Full Length Research Paper
ABSTRACT
The National Department of Health identified the need for Universal Health Coverage, highlighting improved access to quality healthcare in South Africa.Clinical pharmacists play a vital role in various settings, including medication safety, therapeutic drug monitoring and antimicrobial stewardship. Healthcare-related key performance indicators measures quality that ensure accountability, improve patient safety and assist decision-making. To understand the perceptions of pharmacists regarding education, barriers and outcome measures on practices of clinical pharmacy, this study employed qualitative research, with focus-group discussions and in-depth interviews.Dialogue from interviews and focus-groups were audio-taped, transcribed and stored as MS-Word™ documents. NVivo® were utilised to identify themes.Pseudo-names ensured participant confidentiality.Ethics approval was obtained from the Sefako Makgatho University Research and Ethics committee, participating private-healthcare groups and Government Research Offices. Pharmacists were interviewed in eight provinces, identifying seven themes. The majority of pharmacists felt that notable differences exist between the scope of practice of ward- and clinical pharmacists. Most pharmacists did not know the definition of pharmaceutical care.The consensus was that clinical functions require more in-depth work than functions by general pharmacists. All pharmacists experienced barriers to performing their functions. Mostly outcome measures used by pharmacists pertain to antimicrobial stewardship, pharmacists felt that additional training is necessary to perform clinical functions. Clinical work is considered more intense and requires greater involvement in multidisciplinary teams. The study contributes to the state of clinical pharmacy in South Africa. It provides insight into the different levels of clinical pharmacy practice. The findings provide insights into the implementation of Clinical pharmacy services in developing countries.
Key words: Clinical pharmacy, pharmaceutical care, barriers, outcome measures.
INTRODUCTION
Clinical pharmacy, which includes pharmaceutical care or the direct supervision of a patient’s pharmacotherapeutic needs (SAPC, 2014; Bronkhorst et al., 2018), is a rapidly developing field for practicing pharmacists in South Africa (SA).
According to the American College of Clinical Pharmacy (ACCP), clinical pharmacists have advanced education and training to obtain the skills to practice in direct patient care environments (ACCP, 2014). Training of clinical pharmacists in SA includes a Master’s degree in clinical pharmacy. This was originally initiated in 2000 by one University, who graduated around 114 students since (Crafford et al., 2021). Four other universities followed, however not with a modular Master’s degree, and graduated much less students (around 18). Rhodes University offered a PharmD programme (Gous and Schellack, 2014), who graduated around 16 students before discontinuing the course. The slow uptake of clinical pharmacy services can be related to infrastructure and resource limitations (Crafford et al., 2021).
Many institutions employ ward pharmacists to perform pharmaceutical care (NDoH, 2015). Hence, the level of pharmaceutical care differs in different institutions and between practitioners.
In 2015, the National Department of Health (NDoH) published a report describing the need for Universal Health Coverage (UHC), which described the need for improvement of access to quality healthcare in South Africa (NDoH, 2015). Over and above the pharmacist’s role in the stable supply of medicines, they must also play a broader role as caregivers, rather than dispensers. The National Core Standards set out by the NDoH in 2011, described a specific domain for patient safety, clinical governance and patient care (NDoH, 2011). These guidelines are still followed by the Departmental Monitoring Group, to ensure the vision of the guidelines are followed. A Cochrane meta-analysis, of both national and international studies, confirmed clinical pharmacists’ role in various settings (Hindler and Stelling, 2007; CDC, 2014; Kim et al., 2015; Kolman et al., 2016), like therapeutic drug monitoring (TDM) (Simpson, 2004; Viljoen et al., 2016), reduction of medication errors (Simpson, 2004; Wong et al., 2008; Truter et al., 2017), and medication reconciliation (Sebaaly et al., 2015; Van Kemseke et al., 2017; Naicker et al., 2018). Clinical pharmacists also play a role in specific speciality care environments such as cardiology (Francis and Abraham, 2014), and oncology (Dobish et al., 2014). Although studies have been done in SA on the role of the clinical pharmacist in critical care (Bronkhorst et al., 2014) and neonatal care (De Jager et al., 2014), it is generally in limited settings and isolated. In SA, although clinical pharmacists are not recognised as specialists, the South African Pharmacy Council (SAPC) encourages the pharmacist to be part of the multidisciplinary healthcare team (SAPC, 2014).
