Full Length Research Paper

ABSTRACT
The need to have a screening tool for onchocerciasis control to compliment parasitological and molecular diagnosis has remained an important goal. A novel Onchocerca volvulus slide flocculation test (Ov-SFT) was developed using tissue homogenates from rat organs (kidney, liver, heart, spleen, muscle, brain, lungs and testes). Liver followed by spleen and then kidney tissue homogenates performed better than others. Flocculation reactions were performed with antigens extracted from female adult worms of O. volvulus using sodium dodecyl sulphate (SDS) and sera from confirmed onchocerciasis infected patients. Negative and assay controls included non-infected serum and phosphate buffered saline (PBS). Results were subjectively graded as no reaction, 0 or negative. Positive reactions were rated 1 to 5 for low, moderate, medium, high and very high flocculation. The grading corresponded to titre levels ranging from 1/2, 1/4, 1/8, 1/16 and 1/32. The liver homogenate had the highest titre of 1/16 (4) followed by that of the kidney 1/8 (3) and heart 1/4 (2) flocculation reaction. The liver homogenate was validated as binding surface for Ov-SFT for screening field samples. Serum was added undiluted to SDS-extract at 1:40 dilution. Result showed that 33 (50.8%) of the sera samples (n= 65) from onchocerciasis endemic communities receiving ivermectin treatment tested positive. Intensity of antibody reactivity were at 1/2, 1 (1.54%); 1/4, 4 (6.15%); 1/8, 6 (9.23%); 1/16, 9 (13.85%) and 1/32, 13 (20%) dilutions. Three out of the five malaria positive cases were Ov-SFT sero-positive compared to 9 (63.5%) of the 14 malaria negative. There is potential field and point of care application of this test for surveillance and monitoring of onchocerciasis. The possibility of using it with other parasitic and bacterial diseases control is discussed.
Key words: Antibodies, extracted antigens, flocculation test, onchocerciasis, serology, tissue homogenate.
INTRODUCTION
A standard onchocerciasis diagnosis is based on microscopic examination of skin snip for emergedmicrofilaria (mf). Alternative diagnoses involving antigen detection and DNA or RNA molecular based tests are very expensive and require specialized skills (Boatin et al., 1998; Vincent et al., 2000). Detection of DNA or RNA fragments is capable of distinguishing between filarial parasites and other organisms. Among the diagnostic methods used, antibody test holds more promise as screening tool. Serodiagnosis is limited by inherent problem of cross-reactivity due to high molecular weight antigens containing carbohydrate moieties or glycoprotein-complex containing ubiquitous immunodominant phosphorylcholine, which are not recognized by IgE and IgG4 antibody (Lal and Ottesen, 1988; Weiss and Karam, 1989; Guederin et al., 2004; Osue et al., 2008). A major setback to antigen detection is the need to subject the samples to pre-treatment (More and Copeman, 1991; Mbacham et al., 1992) which for serum is to remove interference by specific host antibodies, while for urine is dialysis to obtain concentrated residue. Hence, sample pretreatment will make the field application of antigen detection somehow a difficult process to accomplish. Surveillance for recrudescence is inevitable and is the cornerstone of any disease control and elimination programmes (Guzman et al., 2002). Flocculation tests have been used to screen for Neisseria infections, schistosomiasis and other parasitic diseases using Bentonite flocculation technique (Wallace et al., 1970; Allain et al., 1972).
