Full Length Research Paper
ABSTRACT
To some Cannabis is antisocial anathema, to others it is a harmless sedative-hypnotic, or narcotic analgesic and to others it occupies a cultural position as religious sacrament. Some fear its use leads to psychosis and addiction; to others still it is a legal anomaly and should be decriminalized. Whatever the case may be, in Africa where Cannabis is a recreational drug. It is caught in a bizarrely legal and regulatory maze. Regulations are changing internationally and the Cannabis industry is growing. African, National Medicines Regulatory Authorities, NMRs, have to catch up. But unfortunately some lack competent professionals who require to understand regulatory science, RS, in general, and in particular as it pertains to cannabis products with complex pharmacology. RS is “a range of scientific disciplines that are applied - intellectually and practically - to the quality, safety and efficacy assessment of medical products and that inform regulatory decision making, throughout the life cycle of a medical/health product”. RS helps to answer the following questions: Is there a pathway that will lead cannabis to mainstream medicine in Africa? Will cannabis as a botanical agent have to follow the same time-honoured process that any pharmaceutical must attain to receive regulatory approval? There is no doubt the cannabis and regulatory sciences are going to influence the future shaping and implementation of pharmaceutical medicine laws and regulations in Africa. The aim of the article is to highlight the key regulatory science challenges, in Africa, that belong to either a societal or a biomedical sphere regarding Cannabis for adult use or medicinal purposes or nutrition.
Key words: Cannabis, regulatory science, challenges, Africa.
INTRODUCTION
In the United States, cannabis was widely utilized as a patent medicine during the 19th and early 20th century, described in the United States Pharmacopeia for the first time in 1850. It was dropped from the pharmacopeia in 1937 with legal penalties for possession increasing until recently. This was the time when Marihuana (Cannabis) Tax Act was being aggressively applied in the USA (Bridgeman and Abazia, 2017). Dr James Munch, a pharmacologist and special adviser to the US, Federal Bureau of Narcotics at one court hearing made the following remark: ‘After two puffs on a marijuana cigarette I was turned into a bat’. Dr Munch had tried cannabis on himself for scientific reasons, a form of auto-experimentation (Booth, 2003). Beyond criminilization, legislation in the US which was then adopted by the United Nations then contributed to creating limitations on research by restricting procurement of cannabis for academic purposes. As a result in Africa, there is currently no meaningful research on cannabis.
In many African countries, administering marihuanna by smoking is antisocial anathema as it is regarded as one of the factors that increases drug abuse liability, DAL. To others it is a harmless way of using a psychoative plant with sedative properties, to relax – recreational cannabis - or provides pain relief in cancer as a narcotic analgesic (medicinal cannabis) or used for religious purposes (sacramental cannabis). Some fear cannabis (marijuana – marihuana) that, it leads to psychosis referred to ‘reefer madness’ and addiction and to others in Africa, it still is a legal anomaly and should be decriminalized. Whatever, the viewpoint cannabis incites debate at every level anywhere in the world. The word cannabis conjures up all sorts of ideas in the minds some politicians, pharmacists, pharmacologists, those working in applied therapeutics and botanists who have particular interest in toxonomy of the plant.
CANNABIS TAXONOMY DEBATE
Cannabis taxonomy debate has been raging for 250 years because all Cannabis types are said to be eminently capable of cross-breeding to fertile progeny (Russo, 2019). In literature, it can be seen that the Cannabis species controversy, Cannabis sativa vs Cannabis indica vs afghanica has continued with impassioned arguments by protagonists (Clarke and Merlin, 2016; Small, 2015; McPartland and Guy, 2017). According to Piomelli and Russo (2015) it would appear that the debate is irreconcilable and that it would be more useful to rather emphasize the biochemical and pharmacological distinctions. In addition, some feel that to describe varieties of cannabis as “strains” is not appropriate as this applies only to bacteria and viruses and not to plants. And so, with Cannabis the most appropriate appellation would be “chemovar” and not “cultivar” (Lewis et al., 2018). Going forward, the aforementioned issues are going to pose most basic regulatory problems with the use of cannabis products on the African market, in particular. For example, a single product can be classified as a food product by some producers and a dietary supplement by others. Such a product, for example hemp oil, therefore, may have concurrent regulations depending on how it is classified. Unfortunately, National Medicines Regulatory Authorities, NMRSs, currently, in Africa lack competent professionals to carry out proper classification (Ncube, 2021). They need to fully understand regulatory science, RS, in general, and regulatory science as it pertains to cannabis products such as cannabidiol, CBD, an archetypical “dirty” drug with many myths and misconceptions, and a complex pharmacology.
