Full Length Research Paper
ABSTRACT
Although it is generally accepted that modified ultrafiltration (MUF) improves operative outcomes in pediatric cardiac surgery, the evidence for this remains equivocal. Previous meta-analyses have been affected by significant patient and method heterogeneity. Google Scholar and PUBMED were searched between January 1st 1966 and May 31st 2022. We conducted a meta-analysis after pragmatically minimising patient and method heterogeneity. There were 631 patients (314 MUF vs 317 ‘No MUF’) in the the mortality analysis and 258 patients (129 MUF vs 129 ‘No MUF’) in the ‘duration-of-ventilation’ (DOV) and ‘length-of-hospital stay’ (LOHS) analyses. There was no significant difference in operative mortality, DOV and LOHS. There is no evidence that MUF improves these operative outcomes in paediatric cardiac surgery.
Key words: Modified ultrafiltration, pediatric, cardiac surgery.
INTRODUCTION
Cardiopulmonary bypass (CPB) facilitates the correction of congenital cardiac lesions, however it is associated with physiological changes that are thought to adversely affect surgical outcomes (Seghaye et al., 1996). There is evidence that ultrafiltration (UF) attenuates some of these physiological changes (Elliott, 1993) and it is postulated that this may reduce operative mortality and morbidity (Koutlas et al., 1997). Although the evidence that UF improves operative outcome is equivocal, UF is practiced widely. Conventional UF (CUF) refers to UF conducted during CPB; modified UF (MUF) technically refers to UF conducted after weaning from CPB. What is commonly referred to as ‘MUF’, in clinical practice, is usually a combination of CUF during CPB and MUF after weaning from CPB (Elliott, 1993). MUF alone does not appear to be superior to CUF alone, with respects to attenuating the physiological changes associated with CPB (Wang et al., 1996). It is important to clarify whether MUF actually improves operative mortality and morbidity as there is evidence that aggressive UF leads to acute kidney injury (Manning et al., 2021). In addition, UF in general and MUF in particular require extra equipment and additional procedural steps; this may increase the likelihood of the occurrence of adverse events and could increase the cost of cardiac surgery. Factors such as patient size (Kameyama et al., 2000), filter type (Berdat et al., 2004) and technique of UF (Manning et al., 2021) may affect the efficacy of UF. Attempts, via meta-analysis, to confirm the benefits of MUF have been hampered by patient and methodological heterogeneity. To minimise heterogeneity, we only included studies, in our meta-analysis, that were pragmatically similar with respects to factors that are thought to affect MUF efficacy.
MATERIALS AND METHODS
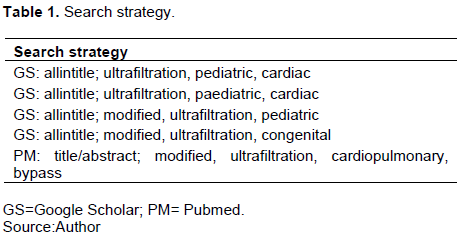
Guided by the PRISMA-P checklist (Moher et al., 2015), PUBMED (PM) and Google Scholar (GS) were systematically searched between January 1st 1966 and May 31st, 2022. The search details are shown in Table 1. PM searches utilised the “title/abstract” option; GS searches utilised the “all in title” option; all searches used the “AND” function. Titles and abstracts were reviewed; full-text papers were examined when an abstract suggested that a paper could contain data comparing outcomes of MUF with CUF. Only English language studies and human studies were included. The search flow is as shown in Figure 1. A meta-analysis was conducted using ‘Meta-Mar’ free online meta-analyser (Meta-Mar, 2022); a continuity correction of 0.5 was applied to studies with ‘zero-events’ in an arm, as recommended by Cheng et al. (2016). The I2 statistic was used to assess heterogeneity (Cheng et al., 2016).

RESULTS
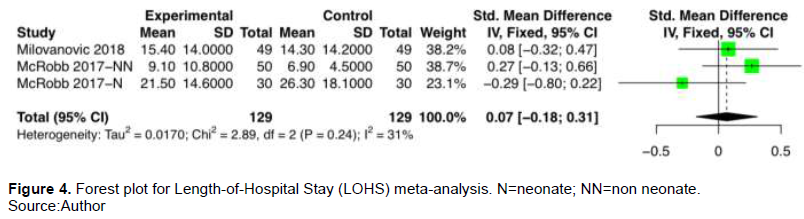
This search yielded 421 results; 27 full-text papers were reviewed. Nine papers, representing 631 patients, were included in the meta-analysis; the key details of the studies included are summarised in Table 2. The results of the mortality and morbidity meta-analysis are as shown in Figures 2 to 4.



