Full Length Research Paper
ABSTRACT
Acute meningitis is a potentially life-threatening neurological emergency which requires rapid diagnosis and early administration of appropriate empirical therapy. The compliance regarding empirical treatment of acute meningitis to the Barts and the London Trust (BLT) guidelines was assessed along with the use of corticosteroids. A retrospective audit for the time period of 1st January, 2008 to 21st May, 2009 was carried out in order to determine the level of compliance to the Trust guidelines in empirical treatment and the use of corticosteroids in acute meningitis. Patients were identified from cerebrospinal fluid specimens sent to the Microbiology Department from five wards in the BLT. This project's primary outcome is the extent to which prescribers follow current Trust guidelines regarding empirical antimicrobial therapy of community acquired meningitis/encephalitis and the extent to which corticosteroids are prescribed as adjuvant treatment. Twenty nine patients with suspected meningitis were identified. Eighty-nine percent of patients were initiated on appropriate antibiotics in accordance with Trust guidelines and 79% of patients on antiviral agents accordingly. When all elements of guideline compliance was assessed (antimicrobial choice, dose, time of administration etc), compliance fell to 38%. Empirical treatment was delayed for more than 6 h from admission in 30% of patients receiving antibiotics and 47% of patients receiving antivirals. Corticosteroids were not used. After identifying fairly low level of compliance, a suitable strategy for the improvement has to be developed. The place of corticosteroid therapy for the treatment of meningitis will be more specific.
Key words: Meningitis, antimicrobial agents, hospital, corticosteroids.
INTRODUCTION
Despite the availability of effective antimicrobial treatment, meningitis remains an important cause of morbidity and mortality globally (Van de Beek et al. 2002; Lepur and Barši? 2007; Van de Beek et al. 2004a). Around 1.2 million cases of acute meningitis occur every year in the world, resulting in 135,000 deaths (Cullen 2005; Van de Beek et al. 2006). Hence, early recognition, assessment of disease severity and administration of appropriate antibiotic therapy are considered to be crucial in achieving a beneficial clinical outcome in patients with meningitis (Fitch and van de Beek 2007). Possible beneficial effects of corticosteroids on morbidity and mortality in meningitis is seen in their ability to attenuate subarachnoid space inflammation caused by inflammatory response, but there is a concern that corticosteroids might decrease cerebrospinal fluid (CSF) penetration of antimicrobials (Heyderman et al. 2003; Van de Beek et al. 2004b; Begg et al. 1999; O'Donnell et al. 2009; Korshin et al. 2007; Peterkovi? et al. 2012).
Empirical antimicrobial therapy of suspected meningitis is needed in the case of delayed lumbar puncture (LP), presence of purulent meningitis or negative CSF Gram stain results and it should be initiated as soon as possible (preferably inside of one hour after admission) (Chadwick and Lever 2002; Gjini et al. 2006). Empirical treatment should depend mainly on the most common meningeal pathogen(s) causing the disease, the patient’s age and underlying conditions, and it should last at least 48 to 72 h or until the diagnosis of meningitis/encephalitis can be ruled out (Sáez-Llorens and O’Ryan 2001; Mitropoulos et al. 2008). Meningitis guidelines for the management of adult patients with suspected bacterial meningitis and meningococcal sepsis have been available on the Bart's and the London intranet since 2001. This guideline represents a complete clinical care pathway for the patient presenting with signs and symptoms of meningitis to Barts and the London Trust (BLT) (Appendix 1) (Begg et al. 1999; Chaudhuri et al. 2008; Solomon et al. 2007; Tunkel et al. 2004).
Aforementioned stated facts along with the Trust guidelines all advocate the importance of early and proper management of patients with suspected or proven meningitis. In that sense it is reasonable to conduct an audit at Barts and The London Trust to assess the quality of patients' care, level of compliance to the Trust guidelines and to identify a strategy for improvement of clinical practice if needed. The aim of this retrospective audit is to review the pharmacological management of patients admitted to the Barts and The London NHS Trust with suspected community acquired meningitis and to assess compliance with the Trust guidelines.