REGULATORY SCIENCE DEFINITION
For the purpose of this article the definition of RS, is derived from a combination of European Medicines Agency, EMA (2011) and Institute of Medicine (2012) definitions. It is “a range of scientific disciplines that are applied - intellectually and practically - to the quality, safety and efficacy assessment of medical products and that inform regulatory decision making, throughout the life cycle of a medical/health product. It encompasses basic and applied medicinal science and social sciences through observation and experiment to contribute to the development of regulatory standards and tools, and to systematically study the structure and behaviour of the regulatory world”. A short and simplistic definition could be ‘RS consists of the application of science to support regulatory activity, particular setting of regulatory objectives’ (Johner, 2020).
Therefore, effective application of RS would require the use of real-world data, RWD to generate real-world evidence, RWE. In other words, any regulatory authority shall need to be supplied with extensive data available on all aspects of the manufacturing, and on the pre-clinical and clinical behaviour of the drug. The technical framework for providing such information by a manufacturer is defined in the International Council for Harmonization, ICH guidelines. Thus, any manufacturer of a cannabis product intended, for example, for prescription use, after approval by a regulatory authority, knows more or less exactly what they need to do. Globally, in different jurisdictions the debate about the manufacture and use of botanical medicines from Cannabis continues.
CANNABIS LEGISLATION AND COMMERCIALIZATION IN AFRICA
It is important for NMRs in Africa to appreciate how RS principle can be applied legislation and commercialization of cannabis has been and continues to be on the forefront of public debate and top of the agenda for policy makers globally. The United Nations Commission on Narcotic Drugs (CND) on 02 December 2020 accepted a World Health Organization recommendation to remove cannabis and cannabis from Schedule IV of the 1961 Single Convention on Narcotic Drugs. The historic vote, in spite of a slim majority in Vienna has a far-reaching implication for global medical cannabis industry from regulatory oversight to scientific research into the plant and its use as a medicine. The following African countries some of which have weak NMRs voted against the recommendation, Algeria, Angola, Burkina Faso, Egypt, Ivory Coast, Kenya, Nigeria and Togo. The passage of Recommendation 5.1 carried broad symbolic significance for medical cannabis. It is, therefore, important for the AU, as whole, to understand the import of cannabis rescheduling that eventually took place in Vienna. The AU at large has to be actively engaged in line with the Plan of Action on Drug Control and Crime Prevention (2019 - 2023) (Putri, 2020).
The passage of the recommendation is expected to help boost medical cannabis legislation efforts around the globe now that the CND tacitly acknowledge the medical utility of the natural products from it. Since the vote, many countries in Africa are seeing potential gold in cannabis which has been legalized or at least decriminalized in the parts of US, Canada, and Europe, with sales booming during Covid-19 pandemic (Kahn, 2021). Today Ghana, Kenya, Lesotho, Rwanda and the Democratic Republic of Congo are among African countries that have taken steps to encourage cannabis farming as a legal cash crop. Africa’s cannabis business has been reported that it could be worth as much as $7.1 billion by 2023. Many companies are flocking to the continent in the hope of cashing in by investing in cannabis cultivation in various parts (Prohibition Partners, 2019). In Africa RS still has to put the necessary regulations into a scientific framework. This should not be understood as if regulatory affairs, which African Medicines Agency, AMA, has been set up to harmonize, are less scientific. There, however, are needs-driven talent and competency development for the next generation of regulatory scientists in Arfica (Semete-Makokotlela et al., 2022). Renewed interest in Cannabis, a botanical agent provides a stepping stone into ever expanding field of regulatory sciences.
