Full Length Research Paper
ABSTRACT
This study investigated the effectiveness of the Mobile Authentication Service (MAS) introduced on antimalarial medicines (AMs) in curbing the incidences of counterfeiting for this group of pharmaceuticals. The assessment of the knowledge, attitude and use of the technology by Nigerian citizens, uncovering areas of deficit as well as proffering recommendations on the current use pattern of MAS by Nigerians was carried out. Nine hundred (900) questionnaires were used to assess the awareness of the Nigerians on the availability of the MAS feature on AMs and their knowledge on the correct use of the feature to get needed information about the authenticity of the AMs. 78% of respondents claimed to have heard about Short Messaging Service to check for counterfeits in AM. 51.4% of the respondents who knew about MAS had actually scratched the tag or had been involved in the process of using the service. 48.8% of these respondents received positive responses as feedback upon sending the pin while 4.7% did not receive any feedback response. While MAS does not provide information about the biopharmaceutical properties of these medicines, it confirms the authenticity of the product source and supply chain, thereby guarding against the possibility of infiltration by counterfeiters. This advantage would be of high benefit for artemisinin-combination therapy (ACTs) medicines and other AMs if exploited properly. Nigeria is the first country where MAS has been deployed extensively for the security of pharmaceuticals thus the need to conduct corresponding studies in other countries to ascertain the effectiveness of the MAS.
Key words: Mobile authentication service (MAS), pharmaceutical supply chain, anti-malarial medications.
INTRODUCTION
The global supply chain especially for pharmaceuticals is complex, as many components of medicines and sometimes the entire pharmaceutical product are manufactured far from where they are being supplied and consumed (Attaran et al., 2012; Mackey et al., 2012). In the public sector, procurement and distribution of medicines in Nigeria is both centralized and decentralized (Attaran et al., 2012; Iwokwagh, 2013). Most medicines are procured and stored by the individual health care institutions, while medications for HIV, malaria and tuberculosis are centrally procured and distributed from the Federal Central Medical Store (CMS) (Erhun et al., 2004). Each state in the varying geo political zones of Nigeria also has its own Central Medical Store, and procures and stores pharmaceuticals for their public facilities (Amin and Kokwaro, 2007; Onwujekwe et al., 2009). Private sector distribution is handled through pharmaceutical wholesalers although it is widely accepted that unlicensed wholesalers play a very significant role in drug distribution at this level of the supply chain (NAFDAC/Sproxil 2015).
The advancement in technology worldwide has increased the sophistication of pharma-counterfeiting and in turn compelled The National Agency for Food and Drug Administration and Control (NAFDAC) to employ technological measures in the fight against counterfeiting of medicines (Bansal et al., 2013; NAFDAC /Sproxil 2015). In the recent years, NAFDAC has introduced a range of fake drugs detecting technologies such as the TruScan device (based on Raman spectroscopy), Black eye, Radio Frequency Identification (RFID) and the Mobile Authentication Service (MAS) using Short Message Service (SMS) (Iwokwagh, 2013; NAFDAC /Sproxil, 2015).
The menace of counterfeit medicines especially AMs had assumed alarming proportions and the effects in terms of mortality rates was staggering (NAFDAC/Sproxil 2015). Given the prevalence of mobile technology throughout the world, it made sense to use a technology that was already in every customer’s pocket pocket (Global medicine supply chain 2012; Damon Beres 2015). Through drug authentication, consumers can avoid purchasing counterfeit medication, while anonymously and passively providing key intelligence to law enforcement agencies regarding the location of fake drugs, anytime authentications fail repeatedly. The goal was to improve the consumers’ overall health and quality of life (Iwokwagh, 2013; Osuolale, 2015).
MAS (also called Mobile Product Authentication) allows consumers to verify that the product they are buying is genuinely from the manufacturer, by using a mobile phone and a simple, free text message. If a fake product is found, a consumer is given a hotline number to call in order to report the fake product, so the issue can be directed to the appropriate authorities.
