Full Length Research Paper

ABSTRACT
Hypertension and diabetes co-morbidity are very common chronic diseases in today’s world. Patients with such conditions may have medication related problems. Assessment was made on the impact of clinical pharmacists’ led education and counselling in patients with co-morbid hypertension and diabetes in a hospital setting. This study was done at the medical outpatient department (OPD) of a Municipal Hospital in Tema in the Greater Accra Region of Ghana. This was an intervention study conducted in patients with co-morbid hypertension and diabetes (n=338). Patients were randomized to the case group (n=144) and the control group (n=194). Patients in the case group received the education and counselling from the clinical pharmacists’, whilst patients in the control group had the usual care. Patients in the case group had a better knowledge (p<0.0001) and adhered (p<0.0001) to their medication than those in the control group. The case group had a significant reduction in body mass index (p=0.005), systolic blood pressure (p<0.0001), diastolic blood pressure (p<0.0001) and fasting plasma blood glucose (p<0.0001). The clinical pharmacists’ led counselling and education to support the management of co-morbid hypertension and diabetes at the hospital helped improved patient outcomes.
Key words: Co-morbid, diabetes, hypertension, intervention, counselling, education.
INTRODUCTION
The cumulative burden of non-communicable diseases (NCDs) demands for health care personnel to address its management comprehensively. These diseases are known to be a principal cause of mortality and morbidity globally (Gouda et al., 2019; WHO, 2018). Patients with co-morbid hypertension and diabetes face a myriad of challenges to their health. Management of these conditions are multifaceted, and patients need accurate information about their condition and medications among other things, to maximize the full benefit of treatment and prevent complications. These conditions are managed primarily with multiple drug therapy or dual therapy depending on patient characteristics and risk factors such as age, sex, past medical history, and social history among others (Alomar, 2014). Furthermore, these diseases affect different organ systems whereby patients are required to receive prescriptions with two or more medicines (Whitson et al., 2016). Universally, patients being on multiple drug therapy have been found to experience increased risk of medication error, undesirable side effects, adverse reactions, or increased medical expenditure (Alomar, 2014). To bridge this gap, pharmaceutical care, that is the delivery of medication-related care to improve the quality of life of the patient, is very essential (da Costa et al., 2019). Pharmacists have a key role in the prevention, identification, and correction of drug-related problems because of their pharmacotherapeutic training (da Costa et al., 2019). The process involves retrieving patient and medication data, recording the objectives, assessing the therapeutic plan, recognizing drug related adverse events or any drug related problem, responding to the problems, designing a monitoring plan, proposing the intervention to the doctor or patient, executing the intervention and implementing a monitoring plan that will continuously improve the quality of life of the patient (Chemello et al., 2014; Cipolle et al., 2012). It also involves the provision of essential services before, during, and after treatment to ensure effective and safe drug therapy (Chemello et al., 2014). Counselling, which is pivotal to pharmaceutical care, helps clients become more empowered to make informed decisions concerning the appropriate treatment with prescription and non-prescription medicines. This includes suitable actions to be taken in the event of side effects and adverse drug reactions. Furthermore, it helps patients comprehend the importance of their medicines and their storage conditions, which will help maintain and promote their well-being, as well as contribute to patient participation in their own care. This adds to the patient’s health literacy (Hickey et al., 2018).
In Ghana, although there is a higher burden of communicable diseases, there has been an upsurge in the number of patients with NCDs (Agyei-Mensah and Aikins, 2010; Dosoo et al., 2019; Gatimu et al., 2016). Many studies around the world in recent times have reported the importance of pharmaceutical care in the management of patients with hypertension (Robinson et al., 2010; Skowron et al., 2011) and diabetes (Nogueira et al., 2020; Sriram et al., 2011). All these reinforce the fact that the normalization of blood glucose, systolic and diastolic blood pressure significantly prevent complications and improve the quality of life of patients. Therefore, pharmaceutical care provided by clinical pharmacists', can have a positive impact on patient care since they can provide education on medicines, disease condition, and therapeutic life style modifications such as diet, exercise, self-monitoring of blood pressure, and blood glucose. Furthermore, most studies are carried out in patients with single conditions rather than those with co-morbid conditions. Patients with co-morbidities are likely to be on multiple drug therapy and need more education and counselling. Therefore, the aim of this study was to assess the impact of counselling and education led by clinical pharmacists in patients with co-morbid hypertension and type -2-diabetes mellitus.