The present article attempts to highlight the key regulatory science challenges that belong to either a societal or a biomedical sphere, Cannabis for adult use or medicinal purposes or nutrition will face in Africa. In other words, the regulatory framework in Africa should, at least for now, apply to all products that contain cannabinoids and all other metabolites obtained from the Cannabis plant. The article proposes ways to address the challenges and suggests solutions based on currently available literature.
GENERAL FEATURES OF REGULATORY SCIENCE
According to Bauschke (2010), at least in the European Union, there seems to be a large number of distinct definitions of regulation. In his review of previous theory of regulation, he opines that defining regulation, is a complex task. He, however, proposes that a broad definition that seems to be appropriate for the regulation of botanical pharmaceuticals such as CBD would be the one that states that “regulation occurs when the state constrains private activity in order to promote public interest” (Francis, 1993). In the case of pharmaceuticals, therefore, the main component of the regulation can be characterized as safety regulation in the interest of public health. It is important, however, to note that the regulation is not confined to pharmaceutical safety but also to regulatory economics. This is based on the peculiar character of pharmaceutical supply and demand and therefore there has to be numerous economic decisions, in the regulatory decision-making process.
The origin of the term ‘regulatory science’ is unknown. One source suggests that it was coined in the 1970s when the newly established US Environmental Protection Agency (EPA) was forced to make decisions based on incomplete and non-existing scientific information such as agrochemicals (Callréus and Schneider, 2013). This does not apply to the authorization of pharmaceutical products which have three distinct components in the regulatory decision-making process. To start with, during drug development a company is expected to produce a well-defined set of data on the quality, safety and efficacy of the medicinal product, such as a CBD product. This information is then submitted to the regulator for assessment which will lead to a dialogue between the regulator and the company. This is what regulatory science is all about and is intimately linked to the ‘precautionary principle’ whose key element is the justification for acting in the face of uncertain knowledge (Callréus, 2005).
It can be argued, for CBD, for example, that the scope of regulatory science, RS, is that laws, regulations and judiciary decisions should incorporate (i) scientific and (ii) non-scientific components. In essence, ‘regulatory science’ if well applied can provide an insight into the changing conditions of scientific practice, and especially the operation of science within the area of, for example, cannabis industry-government-academic relations which continues to be pressured by need to make potentially far-reaching decisions (in terms of both public health and economic costs) on regular basis.
EARLY THERAPEUTIC USE OF CANNABIS AND REGULATORY SCIENCE
In the second half of the eighteenth century, cannabis started to appear in dispensaries, textbooks referred to by pharmacists and physicians in much the same way The British National Formulary, BNF or the US National Library of Medicine MEDLINE website. The first recorded of extract of hashish (usually made from resin or resin glands of the female plant) in alcohol patented as Squire’s Extract, authorized for marketing as an analgesic, was made in 1842 and made under licence in America as Tilden’s Extract. This followed several pre-clinical experiments in dogs that had been carried out by William Brooke O’Shaughnessy in India where he had realized the therapeutic potential for hashish. This was based on information he had obtained from native doctors and scholars in the sub-continent (Booth, 2003). This is arguably the early application RS in relation to the Cannabis plant. After O’Shaunhnessy’s work on Cannabis indica was published, the American Provers’ Union, a group that aimed to attain medical knowledge through first-hand experience produced a book on auto-experiments with the plant (American Provers’ Union, 1859). The first traces of therapeutic use of cannabis are reported in the 1800s when for example, Sir John Russell Reynolds, a doctor of the UK Royal House used to prescribe to Queen Victoria doses of cannabis to treat her strong pains and menstrual cramps. In 1889, the Lancet carried an article by Dr EB Birch which outlined the application of cannabis for the treatment of opium and chloral hydrate withdrawal symptoms. The mixture was said to reduce the opium craving and acted as an anti-emetic (Birch, 1889). Dixon (1899) reported in the British Medical Journal that new preparations of hemp used at the time were safe.
