ABSTRACT
This study reviews the retention strategies used for Lesotho’s doctors and nurses, and it presents an implementation framework that supports and promotes staff retention. Based on the increasing necessity to retain doctors and nurses, the implementation framework is an essential element of retention strategy. A qualitative and quantitative research design method for collecting data was adopted in the form of a self-administered questionnaire and interviews. The sample consists of 120 doctors and nurses. The information was statistically analyzed using statistical package for social sciences (SPSS) and grounded theory. Results show that the current implementation strategy has failed to increase the retention rate of doctors and nurses. It is hoped that the implementation framework presented in this study would help to achieve increased retention rate for doctors and nurses.
Key words: Employee retention, human resource, health professionals, implementation framework, human resource strategies.
Human capital is the most essential asset of any organisation, irrespective of size or division. This is true for the health sector in Lesotho that is currently having a high turnover rate of doctors and nurses. This increase in turnover has made the Lesotho health sector less successful. In order to fulfil its service delivery mandate, another implementation framework is needed to support retention strategies for doctors and nurses.
This study recognises and observes an appropriate implementation framework that can be utilised to retain and manage these retention strategies. It can be expected that the current retention strategies have failed to effectively keep the healthcare professionals in Lesotho, and are permitted to keep falling regardless of the vital commitment doctors and nurses could make to help understand the service delivery mandate. Doctors and nurses are short staffed and the implementation framework that attempts to enhance the retention rate would help address the issue of service delivery and control the scarcity of healthcare professionals in Lesotho.
In the strategy document, the arrangement of incentives
to doctors and nurses was made and implemented to guarantee enhanced retention rate (Ministry of Health and Social Welfare, Government of Lesotho, 2010). The success of some of these financial incentives has been investigated by Dambisya (2007), and fits into two classifications, namely financial and non-financial incentives.
The aforementioned methodologies have been put into practice by the government of Lesotho (GoL) for three years while implementation of the present retention strategy permits the compensation of financial incentives to healthcare professionals in two mountainous regions (Mokhotlong and Qacha's Nek) (Schwabe et al., 2004).
This practice, though well-intentioned, has neglected to accomplish the needed impact since it is both unfair and selective; healthcare professionals working in different parts of the nation do not meet all requirements to get such incentives. Notwithstanding the unfair and selected implementation of financial incentives, there are different payments, for example, occupational risk and call allowance that help to extend discrimination and exclusion, to the detriment of wholesome retention that is both effective and proactive (Schwabe et al., 2004).
While the aforementioned strategy implementation cannot possibly accomplish the required retention, it is important for making apprehension among healthcare professionals that experience discrimination, and are eliminated from the incentive payment.
Moreover, qualification rewards or incentives are paid to those with higher qualifications. In spite of the fact that this incentive payment is oppressive, it requires keeping up a higher standard of qualification and additionally advance the way of life of constant professionals improvement; a necessary component of professionalism and quality assurance.
Maslow theory, according to Lin (2007), indicates that individuals are no longer motivated by money as its power is limited. These discoveries are in accordance with studies completed by Herzberg (1966) referred to in Mbah and Ikemefuna (2012). Mbah and Ikemefuna (2012) carried out the studies in line with these results. However, Schwabe et al. (2004) contended that bonus reward enhanced retention if prepared with rigid salary.In addition, bonding strategy is a non-financial incentive whereby students trained in South Africa, and abroad, are obliged to give benefits in fulfillment of their studies for a period that is equivalent to the duration of the scholarship/bursary; however, just few graduates come back (Schwabe et al., 2004).
These graduates are more willing to reimburse the government costs as opposed to serving which shows that this procedure is not sufficiently thorough to retain graduates. From the aforementioned, it is presumed that the implemented retention strategy has neglected to accomplish expected retention, since Lesotho's health sector is yet to encounter a high turnover of doctors and nurses. This is confirmed by Ministry of Health and Social Welfare, Government of Lesotho (2010) which demon-strates 15% of nurses depart the service consistently, while around 90% of health centers function without healthcare professionals.
Right now, the nation is seriously reliant on non-national medical doctors, among which there is likewise high steady loss rate since they are utilising Lesotho as a stepping stone to South Africa. This circumstance obstructs long pull arranging and maintainability of health service delivery and projects expected to enhance the talented human resource base (Ministry of Health and Social Welfare, 2013).
The rationale for this research is to discover failure of the present retention strategy for health professionals working for the Lesotho Health sector, with the likelihood of helping the department in creating and implementing a successful retention strategy.
Statement of research problem
While the retention strategy is valuable in retaining doctors and nurses, the Lesotho health sector would gain from the know-how of their medical staff. This is valid for the health sector that is facing a high rate of staff leaving the organization+; the increased turnover has constrained the Lesotho health sector to work with a predetermined number of health professionals to the detriment of the guaranteed service delivery mandate (Ministry of Health and Social Welfare, 2010).
From one perspective, according to the WHO (2017), the shortage of medical school in Lesotho represents most doctors and nurses who travel to another country to study, particularly in South Africa. It urges health professionals to search for better paying occupations abroad to complete their studies; the present circumstance seems to be caused by nations, for example, United Kingdom (UK) and Australia that draw in and retain doctors and nurses, while the health sector has not succeeded.
Then again, the health sector has not figured out how to create compelling systems for retention; this along these lines has a colossal unconstructive impact on hospitals, clinics as well as community health centers. The contention here is that a large portion of these facilities is horribly understaffed which is an issue of awesome concern, and each one of those that have been employed are overburdened as they are seriously dwarfed by the measure of patients every day (Matamane, 2014).
The Healthcare and Family Services (HFS) contemplate affirms that more than seventy five percent of the Health centers do not have a full staff supplement, while one in five health focuses is controlled by nursing assistants (Ministry of Health and Social Welfare, 2013).
The lack of staff brings about restricted contact time of patients with medical attendants. Substantial nursing workloads are probably going to detrimentally affect patient care and health results. Currently, retention strategies implemented have not improved the retention rate for healthcare professionals, and a new implementation framework to improve retention has become inevitable for the Lesotho health sector.
This area shows the investigation of writing on retention strategy for doctors and nurses. This review analysed proposing and contradicting disagreement on retention strategy to highlight best practice and distinguish implementation challenges based on a study plan. The plan of the literature review was to classify the research questions that would form the basis on which the study was conducted. The chapter begins with the definition of an implementation framework, the importance of implementation framework, synopsis of Lesotho’s different implementation framework success and failure factors, and how these factors can be incorporated in the revised and updated framework, and the need for a new implementation framework in Lesotho.
Importance of implementation framework
The implementation framework helps with rebuilding of future workers, managing and engaging the productivity of the present workers (Government of Health Western Australia Department of Health, 2012). It is proposed to attract and protect staff and meet existing and planned requests by expanding the importance and nature of the potential workers. It supports the plan stage by supporting careful examination of proof, helping one not to misuse inadequate resources (Health Workforce Australia, 2011). As per the Center for Mental Health (2012), the significance of an implementation framework is to take methodologies to the following level by grasping the vision of the association, bring about the genuine and quantifiable upgrades for individuals comprehensively through deciphering goals into real activity that can be utilized by the association.
Implementation framework defined
Nyamwanza and Mavhiki (2014) describe implementation as the way an association ought to develop, utilise and combine hierarchical structures, control frameworks and culture to take after methodologies that prompt viable and better implementation. As indicated by Li et al. (2008), strategy implementation is a key test for today’s associations. Organisation accomplishment is controlled further by how well techniques are actualised than by how extraordinary the approach is (Speculand, 2009); the implementation of the framework passes on returns, not the making of it (Speculand, 2009). Various structures have been made to help system implementation. Notwithstanding the way that associations welcome the prerequisite for technique and fruitful implementation, the last as often as possible comes up short concerning the targets the affiliation has set itself (Shah, 2005) as referred to in Nyamwanza and Mavhiki (2014).
Synopsis of Lesotho’s different implementation framework success and failure factors
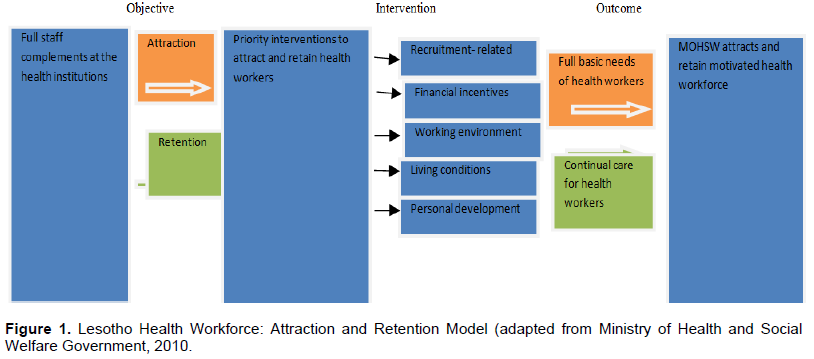
As per literature, many elements affect strategy implementation in an association and, thus, impact organisational performance (Belbin, 2011). A lot of variables can possibly influence a total strategy or one choice. Challenges frequently happen in the succeeding implementation advancement (Li et al., 2008). Managers’ view is frequently imperfect; therefore, in vast majority of times (9/10), they do not prevail to successfully implement the strategies they have made (Speculand, 2009). Speculand contended that managers continually think little of the test of implementing strategy, and accordingly assign the procedure to others, taking their eyes off what should be done; thus, strategies have inadequacies not because the methodology is not right, but rather that the implementation is ineffectively done (Speculand, 2009). The Lesotho retention strategy portrayed underneath has neglected to accomplish retention rate for doctors and nurses on the grounds that the implementation was poor (Ministry of Health and Social Welfare Lesotho, 2013). The Attraction and Retention Model of the Lesotho Health Workforce can be seen in Figure 1.