Among several approaches towards the eradication of fake/substandard pharmaceuticals NAFDAC employed the use of telecommunication in combating this menace. The Mobile Authentication Service (MAS) of NAFDAC is an attempt at turning the mobile phone which is now in the hands of majority of Nigerians into a tool of fighting the war against fake/substandard pharmaceuticals product proliferation in Nigeria (NAFDAC/Sproxil 2015; Osuolale, 2015).
Onwujekwe et al. (2009) in a paper assessing the quality of AMs provided by public and private healthcare providers in South-east Nigeria, observed that people seek treatment for malaria from public sector facilities and a range of formal and informal private sector facilities.
About 60% of all malaria episodes in sub-Saharan Africa are initially treated by private providers, mainly through the purchase of drugs from shops and drug peddlers (Onwujekwe et al., 2009). The "informal private sector", such as patent medicine dealers, is a main source of anti-malarial drugs, but the quality of treatment that they provide is questionable (Bate et al., 2008; Ilomuanya et al., 2012). A major problem with the treatment of malaria is the high level of treatment failures resulting in the large part from the high prevalence of counterfeit drugs bought by the patients (Bate et al., 2008; Snow et al., 2005). Hence the need for enforcement deadline given to pharmaceutical companies by NAFDAC for the implementation of MAS on all AMs and antibiotics sold in Nigeria which was July 2014 (NAFDAC/Sproxil, 2015; Osuolale, 2015; WHO Factsheet on the World Malaria Report 2013; World Health Organization: Medicines, 2010).
This study was therefore designed to evaluate the level of awareness of MAS among the Nigerian populace assessing the extent of utilization of MAS by the Nigerian public and assessing the degree of acceptance of MAS among community pharmacists in Nigeria.
This will be carried out by assessing the knowledge, attitude and use of the technology by the average Nigerian citizen. The study will also attempt to uncover areas of deficit as well as to proffer suggestions and recommendations on the current use pattern of MAS by the general public.
METHODS
Ethics
The Research and Ethics committee of the West African Postgraduate College of Pharmacist gave approval for the research to be carried out without a an ethical approval as the committee deemed that the project was an evaluation of the use of a service, that is, mobile authentication service (MAS) by the populace, that is a service evaluation. The evaluation of the use of MAS among the Nigerian populace utilizing AMs was assessed from April 2015 to July 2015 in Nigeria.
Setting
Situated between 4Ëš and 13Ëš Northern Latitude Nigeria has a suitable climate for malaria transmission throughout the country. Nigeria is made up of 36 states and a Federal Capital Territory which have been constitutionally divided into six geopolitical zones (Federal Republic of Nigeria Draft National Human Resources For Health Strategic Plan 2008 to 2012). This study was carried using a
state selected at random from each of the six geo-political zones in Nigeria and Lagos state. The states used from the respective zones are as listed as follows:
1. South-South Zone (SSZ): Rivers state
2. North-West Zone (NWZ): Jigawa state
3. South-East Zone (SEZ): Enugu state
4. North-Central Zone (NCZ): Nasarawa state
5. South-West Zone (SWZ): Ogun state
6. North-East Zone (NEZ): Taraba state
7. Lagos Zone (LZ): Lagos State
Data sampling
Sample size calculation was based on the assumption that 70% of the Nigerian population utilize mobile phones (Dorlo et al., 2012; Osuolale, 2013). The level of significance utilized for this study was 0.05 and a power of 0.7 was obtained based on the assumption of the number of Nigerians using mobile phones. Utilizing sample size calculator NSS version 12.0 (2013) Australian Bureau of Statistics, a sample size of 778 was obtained. The questionnaire was developed from previous studies developed in Survey Gizmo®, the survey however was online (Adibe, 2009; SurveyGizmo®, 2015; Strauss and Corbin, 1990). The questions captured the detail, rationale and application of methods used within the study design and populations.