It seems that at the time initially, there appeared to be no issues regarding composition or consistency of the product used in spite of a wide range of cannabis medicines. As time went on there were fundamental problems with doses used because it became impossible to judge an exact dosage. The strength of the medicines could vary greatly, even from bottle to bottle of the same brand due to difficulties encountered when processing the cannabis used in them. The only route of administration at the time was oral because of cannabis insolubility in water. In addition, the preparations were unstable in the sense that they tended to separate out with cannabis forming a residue at the bottom of the bottle. As a result, if the bottle was not shaken vigorously the patient receiving the last inch or so of the contents of the container tended to be heavily overdosed. Some practitioners began to titrate, regulatory tool still used even today, the cannabis solution before using it to determine its strength. The overdosing prevalence led to reports being published in medical journals (Booth, 2003), a form of pharmacovigilance put in place. Pharmacists in Britain and America became aware of the cannabis drawbacks being reported and so increased their interest in trying to identify the active principle in the plant extract by using different methods. As a result, there were a number of chemical entities extracted and identified. With these discoveries, the stage was set for pharmaceutical industry to assay accurately, thereby quality assuring any synthetic drug, creating massive advances in chemistry. New drugs such as acetylsalicylic acid whose trade name was aspirin, a minor analgesic was introduced. Physicians and dispensing chemists who became more professional were aware of the new synthetics and started to use only quality-controlled substances even though cannabis was still a licensed medicine (Nutt et al., 2020).
In spite of the data that was available on the safety and usefulness of cannabis at that time, it had had its medical day. In fact, earlier when scientists in the US sought seriously to study cannabis, they began to be hounded and harassed. Both the UN and the US began to apply pressure on cannabis producer countries to change their agricultural and production practices (Booth, 2003).
It can be argued that in the 18th century, to an extent, the principles of what is now being touted as RS were being applied for therapeutic use of cannabis. RS, to an extent has now emerged and being promoted as separate discipline at a time when there so much interest in the cannabis plant and its products. It is important to differentiate regulatory science from ‘regulatory affairs’ of cannabis which now focus on complying with the regulations that have been put in place. Different African regional jurisdictions appear to have different inter and intra cannabis regulations.
REGULATORY SCIENCE VERSUS REGULATORY AFFAIRS
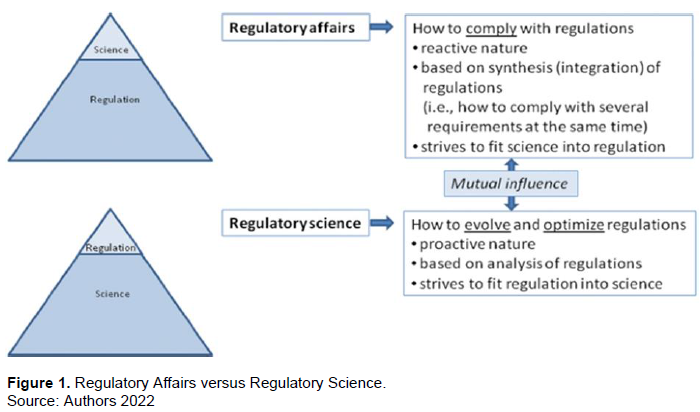
‘Regulatory affairs’ (RA) usually means the application of already defined regulatory principles to a given drug development or drug life cycle in a reactive manner, while ‘regulatory science’, proactively analyses regulatory principles and strives to evolve them along the continuity of scientific progress. Regulatory affairs are often the starting point for regulatory science when it comes to identifying gaps and areas where further optimization is needed or new regulatory principles have to be formulated. RA deals with making sure the wording and publication of regulations (laws, ordinances, guidelines) is legally watertight; how these regulations are monitored (e.g. audited) and enforced; which documents manufacturers have to provide and in what form, Callréus and Schneider (2013) came up with an excellent representation as shown in Figure 1. All the figure is saying is that the scientific evaluation of the logic and effectiveness of the regulations is not part of RA. All this means that any cannabis product to be developed for medical use shall encounter many public health regulatory controls by at least two ministries in Africa. This is so because cannabis is a controlled substance with a potential to be abused. This was the case with Marinol (Dronabinol, tetrahydrocannabinol) THC in sesame oil and to be taken orally when in 1985 the FDA (Health) and DEA (Justice) allowed it to be developed for nausea and vomiting associated with cancer chemotherapy. Hence, the need to understand the difference between RA and RS.