Although the scope of practice of a clinical pharmacist has been published by the South African Pharmacy Council (SAPC, 2014), and practice guidelines have been published (Bronkhorst et al., 2020) no adaptive standard practice guidelines exist for clinical pharmacy practice in SA. Healthcare-related key performance indicators, such as the number of pharmacist-led interventions, the number of drug-related problems identified or the level of patient satisfaction, are quantifiable measures of quality that may ensure accountability for the health care professional (Bronkhorst et al., 2020).
Performance indicators improve patient safety as well as assist role-players in decision-making (Fernandes et al., 2015).
Knowledge of the perceptions of pharmacists who practice clinical pharmacy services at the ward level can help improve the quality of and implementation of patient care in different settings (Dosea et al., 2017). Faced with changes in the role of South African pharmacists, understanding the perceptions of these professionals regarding the practice of clinical pharmacy services is of utmost importance. The terms “Pharmaceutical Care” and “Clinical Pharmacy”, as adopted by the SAPC and the South African Society of Clinical Pharmacy (SASOCP), can be defined as a health science specialty applying the scientific principles of pharmacology, toxicology, pharmacokinetics and therapeutics to the care of patients, and the responsible provision of pharmaceutical care with definite outcomes and improvement of patient care in mind, respectively (Hepler and Strand, 1990; ACCP, 2016).
Aim
The study sets out to describe the perceptions of pharmacists regarding factors such as education, barriers and outcome measures in the practice of clinical pharmacy.
Ethics approval
Ethics approval was obtained from the Sefako Makgatho Health Sciences University Research and Ethics committee (SMUREC) (number: SMUREC/H/110/ 2015:PG). Consent to perform the study was obtained from the participating private healthcare groups as well as the respective Government Provincial Research Offices. Participation in the study was voluntary and pseudo-names were assigned to all participants to ensure anonymity.
METHODS
Clinical pharmacy
It can be defined as ‘a health science specialty that embodies the application, by pharmacists, of the scientific principles of pharmacology, toxicology pharmacokinetics and therapeutics to the care of patients’ (ACCP, 2016).
Pharmaceutical care
Originally defined by Hepler and Strand (1990) as ‘the responsible provision of drug therapy for the purpose of achieving definite outcomes that improve a patient’s quality of life’.
Study design and duration
The qualitative design included focus group discussions and in-depth interviews. Pharmacists in similar geographical locations were grouped together for focus group discussions, and in-depth interviews were held with individual pharmacists in more remote areas.
The data were collected over a six-week period. The researcher had training in qualitative research and collected all the data herself.
Study population and sample
The study participants included pharmacists who were identified from data collected during a previous study (Bronkhorst et al., 2018), where pharmacists performing clinical pharmacy activities or rendering pharmaceutical care duties at the ward level were identified. The study population included pharmacists from private as well as public tertiary hospitals.
A total of five focus group discussions and 28 interviews were conducted with a total of 38 pharmacists being interviewed. The majority of participants were from Gauteng Province (17; 45.9%), female (34; 91.9%), between 31-40 years old (22; 59.5%) and either holding an MPharm degree (19; 51.4%) or busy completing an MPharm degree (11; 29.7%). Qualitative sampling was employed; the sampling procedures did not aim to obtain a representative sample, but rather to select subjects with the purpose of gaining an in-depth understanding of the research question (Hardon et al., 2005).
The homogeneity or heterogeneity of the study sample determined whether it was adequate to meet the needs of the study (Leedy and Ormrod, 2016). The sample size for the present study was small since the target population is homogenous and the aim was to elicit information, not cases. Purposive sampling was used to select clinical pharmacists for in-depth interviews. These pharmacists were selected from different private hospital groups as well as from central and tertiary public hospitals. These participants were best equipped to address the research question as a result of their work experience and scope of practice. Interviews were conducted until all subjects were interviewed or data was saturated.
Data collection instrument
The questions for the focus group discussions were determined following the work of an earlier study (Bronkhorst et al., 2018). In cases where unclear responses were provided or further explanation was required, appropriate probes were used according to the discretion of the investigator. A focus group guide was used, with questions derived from the quantitative results from a previous study (Bronkhorst et al., 2018) to include questions and possible probes about the study problem. The in-depth discussions were intended to explore quantitative results from a previous study.
Data collection and analysis
The audio of the dialogue from the interviews was recorded. Interview audio files were transferred from the digital voice recorder to a computer and stored as Windows Media Audio files. Recorded interviews were transcribed verbatim by the investigator immediately after each of the interviews was conducted, typed and stored as MS Word™ documents. Transcripts were imported into NVivo® 11 software (QSR International, 2011) to apply the necessary coding. A thematic approach to the analysis of the data was followed. Data were coded into categories by the first author and an independent coder and then corroborated to conclude the final categories and overarching themes.