DISCUSSION
CPB causes water retention and a systemic inflammatory response (Seghaye et al., 1996). It is postulated that these physiological changes may adversely affect organ function and result in worse operative outcomes (Hövels-Gürich et al., 2002). There is equivocal evidence that MUF reduces the magnitude of these physiological derangements and improves operative outcome (Kuratan et al., 2011; Hu et al., 2021). Attempts to clarify the matter through meta-analysis have been hampered by significant patient and study heterogeneity (Kuratan et al., 2011; Hu et al., 2021). To the best of our knowledge, we have conducted the largest meta-analysis on a pragmatically homogenous group of pediatric patients. We found that MUF does not improve operative mortality or decrease DOV or LOHS in paediatric cardiac surgery. The I2 statistics for our mortality and morbidity (duration of ventilation) analyses were below 5%, indicating low heterogeneity (Kuratan et al., 2011). As the level of heterogeneity was low in the analyses, the fixed-effects model was used (Melsen et al., 2014). A ‘funnel-plot’ was not used as they are not useful when less than 10 studies are included in a meta-analysis (Sterne et al., 2011).
There are reports that MUF increases post-operative haematocrit (Singh et al., 2020), and reduces the post-operative level of inflammatory mediators such as cytokines (Gru ? nenfelder et al., 2000). It is reasonable to argue that a higher post-operative hematocrit could result in better oxygen delivery to tissues and consequently contribute to a better operative outcome. Similarly, it could be reasoned that lower levels of inflammatory mediators may lead to a milder inflammatory response which could theoretically attenuate organ dysfunction. It is conceivable that MUF, working through pathways such as these, might improve operative mortality and operative morbidity. However, ‘Best practice’ demands that an intervention should only be employed in patient care if there is empirical evidence that it improves patient outcome. Our meta-analysis provides evidence that MUF does not reduce operative mortality or morbidity.
For the purpose of meta-analysis, it was found that it was not possible to use outcomes such as the haematocrit or the volume of post-operative chest tube drainage. This was because different transfusion and CPB blood prime protocols were reported in the literature and the volume of chest tube drainage was not reported in a standard manner. Previous meta-analyses have reported high levels of heterogeneity when these parameters have been used as outcome variables (Kuratan et al., 2011; Hu et al., 2021). To credibly assess the effect of MUF on post-operative morbidity through meta-analysis, it is necessary to choose morbidity outcomes that minimise patient and methodological heterogeneity. Two of such outcomes were chosen: the ‘duration-of-ventilation’ (DOV) and the ‘length-of-hospital stay’ (LOHS). These are composite morbidity end-points as they are dependent on factors such as post-operative organ function and volume of post-operative chest tube drainage.
There is evidence that the efficacy of MUF is related to patient size; MUF seems to be more effective at reducing body water and inflammatory mediators in patients under 3 years of age or who have a body weight less than 10 kg (Kameyama et al., 2000). To pragmatically minimise patient heterogeneity we only included studies who reported a mean or median patient age of 3 years or less.
This age ‘cut-off’ also minimised methodological heterogeneity; it maximised the possibility that similar sized reservoirs would be used in the CPB circuit. In addition, to contribute towards methodological homogeneity, we confirmed that 8 out of the 9 studies included used the same filter type and it was demonstrated that all 9 studies included were comparable with respects to the ‘aggression’ or ‘target’ of MUF. The I2 statistic was below 25% when all 9 studies were included in our mortality meta-analysis. However, the I2 statistic was over 75% when all 9 studies were included in the morbidity meta-analysis. When studies included only reported a mean or median patient age of 1 year old or less in the morbidity analysis, an I2 statistic well below 1% was obtained for the DOV analysis and an I2 statistic of 31% was obtained for the LOHS analysis. These I2 statistic values are generally consistent with low and acceptable levels of heterogeneity, respectively (Kuratan et al., 2011).