Once the difference is well understood by regulatory authorities in Africa, there are a number of questions that regulatory science regarding the cannabis plant has to address. These include. Is there a pathway that will lead cannabis to mainstream medicine? Will cannabis have to follow the same time-honoured process that any pharmaceutical must attain to receive regulatory approval: biochemical uniformity and stability along with safety and efficacy as proven by randomized clinical trials (RCT)? Can a botanical agent become a prescription medicine? The regulatory hurdles paused by these questions are however, surmountable but would require serious considerations in those African countries that have recently legalized cannabis. The AMA can at least borrow a leaf from what the US FDA (2016) has done about the development of botanical medicines such as the extracts of Camellia sinensis (green tea) and Croton lechleri.
REGULATORY SCIENCE HURDLES
In many African countries medicines regulatory ecosystem is very poor, unlike in Canada, The European Union and some states in America, where cannabis use has been legalized. Amongst low- and middle-income countries worldwide, the African region has the highest prevalence of poor-quality medicines with an 18.7% prevalence of substandard and falsified medicines (Ncube et al., 2021). Entry of a botanical medicine such cannabinoids on the African market is going to pause serious challenges. Currently most African countries will have to rely on decisions made by established stringent regulatory authorities such as the FDA or EMA. This is not sustainable and in addition, not all results from USA or Europe can be transferable to all African countries. Unfortunately in Africa mutual recognition, based on treaties or equivalent agreements is less practiced (Samete-Makokotela, 2022). Real world evidence on cannabinoids has to be generated from real world data obtained on the African soil.
AGRONOMICAL CHALLENGE
The biochemical variability of one chemovar to another is going to be an agronomical challenge for outdoor cultivation given the enormous capital outlay that is involved in indoor cultivation. Good agricultural practice (GAP), where they exist, will have to be adhered in order to avoid harbouring of pesticides residues, molds, bacteria and heavy metals that endanger public health.
No matter where cannabis is grown, virtually no health and safety standards have existed for growing it (Deardorff and Wadworth, 2017). According to the UK Hodges report on Cannabis, it is only Canada and Australia who now appear to have these standards in place (Hodges et al., 2022).
ROUTE OF ADMINISTRATION CHALLENGE
Cannabis for recreational purposes usual delivery system is smoking which pauses similar risks in addition to chronic cough, phlegm production, bronchitis, and inhalation of pyrolytic by-products which are many in the plant (Tashkin, 2017; Tashkin and Roth, 2020). It was established that cannabis inhalation whether by smoking or vaporizer produce a rapid peak serum and brain concentrations that maximize intoxication and possible reinforcement that are risk facts for drug abuse liability (DAL) (Schoedel et al., 2011).
Other routes of administering cannabinoids, e.g., trans dermal patches and rectal suppositories have not demonstrated practicality in later stage clinical trials (Huestis, 2007). It evident just from the two early studies that regulation of cannabis extracts as a botanical pharmaceutical is going to be faced with several challenges. A number of studies are under way in Australia, Europe, South America and USA to answer some of the questions as Cannabis legislation continues to be reviewed in the countries (Prohibition Partners, 2022). For example, in Switzerland cannabis will so go on sale as part of the study into regulation (Europenews, 2022).
