Full Length Research Paper

ABSTRACT
The effects of circadian rhythms on the duration of neuromuscular blocking agents are under-investigated. Therefore, the aim of this prospective, observational study was to investigate whether the dosing-time of rocuronium would cause significant differences in the neuromuscular block duration during the four different period of a day in a diurnal based study design. Forty patients were allocated into one of the following four groups according to the surgery timing during a day. Patients undergoing surgery between 07:00 am and 01:00 pm were included in Group M (Group morning, n = 10), between 01:00 pm and 07:00 pm in Group AN (Group afternoon, n = 10), between 07:00 pm and 01:00 am in Group E (Group evening, n = 10), and between 01:00 am and 07:00 am in Group N (Group night, n = 10). All patients received rocuronium in a dose of 0.6 mg/kg. The time to T1 10% and clinical duration were significantly shorter in Group N [24.4 ± 8.0, 28.5 ± 9.0 min, mean ± standard deviation (SD)] when compared with Group AN (32.1 ± 8.6, 36.7 ± 9.1 min, mean ± SD) and Group E (32.5 ± 9.9, 37.0 ± 11.4 min, mean ± SD) (p < 0.05). T1 10% time and clinical duration of rocuronium were significantly shorter when used at nighttime compared to afternoon and evening part of the day. The increased hepatic blood flow and metabolism of rocuronium may be the responsible factors related to this shortening at night.
Key words: Rocuronium, chronobiology, circadian rhythm, neuromuscular non-depolarizing agents, anesthesia, intravenous.
INTRODUCTION
The biologic rhythms are physiological circumstances that provide the adaptation of an organism to the external environment in the absence of environmental time determinants (Chassard and Bruguerolle, 2004). The chronobiology investigates these rhythms and their mechanisms. The most well recognized biologic rhythm is the circadian rhythm that is characterized by a biologic cycle of approximately 24 h (Chassard et al., 2005). There are a great number of studies related to drug and biologic rhythm interactions in clinical medicine (Chassard et al., 2007). However, probably due to two main reasons mentioned, the influence of chronobio-logy on the clinical practice of anesthesiology remains to be determined. The first reason is the combined use of several drugs in the course of anesthesia and therefore, the fear of underestimating or overestimating the interactions between biologic rhythms and anesthetic drugs. In addition to this, because of the concept considering that the circadian rhythms have been overcome with the homeostasis, most of the anesthesiologists have not been interested in chronobiology in their clinical practice (Cheeseman et al., 2007).In the field of anesthesia, the drug dose-response relationship represents an extremely important issue. A large number of clinical and laboratory studies have been designed to establish the factors affecting this dose-response relationship from past to present. Rocuronium is the most rapid onset and the most commonly used non-depolarizing muscle blocker currently available. Factors such as age (Baykara et al., 2002), weight (Leykin et al., 2004), temperature of the patient (Beaufort et al., 1995), as well as the anesthetic agent used for anesthesia maintenance (Maidatsi et al., 2004) affect the duration of action of rocuronium. Whether the chronobiology is another variable affecting the duration of action of rocuronium is controversial. Only one study was under-taken to evaluate the influence of time of day on the clinical duration of rocuronium in the available literature (Cheeseman et al., 2007). However, its design did not include all the time course of a day. The night part of the day denoting the resting period of human individuals had not been considered in the study design. Therefore, we have undertaken a study to in-vestigate whether the dosing-time of rocuronium would cause significant differences in the neuromuscular block duration during the whole day in a diurnal based study design.
MATERIALS AND METHODS
After local ethics committee approval, the patients undergoing elective or emergency abdominal surgery with an expected duration less than four hours between January, 2006 and July, 2006 were enrolled into the study which was conducted according to the Declaration of Helsinki and Good clinical research practice (GCRP) guidelines for pharmacodynamic studies of neuromuscular blocking agents (Fuchs-Buder et al., 2007). The inclusion criteria were 18 to 59 years of age, American Society of Anesthesiologist (ASA) status 1 or 2, actual body weight in the range of 20% of the ideal body weight, normal renal and hepatic function, no history of cardiac and neuromuscular diseases. The exclusion criteria were expected difficult airway, known allergy to one of the study drugs, history of drug usage likely to affect the neuromuscular function. The information about the general anesthesia, monitorization techniques, and the study protocol were given to all subjects and then the informed consent were requested from the patients undergoing elective and emergency surgery the day before and one hour before surgery, respectively.