The method utilized collection of primary data using informal questionnaires administered to the general population irrespective of gender, status or educational background. The questionnaires were administered via non probability cluster random sampling method by the researcher and research assistants across the states selected for the study. The informal questionnaires were used to assess the awareness of the Nigerian populace on the availability of the MAS feature on AMs and their knowledge on the correct use of the feature to get needed information about the authenticity of the AMs. The study locations utilized were NAFDAC registered Pharmaceutical retail premises which sold house hold products as well as Pharmaceutical products and services in the city centres of the States selected for the study. The respondents were randomly selected clients visiting these premises, every other client entering into the premise was asked to fill the questionnaire. This simple random sampling method is representative of potential clients who are utilizing AMs.
Pertinent areas highlighted in the questionnaire include observing the presence of the scratch tag on the AMs, conducting the authentication process, frequency of conducting this process and the outcome received from the process.
The study sample
A total number of nine hundred (900) questionnaires were produced for the process of data collection. An initial pre-test using 30 questionnaires was carried out in a small area in one of the study sites. This was done to assess the understanding of the respondents and to ensure that the questions posed did not mean different things to the respondents. Based on the findings of the pre-test, the questionnaires were modified and consequently administered in each of the study sites. One hundred (100) questionnaires were administered in each of the geo-political zones and three hundred (300) questionnaires in Lagos state. Seven hundred and seventy four (774) questionnaires were collected out of a total of nine hundred (900) a response rate of 86% was recorded which was adequate for the study.
Data collection
The questionnaires were self-administered by the literate respondents. The questions were carefully read and their responses were documented accordingly. For less literate respondents with whom reading the questionnaire or recording their responses posed some challenges, the researcher had to interpret the questions asked using a vernacular language such that they were not at variance from the words and statements contained in the questionnaire.
Data analysis
The tools used for data analysis were correlation coefficient and chi-square. SPSS version 21 (IBM corp. Amonk New York) statistical package was employed in the analysis.
RESULTS
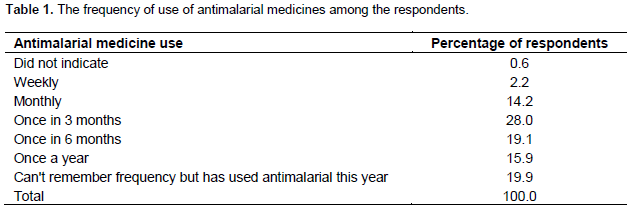
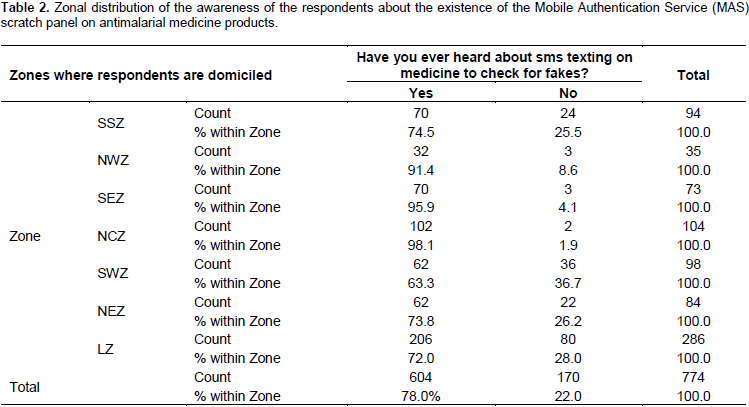
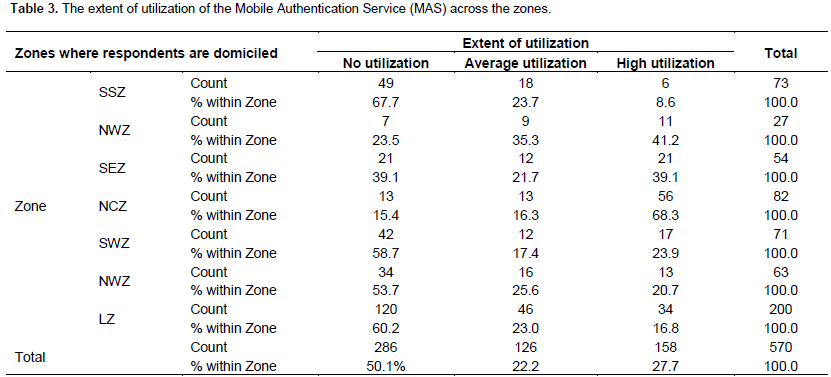
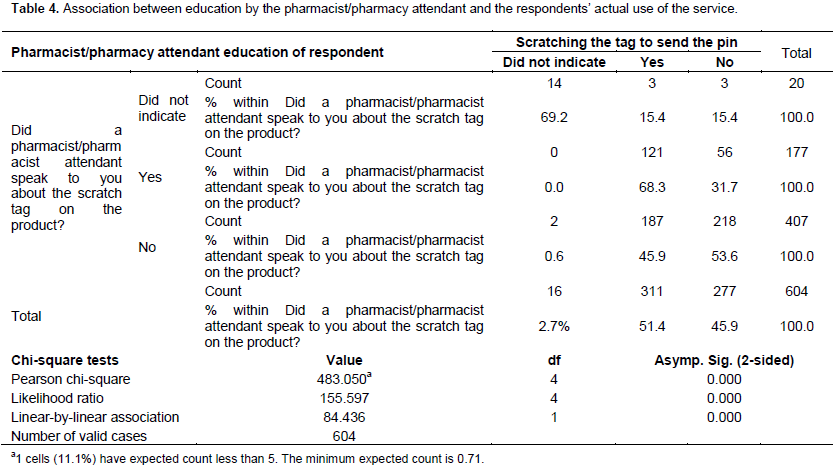
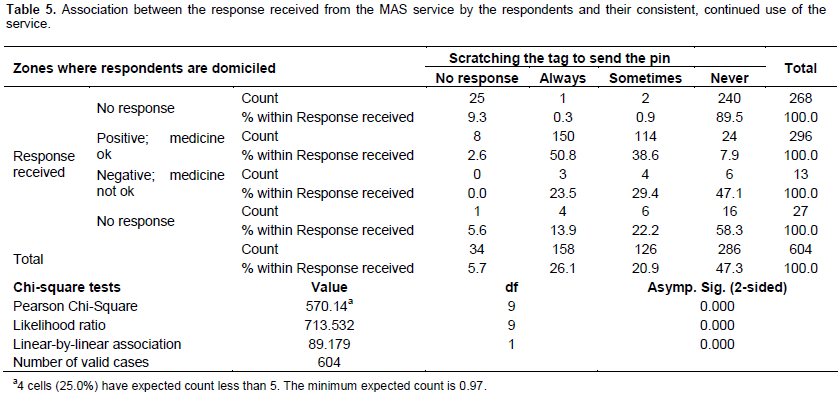
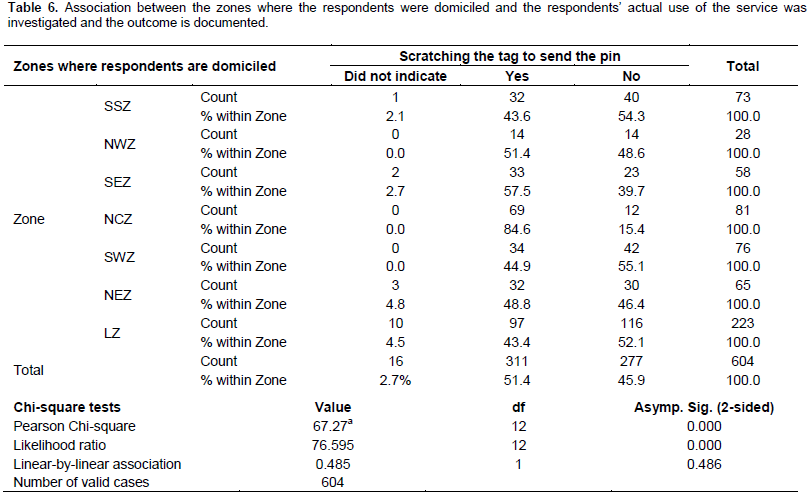
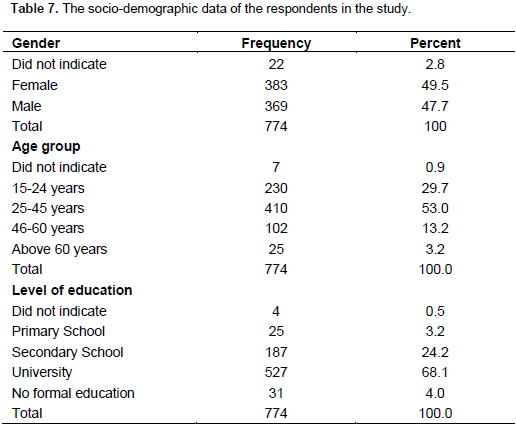
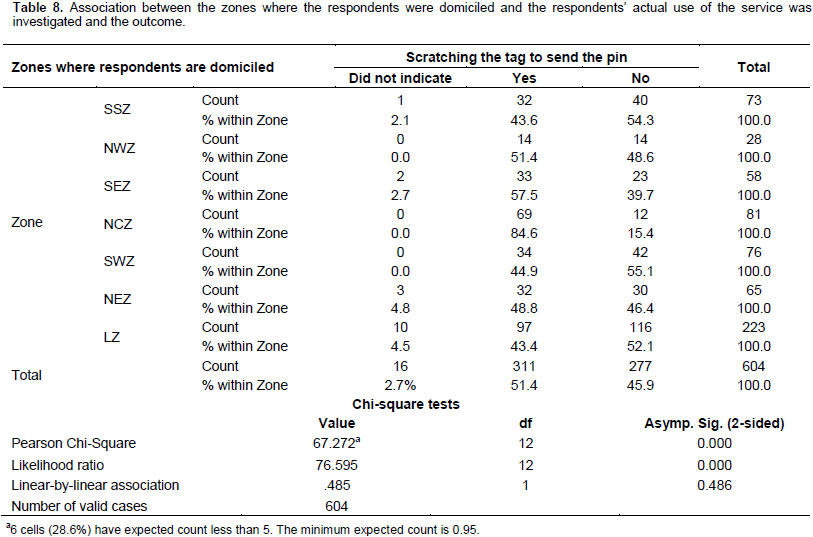
Six geopolitical zones were used for the study with Lagos state as an additional zone on its own. LZ had the highest number of questionnaire retrieved accounting for 37.0%, NCZ, SWZ, SSZ and NEZ accounted for 13.4, 12.7, 12.1 and 10.9% of the questionnaires retrieved respectively. The NWZ accounted for the least number of questionnaires retrieved, that is, 4.5%. Descriptive statistics were utilized in reporting data for socio-demographics of the respondents 53.1% of the respondents were in the 25 to 45 years age bracket with 