REGULATORY SCIENCE: SOCIETAL AND BIOMEDICAL FACTORS
The challenges that cannabis, as botanical medicine can broadly be seen as belonging to either a societal (factors not related to biomedical science) or a biomedical (factors related to biomedical science) sphere. As to the first sphere, considering that there has been and still is debate about legalization of cannabis, ensuring that a medicines regulatory authority, MRA, is perceived as trustworthy in the eyes of various stakeholders, is a condition for its proper functioning. The operations of the MRA must be transparent alongside communication of its inherent limitations of its role and tools. The MRA needs to be aware of the fact that globalization of development, manufacturing and marketing of cannabis-based products is an important transformational factor in both pharmaceutical, food and nutrition industries. This is much so with the burgeoning cannabis industry.
Regarding the biomedical sphere, MRAs in Africa, should be aware of the progress in several areas regarding cannabis and its products. They are likely going to shape regulatory frameworks and their implementation. For example, there are new ways of classifying diseases based on their underlying molecular mechanisms which have to be taken into consideration when a botanical medicine such as cannabis is going to be used. Individualization of medicine prescription which had somewhat taken a back seat in medicine has now come back in the form of a model called ‘personalized medicine’ or ‘precision medicine’, for example, in the treatment of brain pathology (Reddy et al., 2020). In addition to personalized medicine, evidentiary standards need to be developed for cannabis botanical raw material before it becomes a medicine after it is processed through extraction, mixing, excipient addition, formulation and packaging that is defined, exacting and precise. The resultant botanical medicinal product must be examined for it pharmacokinetic and pharmacodynamic properties in addition to possible contamination by pesticides, heavy metals, bacteria and fungi. Any systematic or meta-analysis for all relevant medical indications, must therefore, be based on the pharmacology of the resultant botanical medicinal product (Bilbao and Spangal, 2022).
With more interest being shown in cannabis, MRAs in Africa will have to open up to new innovative clinical trial designs such as adaptive design clinical trials of which there are several types (FDA, 2019). In Europe the first approval of Sativex, nabiximol a specific Cannabis extract, was based on an adaptive design study. Regulatory scientists working with MRAs in Africa would need to pay particular attention to the issues of validity and integrity which are of primary concern associated with adaptive designs. Thus, several regulatory concerns exist. These include acceptable level of adaptation; established standards for reveiew and approval process of clinical data and whether the adapted clinical trial still addresses the objectives of the originally planned clinical trial (Mahajan and Gupta, 2010).
In response to regulatory science challenges of the future several initiatives are underway, though slowly. In January 2006, the African Union (AU) Model Law on Medical Products Regulation was officially endorsed. This model law was developed and promoted by the New Partnership for Africa’s Development (NEPAD) Agency to encourage regional and sub-regional regulatory systems harmonisation. The idea being that in countries involved in, for example, research and development of cannabis products and cannabis-based medicines that hold promise, are developed, tested, and scaled up for the improvement of health impact in Africa. The aim of the African Medicines Regulatory Harmonisation (AMRH) formalized in 2009, is to create more effective, efficient and transparent regulatory mechanisms, through collaborative regional mechanisms that, among others, achieve faster medical products approvals. The initiative also includes strengthening research activities in regulatory science and capacity building (Ncube et al., 2021). It challenges academic world in Africa to set up programmes aimed at relevant research and teaching regulatory science (SAHPRA, 2020). In the case of cannabis regulatory science, this can be done through a collaborative effort between universities, burgeoning cannabis industry in Africa and Regional Centres of Regulatory Excellence (RCORES). For example in the UK, King’s College, London in collaboration with industry launched a Cannabis & Me scientific study into the effects of cannabis and mental health (Sabaghi, 2022).