MATERIALS AND METHODS
Study setting
The study participants were recruited from the medical outpatient clinic, situated at the main outpatient department (OPD) of the Tema Municipal Hospital (TMH). TMH is the biggest government funded public health institution in the Tema Metropolitan Area, which is a Harbour City. The area of operation of the hospital includes the Tema Metropolis, towns and villages around it. The peculiar location of the hospital makes it one of the busiest in the Greater Accra Region of Ghana. TMH which has a bed capacity of about 399 is the chief referral point for other clinics and hospital in the metropolis. It has a medical OPD which operates a clinic for hypertension and diabetic patients.
Study design
This was an intervention study conducted at the medical out-patient clinic of TMH from August, 2018 to June, 2019. Three hundred and thirty-eight patients were recruited voluntarily on clinic days.
Inclusion and exclusion criteria
Co-morbid hypertension and type-2-diabetes patients who were at least 18 years and above. They should have had both conditions for at least six months. They were required to consent to regularly visit the hospital for the period of the study. Patients who were pregnant, had mental challenges or any other forms of diabetes were excluded from the study.
Sampling procedure
Participants were enrolled using a simple random technique. Participants were clients visiting the diabetes clinic. This clinic runs three days in a week (Wednesday, Thursday, and Friday) and attends to eighty-five patients per day on an average. Ten patients were selected for participation each day using a computer-generated sequence of random numbers. A person with no involvement in the study randomly allocated participants into the case and control groups.
The clinical pharmacists and nurses were not aware of the allocation, whereas the pharmacy interns, other pharmacy staff, and the patients were. The sampling frame was the number of patients who were booked for a clinic day. Each patient was given a unique number on each clinic day and patients who had been previously sampled were excluded from subsequent sampling using the dates of their previous clinic attendance. A total of thirty-six clinic days were used for the recruitment of participants at baseline. In all, three hundred and eighty-nine patients were recruited but fifty-one declined to participate in the study. This reduced the number of participants by 13% to 338. They were then grouped into the case (n=144) and control (n=194) groups by computer-generated numbers. At months 3 and 6, there were 187 participants in the control group and 141 in the case group.
Data collection methods
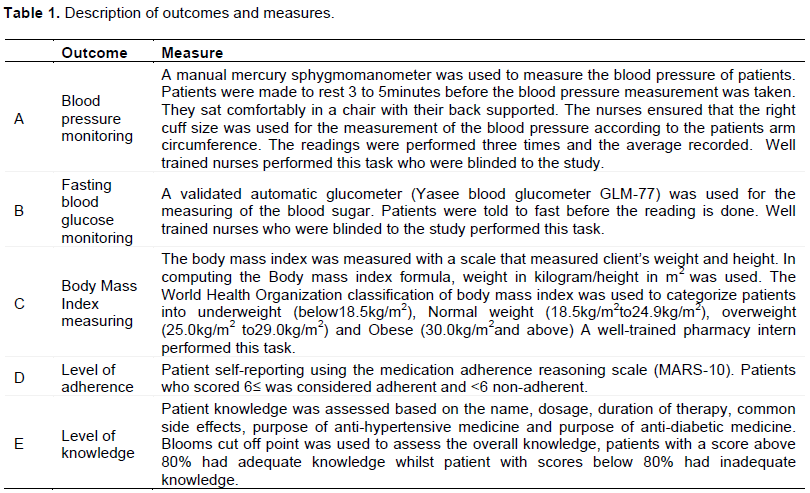
Data collection forms and questionnaires were used for this study. Experts on the subject matter reviewed the developed questionnaire to validate the content for comprehensiveness, clarity and readability. A consent form was thumb printed or signed by all prospective participants. Participants, who were unable to read, write or sign nominated an independent witness to attest to the consent process. A case report form was also generated to document data on their age, weight, height, body mass index, fasting plasma glucose, systolic blood pressure, diastolic blood pressure, adherence, patient knowledge and follow-up visits at months 3 and 6. Bloom’s cut off point was used to categorize the level of knowledge into high, moderate, and low levels. Low and moderate knowledge levels were categorized as inadequate knowledge, while high knowledge levels were categorized as adequate knowledge. For adherence the MARS-10 was used to categorize the level of medication adherence into adherent and non-adherent. The blood pressure was measured by well-trained nurses who were blinded to the study. The body mass index was measured by well-trained pharmacist interns.