Moreover, changes in parasite specific antibodies after short-term ivermectin treatment have been investigated (Osue et al., 2009). The detection of parasite or its molecular and antigenic products unequivocally indicate current infection status. Continued dependence on skin snipping and clinical manifestations with the presence of eye lesions like punctate keratitis are not definitive of the disease and therefore unsuitable for surveillance and monitoring of onchocerciasis treatment control (Winthrop et al., 2006). A combination of screening and diagnostic tests is very apt for accurate impact assessment of any intervention strategy where microfilaria load is expected to be reduced in both the host and vector. This study was aimed at developing and evaluating an onchocerciasis slide flocculation test (Ov-SFT) using homogenized rat tissues as antibody binding support. The objective of this study is to assess five sentinel communities enlisted in 1994 for ivermectin (Mectizan™) treatment. This is to explore the unique functional attribute of IgG antibody class and IgG1, IgG3 and IgG4 (excluding IgG2) isotypes’ ability to bind with heterologous tissues (Bennich and Dorrington, 1983). It is assumed that flocculation test with such binding solid support will confer higher specificity by eliminating cross-reactivity due to IgM agglutinins and unspecific reaction of IgG2 antibody. Secondly, the study was to investigate how long parasite-specific antibodies persist after ivermectin treatment, which has remained unknown? Lastly, the test was to explore the possibility of using adult worm sodium dodecyl sulphate (SDS) extracted antigens as screening tool for onchocerciasis.
MATERIALS AND METHODS
Sample population
Sera were obtained from individuals living in onchocerciasis endemic communities enlisted for the mass drug administration. The gender, age and number of ivermectin treatment taken by each participant were documented.
SDS extracted antigens
Adult female worms of Onchocerca volvulus dissected from nodules preserved for 15 years at -20°C in deep freezer (Gomez-Priego et al., 2005) were placed in 1ml of 150 mM phosphate-buffered saline containing protease inhibitors, 1 mM phenylene sulphonyl chloride and 50 mg/ml N-tosyl–phenylalanine chloromethyl ketone. Adult worms were grounded in liquid nitrogen and suspended in PBS and spun at 10,000 g for 5 min. The homogenate was re-suspended in PBS containing 1% SDS and the supernatant was collected after spinning (Engelbrecht et al., 1992) worms were grounded under liquid nitrogen in PBS containing 1% SDS and suspension centrifuged at 1300 g for 5 min and supernatant fluid designated as SDS-extract (Engelbrecht et al., 1992).
Slide flocculation test
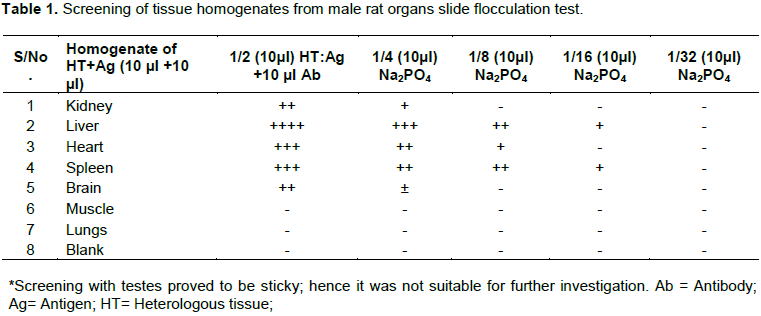
Laboratory bred rats (3) obtained from Nigerian Institute for Trypanosomiasis (and Onchocerciasis) Research. Small animal colony were anaesthetized with ether and dissected. Tissues were teased separately from the heart, muscle, spleen and liver, washed 3 to 5 times with PBS, and homogenized in a porcelain mortar and pestle. After centrifuging for 5 min at 10,000 revolutions/min, the supernatant fluid was decanted and few drops of 0.01% sodium azide were added as preservative. Tissue homogenate (10 µl) and SDS-extracted antigens (10 µl) were mixed at neat and shared into two wells of 10 µl each. An aliquot (10 µl) of antibody containing serum was added and mixed thoroughly. Thereafter, the mixture was double diluted serially in phosphate buffered saline (PBS, 10 µl) in wells of the slide. A detail protocol for slide flocculation test is as shown in Figure 1. Flocculation reactions of serum at neat were subjectively graded as no reaction (–ve=0), and very low (1), low (2), medium (3), high (4) and very high (5) positive reactivity. The highest dilution with flocculation reaction was taken as the assay titre. Series of serial dilutions were performed to determine prozone effects and working concentrations of reactants. Reactivity of different tissue homogenates from rat organs with positive infection and non-infected sera is shown in Table 1.