RESULTS
Demographic data of participant
Five focus group discussions and 13 in depth-interviews were conducted, with 38 participants The majority of participants were from Gauteng Province (17; 45.9%), female (34; 91.9%), and 51.4% (19) were in possession of a postgraduate degree.
Themes
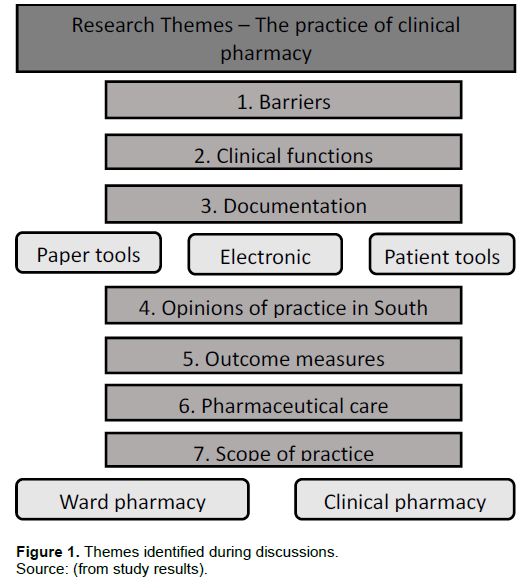
The seven themes and five sub-themes, as identified during the analysis process, were supported with direct quotes and excerpts from the interviews and discussions, where applicable. Grammatical errors were corrected to enhance the readability of quotes. Pseudo-names were assigned to participant quotes to maintain confidentiality. The themes discussed are depicted in a diagrammatical representation shown in Figure 1.
Theme 1: Scope of practice
The majority (89.6%) of pharmacists expressed that there is a notable difference between the scope of practice of a ward pharmacist and that of a clinical pharmacist. However, none of the pharmacists interviewed was aware of the published scope of practice of the clinical pharmacist, nor the scope of practice of a ward pharmacist as set out in the Good Pharmacy Practice. The statements below illustrate the perceptions of pharmacists on the scope of practice of pharmaceutical care.
“A clinical pharmacist makes interventions in drug dosages, renal function, liver functions , and drug interactions. Also, go on ward rounds with the doctors and assist in making decisions about the correct medication choices. The pharmacist would do the prescription evaluation, look at the laboratory results, pharmaceutical calculations and according to that, recommend changes to the doctor regarding the therapeutic plan.”
“Interpretation of a prescription is easier if you are a clinical pharmacist and you have more clinical background and knowledge.”
Theme 2: The definition of pharmaceutical care
Most pharmacists (62.3%) did not know the specific definition of pharmaceutical care. As evidenced by the comments below, most expressed that pharmaceutical care is the responsibility of all pharmacists, however, some felt that pharmaceutical care is the exclusive duty of the clinical pharmacist.
“The philosophy has always been that pharmaceutical care is one of the tools that a clinical pharmacist use to reach his goals. To ensure the patient’s medication-related problems are addressed, medication-related needs mentioned included: indication, effectiveness, safety and adherence, and from that formulate the drug-related problems.”
“I think every pharmacist performs pharmaceutical care, not only ward pharmacists or clinical pharmacists. To my mind it is that you read the prescription, interpret it and then act on it.”
Theme 3: Functions pertaining to clinical pharmacy
The majority of pharmacists (89.8%) felt that therapeutic drug monitoring (TDM) is exclusively a clinical pharmacist’s function. Most of them (94.3%) felt that antimicrobial stewardship (AMS) is an important clinical function. The consensus was that clinical functions are more in-depth work than functions performed by a general pharmacist, as is evident by the following responses:
“Major intervention for a clinical pharmacist for instance is the therapeutic drug monitoring of amikacin. Other functions will be looking at blood culture results, doing renal function adjustments for doses and checking for possible interactions.”
Ward-pharmacists without any clinical pharmacy training stated that they do not have the confidence to do more specialized functions, and will focus more on general work like ordering medication, checking for allergies and therapeutic duplication.
“A ward pharmacist will definitely not do that in-depth intervention. Ordering medication is more of a general pharmacist’s job. They will also look at drug allergies and therapeutic duplication. The clinical pharmacist will evaluate the patient’s data, look at blood gas results, and look at laboratory results to look for infection markers. Antibiotic stewardship and many of the things that come along with it, checking the results, apply the drug-bug match; it’s more for clinical pharmacists.”