MATERIALS AND METHODS
Hospital numbers and specimen details were obtained from the Microbiology Department, for patients whose CSF specimens were taken by LP and sent for analysis from five wards at the Royal London Hospital (RLH) from 1st January, 2008 until 21st May, 2009. One-hundred and sixty-seven patients’ hospital numbers were obtained and their electronic patient records (EPRs) were reviewed in order to determine if they were admitted with suspected community acquired meningitis/encephalitis on admission to the RLH. After looking into EPRs, 94 patients were selected for further review of their medical notes. The selection decision was based on data presented in discharge notes of patients: patients had suspicion of community acquired meningitis/encephalitis and given empirical intravenous antimicrobials initially without clear diagnosis or patients where there was insufficient data to exclude by EPR alone. Seventy-three patients were excluded from the study initially on account of differential/confirmed diagnosis that did not include meningitis/encephalitis. The inclusion criteria for the patients in this audit were:
1. Admission to five wards at the BLT (Ward 1, Ward 2, Ward 3, Ward 4 and Ward 5) with the suspicion of community acquired meningitis/viral encephalitis between 1st January, 2008 and 21st May, 2009.
2. Lumbar puncture performed and CSF specimen sent to the Microbiology for analysis.
3. > 1 month of age.
The exclusion criteria were:
1. Nosocomial meningitis.
2. Immunosuppressive disease (HIV) or long term treatment with immunosuppressive drugs.
3. Presence of ventricular shunt.
4. Head trauma or surgical procedures in the two weeks prior to presenting with signs and symptoms of meningitis.
5. Tuberculous meningitis.
The collected data were analysed using statistical package for social sciences (SPSS) software Student Version 17.0 for Windows. Categorical variables were analysed and described using descriptive statistics such as numbers and percentages. Continuous variables were described using maximum, minimum, mean and standard deviation.
RESULTS AND DISCUSSION
Demographic data
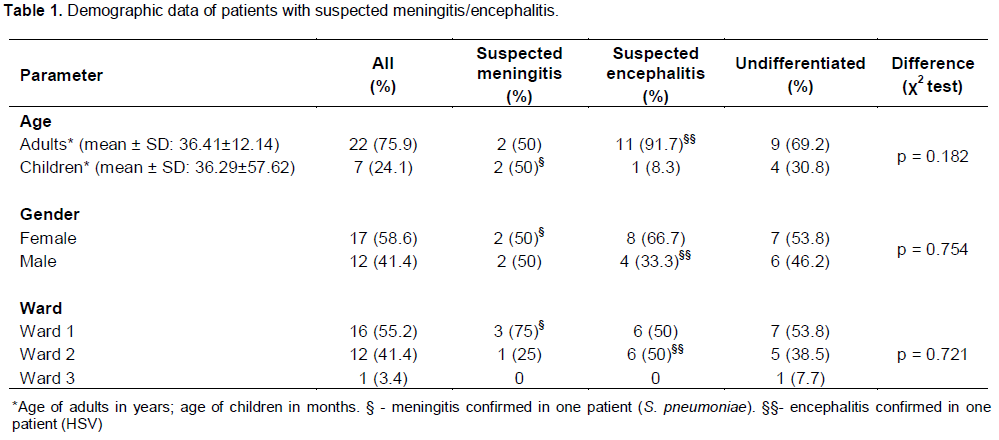
Out of 94 patients’ case notes requested from the BLT Health Records department, only 62 were available for review. After reviewing these notes, 29 patients with suspected meningitis or viral encephalitis fulfilled the inclusion criteria were selected for the data analysis. Their characteristics are presented in Table 1.