Repeatability test
Ten replicates of an enzyme linked immunosorbent assay (ELISA) confirmed antibody positive and negative sera were obtained from NITR Onchocerciasis Serum Bank. The optical density (OD) values were 0.57 and 0.07 respectively. The negative was below the calculated cut-off point of 0.1±0.07 mean plus 2 standard deviation of OD values of non-endemic control sera (n=7) (Osue et al., 2008).
Ov-SFT test on malaria positive serum samples
A subset of serum samples (n=5) parasitological and serologically confirmed to be malaria positive cases and those without malaria (n=14) described by Osue et al. (2013) were tested using Ov-SFT to determine cross-reaction.
Preparation of O. volvulus SDS extract
Onchocercal nodules were placed in 3% collagenase until completely digested. Intact adult worms were washed in phosphate buffered saline (PBS) (Engelbrecht et al., 1992). The 3 homogenates (liver, kidney and spleen) were subjected to further tests from which liver, the tissue with highest flocculation titre was selected.
Secondary sample
Two sera samples that have been analyzed with ELISA and found to be positive and negative for antibodies against O. volvulus were obtained from NITR Onchocerciasis Serum Bank. Ten replicates were made from the sera to determine the consistency and repeatability of the Ov-SFT.
Polymerase chain reaction
Paired serum and skin snip of a sub-set of samples (n=30) were subjected to both Ov-SFT and PCR tests. The details of PCR assay has been described in a different publication elsewhere (Osue et al in press). Briefly, the PCR master mix was made up by 10 µl PCR buffer added to 32.1 µl of de-ionized water in an Eppendorf tube, followed by 5.0 µl of MgCl2. Thereafter, 1 µl of dNTP (1 mM dATP, dCTP, dGTP and dTTP), 0.5 mM dUTP 0.5 U uracil-N-glycosylase and 0.5 U Taq DNA polymerase. Amplification of DNA extract using PCR was performed as described by Morales-Hojas et al. (2006) and Ta Tang et al. (2010). To amplify filarial-specific DNA, the 18S rRNA ITS1 and 5.8S gene primers for forward 5'-GGTGAACCTGCGGAAGGATC-3' and reverse 5- TGCTTATTAAGTCTACTTAA -3' described by Nuchprayoon et al. (2005) and Ta Tang et al. (2010) with accession number AF228574 and AF228575 with positions in reference sequence (gene) at 173-192 (18S) and 512-493 (ITS) (Morales-Hojas et al., 2007; Ta Tang et al., 2010; Albers et al., 2012) were used. Both primer sequences were used at 5 pmol each and 10 to 20 ng of parasite DNA templates at a concentration of 20 pmol per 50 µl volume.
These ITS1 primers satisfied the criteria given for selecting sequence primers by the kit manufacturer, QIAGEN®, Germany. One microlitre of the sample and 1µl of the internal control O. volvulus adult worm DNA were added to the master mix. Eppendorf tubes containing the reagents were vortex at low speed then pulse centrifuged and placed in thermal cycler (Techne, Germany). Amplification was performed in 30 cycles at 94°C denaturing, 55°C annealing and 72°C extension of 30 s each. The duration of the thermal cycling process was about 2 h. Hot start polymerase (TaQ Polymerase, Qiagen, Hilden, Germany) was used for PCR. An activation step of 5 min at 94°C preceded the cycling programme. The complete set of the PCR is represented as follows: (94°C 5:00 [94°C 0:30; 60°C 0:45; 75°C 2:00] 35; 72°C 7:00). Two wells that contained an adult worm O. volvulus DNA fragment, master mix with water instead of sample DNA and three skin microfilaria negative served as positive, internal assay and negative controls, respectively.
Gel electrophoresis
The PCR amplicons were run on 2% w/v gel (2 g of agarose powder was added to 100 ml 1X TBE buffer) was dissolved by boiling in a microwave oven. It was allowed to cool to 60°C and 10 µl Syber Green was then added and swirled gently using magnetic stirrer. Finally, 5 µl of the PCR products were checked by agarose gel electrophoresis with appropriate molecular weight markers (1 kb in multiples of 100 bp) inserted to determine the expected size relative to the marker. The marker, positive and negative controls and samples were loaded. Electrodes were connected with negative terminal at the loading end. Electrophoresis was run at 60 to 100V till migration of dye reached three-quarter of the gel. Current was turned off and the electrodes disconnected. Gel was observed under a UV Trans-illuminator and the molecular weight
band documented in a Syngene Digigenius Gel Documentation System with camera linked to a computer.