Intervention program
The case group was subjected to an intervention program provided by the clinical pharmacists which included a face to face interview which lasted for 10-20 min for the first session. The second session lasted for approximately 10 min which was based on the baseline data. The intervention centered mainly on educating patients on their disease condition, medication, therapeutic lifestyle, and individualized support systems. For educating the patients regarding their conditions, flyers and verbal communication were used by the clinical pharmacists. Aspects of the education included: The meaning of both hypertension and diabetes mellitus, the common signs and symptoms, risk factors, meaning of hypoglycemia and hyperglycemia, the common signs and symptoms of hyperglycemia and hypoglycemia, and common complications.
For educating the patients on their medications, emphasis was made on knowing the name of their medicines, identifying their medicines and what each is being used for, the importance of the medicine on their blood pressure and blood glucose, the common side effects and adverse effects of each medication, the dose to be taken daily, the dosing frequency, the duration of therapy, how to administer their medicines (especially insulin), how to store their medicines, common drug-drug interactions, common drug-food interactions, the importance of adhering to their medicines and refill dates, not sharing their medicines with other people, and keeping the medicines away from children.
In the area of therapeutic lifestyle, the clinical pharmacists used pictorial flyers and verbal communication to emphasize the importance of increasing physical activity (e.g., 30 min daily walks), eating diet rich in vegetables (e.g., green beans, cauliflower, lettuce), fruits (e.g., oranges, apples), fish, lean meat, avoiding adding salt and sugar to meals, avoiding foods such as salted tilapia and sugar-coated biscuits. Participants’ ideas and preferences were discussed before any inputs were made on their diet. In addition, the importance of quitting smoking or the use of nicotine gums, the importance of rest and taking short breaks during working hours, reducing intake of alcohol, inspecting feet daily, cutting nails carefully, keeping feet warm and dry, not walking bare footed, self-monitoring of blood pressure (normal and abnormal ranges) daily, self-monitoring of blood sugar daily, and regular hospital checkups were emphasized.
The individualized supportive care was tailored to the personal needs of each participant. There was variation among the participants in terms of background, social and cultural beliefs, knowledge, among other factors. Participants had the opportunity to ask the clinical pharmacist any question concerning their health outcomes. The control group had no clinical pharmacist involved in counselling and education. They received the usual services provided by the hospital in which patients come for their medication and are counselled for some few minutes due to the heavy patient burden and the lack of health personnel. However, there were continuous telephone follow-up calls for both the case and the control groups.
Monitoring parameters and outcome measures
The parameters listed in Table 1 and related outcome measures were observed at baseline and months 3 and 6 in the case and control groups.
