Full Length Research Paper
ABSTRACT
Misuse of antibiotics is the main cause for resistance development. The objective of this study is to assess patterns of antibiotics use and associated problems at Jimma Health Center. The study was conducted from February 25, 2016 to March 25, 2016. For the analysis of prescribing indicators retrospectively 295 patient charts that fulfills inclusion criteria were systematically selected from a total of 9800 charts from the health center registry department (from March 8, 2015 to March 25, 2016). Prospectively 120 patients were interviewed. The average number of drugs per encounter was 2.2 and percentage of encounter with antibiotics was 32%. 98.9% of medication was prescribed by their generic name and injection encounter was 9%. Amoxicillin was a commonly prescribed antibiotic during the study period (26%). The average consultation and dispensing time were 5.1 and 1.3 min, respectively and 73% of drugs dispensed were adequately labeled. There was a copy of Ethiopian essential drug list and standard treatment guidelines (STG - 2014). There was no drug formulary during the study period and some antibiotics were not available. Result of this study revealed prescribing practices and average number of drugs per prescription slightly deviate from World Health Organization standard. But generic and injection prescribing as well as use of Ethiopian essential drug list was not a problem.
Key words: WHO guideline, antibiotics, prescribing indicators, Jimma Health Center.
INTRODUCTION
An antibiotic is a drug that kills or slows the growth of bacteria. The history of use of antimicrobials has history of mankind. But misuse resulted in development of resistance (Chem et al., 2018). Even though irrational use of antibiotics is a worldwide problem it is more prevailing in developing countries because of different factors (Sarwar et al., 2018). In the United States and Canada 30 to 50% of antibiotics prescription was inappropriate. Similarly, in some Asian and African nations, 50% of antibiotic use has been identified as inappropriate (Nepal et al., 2020).
Studies show that analgesics and antibiotics are commonly prescribed in Ethiopia. Overuse of antibiotics (38%) might be a cause for resistance development and not economical too. Besides, empirical treatment which might result from inappropriate diagnosis is also a problem (Desalegn, 2013). Since antibiotics resistance has been a major challenge in controlling infectious diseases, urgent steps are needed to promote rational use (Meher and Mukharjee, 2014). WHO advocates rational use of antibiotic to minimize antibiotic resistance (Orlando et al., 2020).
WHO has prepared a guideline that helps to evaluate antibiotics use (WHO, 1993), since 80% of antibiotics use occurs in the community either due to inappropriate prescribing or self-medication practice (Lim et al., 2012). Primary health care providers should play a major role in promoting rational use of drugs (Chem et al., 2018).
In primary health care centers and health posts approximately half of medicines prescribed are antibiotics, possibly indicating excessive and inappropriate prescribing of antibiotics. These facilities often lacks laboratory services and can be run single – handedly by a health worker who, although untrained, is expected to provide the full spectrum of services (Nepal et al., 2020). In Ethiopia a lot of studies were conducted on utilization patterns of antibiotics, however, the studies mainly focused on either secondary or tertiary health care facilities. This study is focused on primary health care facility.
METHODOLOGY
Study setting and period
This study was carried out in Jimma Health Center (JHC), which is among the health facilities in Jimma zone, south west Ethiopia from February 25, 2016 to March 25, 2016. JHC was established in 1969. It had 49 staffs (both professionals and non-professionals) during the study period. It gives clinical services for about 30,000 attendants per year coming to the health center out of catchment population of about 52,000 people. Major health care services provided by the three service teams were (1) adult and under five outpatient services include diagnostic and treatment, laboratory and pharmacy services. (2) Disease prevention services were on: counseling and testing of HIV/AIDS, prevention of mother to child transmission (PMTCT), family planning (FP), expanded program on Immunization (EPI), antenatal care (ANC) and postnatal care (PNC) services. (3) Inpatient or admission services: emergency and delivery services were included. The health center provides different pharmacy services (in patient, emergency, outpatient, and pharmaceutical stock management and drug information services) through one window for both inpatients and out patients.
