Full Length Research Paper

ABSTRACT
Helicobacter pylori (H. pylori) is an important global public health concern. It infects approximately one half of the world’s population. Considering the broad spectrum of available H. pylori diagnostic methods and since a reliable diagnosis is mandatory both before and after eradication therapy; thus it is crucial to study the different methods to be able to select the highly accurate laboratory tests that could be used to efficiently diagnose H. pylori infection in clinical practice. In this descriptive-cross sectional study we aimed to evaluate some non-invasive techniques for the diagnosis of H. pylori infection in children and their mothers. Forty children and their 21 mothers who had gastrointestinal symptoms were included. Stool, serum and saliva samples were collected from each enrolled child and mother to detect H. pylori antigens (Ags) in stool using chromatographic immunoassay and IgG antibodies (Abs) in serum and saliva by enzyme linked immune sorbent assay (ELISA). Collected data were analyzed using IBM SPSS software package version. Thirty (75%) children were positive for stool Ags, 10 (25%) were positive for serum Abs and only 5.4% were positive for saliva Abs. H. pylori stool Ag test was the most reliable test in all studied individuals and testing H. pylori IgG Abs in serum was more useful in adults than in children.
Key words: Helicobacter pylori, H. pylori stool antigen, H. pylori antibodies, chromatographic immunoassay, ELISA.
INTRODUCTION
Helicobacter pylori (H. pylori), one of the most common bacterial pathogens in the world, is an important global public health concern (Cheng et al., 2009). This organism infects approximately one half of the world’s population and represents a key factor in the etiology of various gastrointestinal diseases, ranging from chronic active gastritis without clinical symptoms to peptic ulceration, gastric adeno-carcinoma, and gastric mucosa-associated lymphoid tissue lymphoma (Estakhri et al., 2008). The prevalence varies greatly between countries and between population groups within the same country and is inversely associated with socioeconomic status or household hygiene and sanitation (Hanafi and Mohamed, 2013). In developing countries, more than 80% of the population is H. pylori positive, even at young ages, while in developed countries the prevalence generally remains under 40% and is considerably lower in children and adolescents than in adults and elderly people (Yan et al., 2013).
H. pylori infection is commonly acquired in childhood (Luzza et al., 1997). The prevalence of infection among children ranges from 2.4 to 13.6% in developed countries and from 22.6 to 80% in developing countries. This difference may be attributed to poor socioeconomic status and overcrowded conditions during childhood (Ravelomanana et al., 2013). In Egypt, infection is alarmingly high (Mohammad et al., 2008). A prevalence rate of 33% has been reported among children less than 6 years and 72.38% among school children (Frenck et al., 2006).
The diagnosis of H. pylori can be done using invasive and non-invasive methods. Invasive methods need endoscopy and biopsy [histological examination, rapid urease test (RUT), culture, polymerase chain reaction (PCR), and fluorescent in situ hybridization (FISH)]. Non-invasive methods include 13C, 14C urea breath test (UBT), detection of H. pylori antigen (Ag) in stool, and detection of antibodies (Abs) against H. pylori in serum, urine, and saliva (Koletzko et al., 2011; Leal et al., 2011).
Non-invasive tests for H. pylori infection have been helpful in epidemiological studies of prevalence, mode of transmission and spontaneous clearance of the infection. Considering the broad spectrum of available H. pylori diagnostic methods and since a reliable diagnosis is mandatory both before and after eradication therapy; thus it is crucial to study the different methods to be able to select the highly accurate laboratory tests that could be used to efficiently diagnose H. pylori infection in clinical practice (Leal et al., 2008). In this study we aimed to evaluate some non-invasive techniques (Detection of H. pylori stool Ags using rapid chromatographic Immunoassay and H. pylori IgG Abs in serum and saliva by ELISA technique) for the diagnosis of H. pylori infection in children and their mothers.
MATERIALS AND METHODS
This descriptive-cross sectional study was conducted at El-Shatby University Hospital and the Microbiology Department of the High Institute of Public Health (HIPH), in Alexandria, Egypt during a five- month period from May to December 2014.
Forty children and their twenty one mothers who had gastrointestinal symptoms suggestive of H. pylori infection (Heart burn, epigastric pain, nausea, vomiting, anorexia, vague abdominal pain, diarrhea, indigestion, bloating, weight loss, bleeding) were included in the present study. Any child or mother who had received antimicrobial agents (including metronidazole) and /or proton pump inhibitors (PPI) within 2 weeks prior to samples collection was excluded from the study.
Sample size
Using a power of 80% to detect the sensitivity of salivary IgG at predicting the H. pylori in children = 87% and specificity = 73% (Roxo-Rosa et al., 2013), assuming the prevalence of H. pylori in children =50% with precision = 5 and at alpha = 0.05 (Mohammad et al., 2008); a minimum sample size required was calculated using STATA to be 30 children and their mothers for whom all methods were applied.