“Clinical pharmacy should be looking at the bigger picture in terms of evidence-based practice like multiple antibiotics usage, or too many drugs, and drug interactions.”
The participants had some difficulty rating the importance of interventions and felt that there is no standard of practice available for them to measure their work.
“Clinical pharmacy is looking at a holistic approach that is going to matter to the patient in terms of therapy, in terms of mortality, quality and morbidity It is assessing the patient’s basic data such as physical examination, vitals, notes, also medication, to see if all medications are indicated, effective, safe, looking at adherence, reconciliation and laboratory results.”
Theme 4: Documentation of work and tools
Most (73.3%) pharmacists developed their system for documentation of their work, which includes paper-based documentation on notepads or notebooks. The private hospital groups have electronic systems for documentation of specific interventions, especially antimicrobial stewardship interventions. These systems are used in varying degrees, as is evident by the comments:
“A notepad will be used and patient stickers on each page will be followed by patient information and issues detected. Afterwards in the pharmacy, you will read up on issues identified in each patient. Then interventions will be recorded on a system for the healthcare group.”
Many pharmacists (44.3%) stated that they do not record their work, mostly because of time constraints.
“Only around 50% of interventions and reviews are recorded.”
The tools that pharmacists use to assist them in performing their clinical duties include textbooks, for instance, the South-African Medicines Formulary (SAMF) and the National Essential Medicines List (EML) online, especially in the public sector, but most pharmacists prefer to use electronic resources or applications (app) on cellphones or tablets like Medscape.
“Mostly, phone applications are used. Medscape for drug interactions and the Sanford guide for dosing of antibiotics, especially renal dosing. Applications are nice because it is being updated and it provides up-to-date data.”
Theme 5: Barriers
All the pharmacists interviewed (100%) felt they experienced some form of barrier to performing their function optimally.
Dedicated time seems to be the greatest barrier for most of pharmacists (76.3%), as most hospitals do not have dedicated posts for clinical ward-pharmacists and they still need to perform functions about dispensing and stock control in the pharmacy.
“Pharmacists are awarded so little time to spend in the wards If more staff were available, they could easily be allocated to the wards full time.”
Another barrier for most pharmacists is the attitude of other staff members (63.2%), including pharmacy colleagues, management, nursing staff and doctors.
“Teamwork is a challenge. Sometimes the clinical pharmacist is seen as a threat instead of a team member, more like a ‘policeman’ than a team player in the patient’s care.”
“They think a pharmacist is supposed to dispense, you don’t question, you don’t do anything else, you dispense your drugs and that’s it.”
Lack of mentorship, or preceptorship, is experienced as a barrier, and some pharmacists feel that they do not have adequate knowledge and exposure (47.4%).
“I miss mentorship. It is my greatest wish to join a clinical pharmacist to work so that one has the correct guidance to do it right.”
Theme 6: Outcome measures
The majority of pharmacists (78.3%) do not use specific outcome measures to measure the impact of their work. Some outcome measures that are utilised at the moment mostly pertain to antimicrobial stewardship and include the length of therapy, the double cover of the spectrum and appropriate laboratory tests. They also record whether an intervention was accepted or not.
“How many interventions were done and what functions have been done is measured, but in terms of how it benefited or what were the outcomes for the patient, it’s difficult to say.”
Some pharmacists (58.2%) felt that it would be beneficial to look at more patient-based outcome measures, for instance, length of stay and mortality, although the data is not always available to them.
“Clinical pharmacists measure the number of interventions that are accepted and rejected. They can look at vital signs, infection markers, pyrexia going down after the intervention, but the opinion is that it’s on clinical knowledge that they rate what they’ve done, but it cannot always be proven.”
Theme 7: Opinions on clinical pharmacy
The opinion on the state of clinical pharmacy in South Africa differed greatly. Some pharmacists felt very positive (23.6%), while others felt that the profession is in a cul-de-sac due to the tardiness of the authorities to implement specialist registration (33.2%).
“From when I first started working as a clinical pharmacist until now, people are much more aware of what clinical pharmacists do. The doctors are much more receptive of their contribution.”
“It will be great if the pharmacy council can finalise their requirements, so you can know where to proceed. Many pharmacists have now obtained the degree, but you can still not call yourself a clinical pharmacist, because you are not registered as such.”