Statistical analysis
Results of sample analysis are presented in tabular and pictorial formats. Observed differences between groups or sub-groups were subjected to Fischer probability exact test (F-test).
RESULTS
Onchocerca volvulus slide flocculation test
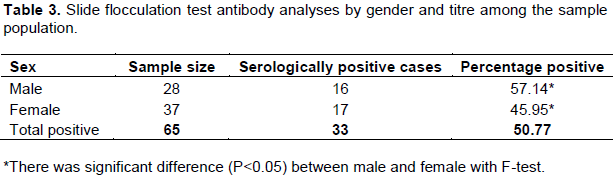
Tissue homogenate from liver was most reactive, followed by kidney and then heart in slide flocculation test is shown in Table 1. Among the tissues (n=8) evaluated, muscle, lung and blank negative control (without tissue) homogenate did not show flocculation. The homogenate from testes was sticky and not suitable for use. Repeatability of Ov-SFT with 10 replicates of onchocerciasis infected patient and non-infection control whose antibody reactivity were confirmed in ELISA had 100 and 0% positive reactions, respectively (Table 2). Overall number of sero-positive sample among sampled population (n=65) using Ov-SFT was 33 (50.8%). There was significant difference in serological positive rate (P<0.05) between male and female as shown in Table 3. Profile of antibody titre ranged from 1/2, 1 (1.54%); 1/4, 4(6.14%), 1/8, 6 (9.23%), 1/16, 9 (13.85%) and 1/32, 13 (20%). Three out of five malaria positive cases compared to 9 (63.4%) of the 14 non-infected malaria were Ov-SFT sero-reactive. Among the paired sera and skin biopsies (n=30) tested with Ov-SFT and PCR amplification showed 12 (40%) sero-reactivity and 0 (0%) positive, respectively.

Analysis of sample by age showed there was detectable antibody reactivity among the age groups with bimodal frequency in the 31 to 40 year (75%) and 51 to 60 year (85.7%) as shown in Table 4. The number of treatment received did not have any significant (p>0.05) influence on the antibody reaction (Table 5). On Table 6, the observed frequencies of ELISA reaction at baseline (pre-treatment) in sample population (n=114) comparatively was significantly higher (p<0.05) than that of Ov-SFT reaction at 18-year post-treatment in a sample population (n=65).



DISCUSSION
A slide flocculation test (SFT) was developed using tissue homogenates from eight organs of rats from which the liver was selected. Effort at developing simple and accurate methods for field screening and diagnosis of neglected tropical diseases has remained a top priority. Application of flocculation test has been used in the past as a dependable tool for testing many parasitic and bacterial infections and non-communicable disease such as rheumatoid arthritis (Norman and Kagan, 1963; Wallace et al., 1970). Another widely used test is the non-treponemal rapid plasma reagin (RPR) used by the Venereal Disease Laboratory (VDL) for screening of syphilis (Radolf et al., 2011). Serum antibodies reactivity with parasite specific antigens in SDS extract from adult worm O. volvulus were measured in Ov-SFT in sera from persons (n=65) resident in onchocerciasis endemic communities enlisted for ivermectin treatment in 1994. A possible mechanism of binding of antibody to heterologous tissue is probably due to immune complexes (ICx) and rat and human Ig aggregates were reported to bind via a crystallisable fragment (Fc) receptor. The Fc receptor was still intact in livers from carbon tetrachloride and galactosamine treated rats. The receptor could also be demonstrated on spleen macrophages and on kidney interstitial cells (van der Laan-Klamer et al., 1987). Inorder to surpass the already identified major difficulty of unspecific appearance of floccules (Allain et al., 1972), double dilution without antigen was performed for each positive sample.