Data collection method
A questionnaire sheet was completed for every individual enrolled in the study with all the relevant information including gastrointestinal symptoms and risk factors related to H. pylori infection. This study was approved by the HIPH Ethics Committee, and written informed consents were obtained from all the mothers of examined children.
Samples collection and processing
Stool, blood and saliva* samples were collected from each of the 40 children and their 21 mothers enrolled in the present study. *Saliva samples were collected from 37 children as it was not feasible to collect saliva from three babies.
At the laboratory
Stool samples were tested for H. pylori Ag using rapid chromatographic Immunoassay (Abon one step test code no: 1155976703) (ABON Biopharm Co 2012).
Small portions of stool samples collected from three different parts (to collect approximately 50 mg) were transferred to the sample collection tube containing extraction buffer. It was then vigorously agitated and after two minutes of resting the tube, two full drops were dropped into the round window of the test cassette. Reading was made after 10 minutes of incubation at room temperature.
Interpretation of the results
Based on the appearance of colored lines across the central window of the cassette, two lines, C (control) and T (test), indicated positive test. Only one line in C indicated negative result. A pale colored line in T was also considered positive. Invalid test was considered if no line appeared in C line region.
The obtained sera were stored at -20°C until used for detection of serum H. pylori IgG using the Immunospec Helicobacter pylori IgG ELISA kit (Catalog No.E30-145) (Immunospec Co 2006).
Qualitative results
The cut-off control corresponds to calibrator one. If the absorbance of the sample was higher than that of the cut-off, the sample was positive for the presence of specific IgG. The ratio between optical density (OD) value of the sample and that of the cut-off was calculated.
The sample was considered:
- Positive: if the ratio was > 1.1.
- Doubtful: if+/- 10% of the cut-off.
- Negative: if the ratio was < 0.9.
Quantitative results
Units (U): Positive results were expressed in U, the OD values of the 5 calibrators were interplotted and the value of the sample was compared to this curve. Containers with collected saliva samples were stored at -80â°C till ELISA test for salivary H. pylori IgG was performed using the WKEA Ab H. pylori IgG Ab ELISA Kit (WH-354) (Wkea Med Supplies Co 2009).
Preparatory work
Preparation of saliva samples: A 0.5 ml of saliva was placed in a sterile centrifugal tube, and then one ml of phosphate buffer solution (PBS) with pH value of 7.4 was added by an automatic pipette. The tube was then centrifuged for 20 min (2000-3000 rpm) and the supernatant was collected carefully in a clean Eppendorf tube.
Interpretation of results
Critical cut off was calculated:
Critical cut off = The average of negative control well + 0.15.
- If sample OD < calculated critical cut off, it is negative.
- If sample OD ≥ calculated critical cut off, it is positive.
Statistical analysis of the data
Data were fed to the computer and analyzed using
N.B. +LR > 1 denotes good performance of a test.
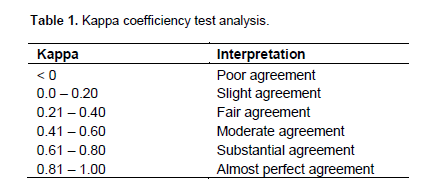
The agreement between different tests was analyzed using Kappa coefficiency test as shown in Table 1:
RESULTS
A total of forty children and their 21 mothers who attended the outpatient clinic at El-Shatby University Hospital and had symptoms suggestive of H. pylori infection were included in this study. The 40 studied children included 22 (52.5%) males and 18 (47.5%) females. Their ages ranged from 7 months to 15 years, with a mean age of 6.3. The mean age of enrolled mothers was 32.6 and their ages ranged from 23 to 52 years.
Eleven (52.38%) of the 21 examined mothers and their children (20 children [50%]) were classified as of high socioeconomic class, 9 (42.85%) and their children (19 children [47.5%]) were of average socioeconomic class and only one (4.76%) and her child (one child [2.5%]) belonged to low socioeconomic class according to modified score for social leveling of families (Fahmy and El Sherbini, 1983).
Of the 21 mothers, 8 (38%) and their children (13 [32.5%]) were from urban areas, while 13 (61.9%) and their children (27 [67.5%]) were from rural areas. In addition, seven of these 21 mothers (33.33%) and 14/40 children (35%) had previous H. pylori infection.
Of the 40 children, 30 (75.0%) were positive for stool Ags, 10 (25.0%) were positive for serum Abs, while two (5.4%) out of 37 children were saliva Ab positive, as it was not feasible to collect saliva from 3 babies. These results were found to be statistically significant. (p1<0.001, p2<0.001, p3= 0.026) (Table 2)
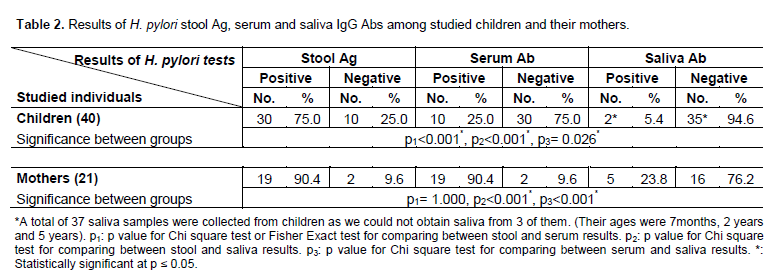
As regards the 21 studied mothers, 19 (90.4%) were positive for each of stool Ags and serum Abs and only 5 (23.8%) were positive for saliva Abs. These results were statistically significant (p2<0.001, p3<0.001) (Table 2).