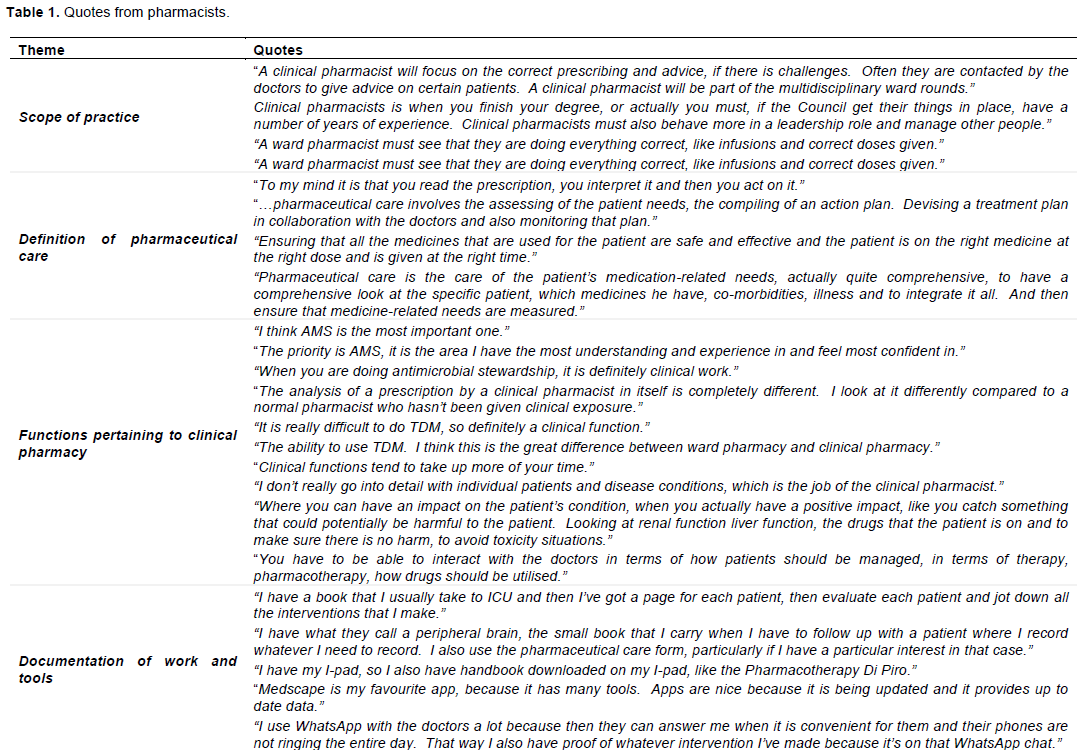
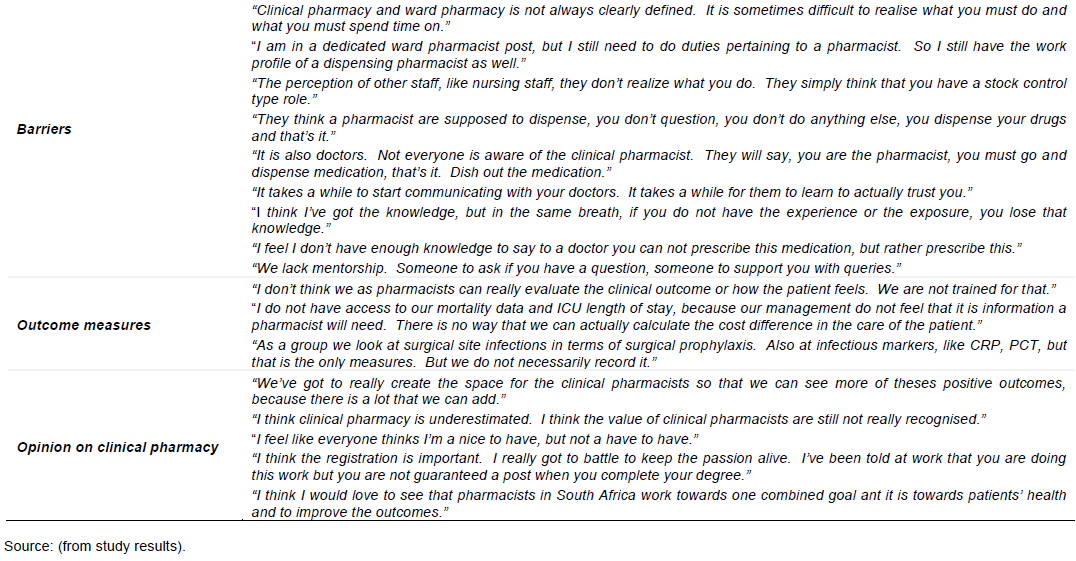
Table 1 contains more direct quotes from participating pharmacists supporting the different themes identified.