Choice of antimicrobials
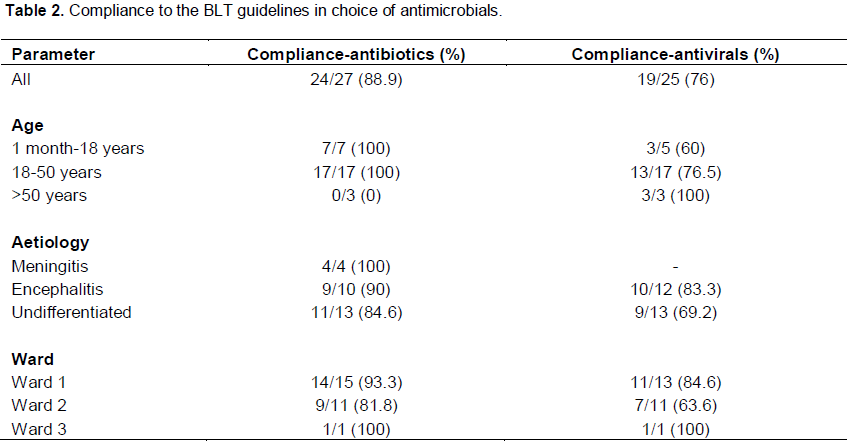
Ceftriaxone was used in all adult patients and in 57.1% (4/7) paediatric patients for the empirical treatment of suspected meningitis. Children younger than 3 months (3/7) were commenced on a combination of cefotaxime and amoxicillin. Cefotaxime is the equivalent cephalosporin to ceftriaxone for the empirical treatment of meningitis in children < 3 months and the addition of amoxicillin is recommended. Aciclovir was the only antiviral drug used for empirical treatment of suspected encephalitis. Compliance to the Trust guidelines in use of antibiotic/antiviral in the empirical treatment of acute meningitis/encephalitis in relation to differential diagnosis was assessed and results are shown in Table 2. Compliance to the Trust guidelines in use of antibiotics was 100% in children and adults between 18 and 50 years, in contrast to older patients where amoxicillin was not introduced to any of 3 patients to cover possible Listeria infection. Compliance to the Trust guidelines in introducing aciclovir in empirical treatment of patients with suspected encephalitis was 76% and it varied among age groups, aetiology groups and different wards. 100% compliance was noted in patients above 50 years of age and in 1 patient treated on a ward 3, while the lowest was seen on the ward 2 (63.6%).
Dose of antimicrobials
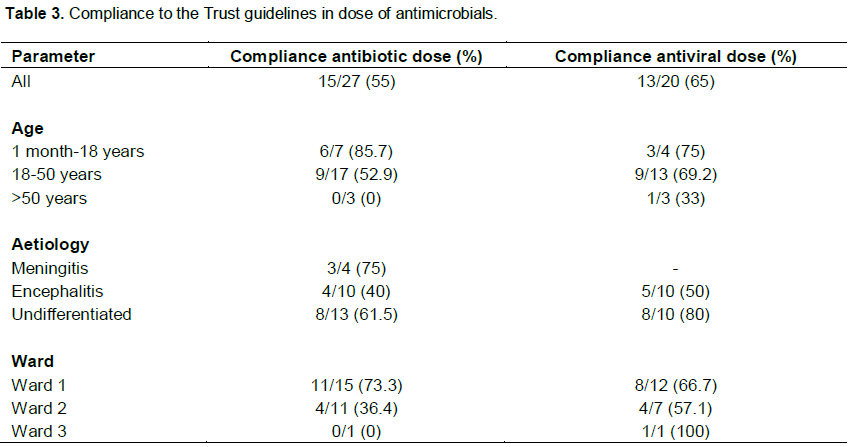
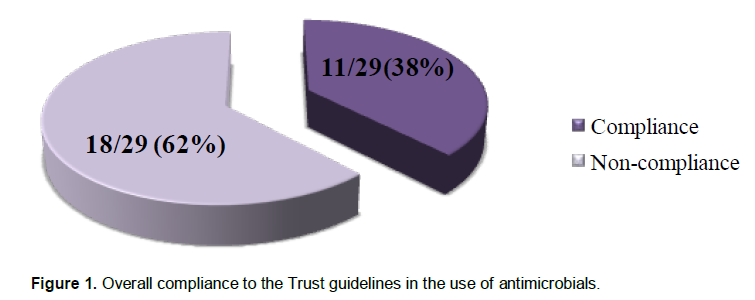
The dose of antimicrobial/antiviral drugs used for the empirical treatment of acute meningitis/encephalitis was studied and compared to those recommended by the Trust guidelines. The mean value for daily dose of ceftriaxone in adults was 2.85 g ± 1.09 (min: 1 g, max: 4 g) and in children 1.31 g ± 0.71 (min: 0.54 g, max: 2.50 g). The mean value for the daily dose of aciclovir in adults was 1851.56 mg ± 666.72 (min: 855 mg, max: 3000 mg), while in children it was 813 mg ± 543.10 (min: 264, max: 1350). Compliance to the Trust guidelines in dosing antimicrobials for the empirical treatment of acute meningitis/encephalitis is presented in Table 3. Where doses varied against the recommended regimen, intentional noncompliance to guidelines were investigated in the medical notes. The dose was deemed non-complaint if there was no intentional or measured deviation documented in the medical notes. Compliance to the Trust guidelines was higher with dosing of antivirals compared to antibiotics (65% vs. 