Incorporation of Lesotho success and failure factors in a revised framework
From the literature review, it is clear that the retention strategy presented earlier has neglected to enhance the retention rate for doctors and nurses in the country since there are insufficient health professionals to convey quality service to patients (Health Sector Strategic Plan (HSSP) 2012 to 2017). The researcher reasoned that managers have neglected to move from plan to activity. This model was implemented with no functional base to control the decision of mediation. The findings of its success and failure are outlined below.
Personal development: According to Dambisya (2007), the Lesotho Health and Social Welfare is offering bursaries/scholarships to students who are contemplating towards acquiring medical education in South Africa and other countries because there are no medical schools in Lesotho (Lesotho Health Sector Strategic Plan 2012/13 to 2016/17, 2013:18). This is in a form of a bonding agreement whereby graduates are required to serve the division for a time that is equivalent to the length of their education programs (Schwabe et al., 2004). This was believed to be a good retention strategy to absorb them into the public service pool during the agreement, however, it gives the idea this is insufficient as some of these doctors and nurses are set up to pay back the departmental expenses, rather than working for it (Dambisya, 2007).
Career/Promotion: In Lesotho, there is lack of opportunity to continue studies in the government health department even if in-service training is provided (Schwabe et al., 2004). There is also a glaring lack of career advancement in nursing; the profession hierarchy is restricted and progressive (Schwabe et al., 2004). In the case of the doctors’ cadre, the succession inside the Medical Doctor unit from Medical Officer to Specialist is small by territorial and worldwide measures (Schwabe et al., 2004). The Health Sector Human Resources Needs Assessment uncovered this, and also exposed the high extent of non-nationals in the Medical Officer occupation in Lesotho (Schwabe et al., 2004).
Working environment: For many years, infrastructure in Lesotho such as clinics and the main transfer hospital, Queen Elizabeth II in Maseru, was worse and the increasing population continued to apply pressure on both inadequate staff and facilities (Coelho and O’Farrel, 2011). In addition, several services were unavailable through the Lesotho public health system and patients were transferred to South African facilities for treatment at premium prices (Public Eye, 2012). Moreover, the National Referral Hospital (QE II) has turned 100 years old, and as a result required either replacement or extensive refurbishment (Netcare Limited Annual integrated report, 2013). The replacement was achieved through public/private joint venture (PPP) understanding between Ts'epong (a consortium involving South Africa's Netcare and a Basotho organisation) and the government of Lesotho through an 18-year PPP contract (Kaplan et al., 2013). The PPP managed to replace the aging QEII, and also improved the network of urban filter (Satellite) clinics (Mwase et al., 2010).
Living conditions: Most support efforts to improve living conditions for Lesotho have not yet been implemented (Ministry of Health and Social Welfare, 2013). Nurses in Lesotho are staying in residences that are not in good condition, while doctors are staying in better places with basic furniture but heat and electricity is a challenge there (Dambisya et al., 2013).
Recruitment related: According to WHO (2017), Lesotho has formed an alliance with Boston University called Lesotho Boston Health Alliance (LeBOHA) in an effort to improve recruitment of health professionals as approach to retain them. Likewise, as far back as the program began more than 30 specialists have connected to come back to Lesotho to join the Family Medicine Speciality Training Program (FMSTP) but only three students were absorbed (WHO, 2017). LeBOHA has not succeeded in getting on a correspondence operation in the media to advance the arrival and retention of doctors, in an effort to attract Basotho doctors back to the country (Rankhone, personal communication 10 May 2015). LeBOHA has also failed to assist the government of Lesotho in drawing a database in order to trace medicinal students, understudies and specialists in the neighbouring country (South Africa) in an effort to comprehend the target audience of the campaign (Rankhone, 2015).
Incorporation of Lesotho success and failure factors in a revised framework
Financial incentives
As indicated by Kossivi et al. (2016), the connection amongst pay and retention has been the subject of many studies. Researchers are not consistent about the effect of pay on retention. For a few, fulfillment with pay emphatically connects with the representative choice to remain in the organisation. For others, pay does not impact on retention (Kossivi et al., 2016). It is imperative that the revised framework will undertake to eliminate inequality and discrimination by not considering equity of pay within Lesotho but also in comparison with neighbouring countries and/or Africa. In terms of salary inequality, doctors and nurses should be paid for their competencies, not supplementary qualifications they hold; they are a team that requires full participation and expertise of both. The updated and revised framework should also include the provision of education allowance for health workers’ children in order to supplement their salaries, waive entry exams to school graduates wishing to study towards health related qualification, provide postgraduate education to young general practitioners, provide subsidised mortgages and homes in areas with a shortage of health workers, provide health workers with supplemented income from donor projects and the MOHSW to implement new incentive programs that will be essential to monitor results and lessons learned to be disseminated to other countries (Kaplan et al., 2013).
Personal development/ Career and promotion
Skilled improvement is not a least retention cause (Kossivi et al., 2016). Hiltropp (1999) sees professions achievement and organisation as the capacity to make representatives remain in their employments. Individual and expert development is a deciding element of retention and advancement openings expand representative responsibility regarding stay (Kossivi et al., 2016).
Leidner (2013) is likewise of the view that representative reliability is enhanced through guidance and growth (Kossivi et al., 2016). It is necessary that in a revised framework, the ministry of finance should, for the sake of consistency, bring some standardisation to the layout of bond understanding and question the conditions to make them more unequivocal and exhaustive for the gatherings to know about the different ramification of breach of understanding.
A bank guarantees that expenditure incurred for sponsorship/traineeship can be easily recouped. In case of breach of obligations, employees subscribes to a bank guarantee and its service charges and graduate certificates are to be confirmed after the proof of service.
In its response, Lesotho should provide clearly defined and transparent career paths, promote them and also open new medical schools by training new therapeutic schools via preparing new units of health professionals and bringing in doctors as a temporary solution.
Working environment
According to Kossivi et al. (2016), a helpful workplace has all the earmarks of fundamental figure worker retention. Spence et al. (2009) confirm supporting the way that ideal workplace adds to representative retention. A useful situation can be characterised as an adaptable environment where working knowledge is agreeable, assets are sufficiently given. On the other hand, the researcher suggests that for further working condition improvement, the Department of Health should put in better equipment such as telemedicine to allow medical providers in isolated locations to confer with experts about diagnosis and cure.
Living conditions
The revised framework should provide benefits that are comparable to non-nationals, develop living condition for doctors and nurses and their relatives by putting resources into framework and administrations (sanitation, broadcast communications, pre schooling and childcare’s etc.), provide subsidies for water and electricity, and guarantee security and protection for doctors and nurses equally at and off work.
Recruitment related
The revised framework should suggest the building of a medical school in the country so that Lesotho will be able to make enough doctors and nurses to address the issues of its population. Moreover, a strong enlistment bundle and a coordinated enrollment and retention procedure - consolidated with the aggregate cooperative energy of the MOHSW systems and objectives - ought to work more in order to address the wide enrollment and retention needs. The basis should be to do projects and administrations that strengthen enlistment and retention, draw in MOHSW healing, exiles and universal graduates to advance professions in the country which will increase the capacity of MOHSW to attract and retain the specialists it requires.
Need for new implementation framework in Lesotho
Lesotho health sector has an employer of 8,600 staff individuals (Ministry of Health and Social Welfare, Government of Lesotho, 2009). Like some other Sub-Saharan nation, Lesotho is at present confronted with extraordinary difficulties to retain doctors and nurses (Ministry of Health and Social Welfare, 2009).
The number of inhabitants in Lesotho is around 2 million (WHO, 2009), which incorporates a devastatingly high human immunodeficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS) rate of 24%-an extreme deficiency of health professionals (Government of Lesotho, 2013). As indicated by the results, it is apparent that the Lesotho health sector is less compelling in conveying quality health services to its population because of the present situation (Ministry of Health and Social Welfare, 2009).
Not very many doctors and nurses are serving the extensive variety of truly sick patients (Smith and Stark, 2009) who require serious care. Basically, a compelling usage system is required to enhance the retention implementation of doctors and nurses, so as to achieve the nation vision 2020 with its vision articulation:
“By the year 2020, Lesotho shall be a stable democracy, a united and prosperous nation at peace with itself and its neighbours (Ministry of Finance and Development Planning, 2004)”.
