Review
ABSTRACT
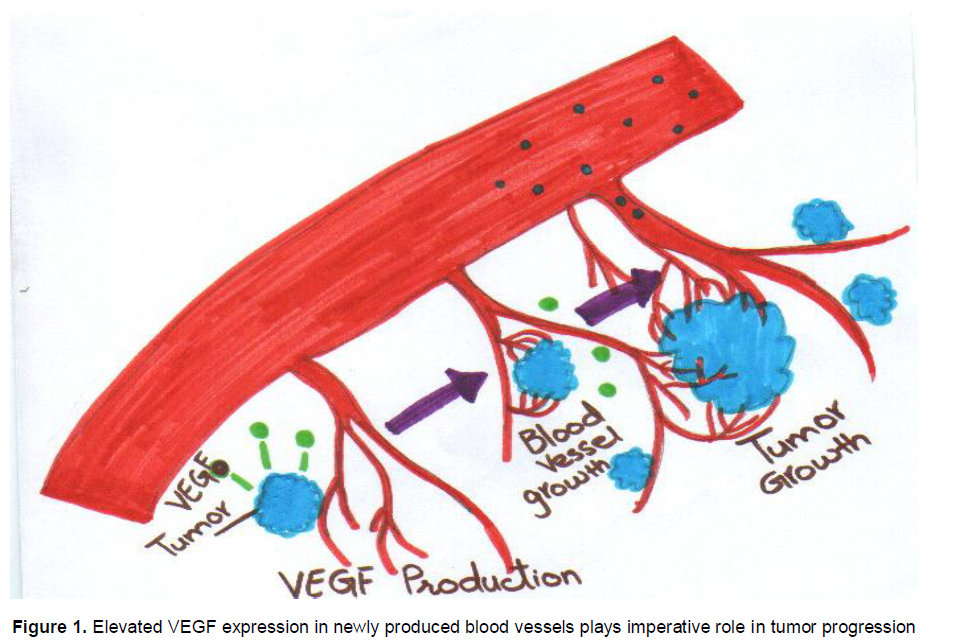
Angiogenesis plays crucial part in the formation and progression of tumor, and vascular endothelial growth factor (VEGF) is one of the most important cytokine which aids in the growth of tumor cells. In various tumors whether locally invasive or metastasize to distal parts, elevated levels of VEGF is observed in blood through angiogenesis, this leads to progression of cancer.
Key words: Vascular endothelial growth factor (VEGF), cancer.
INTRODUCTION
Angiogenesis plays crucial part in the formation and progression of tumor and vascular endothelial growth factor (VEGF) is one of the most important cytokine which aids in the growth of tumor cells. VEGF is a polypeptide structurally associated to platelet-derived growth factor (PDGF). The gene for VEGF is present on chromosome 6p12. Angiogenesis, the process of new blood vessel formation, performs crucial role in both invasive tumor growth and noninvasive tumor growth in breast cancer and other benign and metastasized cancers. There are some benign and malignant tumors such as breast cancer, lung cancer, squamous cell carcinoma, thyroid cancer, etc., in which VEGF has been implicated as a key arbitrator of angiogenesis. Although scientists and clinicians have learned much about the character of VEGF and angiogenesis in breast cancer, many questions related to this phenomenon remain unanswered.
VEGF ISOFORMS AND RECEPTORS
Functions of different isoforms of VEGA are given here briefly:
1. VEGF-A: Angiogenesis, Chemotactic for macrophages and granulocytes, Vasodilation (indirectly by NO release)
2. VEGF-B: Embryonic angiogenesis (myocardial tissue, specifically)
3. VEGF-C: Lymphangiogenesis
4. VEGF-D: Needed for the development of lymphatic vasculature surrounding lung bronchioles
VEGF ROLES IN CANCER CELL PROLIFERATION
Bcl-2 is an anti-apoptotic protein that functions in cell survival, tumor progression and drug resistance, and is induced in response to VEGF in cancer cells (Saleem et al., 2013).
VEGF IN MALIGNANT AND NON-MALIGNANT DISEASE
Tumor develops as a result of abnormalities in the non-vascularizing tissues after certain consequences. Diagnosis of tumor is difficult as diagnosis of other complex diseases (Qadir, 2010; Nisar et al., 2011; Naz, 2012; Janbaz 2012). Extent, strength, aggressiveness and malignancy of tumor depend upon the type of tissue in which tumor arises. Tumor growth is nourished by the formation of blood vessels around the neoplastic cells. VEGF is one of the major growth factor present in the blood surrounding the tumor and causes tumor metastasis. It is an angiogenic cytokine stimulating the cancer propagation in the sera of patients suffering from benign and malignant diseases. Minimum level of VEGF in the healthy individuals than the tumor patients showed that VEGF performs an important role in tumor development, formation and progression of noninvasive and invasive effusions (Kraft et al., 1999).