55%) and it differed among age groups, aetiology groups and different wards, but a significant difference was seen only in compliance among different age groups in antibiotic dosing (χ2 = 2, N = 29) = 6.376; p = 0.041) with significantly lower compliance in patients above 50 years of age compared to other two groups. Overall compliance to the Trust guidelines in the use of antimicrobials (antibiotics and antivirals) is calculated and presented in Figure 1.
Use of corticosteroids in the treatment of suspected meningitis/encephalitis
Corticosteroids were not used in any of 29 patients admitted to the BLT with suspicion of acute meningitis/encephalitis who were included in this study; hence indication for their usage (type of meningitis), dose, timing and duration could not have been assessed.
Time to first dose of antimicrobials from presentation/arrival
Time to first dose of antibiotic or antiviral was calculated as a difference from date and hour of the patient's admission to the hospital written in medical notes to the time of administering of antibiotic or antiviral noted on the patient’s drug chart. Figures 2 and 3 represent the percentage of patients to whom antibiotics/antivirals were given in the first hour, in the period less than 3 h (1 to 3 h), in the period less than 6 h (3 to 6 h) or after 6 h from the patient's presentation/arrival at the hospital.
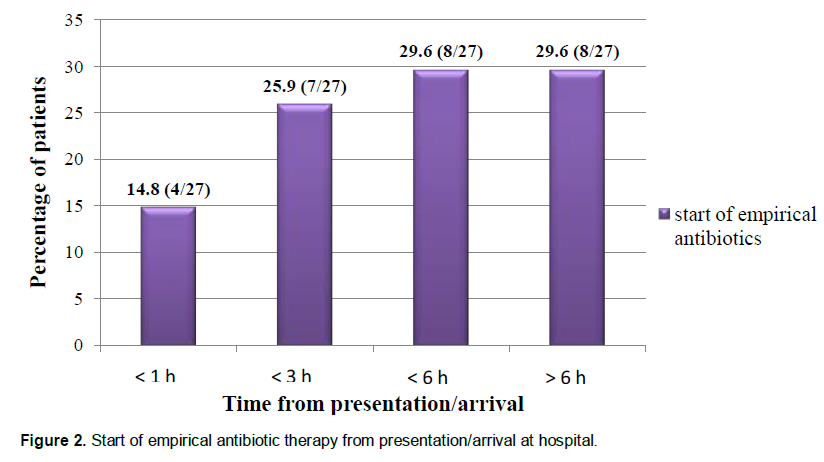
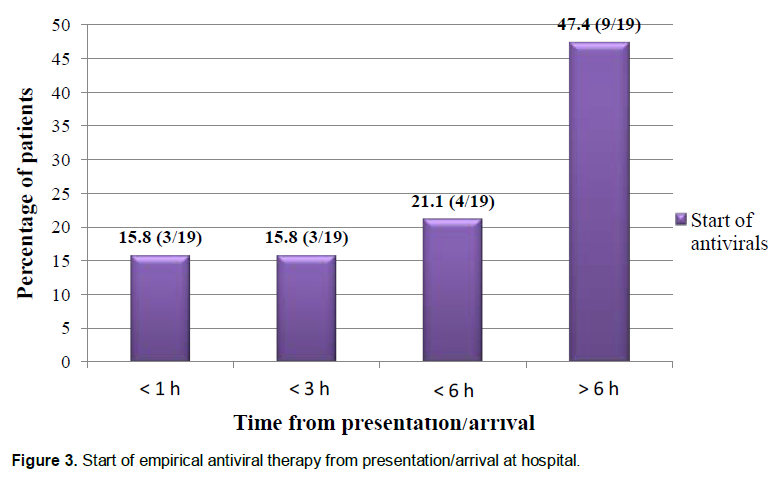
Mean time to first dose of antibiotic from presentation was 6.18 ± 8.39 h (min: 0, max: 32.16), while mean time to first dose of antiviral from presentation was 8.19 ± 9.41 h (min: 0, max: 35.16). The ANOVA test was initially chosen for finding any difference between three wards, but it was not possible to perform post-hoc analysis since one of the wards had only 1 patient (ward 3). An independent sample t-test was performed instead which revealed a significant difference in time to first dose of antibiotic between ward 1 and ward 3 {t (14) = -11.51, p < 0.001} and between ward 2 and ward 3 {t (10) = -2.69, p = 0.023}, while the difference was not significant between ward 1 and ward 2. A significant difference was seen between the same wards in time to first dose of antivirals as well: ward 1 and ward 3 {t (10) = -8.203, p < 0.001}; ward 2 and ward 3 {t (6) = -2.526, p = 0.045). Time to first dose of antibiotics and antivirals at ward 3 was much longer compared to both ward 1 and ward 2.