Data analysis
Prior to data entry and analysis, a unique identification number (ID) was assigned to every completed questionnaire. The coded data forms (questionnaires) were entered into the Epi info 7 data base. Data were processed using Microsoft Excel 2016. Categorical data were presented as frequencies (percentages). Bloom’s cut off point and MARS-10 were used to assess the overall knowledge and adherence respectively. Chi-squared test was used to test the significance of associations. Normality of continuous data was assessed with Shapiro Wilk’s test and was found not to be normally distributed. All continuous data were non-parametric and presented as median (interquartile ranges). The Mann-Whitney U test was used to evaluate the significance of the differences in anthropometric, hemodynamic, and biochemical parameters between the case and control groups. Non-parametric repeated-measures analysis of variance was used to determine the significance of the differences between systolic and diastolic blood pressure and fasting blood glucose across times of visit. p-values < 0.05 were considered statistically significant.
Ethics approval
Ethical clearance for research involving human subjects was obtained from the Committee on Human Research Publication and Ethics (CHRPE) Kwame Nkrumah University of Science and Technology (KNUST). The research protocol, questionnaire, participant information leaflet, and patient consent forms were reviewed and approved by the committee. The ethical approval code and date were CHRPE/AP/409/18 and July 18, 2018, respectively. Additionally, authorization was obtained from the hospital management before the commencement of the study.
RESULTS
Socio-demographic and lifestyle characteristics of the case and control groups
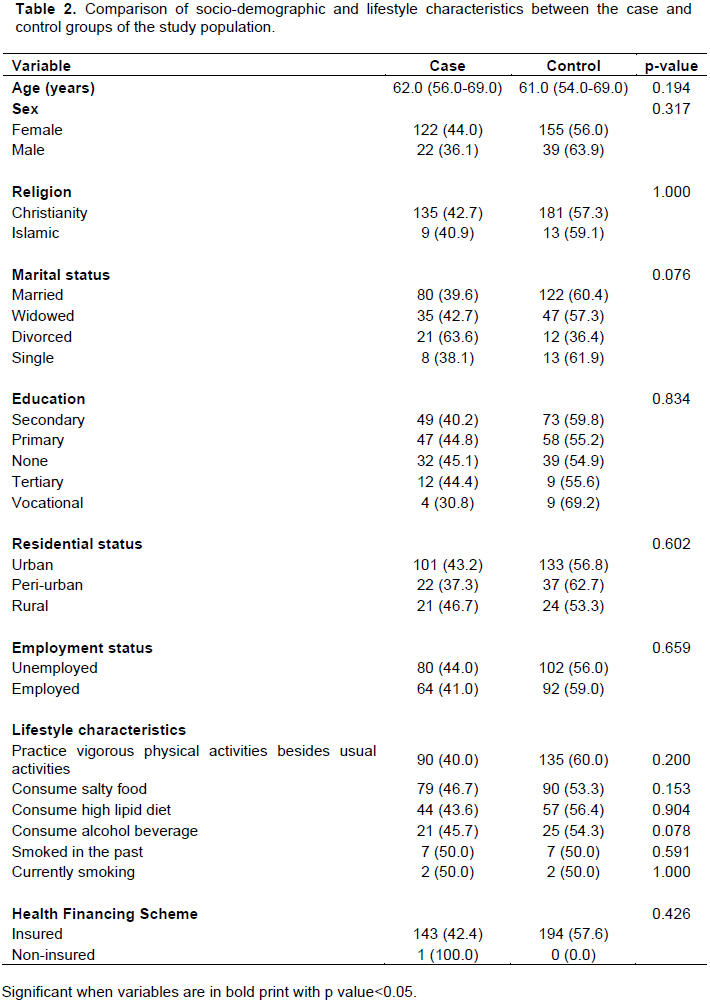
Participants in the case and control group had similar characteristics. There were no statistically significant differences in socio-demographic and lifestyle characteristics (Table 2).