DISCUSSION
Although the South African Pharmacy Council (SAPC) has published a proposed scope of practice for clinical pharmacists, and the required curriculum for specialisation (SAPC, 2014), no requirements or specific key-performance indicators for registration as a specialist pharmacist have been published (SAPC, 2014). Many pharmacists practice pharmaceutical care at the ward level, however, they had some difficulty rating the importance of interventions and felt that there is no standard of practice available for them to measure their work. The majority of pharmacists agreed that there is a notable difference between the scope of practice of a ward pharmacist and that of a clinical pharmacist.
Most pharmacists felt that therapeutic drug monitoring (TDM) is exclusively a clinical pharmacist’s function, while most of them stated that antimicrobial stewardship (AMS) is an important clinical function. International literature describes the roles of clinical pharmacists e.g. participation in ward rounds, drug therapy reviews, preventing drug interactions, optimising dosing and frequency and reducing prescribing errors (Jacobi, 2016). Other clinical pharmacist functions described include developing quality assessment tools and evaluating data, as well as education of peers and other healthcare workers. The consensus was that clinical functions are more in-depth work than functions performed by a general pharmacist and that further training is necessary (Jacobi, 2015; Dosea et al., 2017).
The findings reiterate the statement by Jacobi (2015) that clinical pharmacists need advanced education and training to effectively focus on comprehensive medication management. Ward-pharmacists in the study stated that they do not have the confidence to interact with prescribers the way trained clinical pharmacists do. El-Awaisi et al. (2017) stated that healthcare professionals, including pharmacists, need to develop the knowledge and skills required to effectively gain confidence to work together with the multidisciplinary team to positively impact patient care. In another study, the lack of knowledge and training of pharmaceutical staff were noted as a barrier to the successful implementation of clinical pharmacy services (Dosea et al., 2017).
Groppi et al. (2018) showed the importance of intervention-capture in a study where documentation was shown to advance clinical pharmacy practice by linking clinical and economic outcomes. Although private hospital groups have electronic systems for documentation of specific interventions, especially in antimicrobial stewardship, the majority of pharmacists keep their documentation system, which is not reported to other members of the healthcare team or hospital management. Pharmacists who do not record their interventions felt that is mostly because of time constraints. In a study by Minard et al. (2016), pharmacists felt that documentation of clinical activities was unnecessary, difficult to maintain and tiresome.
All the pharmacists interviewed felt they experienced some form of barrier performing their function optimally. As indicated by the lack of documentation, time seems to be the greatest barrier for most pharmacists, as most hospitals do not have dedicated posts for clinical or ward pharmacists. This fact is echoed in the study by Minard et al. (2016), where pharmacists identified an increased workload as a barrier to the implementation process, in large part due to the availability of time. Another barrier for most pharmacists is the attitude of other staff members, including pharmacy colleagues, management, nursing staff and doctors. The role of the clinical pharmacist as part of the healthcare team is not regularly recognised. In a study by Chevalier et al. (2016), nurses and physicians changed their opinions from before to after implementation of clinical pharmacy services, to agree that pharmacists must participate in ward activities and that having a pharmacists present to manage medication issues allowed them to feel more confident and leaves them to concentrate on their own professional roles.
Preceptorship or mentorship is an aspect that pharmacists felt is lacking in the South African environment. Some felt they do not have adequate knowledge and experience. In the United States, clinical pharmacists undergo a two-year PGY-residency, wherein an established clinical pharmacist mentors the candidate to perform clinical duties (Jacobi, 2016). The results from the study highlights the aspect of a lack of preceptorship in the South African environment. Some pharmacists felt that while not having adequate knowledge and experience, experienced mentors to guide them are not available.
The in-depth investigation on the opinion on the state of clinical pharmacy in SA resulted in varying opinions from practicing pharmacists. Most pharmacists felt positive about the development of the profession over recent years, while others felt that the profession is in a cul-de-sac due to the tardiness of authorities to implement specialist registration.
Further investigation into the motivation for clinical pharmacists to perform their functions and what they expect specialisation to be, may be necessary to establish the success of a practice. None of the pharmacists were aware of the published scope of practice of the clinical pharmacist, nor the specific definition of pharmaceutical care. Although pharmaceutical care has been re-defined many times, it is always used to describe the activity as part of patient care (Alleman et al., 2014). Although the majority of respondents felt that pharmaceutical care is the responsibility of all pharmacists, some felt that it is the exclusive duty of the clinical pharmacist.
