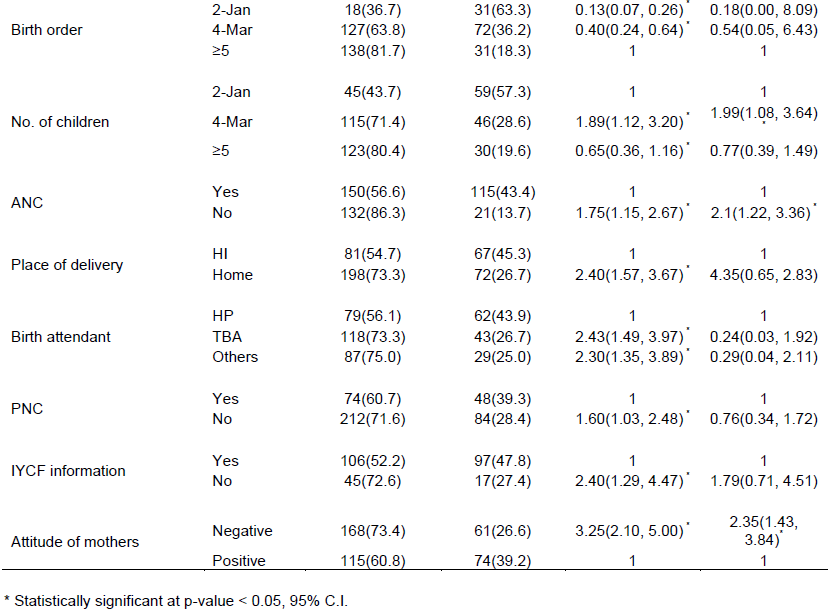
In multivariate analyses; husbands’ occupation, socio economic status, ANC, number of children, age of child and attitude of mothers were significantly associated IYCFP at P < 0.05 (Table 6).
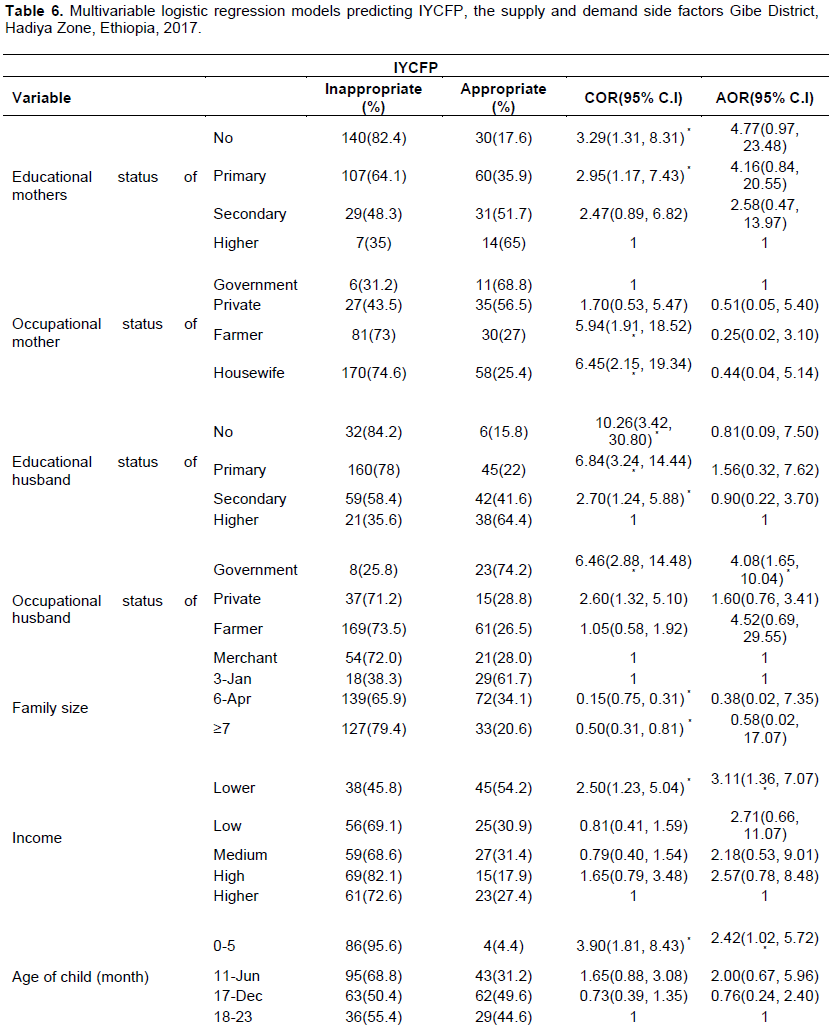
Mothers who had lower income had odds 3.1 times higher of experiencing inappropriate feeding practice [
DISCUSSION
The magnitude of inappropriate IYCFP in the study area is 67.9%, which is high. Thus, it was found that majority (99.3%) of mothers practiced ever breastfeeding, which is similar with other studies done in Mekelle city (98.9%) (Berhe et al., 2013) and EDHS (98%) (International CoEaI, 2011); while higher than study done in Arba Minch (95.8%) (Tamiru et al., 2013). The difference might be due to the fact that breast-feeding practice is common, accessible, acceptable and a norm in the society.