The primary outcome of this study was the extent to which prescribers comply with the Trust guidelines regarding empirical antimicrobial therapy of suspected acute meningitis/encephalitis and the use of corticosteroids. Firstly, the choice of antibiotics and antivirals was studied and it was found to be appropriate in most of the patients. Ceftriaxone was used as antibiotic of choice in adults and children older than 3 months while a combination of cefotaxim and ampicillin was introduced in children younger than 3 months which was all in accordance with the Trust guidelines. However, all 3 patients above 50 years were treated outside of the Trust guidelines, since amoxicillin was not added to ceftriaxone to cover possible Listeria monocytogenes infection. The reason for this might be the unawareness of the probable causative microorganisms or the choice of antibiotic in this age group by the prescribers. Although acyclovir was the only antiviral drug used for empirical treatment in patients included in this study, it was sometimes omitted without any clear reason (contraindication such as renal insufficiency) in the management of patients with suspicion on both meningitis and encephalitis (undif-ferentiated group). Generally, compliance to the Trust guidelines was lower with use of antivirals and the ward 2 was identified as the one with the lowest compliance regarding choice of antimicrobials in empirical treatment.
Fairly low compliance to the Trust guidelines in antimicrobial dosing was noticed in this retrospective audit when all aspects are considered. A trend of lower compliance with increase in patients’ age was observed. The reason for noncompliance in antibiotic (ceftriaxone) dosing was mostly a smaller dose given with appropriate frequency (1 g b.d. instead of 2 g b.d.) or the dose was appropriate but the drug was not given frequently enough (o.d instead of b.d.). This lower dose was mainly seen in patients over the age of 50 implying prescribing may feel the need to dose reduce in older patients, however no calculated renal impairment was found and no intentional deviation was documented. Regarding aciclovir, lower doses were given instead of the recommended dose stated in the Trust guidelines (that is, 5 mg/kg t.d.s. instead of 10 mg/kg t.d.s..). It is important to note that the ward pharmacist intervened for the change of antimicrobial dose in two patients, which was accepted after 1 and 2 days of the treatment start.