92.3% attaining secondary education or better. The frequency of antimalarial medicine use among the respondents was evaluated as shown in Table 1 where more than 62.5% of the respondents had used antimalarial medicine at least once a month, with 99.4% of respondents indicating use of AMs at least once this year. A high level of awareness of the use of MAS was seen through all the zones as shown in Table 2 with all the zones showing more than 70% of the respondents as being aware of MAS. However even though high levels of awareness was seen the extent of utilization was very poor as shown in Table 3, with 50.1% of the respondents not utilizing MAS even when they are aware of it use as reflected in Table 2. Table 4 showed a strong association between education by the pharmacist/pharmacy attendant and the respondents’ actual use of the service, the outcome was that where the pharmacist or technician educated the patient about the tag the more likely it was for the patient to scratch the tag and send the pin number to the service provider, thus the high likelihood ratio and linear by linear association of these variables. Association between the response received from the MAS service by the respondents and their consistent, continued use of the service was investigated and the outcome was that a positive response correlated with continued use of the service as shown in Table 5 with a Pearson Chi-Squared value of 540.14. The association between the zones where the respondents were domiciled and the respondents’ actual use of the service was investigated and the outcome is documented in in Table 6 showed a small linear by linear association between the two variables with a Pearson Chi-Square value of 67.27, the actual use of MAS was not dependent on the zones where the respondents were domiciled.