Time taken to perform Ov-SFT and obtain result within 1 to 3 min is by far faster than other existing tools like the four Ov-antigen standard or 15-min format quick luciferase immunoprecipitation system (QLIPS) (Weil et al., 2000; Ramanathan et al., 2008; Burbelo et al., 2009). The comparative advantages of Ov-SFT are attributed to being simple, sensitive, fast and requires no specialized skill. Before it can be adjudged as a suitable screening tool to detect exposure to infection, it will require further validation tests using active infection sera from filariasis and other parasitic diseases. In declaring an area onchocerciasis free will rely on combining mass screening of people using antibody detection to exclude those not exposed from those exposed to infection. Therefore, only those exposed can be subjected to PCR assay for confirmation. The recorded 50.8% positive rate attested to the fact that the need to have screening to preclude subjecting more people to PCR diagnostic test, thereby reducing cost. It has been posited that antibody testing may be more useful for screening populations for infection or exposure to O. volvulus, whereas antigen testing and PCR are more crucial for diagnosis of infections in individuals and for monitoring the success of therapy (Vincent et al., 2000). Further, PCR and antigen tests are not definitive since they only show presence of parts and not whole life stages of the worm. This is unlike the microscopic test that detects emerged microfilariae from skin snip.
Evaluation of Ov-SFT results with sera from sentinel communities undergoing mass drug administration with ivermectin had shown that there was significant difference in gender reactivity. Higher antibodies in female than male observed in this study is in conformity with documented antibody profile either before or after commencement of treatment control (Gomez-Priego et al., 2005; Osue et al., 2009). In addition, antibody titres recorded in different age classes particularly among the younger class of ≤30 years old (38.5%) calls for concern. We propose adoption of a simple and sensitive antibody screening test as veritable means of monitoring long-term onchocerciasis treatment control. This will be more evidence based than the use of clinical signs like demonstrating presence of microfilaria in anterior chamber proposed by Winthrop et al. (2006).
This study had shown that 18-year of post-ivermectin characterized by varied treatment compliance had not succeeded in totally eliminating parasite-specific IgG antibodies. This is in agreement with reports by others that have shown reduction in antibody levels (Rodriguez-Perez et al., 1999; Guzman et al., 2002; Gomez-Priego, 2005; Gonzalez et al., 2009). When compared with the baseline antibody levels measured with IgG ELISA antibody, Osue (1996) clearly indicated the high levels of those exposed to infection in the study population (n=114) was 98.5% as against the 50.14% recorded in this study using Ov-SFT. More importantly, there was apparently no significant difference in antibody intensity in males (n=28) and female (n=37), the frequency was significantly higher in the former than the latter. The co-endemicity of malaria infection do not pose any problem of cross-reaction. This would appear not to underscore the need to further investigate specificity with other parasites.
This study showed that Ov-SFT is simple, sensitive and fast and requires no specialized skill. Importance of flocculation test has long been recognized for screening of parasitic diseases like schistosomiasis, filariasis, amoebiasis and others as reported by Allen et al. (1972). It has continued to be relied upon in population screening for syphilis in the United States (Radolf et al., 2011). The test is suitable as screening tool to detect exposure to infection.
Further research and development on the wider application of Ov-SFT will require the much needed evaluation in different clinical disease entities. It is practically very necessary for an onchocerciasis endemic area to be declared free or eradicated based on combination of mass screening using antibody detection test to identify those exposed to infection that, thus, require to submit samples for molecular diagnosis using PCR assay and follow up for confirmation with skin microfilarial detection in hospital management or community directed treatment intervention.
We observed that minimal reactive and slight roughness can be interpreted differently by readers. This could lead to variability in results from different operators reading the same test within same or between laboratories (Castro et al., 2012). The authors were of the opinion that flocculation test lends itself for both qualitative and quantitative application with the ASiManager-AT digital flocculation reader designed to read objectively each well of the rapid plasma reagin (RPR) test. This might increase cost and negate the simplicity of the test. Alternatively, we found dependable the use of a simple hand held magnifying glass could improve the ability of observers to enhance good judgement about outcome of reactions in the wells.