Study design
A cross sectional study design was used and data was collected retrospectively and prospectively. For analysis of prescribing indicators, 295 patient charts that fulfill inclusion criteria were systematically selected from a total of 9800 charts from the health center registry department (from March 8, 2015 to March 25, 2016). The first record card was randomly selected and then every 33rd was taken (WHO, Policy Perspective on Medicines, 2002).
Prospectively one hundred twenty patients were interviewed at the outpatient pharmacy while drugs were dispensed to assess the patient care indicators and the availability of standard guidelines and key medications in the stock were observed.
Population
Source population were all in and out patients in JHC and study population were those patients whose records were checked and those patients who were interviewed and health professionals who participated by filling the questioner during the study period.
Sample size determination
Sample size was determined by using correction formula Assumptions, where n is minimum sample size, z is reliability coefficient for the desired confidence interval. Z for 95% is 1.96. P is the proportion of antibiotics prescribed. Thus p = 0.2343, q = 1- p = 1-0.2343 = 0.7657, d = 0.05 (taking 5% as margin of error).
n = (z2pq/d2) = ((1.96)2 × 0.2343 × 0.7657/ (0.05)2) = 276
where Nf = final sample size by using correction formulas, N = total number of patients who were served from March 8, 2015 to March 25, 2016 in JHC. Nf = (n/ (1+n/N)) = 268 + 10% = 295.
Study variables
Dependent variables of this study were: prescribed antibiotics, percent of drugs actually dispensed, average dispensing and consultation time, patient knowledge and labeling pattern of drugs. Whereas the independent variables were socio demographic characteristics, prescribing patterns and drug use problems in prescribing patterns.
Data collection process
Both quantitative and qualitative techniques were used.
Record review
Data collection sheets namely the prescribing indicator and facility indicator forms were used. Prescribing indicator form was used to collect information from patient files at the health center registry. The facility indicator form was used to collect information from health center pharmacy.
Self-administered questionnaire
By using semi structured self-administered questionnaire, information on the availability of key personnel involved in the rational use of drugs was collected and prospectively from patients while drugs were dispensed.
Data processing and analysis
Information obtained was checked and verified before analyzing using computer software SPSS version 16. The cut off for statistical significance was set at 5% level. All the required statistical and non-statistical data analyses were performed. Finally, data was interpreted and presented in tabular forms.
Prescribing indicators
Based on WHO (1993) how to investigate drug use in health facilities guideline the following were assessed: average number of drugs prescribed per encounter; percentage of drugs prescribed by generic name; percentage of encounters in which an antibiotic was prescribed; percentage of encounters with an injection prescribed; and percentage of drugs prescribed from an essential drug list were calculated with their respective formulas as per the guideline.
Ethical approval
Recommendation letter was written to Jimma Health Center from School of Pharmacy, Institute of Health Sciences, Jimma University. Confidentiality of patients’ chart was kept and data was collected anonymously. Besides, verbal consent was taken from the study participants.
RESULTS
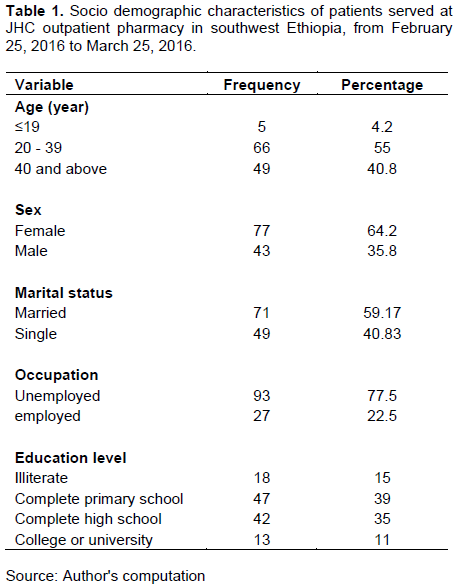
Age composition of the study population was 5 (4.2%), 66 (55%), and 49 (40.8%) below and equal to 19, from 20 to 39 and greater or equal to 40 years, respectively. Sex wise from 120 patients, 43 (35.8%) were males, and 77 (64.2%) were females. Based on marital status, 71 (59.17%) were married and 49 (40.83%) were single. With regard to occupational status employed were 27 (22.5%) and unemployed were 93 (77.5%). Out of patients who were interviewed at outpatient pharmacy, 47 (39%) of them completed primary school, 42 (35%) completed high school, 13 (11%) were college or university graduates, and the remaining 18 (15%) were illiterate (Table 1).