Breast cancer patients
As a consequence of comparative study on patients having breast cancer and healthy woman, VEGF in breast cancer patients has surpassed and elevated to very high concentration. Breast cancer can be propagated and metastasize under the influence of elevated levels of VEGF and it also has an impact on tumor stages. Before initiating the therapy, VEGF level has surpassed in breast cancer patients (Berezov et al., 2009). VEGF has been indicated as a potent angiogenic factor that has an effect on the tumor progression.It has been measured in high concentrations in patients having breast cancer and other cancer types. After treating breast cancer by antiangenic agents combined with conventionally used drugs like temoxifen, methotrexate, flurouracil, adriamycin and cyclophosphamide as a first line therapy especially site specific (Khalid et al., 2009; Hussain et al., 2011; Ehsan et al., 2012; Naz et al., 2012), there is a low concentration of VEGF observed. Menopausal status not only affect the VEGF level in the serum, over expression of estrogen receptor and progesterone receptors have also an influence on its concentration in the serum of breast cancer patients (Foekens et al., 2001).
Tumor growth is dependent on angiogenesis that is carried out by the presence of VEGF . Over expression of estrogen receptor may enhance the concentration of VEGF in the plasma of breast cancer women. After tes-ting on the tubular/ductal breast cancer women compared with those healthy, consequences that VEGF is a signi-ficant factor in the progression and further spreading of tumor to the distant parts and leads to malignancy. These findings may be helpful for further investigations on this issue (Heer et al., 2001). When there is an imbalance which occurs in the aniogenic factor and angiogenesis inhibitors then tumor cell becomes more invasive and malignant because it is supplied by blood vessels having excessive concentrations of growth stimulating cytokines that is VEGF, which propagate the further growth of tumor cells. Patients suffered from node-negative carcinoma have developed malignant condition due to the elevation of VEGF in the serum, so VEGF is consi-dered as an important marker for its progression and propagation (Gasparini et al., 1997). VEGF and basic fibroblast growth factor (bFGF) are two major growth factors imperative role of the tumor growth via angiogenesis. Both of these angiogenic cytokines impart function in the spreading and differentiation of breast cancer into different parts which may be stimulated by over expression of estrogen receptor (Granato et al., 2004). Vascular angiogenesis and vascular permeability are regulated mainly by VEGF which is a growth factor and causes malignant growth of various tumors. Women with benign tumor have less concentration than patients having metastasized tumor growth. Ductal breast cancer patients have very low response towards chemotherapy than lobular or localized breast cancer women (Salven et al., 1999a).
VEGF in the serum of breast cancer patients may be increased. It’s over storage and storage is done by tumor derived interleukin-6 (IL-6) in the platelets. This conforms the role of circulating platelets and IL-6 in the storage of VEGF, ultimately an elevated level of VEGF in the blood of breast cancer patients is seen (Benoy et al., 2002). Angiogenesis is very important and plays crucial role in the survival, and patient response towards therapy also depends on the degree of angiogensis. Temoxifen may also be related with higher VEGF level. Estrogen receptor over expression may enhance VEGF in the malignant effusions (Adams et al., 2000). VEGF enhances tumor growth to the distant parts in patients suffering from breast cancer. This VEGF is elevated to estrogen receptor over activity but is not affected by other serum components such as leptin and prolactin. So it is declared that leptin and prolactin in serum do not affect the tumor metastasis (Coskun et al., 2003). Tumor malignancy and propagation in breast cancer individual is also affected by intratumoral lymphoangiogenesis. VEGF-C in the lymph node performs crucial part in the succession and propagation of tumor cells. Therefore it is concluded that VEGF-C performs important part in tumor metastasis via lymphoangioangenesis. Over expression of estrogen receptor and mutation in the TP-53 gene status has a positive influence to elevate the level of VEGF which ultimately leads to cancerous cells metastasis in the breast cancer patients (Berns et al., 2003).