Two other meta-analyses on pediatric patients have been reported in the literature (Kuratan et al., 2011; Hu et al., 2021), neither of them assessed how MUF affected operative mortality. Both assessed DOV and both found no difference between the MUF and No-MUF groups. However, they reported I2 statistics of 74% (Kuratan et al., 2011) and 87% (Hu et al., 2021). Only one of these meta-analyses assessed LOHS and they found no difference between MUF and non-MUF groups; there was little evidence of heterogeneity (I2 statistic of 15.3%). The duration of cardiopulmonary bypass and the aortic cross clamp time are additional factors that could potentially affect operative outcome. The I2 statistic for all our meta-analyses were well below 25% indicating that the studies included were homogenous in this respect. We have demonstrated, in a group of patients with low heterogeneity, that MUF does not reduce operative mortality. We have also demonstrated that MUF does not reduce operative morbidity, even in a subset of patients (small patients/neonates/young infants) thought to particularly benefit from MUF. This is an important finding as MUF may not be an innocuous procedure and it may increase the cost of surgery.
Although some units have abandoned MUF (Mejak et al., 2019), we think that the potential benefits of MUF have not been fully elucidated yet. For instance, MUF could reduce the need for postoperative blood transfusion and perhaps even reduce the post-operative inotrope requirement. This could reduce the number of adverse events associated with blood transfusion and may even reduce the financial cost associated with blood transfusion and inotrope usage. To determine whether such benefits exist, paediatric cardiac surgery programs would have to standardise blood priming protocols for CPB, as well ‘triggers’ for blood transfusion. In addition, it would be necessary to standardise how chest tube drainage is reported; for example, drainage could be reported as millilitres per kilogram per hour until the chest tube is removed.
In conclusion, the meta-analysis of 631 patients found that adding post-CPB MUF to patients who have had CUF during CBP did not reduce operative mortality or operative morbidity in pediatric patients undergoing cardiac surgery. Cardiac surgery protocols should be kept as ‘simple’ as possible to minimise adverse events and the cost of surgery. The findings may have important implication for the current widespread practice of MUF.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Aeba R, Katogi T, Omoto T, Kashima I, Kawada S (2000). Modified ultrafiltration improves carbon dioxide removal after cardiopulmonary bypass in infants. Artificial Organs (4):300-304. |
|
|
Bando K, Turrentine MW, Vijay P, Sharp TG, Sekine Y, Lalone BJ, Szekely L, Brown JW (1998). Effect of modified ultrafiltration in high-risk patients undergoing operations for congenital heart disease. The Annals of Thoracic Surgery 66(3):821-782. |
|
|
Berdat PA, Eichenberger E, Ebell J, Pfammatter JP, Pavlovic M, Zobrist C, Gygax E, Nydegger U, Carrel T (2004). Elimination of proinflammatory cytokines in pediatric cardiac surgery: analysis of ultrafiltration method and filter type. The Journal of thoracic and Cardiovascular Surgery 127(6):1688-1696. |
|
|
Cheng J, Pullenayegum E, Marshall JK. (2016). Impact of including or excluding both-armed zero- event studies on using standard meta-analysis methods for rare event outcome: a simulation study. BMJ Open 6(8):e010983. |
|
|
Elliott MJ (1993). Ultrafiltration and modified ultrafiltration in pediatric open heart operations. The Annals of Thoracic Surgery 56(6):1518-1522. |
|
|
Gru ? nenfelder J, Zu ? nd G, Schoeberlein A, Maly FE, Schurr U, Guntli S (2000). Modified ultrafiltration lowers adhesion molecule and cytokine levels after cardiopulmonary by- pass without clinical relevance in adults. European Journal of Cardiothoracic Surgery 17:77-83. |
|
|
Hövels-Gürich HH, Vazquez-Jimenez JF, Silvestri A, Schumacher K, Minkenberg R, Duchateau J, Messmer BJ, Von Bernuth G, Seghaye MC (2002). Production of proinflammatory cytokines and myocardial dysfunction after arterial switch operation in neonates with transposition of the great arteries. The Journal of Thoracic and Cardiovascular Surgery 124(4):811-820. |