Comparison of the clinical characteristics of the case and control groups
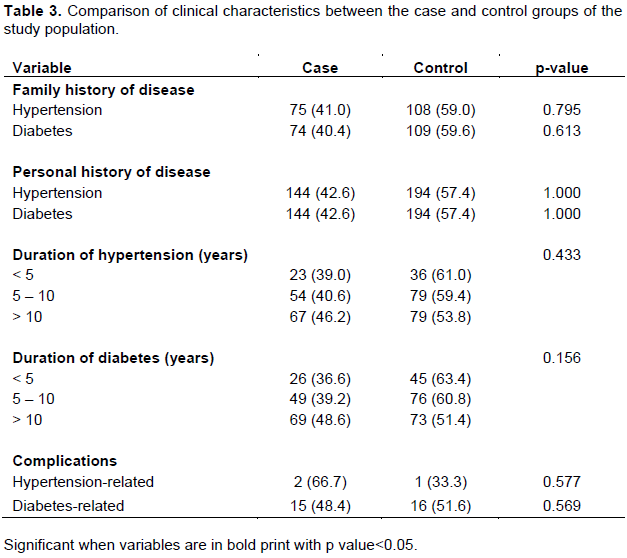
There were no statistically significant differences between the case and control groups with respect to clinical characteristics (Table 3).
Biochemical, anthropometric and hemodynamic profiles of the case and control group stratified by visit type
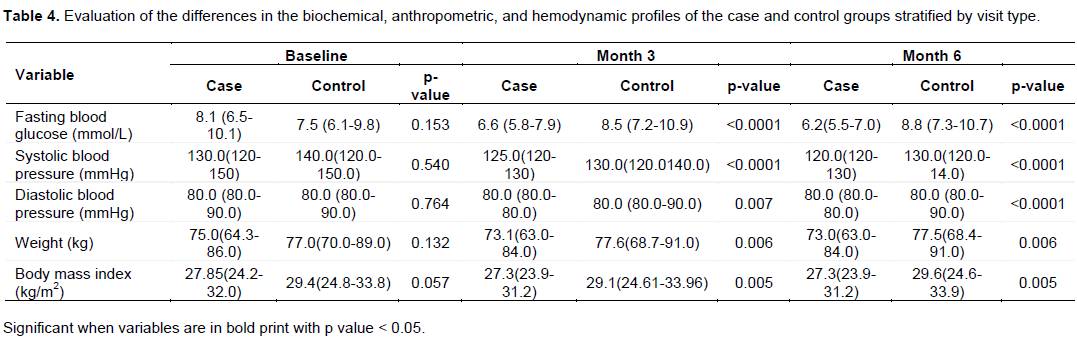
There were no statistically significant differences between the parameters for the case and control groups at baseline. After intervention, the case group had improved outcomes (Table 4).
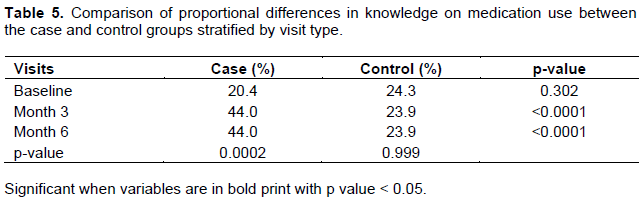
Level of knowledge of the case and control groups stratified by visit type
There was no statistically significant difference in the level of knowledge on medication use between the case and control groups at baseline. However, after intervention, the case group recorded a significantly higher knowledge on medication than the control group at both 3 and 6 month of follow up (Table 5).
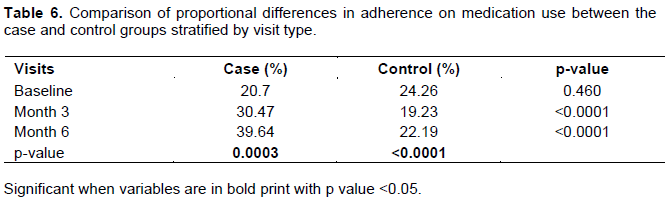
Level of adherence of the case and control groups stratified by visit type
There was no statistically significant difference in the level of adherence on medication use between the case and control groups at baseline. However, after intervention, the case group recorded a significantly higher adherence to medication than the control group at both 3 and 6 month of follow up (Table 6).