The patients were allocated into one of the following four groups according to the surgery timing during a day. The patients undergoing elective surgeries between 07:00 am and 01:00 pm were included in Group M (Group morning, n = 10) and between 01:00 pm and 07:00 pm were included in Group AN (Group afternoon, n = 10). The patients undergoing emergent surgeries between 07:00 pm and 01:00 am were included in Group E (Group evening, n = 10) and between 01:00 am and 07:00 am were included in Group N (Group night, n = 10).
After arrival to the operating room, a 20-gauge intravenous (iv) catheter was inserted on the dorsum of the hand or antecubital fossa. Intravenous midazolam (0.4 mg/kg) premedication was given to all patients following routine ASA monitorization including electrocardiogram with continuous ST-T analysis, non-invasive blood pressure, body temperature, and pulse oximetry (Viridia CMS M1166A, Hewlett Packard, Germany). In addition, Bispectral Index (A-2000 XP, Aspect Medical Systems, Inc, USA), weighted sum of several electroencephalographic sub parameters was installed to monitor depth of anesthesia. Neuromuscular function was assessed quantitatively with an acceleromyograph (TOF-Watch ® SX, Organon, Dublin, Ireland) connected to a laptop computer installed with appropriate software via an interface. All patients were warmed with a blanket laid under the patients.
Anesthetic management
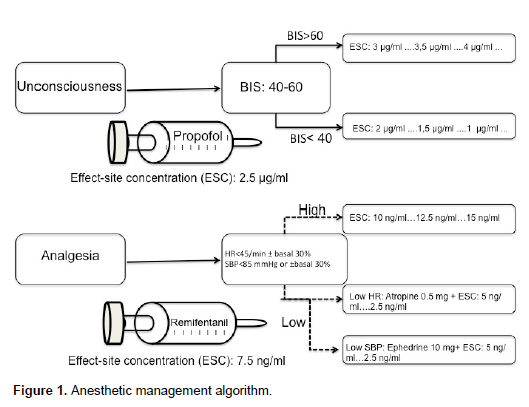
Total intravenous anesthesia (TIVA) with target controlled infusion (TCI) technique using propofol and remifentanil was utilized in anesthesia induction and maintenance of all patients. The demographic data such as age, actual body weight, height and sex were set on the TCI infusion pump (Orchestra ® Base Primea, Fresenius Kabi, Germany), which enables the drug concentration in the plasma (Cp) and at the effect site (Ce) such as brain, to be continuously controlled. The pharmacokinetic model described by Schnider et al. (1998) uses age as a co-variate to improve the accuracy of the model. Because this model has a smaller-volume central compartment and equilibrates more quickly with the effect site, our patients received TCI propofol driven by the Schnider model with effect-site control. Meanwhile, the infusion rate of TCI remifentanil was controlled by Minto's pharmacokinetic model incorporated into software that was previously used specifically for remifentanil (Minto et al., 1997). Syringes containing 1% propofol (10 mg/ml) and remifentanil (50 μg/ml) were simultaneously loaded onto the device and connected to the patient's intravenous catheter using a three-way stopcock.
The anesthesia induction was provided by remifentanil infusion with an effect-site concentration at 7.5 ng/ml following propofol infusion with an effect-site concentration at 2.5 µg/ml. Once the BIS value was lower than 80, the mask ventilation with 100% oxygen was started.
After reaching the target concentrations of anesthetic drugs and before administration of rocuronium, a 50 Hz tetanic stimulation for 5 s was administered followed after 1 min by immobilization of the patient’s fingers. Then the ulnar nerve at the wrist was stimulated in a train-of-four (TOF) mode every 15 s for 3 min. When the calibration process by CAL 2 mode was completed and then stable baseline of the response to TOF was reached, 0.6 mg/kg rocuronium iv was administered in 5 s. The time between rocuronium injection and 95% depression of first twitch (T1) response was noted as “onset time”. As soon as onset time was defined, all patients were intubated. All patients were mechanically ventilated with a tidal volume of 7 ml/kg and frequency of 12/min. In order to achieve the goal of maintenance of desired end-tidal carbon dioxide level (between 35 and 45 mmHg), firstly tidal volume was increased by 20% and secondly frequency of mandatory respirations was increased to 16/min.