Overall, compliance in the use of antimicrobials for empirical treatment of suspected meningitis/encephalitis showed that only one-third of prescribers were complying fully with the Trust guidelines. This result is similar to a Dutch study conducted in 2002, just one year after implementation of the national guidelines (Van de Beek et al. 2002). Higher compliance to Bispectral index (BIS) guidelines was found in a University teaching hospital where in 85% of patients choice of antibiotics was appropriate (Zimmerli 2003). A 10-year retrospective study revealed 65% compliance with Infectious Diseases Society of America (IDSA) guidelines in the management of Intensive Care Units (ICU) patients, which decreased mortality (Brouwer et al. 2010). Low overall compliance in this audit is mostly attributed to using unsuitable dose of generally appropriately chosen antimicrobials. It is possible that prescribers are not aware of the fact that higher doses of antimicrobials are used in meningitis compared to other infections or not familiar with the Trust guidelines for acute meningitis. There was also a tendency to dose lower where there was a lower suspicion of meningitis in the differential diagnosis.
Regarding the use of corticosteroid, these were not used in empirical treatment of any patients involved in this study including the patient with proven Streptococcus pneumoniae meningitis. Reasons for this might be various: recommendation in the Trust guidelines is not precise enough regarding indication, dosing and possible benefits of corticosteroids in empirical treatment of suspected meningitis/encephalitis; prescribers' suspicion of its efficacy due to lack of large amounts of evidence from randomised controlled trials or the fact that none of the patients had suspicion of S. pneumoniae meningitis accompanied with presence of focal neurologic signs and Glasgow Coma Scale (GCS) score of 8 to 11 (1 patient had GCS = 11 and 1 had GCS = 10), since these patients benefit mostly from corticosteroid treatment (Auburtin et al. 2006; Begg et al. 1999; Korshin et al. 2007; Køster-Rasmussen et al. 2008).
There is no precise recommendation in National BIS, British National Formulary (BNF) and hence not in the BLT guidelines about the timing of antimicrobials in empirical treatment of suspected meningitis/encephalitis. However early treatment is advocated (without any delay) administration of therapy. Unicentre retrospective 14-year study conducted on 286 patients and multicentre 2-year study on 187 patients both showed that in the group of patients with unfavourable outcome antibiotic treatment was significantly delayed and that early adequate antibiotic treatment related to the onset of overt signs of meningitis was independently associated with favourable outcome (OR = 11.19; 95% CI 4.37 to 32.57; p < 0.001 and OR = 1.09/h, CI: 1.01 to 1.19, respectively) (Lepur and Barši? 2007; Stockdale et al. 2011). Study conducted in Addenbrooke's hospital (Cambridge) showed that 70% of empirical antibiotics were given in a time period of less than 1 h from arrival of 116 adult patients with suspected meningitis to the hospital (Chadwick and Lever 2002). Median time between arrival and first dose of antibiotic was 90 min, while in the study presented here it was 3.53 h (211.8 min) which is almost 2.5 times longer. Empirical antimicrobial treatment was started after 3 h of presentation in more than half of the patients and after 6 h in one third of patients. There were further delays in the introduction of antiviral therapy since almost half of the patients received treatment after 6 h of presenting to the BLT. Reasons for these delays have not been clear, and some future prospective audit could help to identify this.
One study identified computed tomography (CT) head scan as one of the reasons for the delay of antibiotics, which when greater than 6 h, significantly increased risk of death for 8.4 times (95% CI, 1.7 to 40.9) (Georges et al. 2009). Another study showed that delay in antibiotic introduction longer than 3 h was one of the predictors of 3-months mortality (OR, 14.12; 95% CI, 3.93 to 50.9; p < 0.0001) (Proulx et al. 2005). It was found that time to first dose of antimicrobials was significantly further delayed in ward 3 compared to ward 1 and ward 2 which is consistent with the logistics of patients admission pathway. The patient on the ward 3 received their antimicrobial 32 h after admission. Results obtained from this retrospective audit can be added to other studies with similar research objectives. The advantage of this study can be found in the fact that, while others were mostly concentrating on one aspect of management of patients with suspected meningitis/encephalitis, this retrospective audit looked at antimicrobial choice, dose as well as the timing of pharmacological management of these patients in all age and aetiology groups. In this way a complete picture of patients’ treatment was observed.
A few limitations were identified in the audit. A relatively small number of patients was included in the study out of which only two patients had confirmed diagnosis of meningitis/encephalitis. Only patients with lumbar puncture performed were involved in this audit, since it was a method of recruiting patients. The interpretation of data was limited by the quality of medical note keeping and availability of medical record.