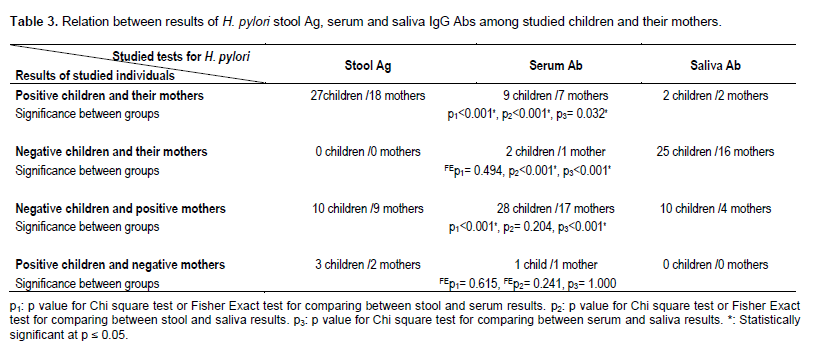
Twenty seven (27) children together with their mothers (18) were concordantly positive for H. pylori stool Ags, while 9 and their mothers (7) were positive for serum Abs and 2 children and their mothers were positive for saliva Abs. These results were statistically significant (p1<0.001*, p2<0.001*, p3= 0.032*) (Table 3).
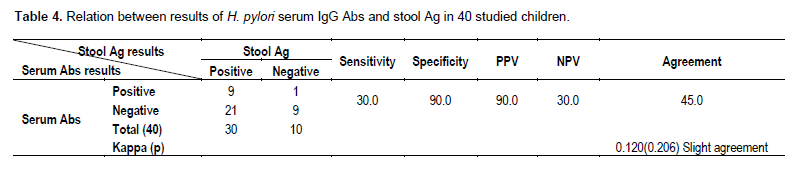
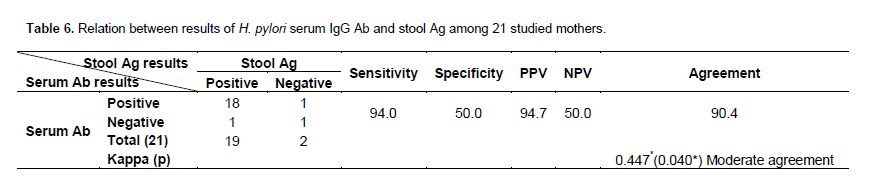
As regards children, the sensitivity of the serum Ab test in relation to stool Ag test was 30 % with a specificity of 90%; positive predictive value (PPV) equals 90% and negative predictive value (NPV) 30%. The agreement between the two tests in the diagnosis of H. pylori infection was 45% (slight agreement) (Table 4). While for mothers, the sensitivity of the H. pylori serum Ab test in relation to stool Ag test was 94% with a specificity of 50%. PPV was 94.74% and NPV was 50%. The agreement between the two tests in the diagnosis of H. pylori infection was 90.48% (moderate agreement) (Table 6).
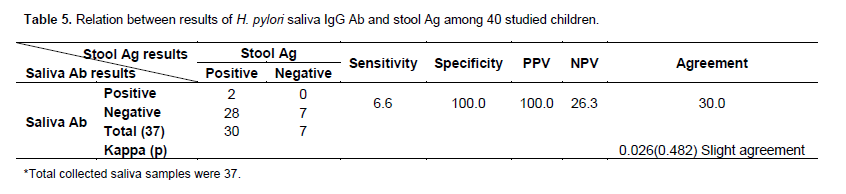
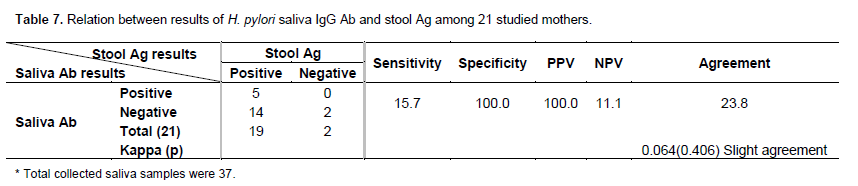
Regarding saliva test, the sensitivity of the saliva Ab test in children in relation to stool Ag test was 6.67 %, with specificity and PPV of 100% each, and NPV of 26.32%. The agreement between the two tests in the diagnosis of H. pylori infection was 30% (slight agreement) (Table 5). While for mothers, the sensitivity of the saliva Ab test in relation to stool Ag test was 15.79%, with specificity and PPV of 100% each, while NPV was 11.11%. The agreement between the two tests in the diagnosis of H. pylori infection was 23.81% (slight agreement) (Table 7).