CONCLUSION
Clinical pharmacists in South Africa are building their practice with varying degrees of influence in the practice around them. Specialist postgraduate training of clinical pharmacists in South Africa is growing and those qualified is set on improving practice. They agreed that post-graduate education is necessary to perform their functions. These functions include multidisciplinary ward rounds, assessment of appropriate drug therapy, including therapeutic duplication monitoring, adverse drug events and side effects and to optimise dosing and dosing-frequency. Therapeutic drug monitoring and antimicrobial stewardship are some of the most important functions of the clinical pharmacist as perceived by South African pharmacists. Although pharmacists perform these functions often, no quality assessments for professional practice are available to measure standards of practice.
In conclusion, the lack of general standard of practice guidelines in South Africa needs to be addressed to standardise practice across the public and private sectors in the country.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Alleman SS, Van Mil JW, Botermann L. Hersberger KE (2014). Pharmaceutical Care: the PCNE definition 2013. International journal of clinical pharmacy 36(3):544-555. |
|
|
American College of Clinical Pharmacy (ACCP) (2014). Standards of Practice for Clinical Pharmacists. Pharmacotherapy 34(8):794-797. |
|
|
American College of Clinical Pharmacy (ACCP) (2016). About Clinical Pharmacists. |
|
|
Bronkhorst E, Gous AG, Schellack N (2020). Practice Guidelines for Clinical Pharmacists in Middle to Low Income Countries. Frontiers in Pharmacology (11)978. |
|
|
Bronkhorst E, Schellack N, Gous AG (2018). A Situational Analysis of the Current State and Working Conditions of Clinical Pharmacy in South Africa. European Journal of Clinical Pharmacology. 20(3):170-175. |
|
|
Bronkhorst E, Schellack N, Gous AG, Pretorius J (2014). The Need for Pharmaceutical Care in an Intensive Care Unit at a Teaching Hospital in South Africa. Southern African Journal of Critical Care 30(2):41-44. |
|
|
Centre for Disease Control and Prevention (CDC) (2014). Core Elements of Antimicrobial Stewardship Programmes. |
|
|
Chevalier B, Neville HL, Thompson K, Nodwell L, MacNeil M (2016). Health Care Professionals' Opinions and Expectations of Clinical Pharmacy Service on a Surgical Ward. Canadian Journal of Hospital Pharmacy 69(6):439-448. |
|
|
Crafford L, Wouters A, Bronkhorst E, Gous AG, Kusurkar RA (2021). Exploring Factors associated With theMotivation of Clinical Pharmacists: A Focus on the South African Context. Frontiers in Medicine 8:747348. |
|
|
De Jager Z, Schellack N, Gous AG (2014). What Role does the Clinical Pharmacist Play in the Neonatal Intensive Care Unit? SA Pharmacy Journal 81(7):22-23. |
|
|
Department of Health (2015). National Department of Health. White paper on National Health Insurance: |
|
|
Dobish R, Chambers C, Iwaasa K, Hubley B, Brigden M (2014). Expanding the Role of Clinical Pharmacists in Community Oncology Practice: Results of Implementation at the Jack Ady Cancer Clinic. Oncology Exchange 13(4):24-28. |
|
|
Dosea AS, Brito GC, Santos LM, Marques TC, Balisa-Rocha B, Pimentel D, Bueno D, Lyra DP (2017). Establishment, Implementation and Consolidation of Clinical Pharmacy Services in Community Pharmacies: Perceptions of a Group of Pharmacists. Qualitative Health Research 27(3):363-373. |
|
|
El-Awaisi A, Joseph S, El Hajj MS, Diack L (2017). A comprehensive systematic review of pharmacy perspectives on interprofessional education and collaborative practice. Research in Social and Administrative Pharmacy 14(10):863-882. |
|
|
Fernandes O, Gorman SK, Slavik RS, Semchuck WM, Shalansky S, Bussieres J, Coucette D, Bannerman H, Lo J, Shukla S, Chan WW, Benninger N, MacKinnon NJ, Bell CM, Slobodan J, Lyder C, Zed PJ, Toombs K (2015). Development of Clinical Pharmacy Key Performance Indicators for Hospital Pharmacists Using a Modified Delphi Approach. Annals of Pharmacotherapy 49(6):656-669. |