During the maintenance period of anesthesia the remifentanil effect-site concentration was adapted by step of 2.5 ng/ml according to the hemodynamic parameters in every 5 min. In case of bradycardia and hypotension, atropine 0.5 mg and ephedrine 10 mg iv were injected, respectively. Meanwhile, propofol effect-site concentration was adjusted to intend intraoperative BIS value of 40 to 60. If BIS value was lower than 40, propofol effect-site concentration had been lowered by 0.5 µg/ml. On the contrary, propofol effect-site concentration had been increased by 0.5 µg/ml if BIS value was higher than 60. The anesthetic management was schematized in Figure 1. During the anesthesia maintenance, the time elapsing between TOF count 0 and first twitch reappearance was noted as “deep neuromuscular block duration”. Moreover, the time elapsing between administration of rocuronium and recovery to 10 and 25% of first twitch height (T1 10%, T1 25%) were recorded as “the time to T1 10% and clinical duration”, respectively. When “clinical duration” was achieved, if necessary, additional rocuronium in a dose of 0.15 mg/kg iv was administered and the time between the injection of rocuronium and the second recovery to 25% of first twitch height was recorded as “second clinical duration”. If an additional rocuronium was not necessary due to the end of surgery, 30 μg/kg neostigmine and 10 μg/kg atropine were administered for the recovery of neuromuscular blockade. Along the recovery period, the time from 25 to 75% of first twitch height recovery was recorded as “recovery index” and the time between T1 25% and TOF ratio of 90% was also recorded as “complete recovery interval”. If the TOF ratio was above 80 and the BIS level was above 70, the patients were then extubated.
All patients were followed in terms of their peripheral temperatures and BIS levels and all these parameters were recorded. In addition to the duration of anesthesia and surgery, the total and hourly propofol, remifentanil and rocuronium consumptions were also noted.
Statistical analysis
The statistical analyses were made by using SPSS 12.0 program (Statistical Program for Social Sciences, Chicago, IL, USA) for Windows with a personal computer. The numeric data were analyzed by the t-test and presented as mean ± SD. Chi-square test was used for the evaluation of categorical variables; correlation analysis was used to determine the relationship between the variables. In comparison of 3 or more groups, Kruskall-Wallis, a non-parametric test was used, in comparison of 2 groups Mann-Whitney U test was used. No power analysis was done. For statistical comparisons, p <0.05 were considered as significant.
RESULTS
Forty patients were enrolled into the study. None of them were excluded due to any reason. No significant difference was found between groups in terms of patient demographics provided in Table 1. Intraoperative hemodynamic parameters were similar between groups and no hemodynamic adverse effect was found. The onset time of rocuronium did not differ between 4 groups with a mean (SD) of 2.65 (1.0) min. Similarly, there was no difference related to the deep neuromuscular blockade duration of rocuronium among groups (Table 2). In contrast, there was a clear relationship between the administration time of rocuronium and the estimates of time to T1 10% and clinical duration of rocuronium. The time to T1 10% was significantly shorter in Group N (24.4 ± 8.0 min, mean ± SD) when compared with Group AN (32.1 ± 8.6 min, mean ± SD) and Group E (32.5 ± 9.9 min, mean ± SD) (p < 0.05). The shortening in T1 10% observed in Group N was 24 and 24.9% compared with Group AN and Group E, respectively.
There was no difference between Group M, Group AN and Group E in terms of time to T1 10%. The time to T1 10% did not differ between Group M and Group N. When the clinical duration of rocuronium was compared between 4 groups, it was found that clinical duration was shorter in Group N (28.5 ± 9.0 min, mean ± SD) when compared with Group AN (36.7 ± 9.1 min, mean ± SD) and Group E (37.0 ± 11.4 min, mean ± SD) (p < 0.05). The longest and the shortest clinical durations were noted in Group AN with a 61.4 min and in Group N with a 20.5 min, respectively. The shortening in clinical duration observed in Group N was 22.3 and 22.9% compared with Group AN and Group E, respectively. There was no difference between Group M, Group AN and Group E in terms of clinical duration. There was also no difference in clinical duration between Group M and Group N. These findings were listed in Table 2.