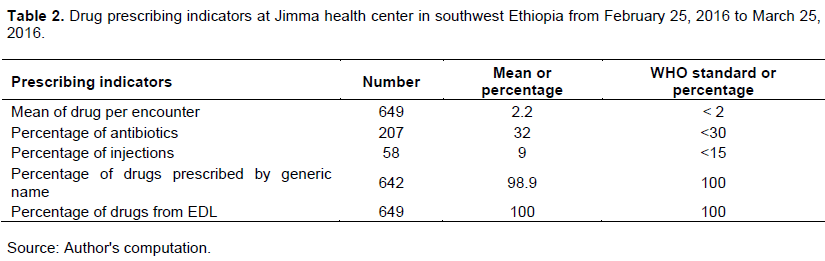
In this study in 295 patient charts, 649 medications were prescribed. Mean of medications per prescription was 2.2 and total number of drugs prescribed by their generic name was 642 (98.9%). Total numbers of antibiotics were 207 (32%) and injections were 58 (9%) (Table 2). All medications were prescribed from essential drug list of Ethiopia.
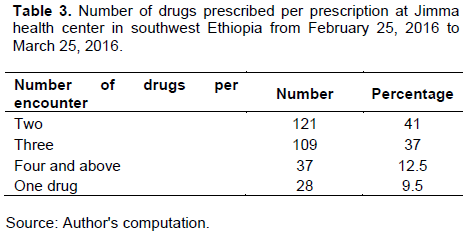
This study revealed that number of drugs per prescription were two (41%) and three (37%) (Table 3).
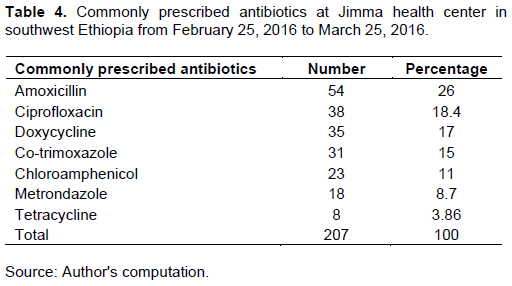
In this study, amoxicillin was the mostly prescribed antibiotic 54 (26%), followed by ciprofloxacin 38 (18.4%), and doxycycline 35 (17%) (Table 4).
Patient care indicators
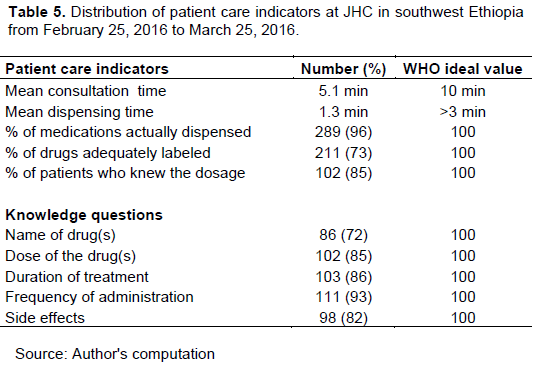
Results of the present study demonstrated that mean consultation time was 5.1 min and mean dispensing time was 1.3 min. Besides, percentage of drugs actually dispensed was 96% and adequately labeled were 73%. Patients’ knowledge of the correct dosage was 85% (Table 5).
Regarding the health facility, there was a copy of standard treatment guidelines (STG-2014) and Ethiopian essential drug list, but did not have drug formulary during the study period. Besides, some key antibiotics were not available. Regarding prescribers, three clinical officers and eight registered nurses were involved in prescribing. Besides, the health center had one pharmacist and one druggist during the study period.
DISCUSSION
Prescribing indicators
This study showed in 295 patient charts 649 medications were prescribed. The average number of drugs per prescription was 2.2 which was higher than the standard set by WHO (<2). Previous study conducted in Jimma Health Center reported 2.24 (Angamo et al., 2011). The slight variation might be due to inclusion of other medications other than antibiotics in the previous study. The study conducted in south and southwestern Ethiopia reported 1.9 and 1.59, respectively (Desalegn, 2013; Yenet, 2005). It was also higher than reports of Meher and Mukharjee (2014), Achalu et al. (2015), Chem et al. (2018), Yimenu et al. (2019) and Sarwar et al. (2018) in which the average number of drugs per encounter was 1.8, 2.17, 1.14, 1.6, and 1.4 respectively.