WHO/UNICEF discourages the use of pre-lacteal foods without being medically indicated (DHS, Yemen National Health and Demographic Survey, 2013). Bottle-feeding is not recommended because improper sanitation and formula preparation with bottle-feeding can introduce microorganisms to the infant that increases the child’s risk of illness and malnutrition (DHS, Yemen National Health and Demographic Survey, 2013) but this study found that about 20.9% of mothers fed their children using bottle. This finding is less than national data (28.5%) (International CoEaI, 2011); also lower than that of a study done in Addis Ababa (54.2%) (Shumey et al., 2013). It is found that deprivation of colostrum, duration of breastfeeding, use of pre-lacteal feeds, age of introduction of complementary feeding and method of feeding are the main factors contributing to under-five stunting (Shumey et al., 2013). The prevalence of pre-lacteal feeding in this study is 49.7% which is much higher than the study done in Mekelle town (10.4%) in 2011 (Berhe et al., 2013), in south Gonder zone (11.1%) in 2007(36) and 27% in EDHS (2011) (International CoEaI, 2011). This result may be due to the traditional practices (“wubaxe”) of introducing pre-lacteal feeding especially water (79.7%) at third day of birth for females, fourth day for males and high home delivery (64.6%) in the study. The study showed that the prevalence of exclusive breastfeeding for infants less than six months was 44.3%. This result is lower when compared with the findings from Mekelle (60.8%) in 2011 (Berhe et al., 2013) and Ethiopia (58%) in EDHS (2016) (International CoEaI, 2011). This finding is also lower than the national targets (70%) by 2015(13). From qualitative finding, “Most of the respondents stated that they used a bottle when the child is less than one year old and that they started to use spoon, cup and their hand after the age of one year.”
Prevalence of achieving the minimum dietary diversity was 22.3%, although this is higher than reported by DHS (4.8%) (International CoEaI, 2011), in Tigray (17.8%) (Shumey et al., 2013), and Ethiopia overall (10.8%) (Department, 2014); it is hardly promising that so few of these children received adequate dietary diversity. In this study, a majority of the children received a diet primarily based on staple foods (grain, roots and tubers), very few of the children received vitamin A rich fruit and vegetables, egg, and flesh foods. Legumes and nuts were more consumed by the 18-23 months age group compared to the other age groups; while other fruit and vegetables were more commonly consumed among 12-17 months age groups. With respect to dietary diversity, our study indicates that diversity of different food groups offered during the past 24 h was low, with the lowest rates reported for vitamin A rich fruit and vegetables and flesh foods. Children of 6–23 months age group go through a reasonably rapid dietary transition from exclusive breastfeeding to complementary feeding (Kimani-Murage, et al., 2013; Yemane and Gebreslassie, 2014).
Introduction of nutritionally adequate and safe complementary foods promotes growth and good nutritional status among infants and young children. This study revealed that 52.4% of children aged 6 - 8 months receive complementary foods. The finding of this study is higher when compared to EDHS (2011) (49%) (International CoEaI, 2011). This is low compared to Uganda (75%) (18), Tanzania (92.3%) (Victor, 2012) and Kenya (81%) (Kimani-Murage, 2011; Kimani-Murage, 2013), in 2010.This may be due to mothers’ knowledge on what and when to start giving additional foods to children and their perception that they are unable to digest foods at this age. “Almost all mothers have suggested that gruel and porridge should be prepared at least from two types of cereals. The age for introduction of additional foods ranges from 2 months to 8 months as indicated in the qualitative finding.