|
|
Francis J, Abraham S (2014). Clinical Pharmacists: Bridging the Gap Between Patients and Physicians. Saudi Pharmaceutical Journal 22(6):600-602. |
|
|
Gous AG, Schellack N (2014). The State of Clinical Pharmacy in South Africa: Current and Future Perspectives. ACCP International Clinical Pharmacist 3:1-2. |
|
|
Groppi JA, Ourth H, Morreale AP, Hirsh JM, Wright S (2018). Advancement of Clinical Pharmacy Practice through Intervention Capture. American Journal of Health-System Pharmacy 75:e283-e289. |
|
|
Hardon A, Boonmongkon P, Streeflan P, Tan ML, Hongvivatana T, Van der Geest S, Van Staa A, Varkevisser C, Acuin C, Chowdhury M, Bhuiya A, Sringeryuang L, Van Dongen E, Gerrits T (2005). Applied Health Research: Anthropology of Health and Health Care. Third Edition. Amsterdam, The Netherlands: Het Spinhuis Publishers. ISBN 978-9055891917 |
|
|
Hepler CD, Strand LM (1990). Opportunities and Responsibilities in Pharmaceutical care. American Journal of Hospital Pharmacy 47:533-543. |
|
|
Hindler JF, Stelling J (2007). Analysis and Presentation of Cumulative Antibiograms: A New Consensus Guideline from the Clinical and Laboratory Standards Institute. Clinical Infectious Diseases 44:867-73. |
|
|
Jacobi J (2016). Clinical Pharmacists: Practitioners who are Essential Members of your Clinical Care Team. Revista Medica Clinica las Condes 27(5):571-577. |
|
|
Kim J, Craft DW, Katzman M (2015). Building an Antimicrobial Stewardship Program: Cooperative Roles for Pharmacists, Infectious Diseases Specialists, and Clinical Microbiologists. Laboratory Medicine 46(3):65-71. |
|
|
Kolman S, Geertsema H, Van den Berg D, Goff D (2016). Engaging Pharmacy Personnel in Antimicrobial Stewardship Using a NovelMethod of Teaching. SA Pharmaceutical Journal 83(1):25-29. |
|
|
Leedy PD, Ormrod JE (2016). Practical Research: Planning and Design. 11th Edition. New Jersey: Prentice Hall. ISBN 978-0-13-374132-2 |
|
|
Minard LV, Deal H, Harrison ME, Toombs K, Neville H, Meade A (2016). Pharmacists' Perceptions of the Barriers and Facilitators to the Implementation of Clinical Pharmacy Key Performance Indicators. |
|
|
Naicker P, Schellack N, Godman B, Bronkhorst E (2018). Creating and Evaluating an Opportunity for Medication Reconciliation in the Adult Population of South Africa to Improve Patient Care. Hospital Practice e1-e11. |
|
|
National Department of Health, NDoH (2011). National core Standards for health Establishments in South Africa. |
|
|
Sebaaly J, Parsons LB, Pilch NA, Bullingon W, Hayes GL, Piasterling H (2015). Clinical and Financial Impact of Pharmacist Involvement in Discharge Medication Reconciliation at and Academic Centre: A Prospective Pilot Study. Hospital Pharmacy 50(6):505-513. |
|
|
Simpson D (2004). Pharmaceutical Care: The Minnesota Model. The Pharmaceutical Journal 258(6949):899-904. |
|
|
South African Pharmacy Council (SAPC) (2014). Board notice 152 of 2014: Scopes of Practice and Qualifications for Specialist Pharmacists. |
|
|
Truter A, Schellack N, Meyer JC (2017). Identifying Medication Errors in the Neonatal Intensive Care Unit and Paediatric Wards Using a Medication Error Checklist at a Tertiary Academic Hospital in Gauteng, South Africa. South African Journal of Child Health. 11(1):5-10. |
|
|
Van Kemseke S, Huyghens L, Ligneel C, Collier H, Cortoos PJ (2017). Medication Discrepancies at the Time of Admission to and Transfer from the Intensive Care Unit and the Role of the Clinical Pharmacist. European Journal of Hospital Pharmacy 24:A22. |
|
|
Viljoen FP, Rheeders M, Brand L, Du Preez JL (2016). Guidelines to Minimise Human Error in South African Laboratories with Regard to Therapeutic Drug Monitoring. Medical Technology.SA 30(1):30-35. |
|
|
Wong IC, Wong LY, Cranswick NE (2008). Minimising Medication Errors in Children. Archives of Disease in Childhood 94(2):161-164. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