It shall have a healthy and well-developed human resource base. Its economy will be strong; its environment well managed and its technology well established (Ministry of Finance and Development Planning, 2004). To make this vision a reality, the framework should concentrate on enhancing retention which will prompt successful service delivery. In this way people using health organisations alongside their families should get help and treatment they may require in all circumstances (Ministry of Finance and Development Planning, 2004). The framework for retention strategies used for doctors and nurses introduced underneath depends on the conclusion got from the audit of writing. It is normal that this framework would upgrade retention rate for doctors and nurses, and enhance service delivery in the association, especially, the hospitals through the implementation of retention elements approved to be viable in enhancing retention, and service delivery. This is reflected in the accompanying model (Figure 2).
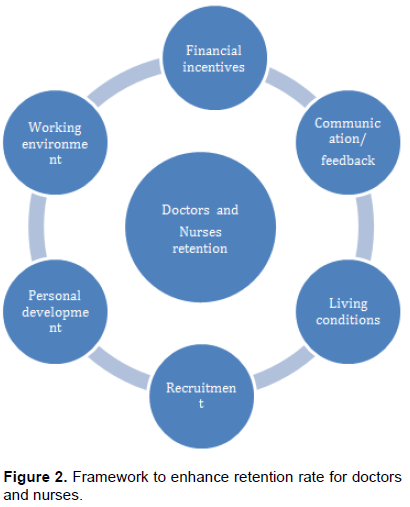
Framework to enhance retention rate
The researcher distinguished six key factors in particular:
1. Financial incentives
2. Working environment
3. Personal development
4. Recruitment
5. Living conditions, and
6. Communication and feedback which will be included in the improved implementation framework.
The researcher witnessed that strategies are commenced and implemented in a vital setting (the overall strategic direction of the company and the need to design new initiatives). Why are a few organizations ready to accomplish remarkable outcomes in both financial and additionally non-financial while others are not (Nyamwanza and Mavhiki, 2014). The implementation framework helps with rebuilding of future workers. It is planned to draw in and protect tremendously refreshing staff.
It advances the plan stage through cautious examination of confirmation, helps to avoid inadequate squander of funds or things that can harm effectively by planning and resourcing in an unexpected way (Health Workforce Australia 2011: National Health Workforce Innovation and Reform Strategic Framework for Action 2011 to 2015). As indicated by Center for Mental Health (2012), significance of implementation framework is to take methodologies to the following level by grasping the vision of the association, realize the genuine and quantifiable upgrades for individuals all around by interpreting beliefs into honest to goodness activity that can be utilised by association (Okumus,2001).
The aforementioned system recommends that if all hospitals utilize it, they would probably effectively implement strategy. Every hospital will highlight certain parts of the framework and accomplish distinctive outcomes. After that, the individuals who embrace the procedure will be closer to accomplishing their objectives while those that do not use this methodology will not accomplish preferred outcomes.
Research gap
Ongoing instability in the health workforce is bringing up issues worldwide about the problem of doctors and nurses turnover and retention. Studies have been carried out on the level of and extent of the health workforce turnover issue, turnover costs and the effect on patients, doctors, nurses and framework result (Onyango, 2016). Though there exists a body of literature on retention and turnover of workers in the human service, there is inadequate one on its extent originating from the extremely constrained measure of research that has been directed. Gaps in existing information incorporate the examination of large scale level variable, for example, organisation size, setting, structure and funding status (Barak, 2001) as referred to in Onyango (2016). Con-sequently, there exists a solid requirement for replication studies. In Lesotho, for instance, literature accessible is from research done in government and Christian Health Association of Lesotho (CHAL) organisations; there is a need to research the same in private facilities.
This research work utilizes two research techniques, qualitative and quantitative techniques: A survey using a research instrument constituted of both Five Point-Likert Scale questions (closed-ended) and open-ended questions and interviews. Three hospitals were selected using simple random sampling. The support of this procedure depends on the way it enables each subject in the examining edge to control circumstances, to be chosen without predisposition in an efficient way.
The essential information incorporated an assessment of the hospital retention strategy and in addition a directed survey on 120 doctors and nurses and personal interviews. The questionnaire was self- directed. An audit of authentic archives was done similarly to throw more light on the organisation retention strategy based on the shared accord amongst doctors and nurses and administration in terms of financial and non- financial incentives. The kind of information gathered was mainly essential. These were gathered
utilising survey and personal interviews.
The questions were done in a way whereby the respondents would give answers to a number of the research questions. Other documents inspected were journals, newspapers, magazines, websites, records, reports relevant to research, textbooks and articles of the Ministry of Health and Social Welfare.
Data collection procedure
Questionnaire
A self-administered questionnaire was used. The instrument was taken from Kukano (2011) and Lennie (2008); nevertheless, a couple of changes were made by the researcher to fit to the present study. The questionnaire was administered among one hundred and twenty (120) doctors and nurses in their hospitals during lunch break. The questionnaire involved 39 items. The first part of the instrument contained a statement of purpose and heading, and was intended to gather biographical or individual information that incorporates place of work, age, gender, and marital status, home language, position, job status, educational attainment and years of work experience with Scott, Mohlomi and Bots'abelo hospitals. The second part of the questionnaire contained headings and 29 five point Likert-scale items for rating the present retention strategies actualised by the Ministry of Health with a particular ultimate objective to improve retention rate of doctors and nurses in Lesotho. The items asked the participants to rate how much they agree or disagree with certain areas of their retention at their different hospitals. The rating scale is thus: 5=strongly agree; 4=agree; 3=neutral; 2=disagree; 1=strongly disagree. By using questionnaire, the research would have a superior likelihood of giving a more precise impression of the pattern of reactions. Reactions were then assembled and evaluated as they answer the question item.
Interview
Interview guides were planned for every hospital to guarantee that the interviewees in every hospital were asked similar questions (Nyamwanza and Mavhiki, 2014). Subsequent to making the essential arrangements, the researcher visited the hospitals concerned to direct the interviews. The interview happened in April 2015; it lasted from 30 min to 1 h in doctors’ lounge. Consent was given by the members to record the interviews. This was used to limit interruptions in the interviews and to empower the members to speak completely about all issues relating to current retention strategies. The interview was done according to interview guide using semi structured approach that allows the members respond well and ensures the flow of the interview. The focus of the interview questions was to allow for more in-depth discussion around the questions that are presented in the questionnaire.
Piloting and response rate
From studies similar to the current one, survey has been disputed to be ineffective as it does interfere with employees’ jobs. However, 60% response rate was experienced in this study as it is supported by the findings of Mugenda and Mugenda (1999). The questionnaire was pilot tested in three hospitals namely Scott hospital, Mohlomi hospital and Bots’abelo hospital. Health professionals were randomly selected from the population reflected in the study, but they were not part of the sample Table 1).
Data analysis
The quantitative data were evaluated utilising the computer software statistical Package for the social Sciences (SPSS). The researcher compiled information as frequencies, and represented them in tables. The subjective information was compiled utilising the simple descriptive percentage method and the information was continually compared.
The research design, methodology, research procedure, respondents of the study and the instrument used were described earlier. This chapter discussed data presentation, analysis and interpretation based on responses received from the respondents (doctors and nurses at the hospitals, Scott, Mohlomi and Bots’abelo). Therefore, the focus of this chapter seeks to answer the study inquiry and purpose of the research. As information was presented, it was crucial that the limitations perceived from the returned questionnaires be drawn.
Response rate
The study focuses on a sample size of 120 which includes doctors and nurse. 10 doctors and 62 nurses filled and returned the questionnaire making a reaction of 60%. This reaction rate was sufficient to make conclusions for the study. The reaction rate was representative. According to Mugenda and Mugenda (1999), a response rate of 50% is adequate for the study and report, a rate of 60% is great and a reaction rate of 70% and over is fantastic. Based on the statement, the reaction rate was viewed as great (Table 2). Table 2 delineates the response rate of usable questionnaire.
Descriptive statistics
Descriptive statistics (numbers and rates) was utilised to determine the biographic information. For retention factors, it incorporates occupation of the respondents, their age, gender, home language, position, current job and level of education. As per Iwu (2012), each instrument must be evaluated before it is utilised for both validity and reliability purposes. The validity and reliability of the instrument were tried by directing pilot study with 100 members (Table 3).