Of the 30 children with positive stool Ags, 10 (34%) were living in urban areas and 20 (66%) were from rural areas. Of the 10 children with positive serum Abs, 6(60%) were from urban areas and 4 (40%) were from rural areas. Regarding the 2 children with positive saliva Abs, one (50%) was from an urban area and the other (50%) was from a rural area. As regards mothers, of the 19 mothers with positive stool Ags and serum Abs, 7 (37%) were from urban areas and 12 (63%) were from rural areas. Of the 5 mothers with positive saliva Abs, 3 (60%) were from urban areas and 2 (40%) were living in rural areas. There was no statistical significant difference between these results.
As regards family size, 27/30 children (90%) with positive stool Ags, had families of 4-6 members and 3(10 %) belonged to families with more than 6 members. For the mothers, 18 /19 (95%) who were positive for each of stool Ags and serum Abs had a 4-6 family size.
Regarding Unhealthy eating habits, of the 30 children who were positive for stool Ags, 25 (83%) shared spoons, glasses and plates with their family members and 8 (62%) of them, their mothers chewed food before giving it to them. While concerning the 19 mothers who were positive for each of stool Ags and serum Abs, 15 (78%) shared spoons, glasses and plates with their family members and 7 (36%) chewed food before giving it to their children.
As regards serum Abs, of 13 mothers who had symptoms suggestive of H. pylori infection, 12 (92.3%) mothers were positive for serum Abs and had 6 (25%) of their children positive for serum Abs. These results were found to be statistically significant (p<0.001*).
DISCUSSION
H. pylori, one of the most common bacterial pathogens of humans, is the main cause of chronic gastritis all around the world. It colonizes the gastric mucosa and appears to persist throughout the host's life unless the patient is treated. It is the only bacterium to be classified as a carcinogen by the world health organization (WHO) because of its role in gastric cancer development. Gastric cancer is the third leading cause of cancer deaths worldwide, and 89% of gastric cancer cases are attributable to H. pylori infection. Thus an accurate and reliable method for diagnosis is crucial (Ahmed and Shammari, 2015; Plummer et al., 2015; Moon et al., 2013). The invasive techniques for diagnosis of H. pylori are difficult, very expensive and not accepted by the patients (Ni et al., 2000). So in clinical settings, a rapid and cost-effective detection method for diagnosis of H. pylori infection is desirable especially in children. Non-invasive testing for H. pylori has been strongly recommended as it is less expensive, more patient friendly than invasive methods and does not need a very complicated laboratory facility (Osman et al., 2014).
Stool Ag test is one of the non-invasive methods that is widely used in the diagnosis of H. pylori infection and had been known with its accuracy and comparability to invasive methods (Ni et al., 2000). In the present study H. pylori stool Ag test was considered the gold standard method for diagnosis of H. pylori infection. This is due to its high sensitivity and specificity in children and adult patients and excellent positive and negative predictive values regardless of H. pylori prevalence as reported by Bakri (2012). In addition, Pourakbari et al. (2013) has recorded that the performance of stool Ag test in adult patients was excellent, with a sensitivity, specificity, and accuracy of 91, 79 and 85%, respectively. Furthermore in 2014, a review done by Garza-González et al. documented that H. pylori stool Ag test seemed to perform well in children with sensitivity of 97%, specificity of 97%, PPV of 88%, and NPV of 99% (Garza-González et al., 2014).
Also in comparison with UBT, stool Ag proved to be equivalent in its sensitivity specificity as reported by Frenck et al. at Cairo University, who concluded that UBT and stool Ag test had the highest sensitivity (98, 94%, respectively) and specificity (89%, 81%, respectively) and that the use of the stool Ag test has been evaluated as equivalent to the UBT (Frenck et al., 2006).
In the present study, stool Ag test was positive in 30/40 examined children (75%) (Table 2). A higher percentage was recorded by Douraghi et al. (2013), where 93.1% of the children were positive for H. pylori stool Ags (Douraghi et al., 2013). Jafar et al. (2013) found that stool samples were positive for H. pylori Ags in 294 (64.2%) children (Jafar et al., 2013). A lower percentage was reported by Issa et al. (2014) where stool Ags were positive in only 45.7% of tested children. Even a much lower percentage (30%) was recorded in an early study that was conducted by Kato et al. (2003).
As regards the studied mothers in this work, 19 (90%) were positive for stool Ags (Table 2). This was in line with Karim et al. (2012) who found that H. pylori stool Ag was positive in 92% of the patients. Lower percentages were reported by Naji et al. (2014) and Segamwenge et al. (2014) where stool Ags were positive in 49 and 33.5%, respectively (Naji et al., 2014; Segamwenge et al., 2014). Korkmaz et al. (2015) reported a much lower percentage where H. pylori stool Ag test was positive in only 19.7% of patients. In this study, immuno-chromatographic assay was used for stool Ag detection as it has the advantage over other immune assay methods that the test results are available within minutes and it does not require the use of expensive laboratory equipment. In a study done in 2013 by Jekarl et al., H. pylori stool Ag had high sensitivity and specificity (84.5 and 96.2%, respectively) (Jekarl et al., 2013). In the current work, all collected stool samples were well formed. This fact could be the reason for the enhanced stool Ag test results, as the accuracy of the stool Ag test is lowered when stool samples are unform or watery, because H. pylori specific Ags in these stool samples are diluted. Therefore, watery stools should not be used, particularly in the determination of the results of eradication therapy. The sensitivity of this test is also lowered in patients with upper gastrointestinal bleeding (Shimoyama, 2013). All our studied individuals didn’t have gastrointestinal bleeding.