CONCLUSION
There is no doubt the cannabis and regulatory science are going to influence the future shaping and implementation of pharmaceutical laws and regulations in Africa. It is anticipated because of cannabis, the role of regulators in Africa, will be more active and change from that of only being a gatekeeper to also being an enabler of progress in cannabis therapeutics, among other uses of cannabis. It is hoped that regulatory science in pharmaceutical medicine, in general and cannabis therapeutics in particular, will highlight not so much how medicines are regulated in Africa but why and how best it is done. This will help even in the development of African traditional remedies acceptance in the mainstream medical practice as is the case of Kampo medicine in Japan (Moschick et al., 2012). In Africa, there is also need to carry out research on environmental and biological factors behind the different effects of cannabis consumption on human brain to provide information to African physicians to prescribe cannabis safely. In addition, cannabis long stigmatized for its illicit use, now needs African regulatory scientists to look at how legal cannabis affects consumption and health among users. Cannabis based medicines are relatively new and promising therapy clinical trials need to be undertaken to understand how to demonstrate their efficacy and safety in different conditions (Martin et al., 2020). This should be based on their specific pharmacology to be considered by well-grounded African regulatory scientists. Training of regulatory scientists in Africa is going to require inputs for local industry, local academia and African RMAs.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
American Provers ((1859)). Union Provings of Cannabis Indica. Forgotten books (Classic Reprint). The American Provers' Union. FB & C Limited, London, UK |
|
|
Bauschke R (2010). Defining regulation: review of previous theory. The effectiveness of European regulatory governance: the case of pharmaceutical regulation. Heidelberg: Ruprecht-Karls-Universität Heildelberg,Thesis pp. 58-60. |
|
|
Bilbao A, Spangal R (2022). Medical cannabinoids: a pharmacology=based systematic review and meta-analysis for all relevant medical indications. BMC Medicine 20:259. |
|
|
Birch BE (1889). The use of Indian hemp in the treatment of chronic chloral and chronic opium poisoning. The Lancet 133(3422):625. Originally published as 1 (3422) |
|
|
Booth M (2003). Cannabis, a history. New York: Picador p 134:351-331 |
|
|
Bridgeman MB, Abazia DT (2017). Medicinal cannabis: History, Pharmacology, and Implications for the Acute Care Setting. Journal of Pharmacy and Therapeutics 42(3):180-188. |
|
|
Callréus T (2005). The precautionary principle and pharmaceutical risk management. Drug Safety 28(6):465-471. |
|
|
Callréus T, Schneider CK (2013). The emergence of regulatory science in pharmaceutical medicine. Journal of Pharmaceutical Medicine 27:345-351. |
|
|
Clarke RC, Merlin MD (2016). Cannabis domestication, breeding history, present-day genetic diversity, future prospects. Critical Review in Plant Science 35:293-327. |
|
|
Deardorff D, Wadsworth K (2017). What's wrong with my marijuana plant. A Cannabis grower's visual guide to easy diagnosis and organic remedies. Ten Speed press, California. New York. p. 2. |
|
|
Dixon WE (1899) The action of some new preparations from Cannabis Indica. British Medical Journal 2:1517. |
|
|
European Medicines Agency (2011) Road Map to 2015 [online]. |
|
|
Europenews (2022). Cannabis has gone on sale in Switzerland as part of study into regulation. |
|
|
Food and Drug Administration (FDA) (2019) Adaptive designs for clinical trials for drugs and biologics. |
|
|
Francis JG (1993). Introduction: The politics of regulation: a comparative perspective. Oxford: Blackwell pp. 1-5 |
|
|
Hodges C., Bhatarah P, Gibbs B (2022). The Hodges Review: From containment to nurturing. Hodgesreview.com |
|
|
Huestis MA (2007) Human cannabinoid pharmacokinetics. Chemistry and Biodiversity 4:1770-1804. |
|
|
Johner C (2020) Regulatory Science: Europe is Flying Blind. |
|
|