The highest percentage of respondents that had tried out the service never used it (47.3%). The percentage increases to 61.1% when using the service to check the product at the point of purchase is considered. Many reasons were proffered by the respondents for using or not using the service which include the need to confirm the quality of the product (26.4%) and not having much knowledge about the service (8.9%).
To determine the level of awareness of MAS among the Nigerian populace, cross tabulations were done between socio-demographic parameters (namely zone, age group, educational level, gender) and the awareness level of the respondents. Among the zones, the North-Central zone (NCZ) had the highest level of awareness (98.1%) while the South-West zone (SWZ) had the least awareness level of 63% (Table 2). Generally, there is a total level of awareness of 78% as against 22% of non-awareness of the service among the population out of 99.4 % of respondents who claimed to have purchased tagged antimalarial medicines.
The level of awareness was highest among the age group of 25 to 45 years with an awareness level of 82%. The age group of above 60 years of age presented the lowest percentage (64%) of awareness. Respondents with tertiary education had the highest level of awareness of MAS (85%) while those with no formal education had the least level of awareness. Gender-wise, the males seemed to be more aware of the service (79.1%) than the females (77.3%) (Table 7). Across the zones, respondents in the North-Central zone (NCZ) were most aware (98.1%) about the existence of the service while the South-West zone (SWZ) seemed least aware (36.7%) of the service as reflected in Tables 2, 3 and 8 showed the association between the zones where the respondents were domiciled and the respondents’ actual use of the service was investigated and the outcome was that the south east zone (SEZ) had % within zone of 57.5% giving a yes response.
DISCUSSION
The extent of utilization of the MAS by the Nigerian public researched into using the socio-demographic parameters reflected overall utilization showed that 50.1% of respondents do not use the MAS service at all. 22.2% expressed average utilization of the service while only 27.7% highly use MAS. The North-Central zone (NCZ) had the highest utilization percentage of 68.3% while the South-South zone (SSZ) had the least usage of 8.6%. The higher percentage of utilization was recorded among the males (30.7%) while the usage among the females was put at 25.1%. The age group of 25-45 years gave the highest utilization percentage of 34.4%. The age group of 15-24 years had the least percentage (14.0%) of MAS utilization. In terms of the level of education of the respondents, those with tertiary educational level had the highest percentage of utilization (31.1%) while those without formal education showed the least percentage of MAS utilization (3.6%) as shown in Table 3. Though high percentages were obtained for awareness, it did not cut across educational levels and age groups thus the need to ensure awareness and enlightenment campaigns are brought to basic levels of language and media to reach the entire populace.
An association between the pharmacists’ educational role in speaking to the respondents about the service and the respondents’ willingness to use the service was investigated. 68.3% of the respondents who actually used the service claimed to have been spoken to by a pharmacist/pharmacy attendant about the service. This represents the largest percentage of those who had used the service. 53.6% of those who were aware of the service but still had not used it claimed they had received no education from the pharmacist or attendant at the outlet. A p-value of 0.00 was obtained upon chi-square analysis which indicates significance in the association as shown in Table 4.
A second association to confirm whether the response received from initially using MAS had any effect on the respondents’ consistent and continued use of the service was investigated. 50.8% of the respondents who got a positive “medicine ok” response from the MAS service claimed to use the service repeatedly with each purchase. The higher percentage of 58.3% of the respondents who had initially used the service and received no response from the MAS claimed they never repeated the use of the service. A significant p-value of 0.00 was also obtained upon chi-square analysis as shown in Table 5.
A third association between the socio-demographic parameters and the use of the service was also investigated. Respondents in North-Central zone (NCZ) indicated the highest percentage of use with 84.6%. The highest percentage of those who had not used the service was found in the South-West zone (SWZ). 56% of those who had used the service had tertiary education level while 52.6% were males.
The use and extent of utilization of MAS for AMs appeared comparable with the level of awareness. The zone, age group, gender and educational level bracket with the highest levels of awareness of MAS also produced corresponding results of the highest use and extent of utilization of the service. The continued and consistent use of the service seemed affected by the response received from the MAS system upon initial use and whether the respondents had been spoken to/educated by the healthcare professional.