Lower number of drugs per prescription promotes rational use of drugs, reduces poly pharmacy and disease complications. In this study percentage of antibiotics per prescription was found to be 32%, slightly higher than WHO standard (<30%). It was also higher than previous study conducted in JHC which was 23.42% (Angamo et al., 2011), Sweden 30% (Goossens et al., 2005) and India 19.44% (Ragma et al., 2017). But less than reports of Chem et al. (2018), Mollahaliloglu et al. (2012) and Sarwar et al. (2018) which were 36.71, 34.8 and 81.5%, respectively. It was also less than study conducted in three developing countries (71.8%) Sudan (Elsalahi et al., 2014), (63.3%) India (Jain et al., 2013) and (34.4%) in Nigeria (Tamuno and Fadare, 2012). Report from Hawassa (58%) and Debretabor hospital 69% (Desta et al., 2012), Gondar hospital 69.6% (YImenu et al., 2019), Addis Ababa 38% (Worku and Tewahido, 2018) and southern Ethiopia 58.1% (Summoro, 2015) was also higher than the present value.
Study conducted in India reasoned lower percentage of antibiotics per prescription might be due to the presence of antibiotic policy explaining the specific antibiotic prescription to the specific site of infection and reduced the generous use of antibiotics to viral illness and symptomatic approach without proper diagnosis (Ragam et al., 2017). Ethiopia does not have separate policy for antibiotics. Antibiotics use was included in STG – 2014 that contains the list of medicines for health centers (List of Medicine for Health Centers, EFMHACA, 2012). But it does not provide enough information on the specific uses of each of the antibiotics (Worku and Tewahido, 2018). Therefore, absence of separate guideline might be a reason for over prescribing of antibiotics in the study area. In addition to the fact that high percentage might be due to cultural beliefs about antibiotics, patients’ expectation to receive and prescribers’ belief on the low therapeutic efficacy of antibiotics. The other reason might be due to the differences among health facilities. In secondary and tertiary health care facilities more complicated cases are managed, as a result more antibiotics are prescribed. Whereas, in primary health care, primary complications in the communities are managed and it may not as such require multiple prescription of antibiotics.
According to this study, amoxicillin (26%) was commonly prescribed followed by ciprofloxacin (18.4%) and doxycycline (17%). Study conducted in Ghana reported amoxicillin (22.5%) and ciprofloxacin (18.4%) (Prah et al., 2017) almost similar with the result of this study. Similarly, study conducted in Gondar (Yimenu et al., 2019) also reported amoxicillin (28.5%) and ciprofloxacin (12%) as the commonly prescribed antibiotics.
Studies conducted in Addis Ababa (Worku and Tewahido, 2018) and Gondar (Getachew et al., 2013) showed amoxicillin as the commonly prescribed antibiotic. Similarly, study in Cameroon revealed that Amoxicillin (29.29%) followed by cotrimoxazole (19.08%) and metronidazole (15.59%) (Chem et al., 2018) were commonly prescribed antibiotics. Study conducted in Jimma University specialized hospital also reported amoxicillin as the most prescribed antibiotic (Asrat and Hailemeskel, 2008).
On the other hand studies conducted in Pakistan, India and China reported penicillins, fluoroquinolones and cephalosporins were the most commonly prescribed antibiotics, even though the commonly used antibiotics in many European countries were tetracyclines, benzylpencillins and sulfonamides (Sarwar et al., 2018). Similar study from Nepal reported that the most commonly prescribed antibiotics were ceftriaxone followed by amoxicillin/cloxacillin, azithromycin and cefixime among others (Nepal et al., 2020). The difference might occur because of regional variations in bacterial susceptibility, resistance, prescribing habit and the difference in prevalence of infectious disease. Types of health care facilities and preference of prescribers might be other factors.