In addition to stool Ag test, serological testings are also useful non-invasive methods for the diagnosis of H. pylori infection. It is easy for patients to accept the test because of its non-invasiveness; the results can be quickly obtained, less likely to be affected by colloidal bismuth, PPIs, or antibiotics (Shah et al., 2014).
In the current study, serum and the saliva IgG Ab tests were done and they were compared to the stool Ag test that was considered as the gold standard method for diagnosing H. pylori infection. It was found that serum IgG Ab was positive in 19 of the 21 enrolled mothers (90%) with sensitivity, specificity and agreement of 94, 50 and 90%, respectively) (Table 6). These results were in concordance with the findings of Pandya et al. (2014) who reported that the IgG Abs evaluated in their study, had a sensitivity of 100% in adults, which permits the safe use of the test in epidemiologic surveys. Also, they recorded a very low specificity, indicating that the ELISA test must be validated for different populations (Pandya et al., 2014). In addition, Shah et al. (2014) reported that serum IgG sensitivity ranged between 90 and 97%, but the specificity ranged between 50 and 96%. In contrast to the results of the current study, Iqbal et al. (2013) reported a higher specificity rate of 80%. As regards children in the present study, 10 out of 40 children (25%) were positive for IgG Abs in serum with sensitivity, specificity and agreement of the test were 30, 90 and 45%, respectively (Table 4). Sensitivity was found to be lower than that of the mothers and this could be attributed to the immature immune response or tolerance to H. pylori that exists in childhood and thus serodiagnosis of H. pylori infection is less useful in children. Similar findings were reported by Okuda et al. (2002) who compared H. pylori IgG and IgA Abs with H. pylori stool Ags (Okuda et al., 2002). Our results were in concordance with that of Pourakbari et al. (2013) who found that ELISA-IgG serum tests in children showed high specificity, but low sensitivity. These findings have significant clinical implications, since a negative test would not be reliable for ensuring the absence of H. pylori infection. Low sensitivity may be attributed to the weak or immature immune response observed in young children (Pourakbari et al., 2013). IgG was also much more specific in children than adults, corroborating the fact that adults are more likely to have been frequently exposed to H. pylori in the past so if it is present in a child, it is so specific to the infection (She et al., 2009). This may explain the difference in specificity.
In this study, it was found that 18 out of the 19 positive mothers for stool Ags (94%) were positive for both stool Ags and serum Abs (Table 6) while in children only 9/30 positive children for stool Ags (30%), were positive for both stool Ags and serum Abs and 21 children were positive for stool Ags but negative for serum Abs. This may be explained by the fact that negative results do not preclude the absence of Abs to H. pylori. Colonization may be present, however it may be in its very early stages or the Ab titer may be too low for the assay to detect. Similar findings were reported by Couturier (2013).
Saliva samples have advantages over serum samples, since their collection is easy, non-invasive, less hazardous and there is a greatly reduced risk of blood-borne infections (Krishnaswamy et al., 2012). In this study we have collected saliva samples from 37 children, as we couldn’t collect saliva from 3 children (their ages were 7 months, 2 years and 5 years) due to their physical resistance and continuous crying.
In the present study, the results of the salivary Abs were inferior to that of stool Ags and serum Abs. Only 5 mothers out of 21(23%) were positive for salivary Abs (Table 7) and only 2 out of 37 children (5%) were positive for salivary Abs. (Table 2) This may be due to the fact that IgG which appears in saliva by trans-capillary leakage is present in low concentration as compared to that present in serum. Factors such as low concentration and variable trans-capillary leakage may be the reasons why salivary IgG assay is less reliable than the serum IgG assay as recorded by Kabir (2003), who in his research concluded that salivary IgG assay has provided inconsistent results with less than optimum sensitivity and specificity.
The calculated sensitivity, specificity and agreement for mothers' salivary Ab tests in the current study were 15.79, 100 and 23.81%, respectively (Table 7) and the corresponding figures for children were 6.67, 100 and 30%, respectively (Table 5). A higher sensitivity and lower specificity percentages were recorded by El-Fakhfakh et al. (2014) who evaluated the frequency of anti-H. pylori serum and salivary Abs positivity among Egyptian patients with gastric disorders and the validity of salivary and serum serological tests for diagnosis of H. pylori, comparing them with tests performed on endoscopy biopsy; where salivary IgG succeeded to diagnose 19 cases from the 31 positive H. pylori patients with a sensitivity of 63.33% and specificity of 92.86% (El-Fakhfakh et al., 2014).