|
|
Hu J, Li P, Chen X, Yan J, Zhang J, Zhang C (2021). Effects of modified ultrafiltration and conventional ultrafiltration combination on perioperative clinical outcomes in pediatric cardiac surgery: A meta-analysis. Medicine 100:3(e24221). |
|
|
Kameyama T, Ando F, Okamoto F, Hanada M, Yamanaka K, Sasahashi N, Hirose K, Matsuno S, Matsuura S (2000). The effect of modified ultrafiltration in pediatric open heart surgery. Annals of Thoracic and Cardiovascular Surgery: Official Journal of the Association of Thoracic and Cardiovascular Surgeons of Asia 6(1):19-26. |
|
|
Koutlas TC, Gaynor JW, Nicolson SC, Steven JM, Wernovsky G, Spray TL (1997). Modified ultrafiltration reduces postoperative morbidity after cavopulmonary connection. The Annals of Thoracic Surgery 64(1):37-43. |
|
|
Kuratan N, Bunsangjaroen P, Srimueang T, Masaki E, Suzuki T, Katogi T (2011). Modified versus conventional ultrafiltration in pediatric cardiac surgery: a meta-analysis of randomized controlled trials comparing clinical outcome parameters. The Journal of Thoracic and Cardiovascular Surgery 142(4):861-867. |
|
|
Maluf MA (2003). Modified ultrafiltration in surgical correction of congenital heart disease with cardiopulmonary bypass. Perfusion 18(1_suppl):61-68. |
|
|
Manning MW, Li YJ, Linder D, Haney JC, Wu YH, Podgoreanu MV, Swaminathan M, Schroder JN, Milano CA, Welsby IJ, Stafford-Smith M (2021). Conventional ultrafiltration during elective cardiac surgery and postoperative acute kidney injury. Journal of Cardiothoracic and Vascular Anesthesia 35(5):1310-1318. |
|
|
McRobb CM, Ing RJ, Lawson DS, Jaggers J, Twite M (2017). Retrospective analysis of eliminating modified ultrafiltration after pediatric cardiopulmonary bypass. Perfusion 32(2):97-109. |
|
|
Mejak BL, Lawson DS, Ing RJ (2019). Con: modified ultrafiltration in pediatric cardiac surgery is no longer necessary. Journal of Cardiothoracic and Vascular Anesthesia 33(3):870-872. |
|
|
Melsen WG, Bootsma MC, Rovers MM, Bonten MJ (2014). The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clinical Microbiology and Infection 20(2):123-129. |
|
|
Meta-Mar (2022). Meta-Mar free online meta analysis service. 2022. |
|
|
Milovanovic V, Bisenic D, Mimic B, Ali B, Cantinotti M, Soldatovic I, Vulicevic I, Murzi B, Ilic S (2018). Reevaluating the importance of modified ultrafiltration in contemporary pediatric cardiac surgery. Journal of Clinical Medicine 7(12):498. |
|
|
Ming ZD, Wei WA, Hong CH, Wei ZH, Xiang DW (2001). Balanced ultrafiltration, modified ultrafiltration, and balanced ultrafiltration with modified ultrafiltration in pediatric cardiopulmonary bypass. The Journal of Extra-Corporeal Technology 33(4):223-226. |
|
|
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews 4(1):1-9. |
|
|
Seghaye MC, Grabitz RG, Duchateau J, Bussea S, Däbritz S, Koch D, Alzen G, Hörnchen H, Messmer BJ, von Bernuth G (1996). Inflammatory reaction and capillary leak syndrome related to cardiopulmonary bypass in neonates undergoing cardiac operations. The Journal of Thoracic and Cardiovascular Surgery 112(3):687-697. |
|
|
Singh S, Okyere I, Mahrous DE (2020). The effect of combined conventional and modified ultrafiltration on mechanical ventilation and hemodynamic changes in paediatric congenital heart surgery. EAS journal of Anaesthesiology and Critical Care 2(1):30-39. |
|
|
Sterne JA, Sutton AJ, Ioannidis JP, Terrin N, Jones DR, Lau J (2011). Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 343:d4002. |
|
|
Takabayashi S, Shimpo H, Yokoyama K, Iwata H (2007). Relationship between increased blood pressure and hematocrit during modified ultrafiltration for pediatric open heart surgery. General Thoracic and Cardiovascular Surgery 55(1):12-18. |
|
|
Wang MJ, Chiu S, Hsu CM, Wang CM, Lin PL, Chang CI, Huang CH, Chu SH (1996). Efficacy of ultrafiltration in removing inflammatory mediators during pediatric cardiac operations. The Annals of Thoracic Surgery 61(2):651-656. |
|
|
Williams GD, Ramamoorthy C, Chu L, Hammer GB, Kamra K, Boltz MG, Pentcheva K, McCarthy JP, Reddy VM (2006). Modified and conventional ultrafiltration during pediatric cardiac surgery: clinical outcomes compared. The Journal of Thoracic and Cardiovascular Surgery 132(6):1291-1298. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