A retrospective review conducted at the Barts and the London NHS Trust of 29 patients who presented with suspected acute meningitis/encephalitis over a period of 18 months showed a relatively low level of compliance to the full application of Trust meningitis guidelines. Although, the choice of antimicrobials was mostly appropriate (except for older patients where amoxicillin was not added), the doses of drugs were often smaller than recommended. The start of empirical therapy was significantly delayed in relation to the hospital admission. Corticosteroids were not introduced in the empirical treatment of patients enrolled in this study, including the one patient later diagnosed of S. pneumoniae meningitis.
RELEVANCE OF THE FINDINGS TO PRACTICE
1. The Trust guidelines need to be reviewed in the light of some recent evidence about the use of corticosteroids in acute meningitis.
2. Causative microorganism in certain age and therapy indicated (for example addition of amoxicillin to cover Listeria monocytogenes infection) are not on the same place in the guidelines (it could be missed by junior physician who is using the guideline for the first time). Hence, it would be useful to place all information such as age group, causative microorganism, recommended the-rapy (dose, frequency and duration) in one table or algorithm.
3. The recommendation for the timing of empirical the-rapy could also be more specific in the Trust guideline, by changing it from ‘give empirical therapy without delay’ to ‘give empirical therapy within the first hour of patient’s arrival to the hospital’.
4. After review of the Trust guidelines for the manage-ment of acute meningitis/encephalitis, education in form of lectures and presentations (including the results of this audit) should be provided for junior physicians and pharmacists where the importance of liaison with the Microbiology department and Microbiology pharmacist would be outlined.
CONFLICT OF INTEREST
Authors declare that they have no conflicts of interest
REFERENCES
|
Van de Beek D, de Gans J, Spanjaard L, Dankert J (2002). Antibiotic guidelines and antibiotic use in adult bacterial meningitis in The Netherlands. J. Antimicrob Chemother. 49(4):661-6. Crossref |
||||
|
Lepur D, Baršić B (2007). Community-Acquired Bacterial Meningitis in Adults: Antibiotic Timing in Disease Course and Outcome. Infection 35(4):225-31. Crossref |
||||
|
Van de Beek D, De Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M (2004a). Clinical Features and Prognostic Factors in Adults with Bacterial Meningitis. New Engl. J. Med. 351(18):1849-59. Crossref |
||||
|
Cullen MM (2005). An audit of the investigation and initial management of adults presenting with possible bacterial meningitis. J. Infect. 50(2):120-4. Crossref |
||||
|
Van de Beek D, de Gans J, Tunkel AR, Wijdicks EF (2006). Community acquired bacterial meningitis in adults. N. Engl. J. Med. 354(1):44-53. Crossref |
||||
| Fitch MT, van de Beek D (2007). Emerg. Diagn. Treatment Adult Meningitis 7(3):191-200. | ||||
|
Heyderman RS, Lambert HP, O'Sullivan I, Stuart JM, Taylor BL, Wall RA (2003). Early management of Suspected Bacterial Meningitis and Meningococcal Septicaemia in Adults. J. Infect. 46(2):75-7. Crossref |
||||
|
Van de Beek D, De Gans J, McIntyre P, Prasad K (2004b). Steroids in adults with acute bacterial meningitis: a systematic review. Lancet Infect. Dis. 4(3):139-43. Crossref |
||||
| Begg N, Cartwright J, Cohen EB, Kaczmarski EB, Innes JA, Leen CL, Nathwani D, Singer M, Southgate L, Todd WT, Welsby PD, Wood MJ (1999). Consensus Statement on Diagnosis, Investigation, Treatment and Prevention of Acute Bacterial Meningitis in Immunocompetent Adults J. Infect. 39(1):1-15. | ||||