The prevalence of H. pylori infection seems to depend mostly not only on the rate of acquisition, but also on the rate of loss of infection and the length of the persistence period between acquisition and loss. Based on these factors, H. pylori prevalence differs from one country to another and may differ between different ethnic, social, or age groups within the same country. Among Egyptian children, H. pylori prevalence was highest in children attending school in socially-deprived areas. Inhabitants of Cairo residing in an overcrowded home had the highest prevalence among the locations studied (Muhammad et al., 2012).
In our study, H. pylori infection was recorded in 37% of mothers who lived in urban areas and 63% of those who lived in rural areas. It represented 34% in children who lived in urban areas and 66% among those who were from rural areas. This was comparable to what was documented by Laszewicz et al. (2014) where they demonstrated statistically significant higher prevalence of H. pylori infection both in adults and children in rural areas. This could be attributed to inadequate sanitary conditions. Absence or poor personal hygiene may also play a role in increasing H. pylori infection. This may be observed in developing countries, which may reflect the combined effects of poor living conditions, poor hygiene and overcrowded cities (Laszewicz et al., 2014). This work showed higher levels of positivity in children (83%) and mothers (78%) who shared spoons, plates and glasses. This was in accordance with the study of Kaya et al. (2014) who reported that some practices that are characterized by lack of hygiene such as sucking the teat before giving it to the baby and sharing spoons, forks and cups were associated with higher prevalence of infection.
Infection by H. pylori remains the most frequent and persistent bacterial infection worldwide; therefore, accurate diagnosis of infection is imperative. Determining the diagnostic method and therapies to use for each patient depends on several factors, such as the patient's clinical condition and the prevalence of infection (Garza-González et al., 2014). The ideal test for diagnosis of H. pylori infection should be noninvasive, highly accurate, widely available and inexpensive. Furthermore, it should be able to discriminate the colonization from H. pylori associated disease. That is why non-invasive tests are useful for primary diagnosis, when a treatment indication already exists, or to monitor treatment success or failure (Jafar et al., 2013).
Limitations of the study
One of the limitations of the present study was that we could not compare our 3 tested non invasive techniques to one of the invasive techniques that need endoscopy/biopsy, as this wasn't feasible during the study period. Another limitation was the relatively small sample size, though we have abided by the statistically calculated sample size based on the prevalence rate of H. pylori in children. Increasing the number of patients would have yielded more profound data.
CONCLUSIONS
1) H. pylori stool Ag test was the most reliable, rapid, simple and easy to perform non invasive test in all studied individuals.
2) Testing H. pylori IgG Ab in serum was more useful in adults than in children in the diagnosis of H. pylori infection.
3) Although saliva IgG Ab test was easy especially among adults, yet it wasn't reliable as its results were inferior to those of stool Ag and serum IgG for the detection of H. pylori infection in both children and adults.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interest.
ACKNOWLEDGEMENT
The author would like to express special appreciation to Dr. Ahmed Fouad Mahmoud Khalil, Lecturer of Paediatrics, Faculty of Medicine, Alexandria University for his great efforts in the selection of cases and for his continuous support and cooperation.
REFERENCES
|
ABON Biopharm Co. (2012). ACON H. Infectious disease antigen detection. China: ABON BIOPHARM (HANGZHOU) CO., LTD. |
|
|
Ahmed SA, Al Shammari HN (2015). Helicobacter pylori infection: seroprevalence and detection of H. pylori IgG by using ELISA. Inter. J. Immunol. 3:21-26. |
|
|
Bakri MM (2012). Evaluation of non-invasive diagnostic tests for Helicobacter pylori infection in symptomatic patients and healthy volunteers. Pak. J. Physiol. 8(2):10-12. |
|
|
Cheng H, Hu F, Zhang L, Yang G, Ma J, Hu J, Wang W, Gao W, Dong X (2009). Prevalence of Helicobacter pylori infection and identification of risk factors in rural and urban Beijing, China. Helicobacter 14(2):128-133. |