Percentage of an encounters with an injection prescribed was calculated to measure the overall level use of commonly overused and costly forms of drug therapy. This study showed that injections were prescribed in 8.9% encounters which were within the limit set by WHO (<15%). It was also less than previous study conducted in JHC (9.9%) and it was encouraging (Angamo et al., 2011). It was much lower than studies conducted in Gondar, Dessie, Hawasa and Wolayita which were reported as 28.7, 37.5, 38.1 and 50%, respectively (Yimenu et al., 2019). Variations might be due to differences in health care facilities. This study focused on primary health care center whereas latter reports were from secondary and tertiary health care facilities.
In this study, total number of drugs prescribed by generic name was 98.9%. It was slightly lower than WHO (100%) standard. But greater than previous study conducted in JHC (75.61%) (Angamo et al., 2011). This shows an improvement and it was encouraging. The results of the present study was also similar to study conducted in Cameroon (Chem et al., 2018), Cambodia Health Center (Chareonkul et al., 2002), Hawasa (Dessalegn, 2013), Jimma (Achalu et al., 2015) which was 98.36, 99.8, 98.7 and 99%, respectively.
But the study conducted in India (Meher and Mukharjee, 2014) reported only 16% of antibiotics were prescribed by their generic name and study from Kenya reported 62.5% were prescribed by their generic names (Yimenu et al., 2019). Generic prescribing reduces the chances of drug duplication (Fadare et al., 2016); besides, it also avoids confusions between prescribers and dispensers.
The variations observed among countries might be due to medication procurement policies. In the case of Ethiopia, procurement policy promotes procurement by generic name. Within the country the difference might be due to the type of health facilities and prescribers. At secondary and tertiary health care facilities in most cases prescribers prefer brand names to prescribe than generic names.
Patient care indicators
This study showed mean consultation and dispensing time 5.1 and 1.3 min, respectively. Previous study conducted at JHC reported 6.39 and 1.25 min for consultation and dispensing times, respectively (Angamo et al., 2011). The values were below the standard set by WHO which were more than 10 min for consultation and more than 5 min for dispensing. It might be due to the work load on service providers at the health center but needs consideration. The percentage of drug actually dispensed was 96%. Previous study reported 77.77% (Angamo et al., 2011) and standard set by WHO was 100%. Even though it was below the standard set there was an improvement and it was encouraging.
The percentage of drugs adequately labeled was 73%. Previous report was 68.33% (Angamo et al., 2011) and WHO standard was 100%. Patients’ knowledge of the correct dosage was 85%. Previous study reported 74.28% and WHO standard was 100%. Since all what were mentioned here contribute to the rational use of drugs they require due attention in order to achieve the standard set.
Facility indicators
Regarding the health facility, JHC had a copy of Ethiopian essential drug list and standard treatment guidelines (STG, 2014) but did not have drug formulary and some antibiotics. In this study, all drugs prescribed were from essential drug list of Ethiopia. Similar study conducted in Cameroon reported all drugs prescribed were from WHO list of essential medications (Chem et al., 2018). The current finding showed good prescribing practice. The presence of STG and EML (Essential Medicine Lists), drug formulary and sufficient availability of key drugs at health facility is an indication for good quality care provision and promotion of rational use of medications. On the contrary, unavailability of them might contribute to treatment failure, costly of treatment and development of antimicrobial resistance (Sarwar et al., 2018).
Literatures show that unavailability of drugs, socio-economic status of patients, absence of in service training for prescribers, prescribers’ qualifications and experience are contributing factors for the inappropriate use of antimicrobials in primary health care centers. Besides, medical facilities were more directed towards secondary and tertiary care hospitals in cities limiting exposure and training opportunities of primary health care center staffs (Chem et al., 2018; Sarwar et al., 2018).
Other study reported that a substantial amount of antibiotics overuse is likely driven by over diagnosis of certain conditions, particularly when the clinical picture of viral or bacterial etiology is similar (Prestinaci et al., 2015). In developing countries, other factors contributing to the excessive use of antibiotics include inadequate patient education, limited diagnostic facilities, availability of antimicrobials that can be purchased without a prescription and lack of appropriate drug regulatory mechanisms (Ayukekbong et al., 2017). Similarly, this study identified the issue of overuse of antibiotics, inadequate counseling and dispensing time, inadequate labeling of dispensed medications, unavailability of some antibiotics, unavailability of drug formulary and absence of in service continuous training on rational use and shortage of pharmacists as contributing factors associated with irrational use of antibiotics at JHC during the study period.