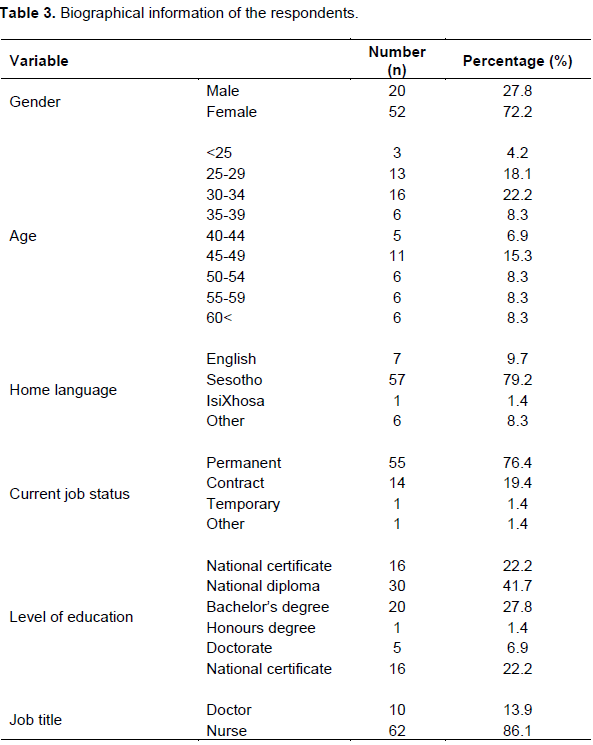
As per the outcomes, a sum of 72 respondents took part in the study. Table 3 demonstrates that most of the members were females (72.2%). This is an indication that both genders were well involved in this study and thus the findings did not suffer from gender bias. The nursing profession is mainly female dominated hence the gender disparity.
The least age of respondents was <25 years and the greatest age was >60 years. Larger parts of respondents were between the ages of 30 to 34 (22.2%). This is an indication that the respondents were fairly distributed in terms of their age group. The greater parts (79.2%) of the respondents were Sesotho speakers. This implies that the respondents were in a position to give credible information relating to this study. The study demonstrated that almost 75% of the respondents (76.4%) were for all time working at this hospital.
This implies that the findings of this research were fairly reached. With respect to level of education, 41.7% of the members hold a National Diploma while 27.8% had a Bachelor’s degree. This implies that majority of the respondents were well educated, which implies that they were in a position to give credible information relating to this study. The bigger percentage was nurses (86.1%), while the remaining 18.42% were doctors. This implies that both the respondents were fairly drawn putting into consideration their duties.
Quantitative findings
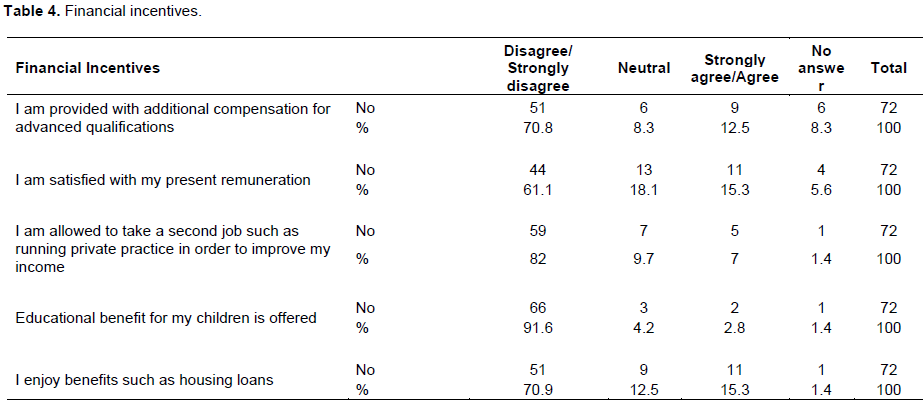
Quantitative findings used frequency and percentage to investigate retention factors. Res-pondents were made to determine the retention strategies utilised at their particular hospitals. The researcher was intrigued to know which strategies were unsuccessful and prevailing so as to build up another structure. The rundown of things outlined from retention strategies for the health workforce, implemented in 2010 by the Ministry of Health was utilised for the respondents to give their perspectives. The questions were replied in a 5-point Likert scale ranging from one to five:1 = strongly disagreed, 2 = agreed, 3 = neutral, 4 = disagreed, 5 = strongly disagreed. The respondents needed to tick to determine how much they agree/disagree with the statements. The retention strategy intervention factors are presented in Table 4. The responses from Table 4 present descriptive appraisal of a possible retention strategy using financial incentives. This presentation covers different levels of satisfaction amongst respondents as follows:
Additional compensation for advanced qualification
At this level, 12.5% of the respondents agreed that they were given additional compensation for higher qualification, while 7.8% disagreed. However, 8 respondents representing 8.3% of the total sample did not respond. Although 12.5% agreement is low, the best part of health professionals expressed the need to be appreciated and cared for; these feelings influencetheir inspiration and level of dedication to their job.
Satisfaction with remuneration is analysed as follows
15.3% of the respondents agreed that they are happy with the present remuneration, 61.1% disagreed, and 18.1% remained neutral while 5.6% did not respond to the statement. In the aspect of retention, 15.3% agreement is low; the majority of respondents indicated that allowances - especially risk allowance - that were withdrawn with no valid reasons and small salaries that do not meet their needs. These appear to have a large impact on why employees leave, and are a major problem with regards to retention issues that the organisation should capitalise on in future to enhance retention. The prizes offered to staff must be significant keeping in mind the end goal to affect their views of the institute and in this manner impact its retention activities.
Private practice involvements at this level
5 respondents representing 7% of the total sample agreed that they are allowed to take a second job such as doing a private practice, in order to improve their income; 82% disagreed and 9.7% remained neutral. However, 1 respondent representing 1.4% did not respond. The majority of respondents disagreeing probably considered this element essential to retention, since the hospital cannot accomplish its vital objectives of retention in the atmosphere of aloofness and despair. Health workers in Lesotho are paid fixed monthly salaries. They felt that they are dishonored as they lead a low standard life in contrast with the rank they possess. The submissions are in agreement with those of Amani (2010). This result confirms the finding of Dovlo (2004) that demonstrates the strong link between salary level and retention. As a result, to acquire positive inspiration, it is significant to build the basic passion for the occupation and give representatives an awareness of other's expectations, accomplishment and development, which involves humanising their purchasing power.
Educational support at this stage
2 respondents representing 2.8% of the sampled population agreed that educational benefits for the children is provided, 91.6% disagrees, with 4.2% remaining neutral with regards to the statement. Nevertheless, 1.4% did not respond to that view. The number does not signify a decent rate that shows support in terms of monetary incentives such as provision of educational benefits to health professional’s children. Money related motivation is a great degree alluring to workforce as they get the advantage rapidly and in solid terms. They believed that providing educational benefits would compensate for their low salaries.
Benefits such as house loans, at this point
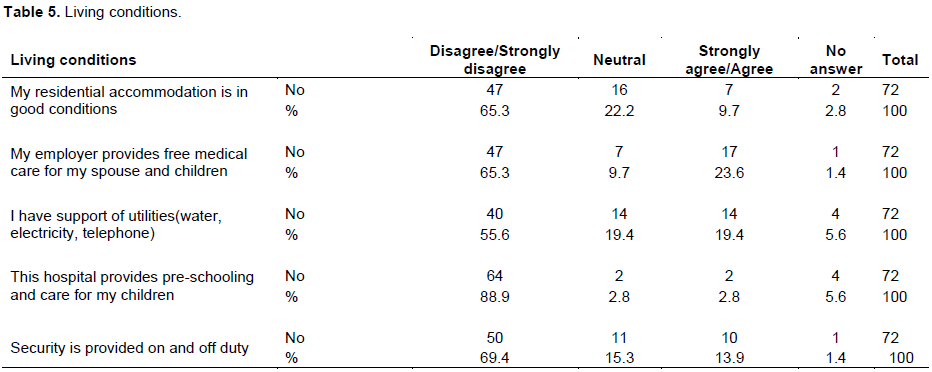
70.9% of respondents disagreed that they enjoy benefits such as house loans, 12.5% remained neutral whilst 15.3% agreed. However, 1 4% did not respond. With very low salary levels, benefits such as those for housing assume improved significance. Majority of respondents suggested that the level of salary is too low to accommodate house loans. Housing is the biggest expense for health workers and most suggested that loans are inadequate due to their low salaries. This forces them to leave. The majority of them recommended that purchasing a house is one of the main objectives for relocation (Table 5).
Conducive residential accommodation at this level
9.7% of the respondents agreed that the residential accommodation is in good condition, 65.3% disagreed, only 22.2% remained neutral to the statement. And 2.8% did not respond to the statement while the 9.7% agreement is very low; majority of nurses indicate the poor residential accommodation compared to those of doctors. They felt that they are discriminated against and not taken care of. These nurses articulated the need to be respected and recognised by maintaining least values for living conditions with excellent emphasis on physical comfort, because these practices can address retention issues. The result confirms the findings of Professor Alan Brown that housing is extremely significant and workers acknowledge least standards.
Provision for free medical care, at this stage
23.6% of respondents agreed that free medical care for spouse and children is provided. Only 65.3% disagreed, while 9.7 % of the respondents were neutral. Never-theless, 4 respondents on behalf of 5.6% of the whole example did not reply to the description. They feel they are not being appreciated. Respondents articulated that giving competitive things like medical assistance and health plans send influential messages to human resources about their significance in the association. They indicated that when prizes given to workers are significant, it impacts on their impression of the association and in this way affect its retention actions. Employees need to be provided and supported by a comprehensive health insurance scheme. These advantages will improve workforce achievement and retention; as a result guarantee accomplishing organisational goals.