|
|
Couturier MR (2013). The evolving challenges of Helicobacter pylori disease, diagnostics, and treatment, part1.Clin.Microbiol.Newsletter.35(3):19-23. |
|
|
Douraghi M, Rostami MN, Goudarzi H, Ghalavand Z (2013). Comparison of stool antigen immunoassay and serology for screening for Helicobacter pylori infection in intellectually disabled children. Microbiol. Immunol. 57(11):772-777. |
|
|
El-Fakhfakh EA, Montasser IF, Khalifa RA (2014). Evaluation of salivary and serum anti-Helicobacter pylori in Egyptian patients with H. pylori related gastric disorders. J. Egypt Soc. Parasitol. 44(1):275-283. |
|
|
Estakhri R, Dolatkhah H, Ghazanchaei A, Pourasgari B, Nourazarian M (2008). Saliva or serum, which is better for the diagnosis of gastric Helicobacter pylori infection? Iran. J. Clin. Infect. Dis. 3(3):121-125. |
|
|
Fahmy SI, El Sherbini FA (1983). Determining simple parameters for social classifications for health research.Bull. High. Inst. Public. Health 13(5):95-107. |
|
|
Frenck RW, Fathy HM, Sherif M, Mohran Z, El Mohammedy H, Francis W, Rockabrand D, Mounir BI, Rozmajzl P, Frierson HF (2006). Sensitivity and specificity of various tests for the diagnosis of Helicobacter pylori in Egyptian children. Pediatr.118:1195-1202. |
|
|
Garza-González E, Perez-Perez GI, Maldonado-Garza HJ, Bosques-Padilla FJ (2014). A review of Helicobacter pylori diagnosis, treatment, and methods to detect eradication. World. J. Gastroenterol. 20(6):1438-1449. |
|
|
Hanafi M, Mohamed A (2013). Helicobacter pylori infection: seroprevalence and predictors among healthy individuals in Al Madinah, Saudi Arabia. J. Egypt. Public. Health Assoc. 88(1):40-45. |
|
|
Immunospec Co. (2006). ELISA/EIA assays: H. pylori IgG. California: Immunospec; p.121. |
|
|
Iqbal S, Fatima S, Raheem A, Khan AH (2013). Agreement between serology and histology for detection of Helicobacter pylori infection. J. Coll. Phys. Surg. Pak. 23(10):784-786. |
|
|
Issa AH, Sharif IS, Mosawi AA (2014). Detection of Helicobacter pylori in stool of primary school pupils in some areas in Basra. J. Basrah. Res. 40:110-114. |
|
|
Jafar S, Jalil A, Soheila N, Sirous, S (2013). Prevalence of Helicobacter pylori infection in children, a population-based cross-sectional study in west iran. Iran. J. Pediatr. 23(1):13-18. |
|
|
Jekarl DW, An YJ, Lee S, Lee J, Kim Y, Park YJ (2013). Evaluation of a newly developed rapid stool antigen test using an immunochromatographic assay to detect Helicobacter pylori. Jpn. J. Infect. Dis. 66:60-64. |
|
|
Kabir S (2003). Review article: clinic-based testing for Helicobacter pylori infection by enzyme immunoassay of faeces, urine and saliva. Alim. Pharmacol. Therap.17(11):1345-1354. |
|
|
Karim R, Ahmed SM, Begum F (2012). Non-invasive stool antigen test for screening of Helicobacter pylori infection and assessing efficacy of treatment in patients with peptic ulcer. South East. Asia. J. Public. Health. 2:28-33. |
|
|
Kato S, Ozawa K, Okuda M, Fujisawa T, Kagimoto S, Konno M., Maisawa S, Iinuma K (2003). Accuracy of the stool antigen test for the diagnosis of childhood Helicobacter pylori infection: a multicenter Japanese study. Am. J. Gastroenterol. 98(2):296-300. |
|
|
Kaya AD, Gülen D, Aydin M, SaraçoÄŸlu GV, Uzun A (2014). Detection of H. pylori antigen in the stool samples of children, in Tekirdag, Turkey. Sci. Res. 6:865-869. |
|
|
Kirkpatrick LA, Feeney BC (2013). A simple guide to IBM SPSS statistics for version 20.0. Student ed. Belmont, Calif.: Wadsworth, Cengage Learning. |
|
|
Koletzko S, Jones NL, Goodman KJ, Gold B, Rowland M, Cadranel S, Chong S, Colletti RB, Casswall T, Elitsur Y, Guarner J, Kalach N, Madrazo A, Megraud F, Oderda G (2011).Evidence- based guidelines from ESPGHAN and NASPGHAN for Helicobacter pylori infection in children. J. Pediatr. Gastroenterol. Nutri. 53(2):230-243. |
|
|
Korkmaz H, Findik D, Ugurluoglu C, Terzi Y (2015). Reliability of stool antigen tests: Investigation of the diagnostic value of a new immunochromatographic Helicobacter pylori approach in dyspeptic patients. Asian. Pac. J. Cancer Prev. 16(2):657-660. |
|
|
Krishnaswamy RM, David CM, Govindaiah S, Krishnaprasad RB, Jogigowda, SC (2014). Salivary IgG assay to detect Helicobacter pylori infection in an Indian adult population.Indian. J. Dent. Res. 23:694-695. |
|
|