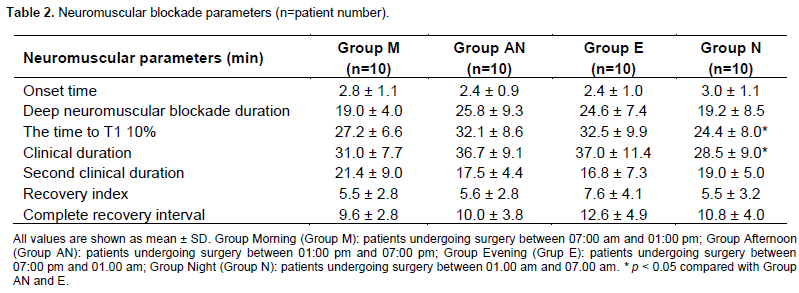
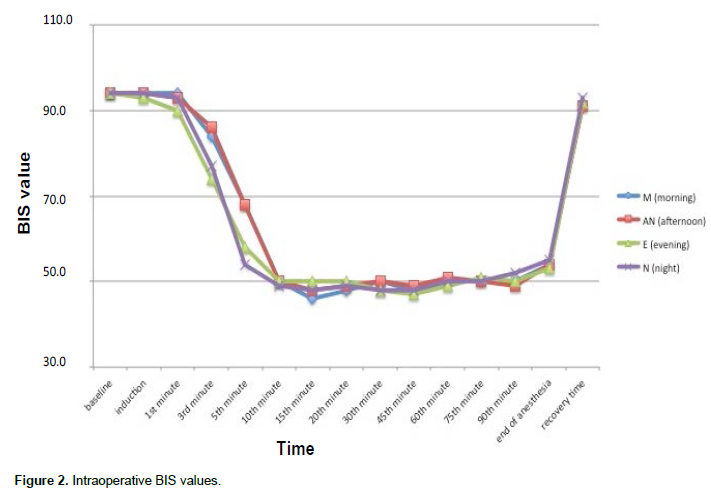
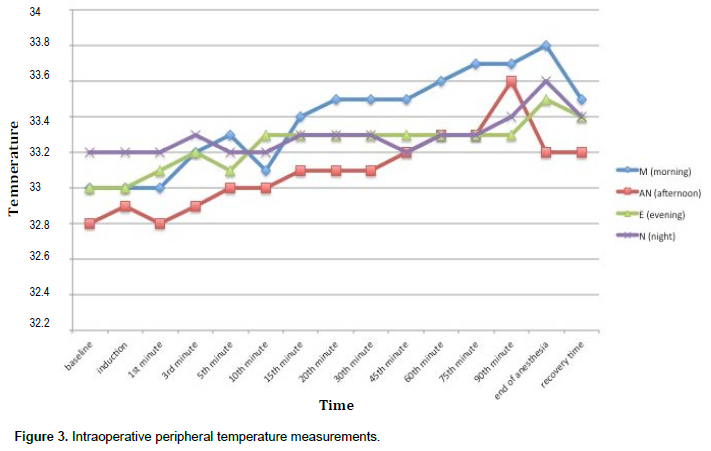
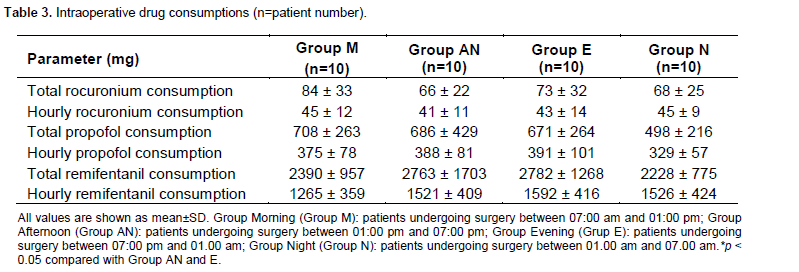
Although the second clinical duration was shorter in Group N compared with Group M, this was not statistically significant. The recovery index and complete recovery interval did not differ at any time throughout the day between groups (Table 2). The BIS levels and peripheral temperature measurements were similar between the groups (Figures 2 and 3). There was no statistically significant difference between four groups in terms of intraoperative total and hourly propofol, remifentanil and rocuronium consumptions (Table 3).