The level of awareness in the general population (78%) however, does not seem to translate to willingness of the population to use the service (54.4%) and much less to the regular, continued and consistent use of the service (26.1%) which is the intent of the introduction of the service and the premise on which the MAS service as a counterfeit deterrent is hinged upon. Among those who knew how to use the service, 61.1% do not use the service to check their products at the point of purchase.
While a sizeable proportion of the respondents (26.4%) indicated that their use of the service was to confirm the authenticity of the medicine, respondents presented various reasons for their unwillingness to use the service. 4.7% felt that once a pharmacy or representative was adjudged as ‘standard’, there was no need to authenticate the medicine’s quality. Some stated that upon seeing the scratch tag on a product, it meant that the product was original even without employing the service. In most communities, the pharmacist is the first accessed healthcare professional. There is a need for community and hospital pharmacists to ensure that the patient is not only educated on the benefit of the service but is also encouraged and if need be, assisted to employ the service as it should be used.
There were also the issues of network failure and a proportion of respondents feeling that they could not be bothered about using the service. There is a challenge of technological support which needs to be looked into. MAS, as a tool relies on technology thus the need to liaise with telecommunication providers, not only for free MAS messaging, but to ensure that as much as is possible, network challenges are minimized.
By virtue of its design, the effectiveness of MAS in curbing counterfeiting is not just in its use but its regular use per unit, per purchase. In other words, every single scratch panel is meant to be scratched and pin sent to the default code to receive a response regarding the product’s quality at the point of purchase. It does not matter if two individual packs are of the same brand or in one pharmacy. Each code is unique and is meant to protect the single unit pack bearing it and not the brand per se nor is it to endorse any outlet. This is what puts the power of safe guarding one’s health literally in one’s own hands.
With the actual consistent use of MAS at 26.1% of respondents, there appears to be a gulf between the awareness level and the regular utilization of the service. The extent of utilization was highest with the highest level of education and lowest with those without formal education. This may be an indication that the communication of the service, either in content or channels employed, may be occluded from a section of society.
Two decades ago, chloroquine had been the preferred drug of choice for malaria therapy (Ilomuanya et al., 2012). Its effectiveness was overtaken by the emergence of resistance by the malaria parasites. Chloroquine-resistance has been traced to the use counterfeit and substandard medicinal products by patients (Onwujekwe et al., 2009). The last decade ushered in the newer and more effective artemisinin compounds which are now being used as first line antimalarial therapy in combination with existing AMs. It is mandatory in Nigeria that all artemisinin-combination therapy (ACTs) medicines utilize the MAS (Onwujekwe et al., 2009; NAFDAC /Sproxil, 2015), however while MAS does not provide information about the biopharmaceutical properties of these medicines, it confirms the authenticity of the product source and supply chain, thereby guarding against the possibility of infiltration by counterfeiters. This advantage is of high benefit for artemisinin-combination therapy medicines if exploited properly.
Nigeria is the first country where MAS has been deployed extensively for the security of pharmaceuticals. Apart from Nigeria, Kenya, Ghana and India have also used the service but on pilot scales. These countries have recently employed the service publicly on their pharmaceuticals thus the need for corresponding studies to ascertain MAS effectiveness. While MAS can guarantee the integrity of the supply chain of pharmaceuticals, the safety, efficacy and quality of the medicine are not taken into account. There must be a framework to ensure that the manufacturers/importers and their respective products are periodically assessed for quality and effectiveness.