This study also showed that the majority 50.5% of children received minimum meal frequency. However, very few 22.3% children aged 6 - 23 months met the requirements for minimum dietary diversity in the previous day. This is lower than that in Tanzania; 38.0% of children received minimum dietary diversity (Victor, 2012; Kedir, 2016). Similarly in South Asia, the minimum meal frequency and dietary diversity were reported by WHO in 2010 to be less than 50% (Senarath, et al., 2012). The study finding is also high when compared to EDHS (2011) (minimum meal frequency of 4% and minimum dietary diversity (5%) (International CoEaI, 2011). This may be due to the difference used to calculate minimum meal frequency. In this study the proportion of minimum meal frequency was calculated for 6 - 23 months without considering age specific meal frequency, that is, 6 - 8 months, 9 - 11 months and 12 - 23 months. However, inappropriate infant and young child feeding practice was significantly associated with husbands’ occupation, socio economic status, ANC, place of delivery, number of children, age of children and attitude of mothers after controlling other predictors.
The observed association between low income and IYCFP is consistent with another study done in Ethiopia, Saudi Arabia (International CoEaI, 2011; Al-Hreashy et al., 2008). The possible justification might be low income mothers did not give attention to feeding their children. The odds of inappropriate IYCF practices were significantly associated with being husband government employee, which was consistent with a study done in Oromia, Ethiopia (Yonas et al, 2016). This might be because government employee does not usually stay at home, give less attention to their child and has insufficient time. Another predictor was mothers with infants in the age group 0 - 5 months, which is supported by a study done in Northwest Ethiopia (Kedir, 2016). This may be due to the fact that mothers could not exclusively breastfeed as mothers who had no ANC visit were 2.1 times more likely to experience inappropriate IYCFP; this is supported by study conducted in Axum town (Yonas et al., 2016). This
indicates that mothers who attend ANC with repeated visits might have a great chance to get maternal health related to well IYCF and child care advice. Mothers who had negative attitude towards IYCFPs were strongly associated with inappropriate IYCF, which is line with study done in Oromia, Ethiopia (Yonas, 2016). Positive attitude might enhance women to practice appropriate IYCF.
Women with 3 - 4 children are 2 times more likely to practice inappropriate IYCF compared to women with children 1 - 2. This finding is consistent with IYCFPs’ study done in Oromia Region (Yonas, 2016).
Our study has several strengths, including employing a validated and standardized questionnaire that we tested and revised. Our study also used newly implemented World Health Organization guidelines on IYCFP. Nevertheless, this study has its own limitations; differences in the measurement of the feeding practices, and the real meaning of each practice could be sources of difficulty for building and interpreting composite feeding practice, and lack of a standard definition and the variations in the methods used to construct scores were considered as limitations of this study.
CONCLUSION AND RECOMMENDATIONS
There is high prevalence of inappropriate IYCF practice in the study area. The study showed high proportion of mothers giving pre-lacteal fed, discarding colostrum and using nipple bottle for feeding.
Being a government employee, low income, lack of ANC visit, and mothers with index child age of 0 - 5 months, negative attitude of mothers and number of children (3 - 4) were all predictors of IYCFP.
Appropriate IYCF should be a high priority to build the health of future generations. Therefore; concerned bodies should give strong attention to health interventions programs to develop individuals’ ability to increase IYCFPs. Interventional initiatives should focus on improving socio-economic status, mobilizing communities and families through the media, networks such as the Women’s Forum to support IYCF practices.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
Our gratitude goes to data supervisors, data collectors, study respondents, Jimma University, and the Hadiya Zone Health Department and Gibe Woreda Health Office for facilitating the study.