Support of utilities (water, electricity, telephone) at this level
19.4% of the respondents agreed and neutral respectively that they have support of utilities, 55.6% disagreed, only 5 respondents representing 5.6% did not respond to the statement. While the 19.4% agreement is low, the majority of respondents specified the lack of utilities at their residential accommodation; they spend days without running water and paying for electricity that is too costly to pay for. The respondents believe that accessibility of facilities can improve retention by attracting and retaining other available labour pools, as well as non- national workers. Employees feel more relaxed in safe and protected housing with all the services. Management should play a leadership role by providing high excellent accommodation that is efficient element to achievement because it can help to retain workers who may struggle with the problems of living in a remote location, away from home or family.
Provision of non-financial incentive at this level
2.8% of the respondents are neutral and agreed respectively that they were provided with pre-schooling and care for children, 88.9% disagreed. However 4 respondents representing 5.6% of the total sample did not respond. The 2.8% agreement is very low; the majority of health professionals expressed the necessity to be assisted. They expressed that practices, for example, making day care services accessible in the premises can assist them to keep up stability among individual and work life. These would therefore advance retention, as it encourages employees to spend extra time with their kids, and bring about strong work/life goals.
Security at this level
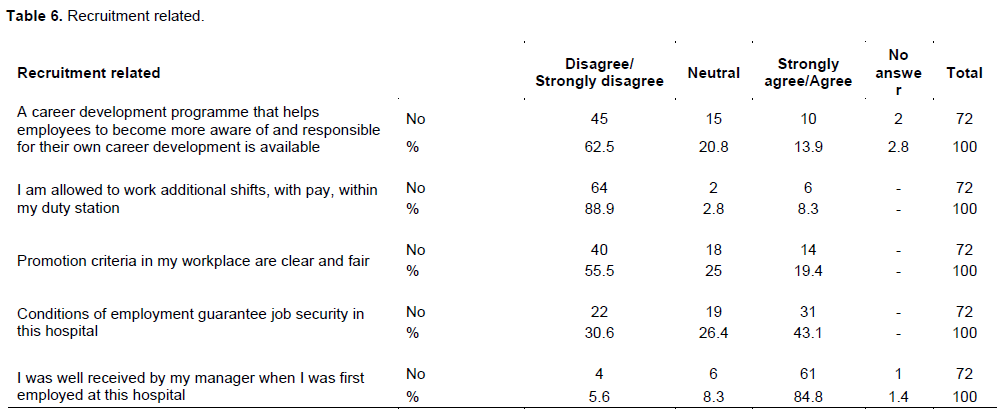
13.9% of respondents agreed that security is provided on and off duty. Only 69.4% disagreed, while 15.3% of the respondents were neutral. On the other hand, 1 respondent on behalf of 1.4% of the whole example sample did not reply the statement. The majority of respondents attributed insecurities. Employees point out that their objective to stay and be focused on an organisation could be clarified inside the setting of Abraham Maslow's hierarchy of needs theory. The theory explains that individuals are influenced to fulfill five need levels and the second lower level of the hierarchy represents safety needs, which can be satisfied through protection from elements, security, order, law, stability, and so on. In the event that these necessities are not satisfactorily fulfilled, then the individual hunts for another job. In order to enhance retention, employees need a place with zero tolerance for violence; they need to be safe and relaxed enough to deal with patients and management demands every day (Table 6).
Available career development programme at this level
This study indicated 62.5% of the respondents disagreed that their organisation had a profession improvement program that helped them to end up distinctly more mindful of and in charge of their profession advancement, and 13.9% agreed. Almost 20.8% were neutral while 2.8% did not respond. Though less percentage agreed, the majority of them talked about lack of career development plan, which results in the hospital
being unable to retain skilled doctors and nurses.
Permission to work additional shifts, at this stage
88.9% of the respondents disagreed that they are paid for additional shifts within their duty station. Only 8.3% agreed while 2.8% were neutral. Most participants complained about perceived higher work overload within their duty stations without additional pay, which results in failure to deliver high-quality care due to lack of incentive. They recommended remuneration as an act of appreciation for added effort invested. In this study, it was discovered that the existing salary structure provides no incentives for additional shifts.
Promotion opportunities at this level
Is characterised by the fact that 19.4% agreed that the promotion criteria in the workplace is clear and fair, 55.5% disagreed and 25% were neutral. In this study, participants articulated that there is lack of understandable structures at the Department of Health for promotion. The majority indicated that it is often vague. Health workers believe chances for promotion is among the mostly important rationale why employees terminate their service. A relative study was done among13 British universities and found that over a quarter of academics were in the top of their academic scale, which meant no promotion or progression beyond annual “cost of living” (Netswera et al., 2005). When employees experience that they have outgrown their assignments and that additional preparation does not upgrade their profession moves inside the organisation, they choose to depart. And also the limited self-development opportunities cause them not to stay similarly located for the next upcoming years.
Conditions of employment at this point
Revealed that 43.1% of the respondents agreed that conditions of employment guarantees job security, 30.6% disagreed while 26.4% were neutral. The 43.1% signifies a good percentage that reveals provision of job security in the hospital. The majority articulated that professional constancy is useful for the stimulation of staff. Such protection keeps them away from the apprehension of becoming jobless. This result proves the findings of Nyamekye (2012) that employees will be common just when they are treated with kindness, love, warmth and pride.
First day at work is analyzed as follows
84.8% of the respondents agreed that they were well received by their managers when they were first employed at the hospital, 5.6% disagreed, 8.3% remained neutral and 1.4% did not respond to the statement. This appears to have a large impact on employee retention. Participants indicated that early introductions are enduring; the way an employee is introduced to the organisation from the principal day at work sets the tone for how they feel regarding the organisation. Therefore, a meaningful orientation program with several sessions of follow-up is recommended. They indicate that the sooner a new employee gains a comfort level, the earlier another employee picks up a solace level; and the sooner that individual will get to be distinctly gainful, also giving out data about the organisation, such as, its main goal, items, administrations, history, objectives, structure and so forth will set up a firm connection between the individual and the organisation from the onset. And, this will make it less demanding for an employee to relate to the organisation and discover importance in the work; and as a result increase retention (Table 7).
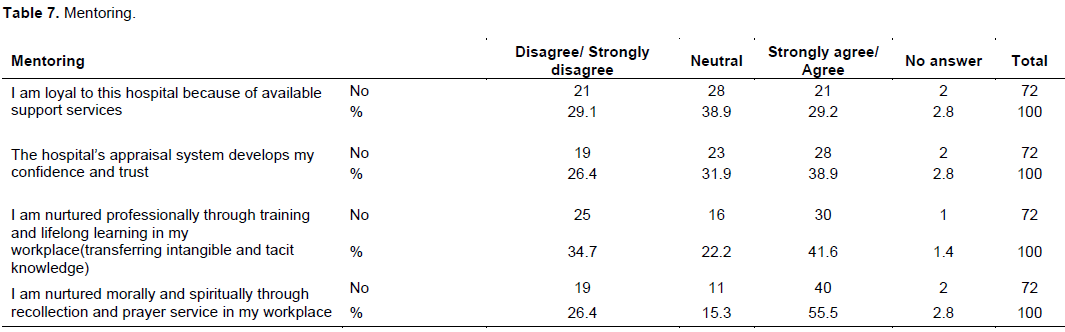
Loyalty to the hospital at this point shows
29.2% agreed that they are loyal to the hospital because of available support services, 29.1% disagreed, and 38.9% neutral. Nevertheless, 2 respondents representing 2.8% did not respond.
Although the percentage of agree and disagree about lack of loyalty was similar, those who disagreed indicated that they deserve support services, especially mentorship from this hospital. Yazinski (2009) indicated that a mentoring program integrated with a goal-oriented feedback system provides a structured mechanism for developing strong relationships within an organisation and is a firm foundation for employee retention and growth.
Development of confidence and trust
This stage indicated that 38.9% agreed that the hospital appraisal systems develop their confidence and trust, 26.4% disagreed and 31.9% were neutral. On the other hand, 2.8% did not respond to the statement. The figure represents a good percentage that reflects an environ-ment with trust and confidence. The 38.9% indicated that performance appraisal encourages an open and trusting relationship within the hospital and as a result, increases work fulfillment by advising groups when an occupation is well done and assisting them to develop where they go wrong.
Transfer of intangible and tacit knowledge is analysed as follows
41.6% of the respondents agreed that they are nurtured professionally through training and lifelong learning in the workplace(transferring intangible and tacit knowledge), 34.7% disagreed, 22.2% were neutral and only 1.4% did not respond. The majority of agreement (41.6%) indicated that mentoring is efficient between generational learning exchange instruments and might be especially imperative to an organisation experiencing retention problems. According to Frank as cited in Ghansah (2011:61), mentoring is successfully well known to most organisations as a preparation mechanism; nevertheless it is similarly imperative in exchanging insubstantial and inferred information. The findings are in line with those of Frank as cited in Ghansah (2011: 61). This outcome confirms the finding of Hom (1995) which indicates that mentoring is a practical way for employees to give out “lessons learned,” as the mentoree time and again has the chance to profit by the coach's experimentation encounter.