DISCUSSION
Pharmaceutical care interventions which focused on patient education and counselling have resulted in the improvement of the quality of life of patients worldwide (da Costa et al., 2019; De La Monte and Wands, 2008; Nogueira et al., 2020; Saleem et al., 2015; Shao et al., 2017; Skowron et al., 2011; Tommelein et al., 2014). The results of the present study support the fact that pharmaceutical interventions have positive effects on patients’ health even in co-morbid conditions. In this study, the baseline median body mass index of the case group decreased from 27.85 to 27.3 kg/m2 as compared to the control group where there was an increase from 29.4 to 29.6 kg/m2 (p = 0.005). In a randomized controlled trial in patients with diabetes mellitus, there was a reduction in the median body mass index of the case group from 34.10 to 32.40 kg/m2 (p < 0.001) (Korcegez et al., 2017). This reiterates the fact that pharmacist involvement in the healthcare of patients can help in the reduction of body mass index and improve health outcomes. Additionally, the median fasting blood glucose of the case group decreased from 8.1 to 6.2 mmol/L compared to the control group where there was an increase from 7.5 to 8.8 mmol/L (p < 0.0001). In a systematical review involving 2,997 patients in 25 studies, pharmaceutical care intervention programs helped in reducing the plasma glucose of patients (Iqbal et al., 2019). Poor glycemic control is associated with many complications which can result in disabilities and even death (Haghighatpanah and Nejad, 2018). Pharmacist involvement in counselling and other supportive care has a positive outcome on the fasting plasma glucose of patients. Additionally, the median systolic blood pressure improved for both the case (from 130 to 120 mmHg) and control group (140 to 130 mmHg) after the 6-month study period with p < 0.0001. However, the case group had a better outcome. In a cluster, randomized, controlled trial in patients with hypertension, the case group had a significant reduction in systolic blood pressure compared to the control group (p < 0.001) (Anderegg et al., 2018). The median diastolic blood pressure of both the case and control group was normal (80 mmHg). However, most patients in the case group had an improved diastolic pressure compared to those in the control group. In an exploratory study in Ghana, in a community setting, pharmaceutical care intervention improved the diastolic blood pressure of patients with hypertension (p = 0.01) (Marfo and Owusu-Daaku, 2017). With respect to patients’ knowledge, there was no statistically significant difference between the case and control groups at baseline. However, after intervention, the case group recorded a significantly higher knowledge on medication compared to the control group at both month 3 (44.0 vs 23.9%, p < 0.0001) and month 6 (44.0 vs 23.9%, p < 0.0001). In a randomized control study in hypertension patients where educational intervention was provided by a pharmacist to the case group, there was an increase in the median knowledge score from 12 to 20 (p<0.001) (Muhammad et al., 2018). Lack of knowledge on medicines can lead to over dose or under dose of medication, which can further lead to treatment failure and put the health of the patient at risk (Saqib et al., 2019). Although in public hospitals, pharmacists are overburdened with the number of patients or prescriptions they attend to, nevertheless there is a need for pharmacists to encourage drug-therapy information awareness, counselling on medicines etc. which will improve on patient outcomes and also prevent any untoward effects. In respect to adherence to medication, there was no statistically significant difference in the proportion of patients who were adherent to their medication between the case and control, however after the intervention, the case group had a higher adherence level compared to the control group at both month 3(30.47 vs 19.23%, p < 0.0001) and month 6(39.64 vs 22.19%, p < 0.0001). Adherence to medication is important when it comes to the management of patients with hypertension and diabetes. Non- adherence to prescribed medicines, sub-optimal utilization of pharmacotherapy and lack of monitoring contribute to the poor control of blood sugar and blood pressure in hypertension and diabetes patients (Bajorek et al., 2016). Improvement in medication adherence has been found to be linked to the patient knowledge and understanding, their beliefs about their treatment and health condition (Kardas et al., 2013). Hence the need for pharmacists and other health care team members to educate and counsel their patients about their medication and health condition.