Institute of Medicine (2012) Strengthening a workforce for innovative regulatory science in therapeutics development: Workshop summary. Washington DC: The National Academic Press pp. 19-30 |
|
|
Lewis MA, Russo EB, Smith KM (2018) Pharmacological foundations of Cannabis chemovars. Planta Medica 84(4):225-233. |
|
|
Kahn J (2021). International- Cannabis Industry. Can weed give Africa's economies a buzz. Fortune. June 2, 2021 |
|
|
Mahajan R, Gupta K (2010). Adaptive design clinical trials: Methodology, challenges and prospect. Indian Journal of Pharamcology 42(4):201-207. |
|
|
Martin JH, Hill C, Walsh A, Efron D, Taylor K, Kennedy M, Galletis R, Lightfoot P, Hanson H, Agar M, Lacey J (2020). Clinical trial with cannabis medicines - guidance fot ethics committees, governance officers and researchers to streamline ethics apllications and ensuring patient safety: considerations from Australian experiene. Trial 21:932 |
|
|
McPartland JM, Guy GW (2017). Models of cannabis taxonomy, cultural bias and conflicts between scientific and vernacular names. Botanic Review 83:327-381. |
|
|
Moschick EC, Mercado C, Yoshino T, Mutsuura K, Watanabe K (2012) Usage and attitude of physicians in Japan concerning traditional Japanese medicine (Kampo): A descriptive evaluation of representative questionnaire-based survey. Evidence-Based Complementary and Alternative Medicine 2012:139818. |
|
|
Ncube BM, Dube A, Ward K (2021) Establishment of the African Medicines Agency: Progress, challenges and regulatory readiness. Journal of Pharmacy Policy and Practice 14(29):1-12. |
|
|
Nutt D, Bazure S, Phillips LD, Schlag AK (2020) So near yet so far: why wont the UK prescribe medicinal cannabis. British Medical Journal Open 10:e038687. |
|
|
Putri D (2020). Cannabis rescheduling: What could it mean for Africa?. Briefing paper. International Drug Policy Consortium and Transnational Institute. |
|
|
Piomelli D, Russo EB (2015). The Cannabis sativa versus Cannabis indica debate: an interview with Ethan Russo. Cannabis Cannabinoid Research 1:44-46. |
|
|
Prohibition Partners (2022). Africa cannabis market could be worth over $US7.1 billion annually by 2023. The African Cannabis Report. Prohitionpartners.com 21.03.2019 |
|
|
Reddy V, Grogan D, Ahluwalia M, Salles EL, Ahluwalia P, Khodadadi H, Alverson K, Nguyen A, Raju SP, Braun M, Vale FL, Costigliola V, Dhandapuni K, Baban B, Vaibhav K (2020).Targeting the endocannabinoid system: A predictive, preventive and personalize medicine-directed approach to the management of brain pathologies. EPMA Journal 11(2):217-250 |
|
|
Russo EB (2019). The case for the entourage effect and conventional breeding of chemical cannabis: No "Strain" no Gain. Frontiers in Plant Science 9:1969. |
|
|
Sabaghi D (2022). Inside The Largest Ever Independent Cannabis Study In The UK forbes. |
|
|
South Africa Health Products Regulatory Authority (SAHPRA) (2020). The innovation in regulatory science capacity development in Africa, virtual meeting report. 30 June, 2020. |
|
|
Schoedel KA, Chen N, Hilliard A, White L, Scot C, Russo E, Wright S, Guy G, Romach MK, Sellers EM (2011). A randomized double-blind placebo-controlled crossover to evaluate the subjective abuse potential and cognitive effects nabiximols oromucosal spray in subjects with a history of recreational cannabis use. Human Psychopharmacology 26(3):224-236. |
|
|
Semete-Makokotlela B, Mahlangu GN, Mukanga D, Darko DM, Stonier P, Gwaza L, Nkambule P, Matsoso P, Lehnet R, Rosenkranz B, Pillai GC (2022). Needs-driven talent and competency development for the next generation of regulatory scientist in Africa. British Journal of Clinical Pharmacology 88(2):579-586 |
|
|
Small E (2015). Evolution and classification of Cannabis sativa (marijuana hemp) in human utilization. Botanical Review 81:189-294. |
|
|
Tashkin DP (2017) Effects marijuana smoking on the lung. Annals of the American Thoracic Society 13:239-247. |
|
|
Tashkin DP, Roth M (2020). Impact of marijuana smoking on lung function in older persons. European Respiration Journal 55:1902328 |
|
|
US FDA (2016). Botanical Drug Development Guidance for Industry. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