Nurturing morally and spiritually at this level
55.5% of the respondents agreed that they are nurtured through recollection and prayer service in the workplace and 26.4% disagreed. Only 15.3% were neutral, while 2 respondents on behalf of 2.8% of the complete example did not reply. From the aforementioned, it means that the management – employee, employee– employee relationship and support is generally good. It is understandable that there is inspiring communication in the place of work. When employees are not working in isolation, the peer support and sharing of ideas will raise a professional environment and thus advances retention (Table 8).
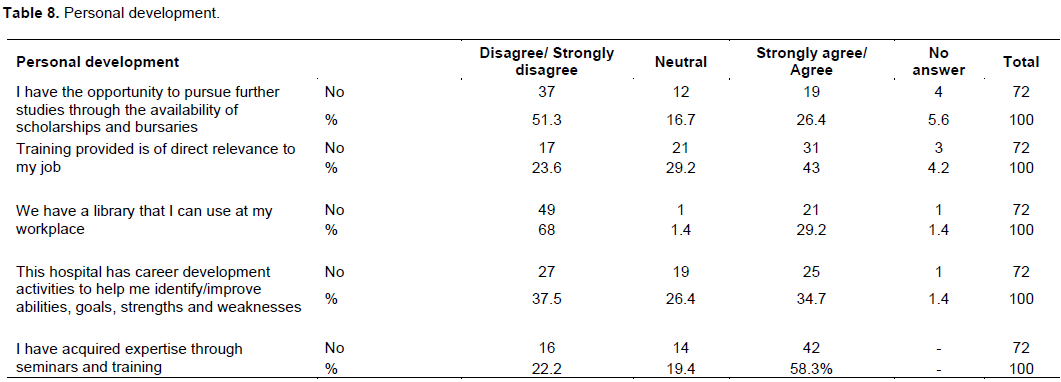
Availability of scholarships and bursaries at this point
51.3% of the respondents disagreed that they have opportunities to pursue further studies through the availability of scholarships and bursaries, 26.4% agreed and 16.7% were neutral while 5.6% did not respond. These results show that the employers do not financially support health professionals to pursue further studies. The fact that there is no medical school in the country is the barrier to retention, because those awarded scholarships to study abroad produced graduates that are unable to meet demand and therefore impact negatively service delivery. The participants mentioned that they have to take an online course which is self-sponsored should they want to pursue additional studies, and also indicated that the experience of failing to obtain sponsorship or bursary can be a critical obstacle to retention as they expect these training opportunities to be a basic entitlement for the workforce in the public sector.
Provision of training at this level showed
43% of the total sampled agreed that training provided is of direct significance to their job, and 23.6% disagreed while 29.2% were neutral. On the other hand, 4.2% respondents did not respond to the statement. From the above, it is evident that a remarkable number of doctors and nurses are taking up duties that are in line with their preparation or potential. The submission agrees with Muula and Maseko (2005), who indicated that preparing can be an inspiring variable that helps with the retention of healthcare professionals.
Access to library at this level
68% disagreed that they have a library that they can use in the workplace, 29.2% agreed and 1.4% were neutral and not responding respectively. The study showed that 68% of the respondents need a library in the workplace in order to be kept abreast with unknown and latest diseases, and to sharpen their knowledge and skills for effectual service delivery.
Career development activities
34.7% agreed that the hospital has profession advancement exercises to help them recognise/enhance capacities, objectives, qualities and shortcomings; 37.5% disagreed and 26.4% were neutral. Only 1.4% did not respond. With the results above, there appears to be a great need for career development that is not currently being addressed. Perhaps it is merely a perception of employees that one can constantly expect to be groomed by the organisation in order to develop in the above-mentioned areas of development. Consequently, the Ministry of Health should accord these actions to employees in order to generate a motivating and demanding environment.
Acquisition of expertise at this point
58.3% agreed that they have acquired expertise through seminars and training, 22.2% disagreed and 19.4% were neutral. The agreeing figure reflects a good percentage that reflects provision of seminars and training in the hospital. The respondents revealed that they perceived seminar places as excellent motivation for professional advancement as it is crucial to amend their knowledge with a definite end goal to address the problems of patients. The results are in line with those of Butler (2005) as referred in Mokoka et al. (2010), who maintain that the great work environments are areas where medical caretakers are provided with opportunities to develop (Table 9).
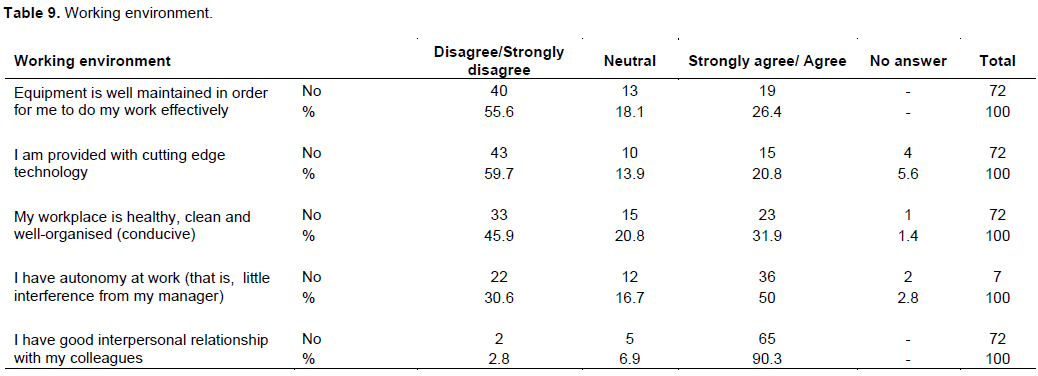
Availability of equipment at this level
55.6% disagreed that equipment is well maintained in order for them to do their work effectively, 26.4% agreed while 18.1% were neutral. From the information aforementioned, it is clear that the performance of health professionals is negatively affected due to lack of equipment.
The respondents declared they that no one cared for them as they lacked drugs, equipment and had problems related to staff which they experienced every day. In this study, the respondents showed lack of equipment, mostly circulatory strain machines and bed cloth is very upsetting, because it has unconstructive impact on the nature of care. According to respondents, the lack of linen in the hospital was the reason for patients developing bed sores as it was difficult to keep patients dry at all times. The terrible working conditions made it difficult for these hospitals to maintain healthcare professionals.
Provision of technology at this level shows that 59.7% disagreed and 20.8% agreed that they are provided with cutting edge technology, while 13.9% were neutral. However, 5.6% did not respond. The participants indicated that there are no computers in the workplace; lack of satisfactory innovation remains a major obstacle to the Lesotho prescription and conquer the test of the present day solution, therefore execution and the nature of care suffers.
The Ministry of Health should make it a priority to provide hospitals with computers in order for healthcare professionals to be kept abreast with advances in technology to improve the quality of care. This statement was confirmed in the study conducted in the North West region of Cameroon, by Tita et al. (2005), who found that the dearth of essential supplies was felt by many healthcare employees to hinder their utilization of proof based-and basic medication. The respondents recommended an introduction to advance technology to assist them treat patients distantly.
Conducive working environment at this level
31.9% agreed that the workplace is healthy, clean and well-organised (conducive), 45.9% disagreed while 20.8% were neutral. Conversely, 1 respondent representing 1.4% did not respond. In the present study, the working environment is not safe; the units are overloaded, exposing the respondents and other healthcare providers to communicable diseases. Moreover, the patients are also exposed to universal infections because of the shortage of separation units. The hospital buildings were not up to standard.
The respondents working in female wards at mental institutions feel unsafe due to physical attacks from patients. The majority of respondents cited hazardous work environment, some working in specific areas such as low-cost wards, theatre departments and labour wards seeming that they were exposed to a higher risk of disease. Low-cost wards generally have unclean conditions and there is higher exposure to human immunodeficiency virus (HIV) in labour wards due to regular needle-stick injuries and a shortage of protective measures.
Although the supply of gloves and gowns seems adequate, some basic protective equipment such as goggles and shoes are not provided. The dangerous working environment needs to be addressed, as the work of doctors and nurses is very demanding and hard work should be made to guarantee that they can carry out their employment well by using their insight without limitations, inside a protected location. This ought to bea basic element of any strategy to improve retention of staff.
Autonomy at this stage is analysed as follows
50% agreed that they have little interference from their managers in the workplace, 30.6% disagreed and 16.7% were neutral. However, 2.8% did not respond. This figure reflects a good percentage that shows autonomy in the workplace. This study has shown that autonomy is offered by these hospitals and also fewer repetitiveness of the job which is likely to impact work accomplishment. Worker cooperation enhances inspiration through power sharing and expanded duty, which is seen as a sign of positive reactions. Workers’ teamwork allows people to settle on main administrative decisions that influence different workers. This leads to increased work achieve-ment and implementation, which in turn enhances retention.