CONCLUSION
Based on findings of this study, prescribing practices for antibiotics and average number of drugs per prescription deviate from standard set by World Health Organization. Therefore, it requires close regulation. But generic and injection prescribing and prescribing from essential drug list was not a problem. In this study, amoxicillin was the most prescribed antibiotics followed by ciprofloxacin. Duration of dispensing time, appropriate labeling and patients’ knowledge and availability of enough antibiotics and trained manpower also need due consideration.
LIMITATION OF THE STUDY
This study was conducted in Jimma health center. Therefore, the findings cannot be generalized to all health facilities in Jimma town. Moreover, some results were compared with findings of secondary and tertiary health care facilities.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
ACKNOWLEDGEMENTS
The author thanks school of pharmacy, Institute of health sciences, Jimma University for allowing them to conduct the study and writing recommendation letter to Jimma health center. Also staffs of Jimma health center were appreciated for their willingness and support during the study period. Last but not least, thanks go to those patients who participated in an interview.
REFERENCES
|
Achalu ST, Yimam B, Kebede MT (2015). Antibiotics utilization pattern in pediatric ward: The case from tertiary teaching hospital, south west Ethiopia. International Journal of Advanced Multidisciplinary Research 2(9):54-61. |
|
|
Angamo TM, Wabe TN, Raju JN (2011). Assessment of patterns of drug use by using World Health Organization's prescribing, patient care and health facility indicators in selected health facilities in southwest Ethiopia. Journal of Applied Pharmaceutical Science 1(7):62-66. |
|
|
Asrat A, Hailemeskel M (2008). Drug prescribing practice in Jimma University specialized hospital pediatric ward, Ethiopia. International Research Journal of Pharmacy and Pharmacology 2(6):132-138. |
|
|
Ayukekbong JA, Ntemgwa M, Atabe AN (2017). The threat of antimicrobial resistance in developing countries: causes and control strategies. Antimicrobial Resistance and Infection Control 6(1):1-8. |
|
|
Chareonku C, Khum V, Boonshuyar C (2002). Rational drug use in Cambodia: study of three pilot health centers in kampong horn province, south east Asian. Journal of Tropical Medicine and Public Health 33:418-424. |
|
|
Chem ED, Anong DN, Akoachere J-FKT (2018). Prescribing patterns and associated factors of antibiotic prescription in primary health care facilities of Kumbo east and Kumbo west health districts, North West Cameroon. PLoS ONE 13(3):e0193353. |
|
|
Desalegn AA (2013). Assessment of drug use pattern using WHO prescribing indicators at Hawassa University teaching and referral hospital, south Ethiopia: a cross-sectional study. BMC Health Services Research13:170. |
|
|
Desta Z, Abula T, Ganes A, worku A (2002). Prescribing pattern of drugs for outpatient in three hospitals in North West Ethiopia. Journal of health Development 16(2):183-189. |
|
|
Elsalahi SH, Mudawi ME, Ahmed AE (2014). Evaluation of prescribing patterns in primary health care centers of Khartoum state, Sudan. An International Journal of Advances in Pharmaceutical Sciences 5(4):2242-2247. |
|
|
Fadare JO, Adeoti AO, Desalu OO, Enwere OO, Makusidi AM, Ogunleye O, Sunmonu TA, Truter I, Akunne OO, Godman B (2016). The prescribing of generic medicines in Nigeria: knowledge, perceptions and attitudes of physicians. Expert Review of Pharmaco Economics and Outcome Research16(5):639-650. |
|
|
Getachew E, Aragaw S, Adissie W, Agalu A (2013). Antibiotic prescribing pattern in a referral hospital in Ethiopia. African Journal of Pharmacy and Pharmacology 7:2657-2661. |
|
|
Goossens H, Ferech M, Vander Stichele R, Elseviers M, Group EP (2005). Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet 365:579-587. |