DISCUSSION
This is the first human study investigating the effects of the rocuronium administration time on the neuromuscular blockade characteristics during the 24 h. The primary finding of our study was that, T1 10% time and clinical duration of rocuronium were significantly shorter at night compared to afternoon and evening part of the day under total intravenous anesthesia with propofol and remifentanil. The onset time of rocuronium is approximately 1.5 to 1.7 min considering its pharmacodynamic properties (Naguib and Lien, 2009). However, the onset time was found longer in our study (mean, 2.65 min).
Na and coworkers demonstrated that the prior administration of remifentanil during TCI propofol and remifentanil anesthesia prolonged the onset time of rocuronium due to decreased cardiac output in their well-designed study (Na et al., 2012). This may also explain our prolonged onset time due to our comparable sequence of anesthesia induction. Nevertheless, there was no difference in terms of onset time or deep neuromuscular blockade of rocuronium between the 4 study groups.
There was a clear relationship between the dosing time of rocuronium and the time to T1 10%, and clinical duration. The time to T1 10% and clinical duration were shorter at night compared with afternoon and evening application. These findings were not consistent with the study data previously published.
Cheeseman et al. (2007) demonstrated that the minimum duration of action of rocuronium dosing of 0.6 mg/kg was between 14:00 and 17:00 corresponding to the timing of our Group AN. There was an important difference in study design between these two studies. Unlike from our study, there was no patient enrollment in the night period of a day due to some anticipated difficulties. Therefore, the authors could not conclude on the clinical duration of rocuronium during the resting period of participants.
The clinical duration of a neuromuscular blocker indicates that the duration of neuromuscular blocker action becomes terminated, as it has been mostly metabolized in human body. In practice, if the clinical duration of a neuromuscular blocker has been achieved, anesthesiologist should give either an additional neuromuscular blocker or a reversal agent of neuromuscular blocker according to the circumstances (that is, ongoing or ending surgery). Therefore, quantifying these parameters is very important to decide what should be done in the course of a surgical anesthesia.
The mechanism underlying this chrono-pharmacological aspect of rocuronium may be attributed to its metabolism pathway. A large portion of circulating rocuronium is taken by the liver, metabolized and then excreted into the bile. Lemmer and Nold (1991) found significant circadian differences in estimated hepatic blood flow (EHBF) measured by injection of indocyanine green during the different part of the day in healty male volunteers. In this study, the peak EHBF was reached at 04:00 am. They also showed no difference in the distribution volume. Likewise, in another study investigating the oxaliplatin pharmacokinetics and chronopharmacological aspects, the hepatic blood flow was found maximum between 02:00 am and 08:00 am, and minimum at 02:00 pm within a day (Levi et al., 2000). Therefore, we may speculate that the clinical duration of rocuronium appears to be shorter with bedtime compared with AN or E administration.
There was an absence of statistical significance in terms of second clinical duration between four groups. The additional rocuronium dosage was 0.15 mg/kg. Therefore, this finding can be explained by application error in smaller drug doses rather than the hepatic blood flow differences. There were no difference regarding recovery index and complete recovery interval between groups. There are a number of limitations in this study. Probably, the most important one is the formation of four different groups instead of two study groups. This would be more appropriate for investigations on circadian rhythms. The number of patients were not determined using a power analysis statistically. In addition to this, this study was not sufficient to establish the real mechanism related to diurnal variation of clinical duration of rocuronium.
Future clinical trials assessing the blood rocuronium levels or rocuronium and receptor interactions are needed to clarify this issue. Additionally, the effect of the diurnal changes associated with elective or emergency was another potential confounding factor in the study design. This effect was underestimated in this study.