Interpersonal relationships at this stage
90.3% agreed that they have great interpersonal relations with their co-workers, 2.8% disagreed and 6.9% were neutral. A number of members noticed that friends in the work environment could impact health workers’ choice to stay or leave, as well as fellowship and support amongst co-worker and companions. Few narrated that workers are occasionally ill-treated in words and physically by patients and their relatives. Mokoka et al. (2010) agreed with this, where relations with co-workers were positive and collegial; workers agreed that patients likewise got great care, while medical caretakers who helped each other made the workload more manageable, adding to lower turnover rates in such hospitals.
Qualitative findings
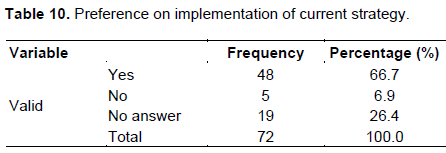
The qualitative data were broken down utilising grounded theory approach depicted by Strauss and Corbin (1990). This uncovered the achievement and disappointment elements of methodologies presently implemented by the Ministry of Health. Members were questioned about their perspectives on the present retention strategies whether they wish it to be implemented in contrast with an end goal to upgrade retention rate (Table 10).
In Table 10, 66.7% respondents prefer their current strategy be implemented differently, whereas 6.9% do not prefer a different implementation. Only 26.4% did not respond to the inquiry. The preference of bigger part of the respondents is because of the way the existing retention strategy has failed to retain doctors and nurses in Lesotho (Table 11)
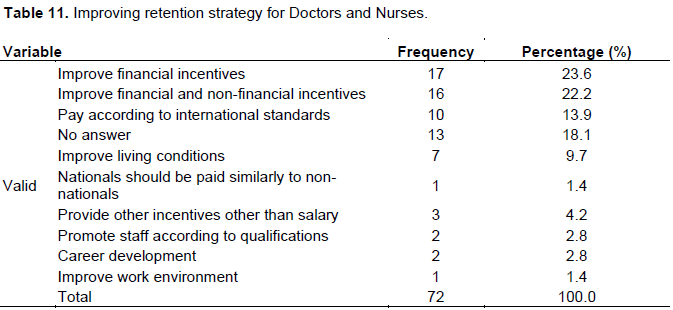
As seen in Table 11, different views surfaced from this study. The most reasonable answers are: improve financial incentives according to 23.6% of the participants. Another factor is improving financial and non-financial incentives according to 22.2% of the respondents and to compensate according to international standards according to 13.9% of the participants. This is identified in many studies, articles and responses from the interviews and it is believed to have some retention influence on health professionals. The diverse pay structures that are utilised by organisations in Lesotho permit flexibility for the private sectors and parastatals to set aggressive pay packages, leaving government lagging behind in payment. As a result, inhabitants depart for greener pastures (Table 12).
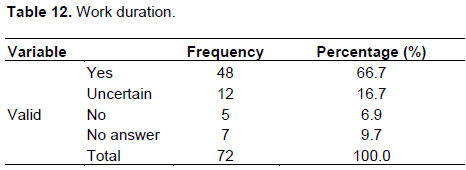
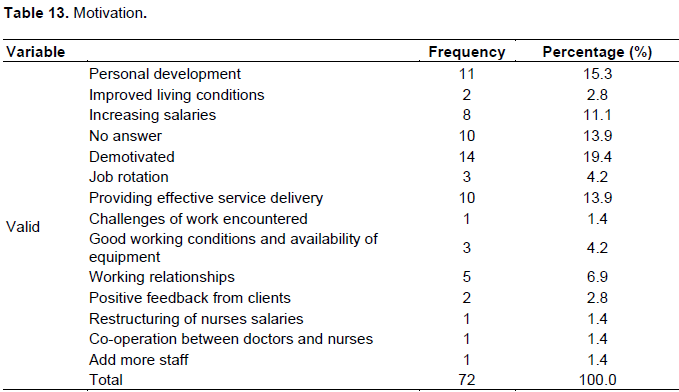
To this question, 66.7% of the participants will continue working in this hospital in the next 12 months, whereas 16.7% are uncertain. Only 6.9% will not continue. The choice of employees will always differ, as there are many factors involved. What may be a reason to one individual may not pertain to another. However, some of the reasons for wanting to leave the hospital include workload, lack of service delivery, lack of career develop-ment, non-conducive work environment and small salary (Table 13).
In Table 13, the necessary motivational reason to stay with the hospital is personal development, as shown by 15.3% of the participants. Moreover, salaries were improved as outlined by 11.1% of the respondents.
However, 19.4% of the respondents were demotivated. And lack of motivation discourages retention (Table 14).
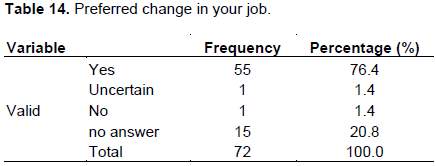
This study confirms that most of the participants consent that there is something that can be changed or improved in their jobs: 76.4% of the participants believe that changes or improvements can be made in their jobs.
As distinguished in literature at some point after the implementation strategy, some factors failed. An example of such as noted in the literature review is that the payment of incentives and allowance in Lesotho was initially unequal and unreasonable.
There are no medical schools in the country, which results in losing doctors to the South African healthcare system after the completion of their training. Clinics and the main transfer hospital Queen Elizabeth II in Maseru were in a terrible condition and the growing populace was treated under pressure by both insufficient staff and facilities. It has also been noted that there is an imbalanced allocation of residences among doctors and nurses. Nurses are staying at residences that are poor condition, while doctors are staying at improved places with basic furniture (Table 15).
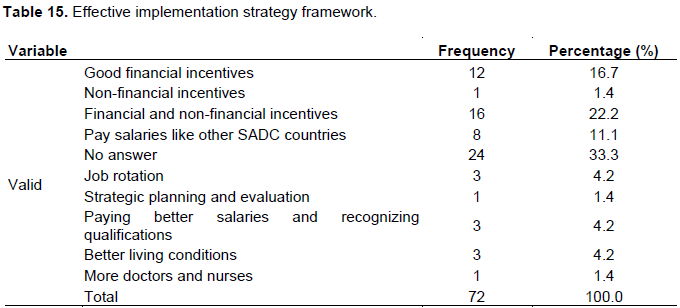
Table 15 shows that the most important reason to achieve desired retention strategies for doctors and nurses are good financial incentives, arrangement of monetary and non-monetary motivation and paying salaries similar to other SADC countries (16.7% good financial incentives, arrangement of monetary and non-monetary motivation (22.2%) and salaries similar to other SADC countries, 11.1% is for effective retention pay (Table 16).
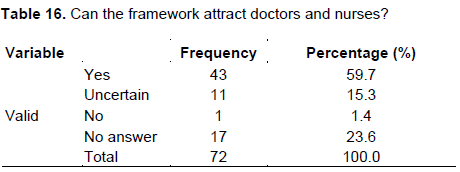
This study shows that 59.7% of respondents believe that the new implementation framework will be able to attract and retain doctors and nurses. An example that can be noted from the opinions given by respondents who has mentioned that improved living conditions, a conducive working environment, financial incentives and career progression, improved salaries, a sports facility that empowers workers to exercise and live a healthy life - all of these serve to increase retention.
For the outcomes of the questionnaire, the retention interventions, for example, the arrangement of financial and non-financial incentives as far as the retention of doctors and nurses in the health sector has been unsuccessful, both in literature in Lesotho and Sub Saharan nations. Most hospitals in Lesotho offer a lower compensation for public sector workforce serving in the nation than for those serving in private areas. However, the total of the incentive differs among divisions.
The study demonstrates that when the Ministry of health concentrates on financial and non-financial incentives, retention rate is low. This finding is similar to that of Ditlopo et al. (2011) past review who discovered that financial incentives alone are inadequate to hold health professionals. Ditlopo et al. additionally exhibits that non-financial incentives identified with working and accommodation conditions could impact retention. A few reviews perceived that health professionals will dependably move frequently for reasons beyond the impact of any workforce retention program.
Hence no single measure is probably going to enhance retention if different variables are not thought about. The afore mentioned factors clearly illustrate that employee retention factors such as financial incentives, personal development, living conditions, working environment and recruitment have a direct impact on retention. If these factors are present in the organisation the possibility for turnover decreases. It is clear that if the above mentioned factors exist in the organisation it will not only assist to attract new employees into the organisation but will also lead to the enhanced retention of the existing employees.
Results from Scott, Mohlomi and Bots'abelo hospitals’ interviews demonstrated that working conditions were not favourable for doctors and nurses. Doctors and nurses were not cheerful about the financial incentives provided. Their answers were fixated on improved pay and employee benefit. From the interviews, the researcher has found that remittances have some retention powers for nurses and doctors in hospitals.