Laszewicz W, Iwa'nczak F, Iwa'nczak B (2014). Seroprevalence of Helicobacter pylori infection in Polish children and adults depending on socioeconomic status and living conditions. Adv. Med. Sci. 59(1):147-150. |
|
|
Leal YA, Flores LL, Garcia-Cortés LB, Cedillo-Rivera R, Torres J (2008). Antibody-based detection tests for the diagnosis of Helicobacter pylori infection in children: a meta-analysis. PLoS. One. 3(11):3751. |
|
|
Leal YA, Cedillo-Rivere R, Simon JA, Velazquez JR, Flores LL, Torres J (2011). Utility of stool sample-based tests for diagnosis of Helicobacter pylori infection in children. J. Pediatr. Gastroenterol. Nutr. 52(6):718-728. |
|
|
Luzza F, Oderda G, Maletta M, Imeneo M, Mesuraca L, Chioboli E, Lerro P, Guandalini S, Pallone F (1997). Salivary immunoglobulin G assay to diagnose Helicobacter pylori infection in children. J. Clin. Microbiol. 35(12):3358-3360. |
|
|
Mohammad M, Hussein L, Coward A, Jackson S (2008). Prevalence of Helicobacter pylori infection among Egyptian children: impact of social background and effect on growth. Public Health Nutr. 11(03):230-236. |
|
|
Moon DI, Shin EH, Oh HG, Oh JS, Hong S, Chung Y, KimO (2013). Usefulness of a Helicobacter pylori stool antigen test for diagnosing H. pylori infected C57BL/6 mice. Lab. Anim. Res. 29(1):27–32. |
|
|
Muhammad JS, Zaidi SF, Sugiyama T (2012). Epidemiological ins and outs of Helicobacter pylori: a review. J. Pak. Med. Assoc. 62(9):955-959. |
|
|
Naji AS, Ameri GA, Alkadasi MN, Hanash S, Ali WA, Zaid AA (2014). Comparison of stool antigen and blood antibody test methods for detection of Helicobacter pylori infection and the risk factors. Int. J. Curr. Microbiol. 3(12):118-127. |
|
|
Ni YH, Lin JT, Huang SF, Yang JC, Chang MH (2000). Accurate diagnosis of Helicobacter pylori infection by stool antigen test and 6 other currently available tests in children. J. Pediatr.136(6):823-827. |
|
|
Okuda M, Miyashiro E, Koike M, Tanaka T, Bouoka M, Okuda S, Yoshikawa N (2002). Serodiagnosis of Helicobacter pylori infection is not accurate for children aged below 10. Pediatr. Int. 44:387-390. |
|
|
Osman HA, Hasan H, Suppian R, Bahar N, Hussin NS, Rahim AA, Hassan S, Andee DZ, Zilfalil BA (2014). Evaluation of the Atlas Helicobacter pylori stool antigen test for diagnosis of infection in adult patients. Asian. Pac. J. Cancer Prev. 15(13):5245-5247. |
|
|
Pandya HB, Patel JS, Agravat HH, Singh NK (2014). Non-Invasive Diagnosis of Helicobacter pylori: Evaluation of two enzyme immunoassays, testing serum IgG and IgA response in the anand district of central Gujarat, India. J. Clin. Diagn. Res. 8(6):12-15. |
|
|
Plummer M, Franceschi S, Vignat J, Forman D, de Martel C (2015). Global burden of gastric cancer attributable to Helicobacter pylori. Int. J. Cancer 136:487-490. |
|
|
Pourakbari B, Ghazi M, Mahmoudi S, Mamishi S, Azhdarkosh H, Najafi M, Kazemi B, Salavati A, Mirsalehian A (2013). Diagnosis of Helicobacter pylori infection by invasive and noninvasive tests. Braz. J. Microbiol. 44(3):795-798. |
|
|
Ravelomanana L, Imbert P, Kalach N, Ramarovavy G, Richard V, Carod J, Ravelomanana N, Al Nakib M, Langue J, Avenell C, Raymond J (2013). Helicobacter pylori infection in children in Madagascar: risk factors for acquisition. Trop. Gastroenterol. 34(4):244-251. |
|
|
Roxo-Rosa M, Oleastro M, Vale F (2013). Helicobacter pylori eradication-the alternatives beyond antibiotics. Formatex. 3,1656-1657. |
|
|
Segamwenge IL, Kagimu M, Ocama P, Opio K (2014). The utility of the Helicobacter pylori stool antigen test in managing dyspepsia: an experience from a low resource setting. Afr. Health Sci. 14(4):829-834. |
|
|
Shah SA, Khan AA, Hussain N, Aslam H, Abbas N, Ul A, Khalid A(2014). Diagnostic Accuracy of Serology Testing for Helicobacter Pylori in Perforated Peptic Ulcer. J. Rawalpindi. Med. Col. 18(2):250-253. |
|
|
She RC, Wilson AR, Litwin CM (2009). Evaluation of Helicobacter pylori Immunoglobulin G (IgG), IgA, and IgM serologic testing compared to stool antigen testing. Clin. Vaccine Immunol. 16(8):1253-1255. |
|
|
Shimoyama T (2013). Stool antigen tests for the management of Helicobacter pylori infection. World J. Gastroenterol. 19(45):8188-8191. |
|
|
Wkea Med Supplies Co. (2009). Elisa kits: H. pylori., China: Wkea Med Supplies Co, p. 6. |
|
|
Yan TL, Hu QD, Zhang Q, Li YM, Liang TB (2013). National rates of Helicobacter pylori recurrence are significantly and inversely correlated with human development index. Aliment. Pharmacol. Ther. 37:963-968. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