CONCLUSION
Malaria medicines are constantly in high demand and unfortunately, they have become a target for pharma-counterfeiting. While MAS does not provide information about the biopharmaceutical properties of these medicines, it confirms the authenticity of the product source and supply chain, thereby guarding against the possibility of infiltration by counterfeiters. The strong association between education by the pharmacist/pharmacy attendant and the respondents’ actual use of the service reflected that pharmacist involvement in patient care would increase the use of MAS. This advantage would be of high benefit for artemisinin-combination therapy (ACTs) and other AMs if exploited properly. Nigeria is the first country where MAS has been deployed extensively for the security of pharmaceuticals. There may be a need to have corresponding studies carried out in other countries to ascertain the effectiveness of the MAS.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adibe MO (2009). Prevalence of concurrent use of herbal and synthetic medicines among outpatients in a mission hospital in Nigeria. Int. J. Drug Dev. Res. 1:60-66. |
|
|
Amin AA, Kokwaro GO (2007). Antimalarial drug quality in Africa. J. Clin. Pharm. Ther. 32(5):1-15. |
|
|
Attaran A, Barry D, Basheer S, Bate R, Benton D, Chauvin J, Garrett L, Kickbusch I, Kohler JC, Midha K, Newton P, Nishtar S, Orhii P, McKee M (2012). How to achieve international action on falsified and substandard medicines. BMJ. 345:e7381. |
|
|
Australian Bureau of Statistics (2015). National Statistics service (NSS) View (Accessed April 2 2015) |
|
|
Bansal D, Malla S, Gudala K, Tiwari P (2013). Anti-Counterfeit Technologies: A Pharmaceutical Industry Perspective. Sci. Pharm. 81(1): 1–13. doi: 10.3797/scipharm.1202-03 |
|
|
Bate R, Coticelli P, Tren R, Attaran A (2008). Antimalarial drug quality in the most severely malarious parts of Africa: A six country study. PLos ONE. 3(5): 1-3. |
|
|
Damon Beres (2015). In Parts Of Africa, Cell Phones Are Everywhere And Landlines Barely View (Accessed March 30, 2015) |
|
|
Dorlo TPC, Ravinetto RM, Beijnen JH, Boelaert M (2012). Substandard medicines are the priority for neglected tropical diseases. BMJ 345: e7518 |
|
|
Erhun WO, Babalola OO, Erhun MO (2004). Drug Regulation and Control in Nigeria: The Challenge of Counterfeit Drugs. J. Health & Population in Developing Countries. 4(2):23-34. |
|
|
Federal Republic Of Nigeria Draft National Human Resources For Health Strategic Plan (2008). Available at: View (Accessed May 26, 2015) |
|
|
Global Medicine Supply Chain (2012). Foreign Affairs 2012. |
|
|
Ilomuanya MO, Kalu C, Nnakebe C, Achonu L, Ifudu ND, Ette E, Odulaja JO (2012). Survey of first line therapy for uncomplicated Malaria in compliance with malaria policy change in a faith based hospital in Lagos Nigeria. World J. Pharmaceut. Res. 1(2):1-9. |
|
|
Iwokwagh NS (2013). Assessment of new media use in the fight against counterfeit medicines in Nigeria. International Conference on Communication, Media, Technology and Design Famagusta – North Cyprus. 2013 Available at: View (Accessed May 26, 2015) |
|
|
Mackey TK, Liang BA, Kubic TT (2012). Fighting Fraud in the Global Medicine Supply Chain. Foreign Affairs 2012. |
|
|
Onwujekwe O, Kaur H, Dike N, Shu E, Uzochukwu B, Hanson K, Okoye V, Okonkwo P (2009). Quality of anti-malarial drugs provided by public and private healthcare providers in south-east Nigeria. Malar. J. 8:22. ISSN 1475-2875 |
|
|
Osuolale JA (2013). The Use of Mobile Phone to check for the Authenticity of Pharmaceutical Products in Nigeria a case study of Mobile Authentication Service (MAS) Available at: View (Accessed May 30, 2015) |
|
|
Snow RW, Guerra CA, Noor AM, Myint HY, Hay SI (2005). The global distribution of clinical episodes of Plasmodium falciparum malaria. Nat. Inter. weekly J. Sci. 434: 214-217. |
|
|
Strauss A, Corbin J (2015). Basics of qualitative research: Grounded theory procedures and techniques. London: Sage; 1990. |
|
|
WHO (2013). Factsheet on the World Malaria Report 2013 Available at: |
|
|
World Health Organization (2010). Medicines: Counterfeit Medicines. Available at: View (Accessed June 3, 2015) |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