REFERENCES
|
Al-Hreashy FA, Tamim HM, Al-Baz N, Al-Kharji NH, Al-Amer A, Al-Ajmi H, Eldemerdash AA (2008). Patterns of Breastfeeding Practice during the First 6 Months of Life in Saudi Arabia. Saudi Medical Journal 29(3):427-431. |
|
|
Berhe H, Mekonnen B, Bayray A, Berhe H (2013). Determinants of Breastfeeding Practices among Mothers Attending Public Health Facilities, Mekelle, Northern Ethiopia: A Cross Sectional Study. International Journal of Pharmaceutical Sciences and Research 4(2):650-660. |
|
|
Ethiopia Demographic and Health Survey (2011). Central Statistical Agency Addis Ababa, Ethiopia ICF International Calverton, Maryland, USA March 2012. How Many Child Deaths Can We Prevent This Year? The Lancet 362(9377):65-71. |
|
|
Kimani-Murage EW, Madise NJ, Fotso JC, Kyobutungi C, Mutua MK, Gitau TM, Yatich N (2011). Patterns and determinants of breastfeeding and complementary feeding practices in urban informal settlements, Nairobi Kenya. BMC Public Health 11(1):396. |
|
|
Kramer MS, Kakuma R (2002). The Optimal Duration of Exclusive Breastfeeding: A Systematic Review. World Health Organization, Geneva. |
|
|
Ministry of Human Resource Development (2004). National Guidelines on Infant and Young Child Feeding. Ministry of Human Resource Development Department of Woman and Child Development (Food and Nutrition Board) Government of India, 2004. |
|
|
PAHO/WHO (2001). Guiding Principles for Complementary Feeding of the Breastfed Child. Pan American Health Organization/ World Health Organization, Washington DC. 2015. |
|
|
Kedir RT, O'Connor TP, Belachew T, O'Brien NM (2016). Infant and Young Child Feeding (IYCF) Practices Among mothers of children Aged 6 -23 months in two Agro-ecological Zones of rural Ethiopia, International Journal of Nutrition and Food Sciences 5(3):185-194. |
|
|
Senarath U, Jayawickrama H, Siriwardena I, Dibley MJ (2012). Determinants of Inappropriate Complementary Feeding Practices in Young Children in Sri Lanka: Secondary Data Analysis of Demographic and Health Survey 2006-2007. Maternal Child Nutrition 8:60-77. |
|
|
Shumey A, Demmissie M, Berhane Y (2013). Timely initiation of complementary feeding and associated factors among children aged 6 to 12 months in Northern Ethiopia: an institution-based cross-sectional study. BMC Public Health 13(1):1050. |
|
|
Tamiru D, Bogale B, Merdekios B (2013). Breastfeeding Patterns and Factors Associated with Exposure to Sub-Optimal Breastfeeding Practices in Rural Communities of Arba Minch Zuria, Ethiopia. Global Health Perspectives 1(2013):105-112. |
|
|
Kibebew A (2012). Infant and Young Child Feeding Practices among mothers Living Harar Town. Harar Bull. Health Science 4:66-78. |
|
|
Bahl R, Frost C, Kirkwood R, Edmond K, Martines J, Bhandari N, Arthur P (2015). Infant Feeding Patterns and Risks of Death and Hospitalization in the First Half of Infancy: Multicentre Cohort Study. Bulletin of the World Health Organization 83:418-26. |
|
|
International CoEaI (2011). Ethiopia Demographic and Health Survey of 2011. |
|
|
UNICEF-WHO-The World Bank Group (2016). Global Database on Child Growth and Malnutrition. Joint child malnutrition estimates - Levels and trends (2016 edition). |
|
|
Victor R (2012). Infant and young child feeding practices among children aged 0-23 months in Tanzania. |
|
|
WHO/UNICEF (2003). Global Strategy for Infant and Young Child Feeding, World Health Organization, Geneva. |
|
|
WHO/UNICEF (2016). Infant and Young Child Feeding Counseling: An Integrated Course. Participant's Manual. 2016. |
|
|
WHO/UNICEF/USAID/FANTA/IFPRI (2008a). Indicators for Assessing Infant and Young Child Feeding Practices: Part1: Definitions. World Health Organization, Geneva. (2008b). |
|
|
WHO/UNICEF/USAID/FANTA/IFPRI (2010). Indicators for Assessing Infant and Young Child Feeding Practices: Part 2: Measurement, World Health Organization, Geneva. |
|
|
Yemen National Health and Demographic Survey (2013). Ministry of Public Health and Population and Central Statistical Organization Sana'a, Yemen. |
|
|
Yonas F Asnakew M, Wondafrash M, Abdulahi M (2016). Infant and Young Child Feeding Practice Status and Associated Factors among Mothers of under 24-Month-Old Children in Shashemene District, Oromia Region, Ethiopia. Open Access Library Journal 2(07):1-5. |
|
|
Victor R (2012). Infant and Young Child Feeding Practices among Children Aged 0-23 Months in Tanzania. Maternal and Child Nutrition Journal 3:357-364. |
|
|
DHS, Yemen National Health and Demographic Survey (2013). Sana'a, Yemen. Preliminary Report, Ministry of Public Health and Population. 2014. |
|
|
Yemane SAT, Gebreslassie M (2014). Timely Initiation of Complementary Feeding Practice and Associated Factors Among Mothers of Children Aged from 6 to 24 Months in Axum Town, North Ethiopia. International Journal of Food Science 3:438-442. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