STRENGTH OF THE STUDY
To our knowledge, studies have been conducted on the impact of education and counselling provided by pharmacists in chronic disease in Sub-Saharan Africa, however there appears to be paucity of research information in patients with co-morbid hypertension and diabetes.
LIMITATIONS OF THE STUDY
This study was conducted in a municipal hospital with a study population of three hundred and thirty- eight patients, which though adequate for this specific study, may not fully represent the general outcome of education and counselling provided by pharmacists in the management of patients with co-morbid hypertension and diabetes.
CONCLUSION
The counselling and education led by clinical pharmacists improved the health outcomes of patients with hypertension and diabetes seeking care at the hospital. Thus, the clinical pharmacy services instituted at the hospital were efficient in supporting therapy and improving patient outcomes.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Agyei-Mensah S, Aikins AD (2010). Epidemiological Transition and the Double Burden of Disease in Accra, Ghana. Journal of Urban Health 87(5):879-897. |
|
|
Alomar MJ (2014). Factors affecting the development of adverse drug reactions. Saudi Pharmaceutical Journal 22(2):83-94. |
|
|
Anderegg MD, Gums TH, Uribe L, MacLaughlin EJ, Hoehns J, Bazaldua OV, Ives TJ, Hahn DL, Coffey CS, Carter BL (2018). Pharmacist intervention for blood pressure control in patients with diabetes and/or chronic kidney disease. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy 38(3):309-18. |
|
|
Bajorek B, Lemay KS, Magin P, Roberts C, Krass I, Armour CL (2016). Implementation and evaluation of a pharmacist-led hypertension management service in primary care: outcomes and methodological challenges. Pharmacy Practice (Granada) 14(2):0-0. |
|
|
Chemello C, Souza FD, Patricio ED, Farias MR (2014). Pharmaceutical care as a strategy to improve the safety and effectiveness of patients' pharmacotherapy at a pharmacy school: a practical proposal. Brazilian Journal of Pharmaceutical Sciences 50:185-93. |
|
|
Cipolle RJ, Strand LM, Morley PC (2012). Pharmaceutical care practice: the patient-centered approach to medication management. McGraw Hill Professional pp. 1-5. |
|
|
da Costa FA, Van Mil JF, Alvarez-Risco A (2019). The pharmacist guide to implementing pharmaceutical care. Springer International Publishing pp. 4-6. |
|
|
De la Monte SM, Wands JR (2008). Alzheimer's disease is type 3 diabetes-evidence reviewed. Journal of Diabetes Science and Technology 2(6):1101-13. |
|
|
Dosoo DK, Nyame S, Enuameh Y, Ayetey H, Danwonno H, Twumasi M, Tabiri C, Gyaase S, Lip GY, Owusu-Agyei S, Asante KP (2019). Prevalence of hypertension in the middle belt of Ghana: a community-based screening study. International Journal of hypertension. |
|
|
Gatimu SM, Milimo BW, San Sebastian M (2016). Prevalence and determinants of diabetes among older adults in Ghana. BMC Public Health 16(1):1-2. |
|
|
Gouda HN, Charlson F, Sorsdahl K, Ahmadzada S, Ferrari AJ, Erskine H, Leung J, Santamauro D, Lund C, Aminde LN, Mayosi BM (2019). Burden of non-communicable diseases in sub-Saharan Africa, 1990-2017: results from the Global Burden of Disease Study 2017. The Lancet Global Health 7(10):e1375-87. |
|
|
Haghighatpanah M, Nejad ASM (2018). Factors that correlate with poor glycemic control in type 2 diabetes mellitus patients with complications. Osong public health and research perspectives 9(4):167. |