In conclusion, the widely recommended Ov16 and other recombinant antigens with confirmed high sensitivity and specificity for serological screening should be used to further develop this test. Secondly, the Ov-SFT can be adapted to other important communicable and non-communicable diseases. This study has proven the huge potential of the modified classical flocculation test using heterologous tissue homogenate as a binding substrate. It will no doubt require further research and development to validate the laboratory and field application as a novel screening tool.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors thank the Management of the Nigerian Institute for Trypanosomiasis (and Onchocerciasis) Research for providing fund for the project. Their appreciation goes to Mr. Friday Idowu and Mr. Emmanuel Yarnap for reading the antigen-antibody reactions and Mr. Kehinde David for dissecting the rats. They thank Mr. J. Gazama and Mr. Samson Itua for skin snipping and collection of blood and extraction of serum samples. They are also grateful to the Chairman, Head of Health and the Onchocerciasis Coordinator of Kachia LGA, Kaduna State, Nigeria and thank the Village Heads and the people of the study communities for their voluntary participation in the field study.
REFERENCES
|
Allain DS, Chisholm ES, Kagan IG (1972). Use of the bentonite flocculation test for the diagnosis of schistosomiasis. Health Serv. Rep. 87(6):550-554. |
|
|
Bennich H, Dorrington KJ (1973). Thermally induced structural changes in immunoglobulin E. J. Biol. Chem. 248(24):8378-8384. |
|
|
Boatin BA, Toé L, Alley, ES, Dembélé N, Weiss N, Dadzie KY (1998). Diagnostics in onchocerciasis: future challenges. An. Trop. Med. Parasitol. 92:S41-S45. |
|
|
Burbelo PD, Leahy HP, Iadarola MJ, Nutman TB (2009). A Four-Antigen Mixture for Rapid Assessment of Onchocerca volvulus Infection. PLoS. Negl. Trop. Dis. 3(5):e438. |
|
|
Castro AR, Binks DD, Raymer D.L, Kikkert SE, Jost HA, Park MM, Card BD, Cox DL (2012). Evaluation of a Digital Flocculation Reader for the Rapid Plasma Reagin Test for the Serological Diagnosis of Syphilis. Sex. Transm. Dis. 39(3):223-225. |
|
|
Engelbrecht F, Eisenhardt G, Turner, J, Sundaralingam J, Owen D, Braun G, Connor DW (1992). Analysis of antibody responses directed against two O. volvulus antigens defined by monoclonal antibodies. Trop. Med. Parasitol. 43:47-53. |
|
|
Gomez-Priego A, Mendoza R, de-la-Rosa JL (2005). Prevalence of antibodies to Onchocerca volvulus in residents of Oazaca, Mexico, treated for 10 years with ivermectin. Clin. Diag. Lab. Immunol. 12(1):40-43. |
|
|
Gonzalez RJ, Cruz-Ortiz1 N, Rizzo N, Richards J, Zea-Flores G, Domı’nguez A, Sauerbrey M, Catu´ M, Oliva O, Richards Jr FO, Lindblade KA (2009). Successful interruption of transmission of Onchocerca volvulus in the Escuintla-Guatemala focus, Guatemala. PLOS. Negl. Trop. Dis. 3(3):e404. |
|
|
Guzman GE, Awadzi K, Opoku N, Narayanan RB, Akuffo HO (2002). Comparison between the skin snip test and simple dot blot assay as potential rapid assessment tools for onchocerciasis in the post-control era of in Ghana. Clin. Diag. Lab. Immunol. 9(5):1014-1020. |
|
|
Lal RB, Ottesen EA (1988). Enhanced diagnostic specificity in human filariasis by IgG4 antibody assessment. J. Infect. Dis. 158(5):1034-1037. |
|
|