|
|
Jain S, Yab Khan Z, Upadhyaya P, Abhijeet K (2013). Assessment of prescription pattern in a private teaching hospital in India. International Journal of Pharmaceutical Science 3(3):219-222. |
|
|
Lim Y, Sivasampu S, Hwong A, Sim B Chandrasekaran S (2012). Prescribing patterns and factors influencing the choice of antibiotics in upper respiratory tract infections. Clinical Research Center Findings, Ministry of Health Malaysia, pp. 1-2. |
|
|
List of Medicine for Health Centers, Ethiopian Food, Medicine and Healthcare (EFMHACA) (2012). Administration and Control Authority, Addis Ababa, Ethiopia, 2012. |
|
|
Meher BR, Mukharjee D (2014). Udayshankar A study on antibiotic utilization pattern in a general medicine ward of a tertiary care teaching hospital. Journal of Chemical and Pharmaceutical Research 6(7):1847-1849. |
|
|
Mollahaliloglu S, Alkan A, Donertas B, Ozgulcu S, Akici A (2013). Assessment of antibiotic prescribing at different hospitals and primary health care facilities. Saudi Pharmaceutical Journal 21(3):281-291. |
|
|
Nepal A, Delia H, Suzanne R, Linda AS (2020). Analysis of patterns of antibiotic prescribing in public health facilities in Nepal. Journal of infection in Developing Countries 14(1):18-27. |
|
|
Orlando V, Valeria Marina Monetti MV, Juste MA, Russo V, Mucherino S, Trama U, Guida A, Menditto E(2020). Drug Utilization Pattern of Antibiotics: The role of age,sex and municipalities in determining variation. Risk Management and Publication Policy 13:63-71. |
|
|
Prah J, Kizzie-Hayford J, Walker E, Ampofo-Asiama A (2017). Antibiotic prescription pattern in a Ghanaian primary health care facility. Pan African Medical Journal 28:214. |
|
|
Prestinaci F, Pezzotti P, Pantosti A (2015). Antimicrobial resistance: a global multifaceted phenomenon. Pathogens and Global Health 109(7):309-318. |
|
|
Ragam AS, Acharya S, Holla R (2017). Assessment of drug use pattern using World Health Organization prescribing indicators in a tertiary care hospital in Mangalore: A cross-sectional study. National Journal of Physiology, Pharmacy and Pharmacology 7(10):1026-1030. |
|
|
Sarwar RM, Saqib A, Iftikhar S, Sadiq T (2018). Antimicrobial use by WHO methodology at primary health care centers: a cross sectional study in Punjab, Pakistan. BMC Infectious Diseases 18:492. |
|
|
Standard treatment guidelines (STG) (2014). Standard treatment guidelines for health centers, Ethiopian Food, Medicine and Healthcare Administration and Control Authority, Addis Ababa, Ethiopia, 2014. |
|
|
Summoro TS, Gidebo KD, Kanche ZZ, Woticha EW (2015). Evaluation of trends of drug-prescribing patterns based on WHO prescribing indicators at outpatient departments of four hospitals in southern Ethiopia. Drug Design and Development Therapy 9:4551-4557. |
|
|
Tamuno I, Fadare JO (2012). Drug prescription pattern in a Nigerian tertiary hospital. Tropical Journal of Pharmaceutical Research 11(1):146-152. |
|
|
Worku F, Tewahido D (2018). Retrospective assessment of antibiotics prescribing at public primary healthcare facilities in Addis Ababa, Ethiopia. Interdisciplinary perspective Infectious disease 4323769. |
|
|
World Health Organization (WHO) (1993). How to investigate drug use in health facilities: Selected drug use indicators. EDM Research series No. 07. WHO, Geneva Switzerland. WHO/DAP/93.1. |
|
|
Yenet W (2005). Base line survey on drug prescribing indicators for outpatients in Jimma University specialized hospital, south west Ethiopia. Ethiopian Journal of Health Science 15(2):147-155. |
|
|
Yimenu KD, Emam A, Elemineh E, Atalay W (2019). Assessment of antibiotic prescribing patterns at outpatient pharmacy using World Health Organization prescribing indicators. Journal of Primary Care and Community Health 10:1-8. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