|
|
Hickey KT, Creber RM, Reading M, Sciacca RR, Riga TC, Frulla AP, Casida JM (2018). Low health literacy: Implications for managing cardiac patients in practice. The Nurse Practitioner 43(8):49. |
|
|
Kardas P, Lewek P, Matyjaszczyk M (2013). Determinants of patient adherence: a review of systematic reviews. Frontiers in pharmacology 4:91. |
|
|
Korcegez EI, Sancar M, Demirkan K (2017). Effect of a pharmacist-led program on improving outcomes in patients with type 2 diabetes mellitus from Northern Cyprus: a randomized controlled trial. Journal of Managed Care and Specialty Pharmacy 23(5):573-82. |
|
|
Marfo AF, Owusu-Daaku FT (2017). Exploring the extended role of the community pharmacist in improving blood pressure control among hypertensive patients in a developing setting. Journal of Pharmaceutical Policy and Practice 10(1):1-9. |
|
|
Muhammad A, Rahman NU, Saeed Ur Rashid N, Atif R, Humayun R, Misbah S, Saleha S (2018). Impact of pharmacist's intervention on disease related knowledge, medication adherence, HRQoL and control of blood pressure among hypertensive patients. Pakistan Journal of Pharmaceutical Sciences 31(6): 2607-2616. |
|
|
Nogueira M, Otuyama LJ, Rocha PA, Pinto VB (2020). Pharmaceutical care-based interventions in type 2 diabetes mellitus: a systematic review and meta-analysis of randomized clinical trials. Einstein (São Paulo) 18:eRW4686. |
|
|
Robinson JD, Segal R, Lopez LM, Doty RE (2010). Impact of a pharmaceutical care intervention on blood pressure control in a chain pharmacy practice. Annals of Pharmacotherapy 44(1):88-96. |
|
|
Saleem F, Hassali MA, Shafie AA, Ul Haq N, Farooqui M, Aljadhay H, Ahmad FU (2015). Pharmacist intervention in improving hypertension?related knowledge, treatment medication adherence and health?related quality of life: a non?clinical randomized controlled trial. Health Expectations 18(5):1270-1281. |
|
|
Saqib A, Atif M, Ikram R, Riaz F, Abubakar M, Scahill S (2018). Factors affecting patients' knowledge about dispensed medicines: A Qualitative study of healthcare professionals and patients in Pakistan. PloS One 13(6): e0197482. |
|
|
Shao H, Chen G, Zhu C, Chen Y, Liu Y, He Y, Jin H (2017). Effect of pharmaceutical care on clinical outcomes of outpatients with type 2 diabetes mellitus. Patient Preference and Adherence 11:897-903. |
|
|
Skowron A, Polak S, Brandys J (2011). The impact of pharmaceutical care on patients with hypertension and their pharmacists. Pharmacy practice. 9(2):110. |
|
|
Sriram S, Chack LE, Ramasamy R, Ghasemi A, Ravi TK, Sabzghabaee AM (2011). Impact of pharmaceutical care on quality of life in patients with type 2 diabetes mellitus. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences 16(Suppl1): S412. |
|
|
Tommelein E, Mehuys E, Van Hees T, Adriaens E, Van Bortel L, Christiaens T, Van Tongelen I, Remon JP, Boussery K, Brusselle G (2014). Effectiveness of pharmaceutical care for patients with chronic obstructive pulmonary disease (PHARMACOP): a randomized controlled trial. British Journal of Clinical Pharmacology 77(5):756-66. |
|
|
Whitson HE, Johnson KS, Sloane R, Cigolle CT, Pieper CF, Landerman L, Hastings SN (2016). Identifying patterns of multimorbidity in older Americans: application of latent class analysis. Journal of the American Geriatrics Society 64(8):1668-1673. |
|
|
World Health Organization (WHO) (2018). Noncommunicable diseases Country Profiles 2018. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