Mbacham GV, Titanji VP, Thumberg L, Holmdahl R, Rubin K (1992). A monoclonal antibody-based immunodiagnostic assay for onchocerciasis. Trop. Med. Parasitol. 43(2):83-89. |
|
|
More SJ, Copeman DB (1991). Antigen detection ELISAs: pretreatment of serum to reduce interference by specific host antibodies. Trop. Med. Parasitol. 42:191-194. |
|
|
Norman L, Kagan IG (1963). Bentonite, latex, and cholesterol flocculation tests for the diagnosis of trichinosis. Pub. Health Rep. 78(3):227-232. |
|
|
Osue HO, Engelbrecht F, Edeghere LE, Odama LE, Galadima M (2008). Sensitivity of some immunoglobulin G class and subclass antibodies to adult Onchocerca volvulus SDS-extracted antigens. Sci. World J. 3(2):1-4. |
|
|
Osue HO, Galadima M, Engelbrecht F, Odama L, Edeghere HI (2009). Quantitative changes in antibodies against onchocercal native antigens two months post-ivermectin treatment of onchocerciasis patient. Afr. J. Clin. Exp. Microbiol. 10(1):26-37. |
|
|
Osue HO, Inabo HI, Yakubu SE, Audu PA, Galadima M, Odama LE, Musa D, Ado SA, Mamman M (2013). Impact of Eighteen-Year Varied Compliance to Onchocerciasis Treatment with Ivermectin in Sentinel Savannah Agrarian Communities in Kaduna State of Nigeria. Hindawi Publishing Corporation ISRN Parasitology, 2013:1-10. |
|
|
Osue HO (1996). Onchocerca volvulus antigen-specific IgA, IgM, IgG class and subclass antibodies and circulating eosinophils in clinical onchocerciasis patients from Kachia LGA of Kaduna State. M.Sc. Thesis, Microb Dept ABU, Zaria. |
|
|
Ramanathan R, Burbelo PD, Groot S, Iadarola MJ, Neva FA, Thomas BN (2008). A luciferase immunoprecipitation systems assay enhances the sensitivity and specificity of diagnosis of Strongyloides stercoralis infection. J. Infect. Dis. 198(3):444-451. |
|
|
Rodriguez-Perez MA, Danis-Lozano A, Rodriguez MH, Bradley JE (1999). Comparison of serological and parasitological assessments of Onchocerca volvulus transmission after 7 years of mass ivermectin treatment in Mexico. Trop. Med. Intern. Health 4:98-104. |
|
|
Toe´ L, Boatin BA, Adjami A, Back C, Merriweather A, Unnasch TR (1998). Detection of Onchocerca volvulus Infection by O-150 Polymerase Chain Reaction. J. Infect. Dis. 178:282-285. |
|
|
van der Laan-Klamer SM, Harms G, Hardonk MJ (1987). Immunohistochemical demonstration of FC receptors in rat tissues using immune complexes as ligand Histochemie. Histochem. Cell Biol. 84(3):257-262. |
|
|
Vincent JA, Lustigman S, Zhang S, Weil GJ (2000). A comparison of newer tests for the diagnosis of onchocerciasis. Ann. Trop. Med. Parasitol. 94:253-258. |
|
|
Wallace R, Diena BB, Yugi H, Greenberg L (1970). The bentonite flocculation test in the assay of Neisseria antibody. Can. J. Microbiol. 16(8):655-659. |
|
|
Weil GJ, Steel C, Lifts F, Means G, Lobos E, Nutman TB (2000). A rapid-format antibody card test for diagnosis of onchocerciasis. J. Infect. Dis. 182:1796-1799. |
|
|
Weiss N, Karam M (1989). Evaluation of a specific enzyme immunoassay for onchocerciasis using a low molecular weight antigen fraction of Onchocerca volvulus. Am. J. Trop. Med. Hyg. 40:261-267. |
|
|
Winthrop KL, Proa-o R, Oliva O, Arana B, Mendoza C, Dominguez A, Amann J, Punkosdy G, Blanco C, Klein R, Sauerbrey M, Richards F (2006). The reliability of anterior segment lesions as indicators of onchocercal eye disease in Guatemala. Am. J. Trop. Med. Hyg. 75(6):1058-1062. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