The interviews established that the Scott, Mohlomi and Bots'abelo hospitals had inadequate education opportunities regardless of the guidelines. This illustrates that it might give qualified individuals who have worked for the office for at least 3 years and under 50 years old conditioned scholarship in a form of bonding strategy for durable training. Recruitment is done utilising diverse strategies, however the present doctors and nurses emergency in the Lesotho health sector affirms failure to create adequate quantities of expert health workforce. The nation has 89 doctors of which 80% are immigrants from other African nations; the majority are anticipating affirmation in South Africa to land higher paying positions. Nurses are likewise hard to find. There is proof of lack of housing. There are insufficient houses to suit all the key health workers. Accommodation board just prevails with regards to assigning houses to doctors, who value the houses given by the health offices; nurses remain in the houses that are in awful condition and minor upkeep of the houses does not succeed.
CONCLUSION AND RECOMMENDATIONS
The main finding of this study was that the present framework implemented by the Lesotho Health sector with an attempt to upgrade retention was unsuccessful. As seen in the problem statement, the present retention strategies have not enhanced the retention rate for doctors and nurses.
Regardless of this disappointment another imple-mentation framework ends up being vital for the Lesotho health sector to advance retention. The literature review could decide why particular elements were unsuccessful in supporting retention and definitely how the fruitful ones oversaw. This literature has been maintained by the outcome got from the feedback of the survey and interviews carried out at Mohlomi, Bots'abelo and Scott hospital. It can be seen from the analysis that the health sector does not have a viable framework as the present circumstance was described by absence of doctors and nurses, expanded workloads, and poor service delivery. The study suggests that Lesotho health sector build up a new implementation framework so as to accomplish its favoured purpose.
Lesotho health sector needs to implement framework that would enhance degree of consistency of doctors and nurses whose skills are basic to service delivery. Administration needs to set up an acknowledgment program for its health workforce. Lesotho ought to pay compensations that are reasonable as well as incorporate stipends. Doctors and nurses ought to be perceived for the association they make, to build up favourable workplace. Government ought to construct medical schools in the nation to help health professionals acquire higher qualification broadly without investing a great part of the energy out of the nation, build up an open criticism orientated environment and present retention framework arrangement which join a few parts of the private sector practices.
The authors have not declared any conflict of interests.
REFERENCES
|
Amani A (2010).The Health Worker Crisis in Cameroon. Thesis: Master of Public Health. Georgia State University.
|
|
|
|
Belbin C (2011). Employee Perceptions of Workforce Retention Strategies in A Health System. Dissertation: Doctor of Business Administration. University of Southern Queensland.
|
|
|
|
|
Centre for Mental Health (2012), Department of Health, Mind, NHS Confederation Mental Health Network; Rethink Mental Illness, Turning Point.2012. No Health without Mental Health: Implementation Framework. Department of Health. London. Available at:
View [Accessed 12 November 2014]
|
|
|
|
|
Coelho CF, O'Farrell CC (2011). "The Lesotho Hospital PPP Experience: Catalyst for Integrated Service Delivery." World Hospitals and Health Services: The Official Journal of the International Hospital Federation. 47(3):39-41.
|
|
|
|
|
Dambisya YM (2007). A Review of Non-Financial Incentives for Health Worker Retention in East and Southern Africa. University of Limpopo, South Africa. EQUINET Discussion Paper no.44.
|
|
|
|
|
Dambisya YM, Lipinge SO, Dulo C (2013). Assessment of the Support Needed for the Lesotho Recruitment and Posting Policy. University of Limpopo., South Africa. University of Namibia, Namibia. Mustang Management Consultants, Kenya. EQUINET.
|
|
|
|
|
Ditlopo P, Blaauw D, Rispel LC, Thomas S, Bidwell P (2013). Policy implementation and financial incentives for nurses in South Africa: A case study on the occupational specific dispensation, University of Witwatersrand, Johannesburg, pp.138-146.
|
|
|
|
|
Dovlo D (2004). The Brain Drain in Africa: An Emerging Challenge to Health Professionals' Education. 2(3):1-18.
|
|
|
|
|
Ghansah E (2011). The Role of Employee Retention on Job Performance: A Case Study of Accra Brewery Company Limited, Accra. Thesis: Commonwealth Executive in Business Administration. Kwame Nkrumah University of Science and Technology.
|
|
|
|
|
Government of Health Western Australia Department of Health (2012). East Perth Western Australia.
View [Accessed 10 July 2014]
|
|
|
|
|
Government of Lesotho (2013). Health Sector Strategic Plan 2012/13-2016/17. Department of Health. Maseru. Lesotho.
View [Accessed 19 April 2013]
|
|
|
|
|
Health Workforce Australia (2011). National Health Workforce Innovation and Reform Strategic Framework for Action 2011–2015.
|
|
|
|
|
Iwu CG (2012). A model of employee satisfaction amongst health-related professionals in South Africa: The case of Western Cape Province. Thesis: Doctor of Technology: Human Resource Management. Cape Peninsula University of Technology.
|
|
|
|
|
Kaplan AD, Dominis S, Palen JGH, Quain EE (2013). Human resource governance: what does governance mean for the health workforce in low- and middle-income countries. Available at:
View [Accessed 02 April 2015]
Crossref
|
|
|
|
|
Kukano C (2011). Implementing Personnel Retention Strategies at CorJesu College in the Philippines. Thesis: Master of Education. University of South Africa.
|
|
|
|
|
Kossivi B, Xu M, Kalgora B (2016) Study on Determining Factors of Employee Retention. Open J. Soc. Sci. 4:261-268.
Crossref
|
|
|
|
|
Lennie GM (2008). Retention Strategies for skilled SARS Customs Employees. Masters: Business Administration. Nelson Mandela Metropolitan University.
|
|
|
|
|
Lin YP (2007). The Correlation between Management and Employee Motivation in Sasol Polypropylene Business South Africa. Thesis: Magister Commerce: Business Management. University of Pretoria.
|
|
|
|
|
Matamane S (2014). Factors Affecting Turnover of Nurses in Rural Clinics of Lesotho.Thesis.Master of Business Administration.The UFS Business School University of the Free State Bloemfontein.
|
|
|
|
|
Mbah SE, Ikemefuna CO (2012). Job Satisfaction and Employee's Turnover Intentions in Total Nigeria Plc. In Lagos State. Int. J. Hum. Soc. Sci. 2(14):275-287.
|
|
|
|
|
Ministry of Health and Social Welfare, Government of Lesotho (2009). Continuing Education Strategy 2010-2015. Maseru. Lesotho.
|
|
|
|
|
Ministry of Health and Social Welfare Government of Lesotho (2010). Retention Strategy for the Health Workforce Available at:
View [Accessed 02 July 2013]
|
|
|
|
|
Ministry of Health and Social Welfare Lesotho (2013). Retention Strategy for the Health Workforce. Maseru. Lesotho.
|
|
|
|
|
Mokoka E, Oosthuizen MJ, Ehlers VJ (2010). Retaining professional nurses in South Africa: Nurse Managers' perspectives'. Health SA, 15(1):484-493.
|
|
|
|
|
Mugenda OM, Mugenda AG (1999). Research Methods: Quantitative and Qualitative Approaches. Acts Press, Nairobi.
|
|
|
|
|
Netswera FG, Rankhumise EM, Mavundla TR (2005). Employee Retention Factors for South African Higher Education Institution: A Case Study. SAJ. Hum. Resour. Manage. 3(2):36-40.
Crossref
|
|
|
|
|
Nyamekye F (2012). Impact of Motivation on Employee Retention: A Case Study of Standard Chartered Bank Ghana Limited. Thesis: Masters Business Administration. Kwame Nkrumah University of Science and Technology.
|
|
|
|
|
Nyamwanza T, Mavhiki S (2014). Strategy Implementation Framework Used by SMEs in Zimbabwe. J. Bus. Manage. 3(2):01-16.
|
|
|
|
|
Okumus F (2001). Towards a strategy implementation framework. Int. J. Contemp. Hosp. Manage. 13(7):327-338.
Crossref
|
|
|
|
|
Rankhone M (2015). Lesotho Medical Students Abroad. Personal Communication. 10 July 2015.
|
|
|
|
|
Smith B, Stark R (2009). Transforming District Health Services in Lesotho: A collaborative Program of the MOHSW and LeBoHA. Boston.
|
|
|
|
|
Schwabe C, Lerotholi K, McGrath E (2004). Ministry of Health and Social Welfare. Human Resources Development & Strategic Plan 2005-2025. Maseru.
|
|
|
|
|
Smith B, Stark R (2009). Transforming District Health Services in Lesotho: A collaborative Program of the MOHSW and LeBOHA. Boston.
|
|
|
|
|
Speculand R (2009). Six necessary mind shifts for implementing strategy. Bus. Strateg. Series 10(3):167-172.
Crossref
|
|
|
|
|
World Health Organization (2009). WHO Country Cooperation Strategy 2008-2013.Lesotho.Brazzaville, Republic of Congo. WHO Regional Office for Africa. Available at
View [Accessed 11 July 2017]
|
|
|
|
|
WHO (2017). Stemming and reversing the out-migration of human resources for health in Lesotho. Lesotho. Available at
View [Accessed 11 July, 2017]
|
|
|
|
|
Yazinski SK (2009). Strategies for Retaining Employees and Minimizing Turnover. University of Scranton.
|
|