CONCLUSION
This study demonstrated that the clinical duration of rocuronium became shorter at night compared with the noon and evening part of the day under propofol and remifentanil anesthesia. Although the effect of this shortening on clinical practice looks like limited, it could be more significant as enough data about the diurnal changes related with rocuronium are provided in the future.
ACKNOWLEDGEMENTS
This study demonstrated that the clinical duration of rocuronium became shorter at night compared with the noon and evening part of the day under propofol and remifentanil anesthesia. Although the effect of this shortening on clinical practice looks like limited, it could be more significant as enough data about the diurnal changes related with rocuronium are provided in the future.
CONFLICT OF INTEREST
There is no conflict of interest as regard this study.
REFERENCES
|
Chassard D, Bruguerolle B (2004). Chronobiology and Anesthesia. Anesthesiology. 100: 413-427. crossref |
||||
|
Chassard D, Allaouchiche B, Boselli E (2005). Time is everything: the pendulum swings on. Anesthesiology 103:454-456. crossref |
||||
|
Chassard D, Duflo F, de Queiroz Siqueira M, Allaouchiche B, Boselli E (2007). Chronobiology and anaesthesia. Curr. Opin. Anaesthesiol. 20:186-190. crossref |
||||
|
Cheeseman JF, Merry AF, Pawley M, de Souza RL, Warman GR (2007). The effect of time of day on the duration of neuromuscular blockade elicited by rocuronium. Anaesthesia. 62:1114-1120. crossref |
||||
|
Baykara N, Woelfel S, Fine GF, Solak M, Toker K, Brandom BW (2002). Predicting recovery from deep neuromuscular block by rocuronium in children and adults. J. Clin. Anesth. 14:214-217. crossref |
||||
|
Leykin Y, Pellis T, Lucca M, Lomangino G, Marzano B, Gullo A (2004). The pharmacodynamics effects of rocuronium when dosed according to real body weight or ideal body weight in morbidly obese patients. Anesth. Analg. 99:1086-1089. crossref |
||||
| Beaufort AM, Wierda JM, Belopavlovic M, Nederveen PJ, Kleef UW, Agoston S (1995). The influence of hypothermia (surface cooling) on the time-course of action and on the pharmacokinetics of rocuronium in humans. Eur. J. Anaesthesiol. 11:S95-106. | ||||
|
Maidatsi PG, Zaralidou AT, Gorgias NK, Amaniti EN, Karakoulas KA, Giala MM (2004). Rocuronium duration of action under sevoflurane, desflurane or propofol anaesthesia. Eur. J. Anaesthesiol. 21:781-786. crossref |
||||
|
Fuchs-Buder T, Claudius C, Skovgaard T, Eriksson I, Mirakhur RK, Viby-Mogensen J (2007). Good clinical research practice in pharmacodynamic studies of neuromuscular blocking agents II: the Stockholm revision. Acta. Anaesthesiol. Scand. 51:789-808. crossref |
||||
|
Schnider TW, Minto CF, Gambus PL, Andresen C, Goodale DB, Shafer SL, Youngs EJ (1998). The influence of method of administration and covariates on the pharmaco- kinetics of propofol in adult volunteers. Anesthesiology. 88:1170-1182. crossref |
||||
|
Minto CF, Schnider TW, Shafer SL (1997). Pharmacokinetics and pharmacodynamics of remifentanil. II. Model application. Anesthesiology 86:24-33. crossref |
||||
| Naguib M, Lien CA (2009). Pharmacology of muscle relaxants and their antagonists. In: Miller's Anesthesia, ed: Miller R. 859-911. | ||||
|
Na HS, Hwang JW, Park SH, Oh AY, Park HP, Jeon YT, Do SH (2012). Drug-administration sequence of target-controlled propofol and remifentanil influences the onset of rocuronium. A double-blind, randomized trial. Acta. Anaesthesiol. Scand. 56:558-564. crossref |
||||
|
Lemmer B, Nold G (1991). Circadian changes in estimated hepatic blood flow in healty subjects. Br. J. Clin. Pharm. 32:627-629. crossref |
||||
|
Levi F, Metzger G, Massari C, Milano G (2000). Oxaliplatin pharmacokinetics and chronopharmacological aspects. Clin. Pharmacokinet. 38:1-21. Pubmed |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