|
O'Donnell EP, Hurt KM, Scheetz MH, Postelnick MJ, Scarsi KK (2009). Empiric antibiotic selection for infectious emergencies: bacterial pneumonia, meningitis and sepsis. Drugs Today (Barc). 45(5):379-93. Crossref |
||||
|
Korshin A, Køster-Rasmussen R, Meyer CN. Danish Bacterial Meningitis Group (2007). Adjunctive steroid treatment: local guidelines and patient outcome in adult bacterial meningitis. Scand J. Infect. Dis. 39(11-12):963-8. Crossref |
||||
|
Peterković V, Trkulja V, Kutleša M, Krajinović V, Lepur D (2012). Dexamethasone for adult community-acquired bacterial meningitis: 20 years of experience in daily practice. Neurology 259(2):225-36 Crossref |
||||
|
Chadwick DR, Lever AML (2002). The impact of new diagnostic methodologies in the management of meningitis in adults at a teaching hospital. QJM 95(10):663-70. Crossref |
||||
|
Gjini AB, Stuart JM, Cartwright K, Cohen J, Jacobs M, Nichols T, Ninis N, Prempeh H, Whitehouse A, Heyderman RS (2006). Quality of in-hospital care for adults with acute bacterial meningitis: a national retrospective study. QJM 99(11):761-9. Crossref |
||||
|
Sáez -Llorens X, O'Ryan M (2001). Cefepime in the empiric treatment of meningitis in children. Pediatr. Infect. Dis. J. 20 (3):356-61. Crossref |
||||
| Mitropoulos IF, Hermsen DE, Rotschafer CJ (2008). Central Nervous System Infections. In: Pharmacotherapy-A pathophysiologic approach. McGraw – Hill. pp 1923-1942. | ||||
|
Chaudhuri A, Martin PM, Kennedy PG, Andrew Seaton R, Portegies P, Bojar M, Steiner I, EFNS Task Force (2008). EFNS guideline on the management of community-acquired bacterial meningitis: report of an EFNS Task Force on acute bacterial meningitis in older children and adults. Eur. J. Neurol. 15 (7):649-59. Crossref |
||||
|
Solomon T, Hart IJ, Beeching NJ (2007). Viral encephalitis: a clinician's guide. Pract. Neurol. 7(5):288-305. Crossref |
||||
|
Tunkel AR, Hartmen BJ, Kaplan SL, Kaufman BA, Roos KL, Scheld WM, Richard JW (2004). Practice Guidelines for the Management of Bacterial Meningitis by The Infectious Diseases Society of America. Clin. Infect. Dis. 39(9):1267-84. Crossref |
||||
|
Stockdale AJ, Weekes MP, Aliyu SH (2011). An audit of acute bacterial meningitis in a large teaching hospital 2005-10. QJM 104(12):1055-63. Crossref |
||||
|
Georges H, Chiche A, Alfandari S, Devos P, Boussekey N, Leroy O (2009). Adult community-acquired bacterial meningitis requiring ICU admission: epidemiological data, prognosis factors and adherence to IDSA guidelines. Eur. J. Clin. Microbiol. Infect. Dis. 28(11):1317-25. Crossref |
||||
|
Zimmerli W (2003). Acute bacterial meningitis: a time for a better outcome. Intensive Care Med. 29(11):1868-70. Crossref |
||||
| Brouwer MC, McIntyre P, de Gans J, Prasad K, van de Beek D (2010). Corticosteroids for acute bacterial meningitis. Cochrane Database Syst. Rev. 8(9):1-73. | ||||
|
Auburtin M, Wolff M, Charpentier J, Varon E, Le Tulzo Y, Girault C, Mohammedi I, Renard B, Mourvillier B, Bruneel F, Ricard JD, Timsit JF (2006). Detrimental role of delayed antibiotic administration and penicillin-nonsusceptible strains in adult intensive care unit patients with pneumococcal meningitis: the PNEUMOREA prospective multicenter study. Crit. Care Med. 34(11):2758-65. Crossref |
||||
|
Køster-Rasmussen R, Korshin A, Meyer CN (2008). Antibiotic treatment delay and outcome in acute bacterial meningitis. J. Infect. 57(6):449-54. Crossref |
||||
|
Proulx N, Frechette D, Toye B. Chan J, Kravcik S (2005). Delays in the administration of antibiotics are associated with mortality from acute bacterial meningitis. QJM 98(4):291-8. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