Under the influence of chemotherapy for breast cancer, there is a considerable low level of VEGF detected, which shows that elevated VEGF has an impact on tumor progression Figure 1 after chemotherapy has become lowered. Pathological condition of breast cancer mainly surpassed to high degree due to various growth factors. Over stimulation of steroid hormone receptor status increased because of elevated concentration of VEGF in the patients having breast carcinoma (Manders et al., 2003). Therapeutic drugs work positively to control the tumor growth (Qadir and Malik, 2010; Masood et al., 2011; Javed et al., 2011; Qadir, 2011; Ameen et al., 2012), ultimately minimum concentrations of VEGF is detected in the serum of breast cancer patients after anticancer therapy (Kim et al., 2009; Colleoni et al., 2002). Pin-1 or VEGF in high concentrations is detected in the serum of patients having breast cancer. It is confirmed by investigations on different groups of patients suffering from breast cancer, the levels of VEGF at extreme point in the serum which leads to further proceeding of tumor cells (Quaranta et al., 2007). Platelets and leukocytes release VEGF and it leads to high concentration in the plasma. This elevated level of VEGF acts as an important angiogenic cytokine in the blood cells surrounding the neoplastic cells which ultimately leads to metastasis of tumor to distant parts. Physiological production of VEGF as an important angiogenic cytokine is by the uterine cells, but due to pat-hological changes in its secretion from uterus leads the tumor to propagate, causing its spread to distant parts.
Ultimately, it may lead to metastasis of tumor. High level of VEGF has key effect on breast cancer. VEGF level considerably decreases due to postmenopausal uterus which could prove protective against breast cancer progressing and spreading (Lowery et al., 2008).
METASTISIZED THYROID CANCER
Tumor formation, development and progression depend upon the concrete and distinct nutritive support that is supplied to thyroid tumor cells by the blood vessels formed around the cancerous area. VEGF is produced at the location of cancerous cells as a growth factor due to angiogenesis. Over expression of VEGF cause the aggressiveness and advance distribution of thyroid cancer. Elevated VEGF levels may also be due to stimulation by thyroid stimulated hormone (TSH). VEGF concentrations in the serum of patients distressed from differentiated thyroid cancer are more than those with non-differentiated thyroid cancer. On the basis of these findings, it is hypothesized that there would be drastically higher levels of VEGF in the serum of patients with persistent or intermittent thyroid cancer than those who had been cured from disease (Tuttle et al., 2002).
COLORECTAL CANCER
Concrete and explicit tumors progress and propagate due to the influence of VEGF which is an imperative angiogenic cytokine. In colorectal cancer patients, VEGF is detected in the serum before and after the operative measures. After performing tumor surgical procedure, decrease of VEGF in the serum is observed. VEGF concentration in the patients suffering from colorectal cancer changes as the tumor progresses or metastasize which indicates that there is a solid relationship between the VEGF con-centration and tumor stages, degree of tumor invasion and dissemination of tumor to the distant parts. High level of VEGF in the serum of patients with colorectal cancer has a significant role in the further progress, metastasis and sequence of tumor growth (Karayiannakis et al., 2002). Patients having colorectal cancer showed an unambiguous meditation of VEGF in their plasma. VEGF comes as a consequence of degranulation of granulocytes and platelets which are there in the plasma. The data collected after observing the VEGF serum level of cancer patients compared with vigorous individuals. Tumor cells nurture very swiftly under the influence of VEGF in the plasma of colorectal patients indicating a very crucial part before and after the surgery. Metastasis of cancerous cells occurs very hastily to the distant areas in colorectal cancer individuals due to extreme level of VEGF (Cubo et al., 2004). Restoration of physical condition and survival, after resection is very difficult because of the high level of VEGF in the serum of colorectal cancer patients. This elevated concentration leads to progression and auxiliary scattering of cancerous cells and it is independent of tumor stages. After testing the serum level of patients anguish from colorectal can-cer compared with individuals recovered from disease, it is suggested that VEGF in plasma has considerable importance in the headway and succession of tumor cell growth (Karayiannakis et al., 2002). Patients with eleva-ted serum concentration of VEGF having gastrointestinal and colorectal carcinoma showed to be more progressive and tumor had metastasized in these patients. Tumor enlargement occurs very rapidly in these patients. Studies on the patients having gastrointestinal and colorectal cancers indicated the fact that patients with minimum concentration of VEGF will continue to exist for longer periods of times as compared to those with more VEGF and similarly these patients with low VEGF respond to chemotherapy better than those having high VEGF in their plasma. These findings advocate that due to high level of VEGF in the serum of colorectal as well as gastrointestinal cancer patients, there is less response towards chemotherapeutic treatment and fewer probability of their endurance (Hyodo et al., 1998).
OVARIAN CANCER
Before operating measures, VEGF in the serum of ovarian cancer patients is observed in very high concen-trations. This high level of VEGF is detected in the loca-lized tumors as well as in the adnexal masses of malignant tumors. Due to the presence of elevated level of VEGF in the serum of patients suffering from ovarian cancer, this leads to fatal condition because tumor is at its peak degree in the distant parts of the body (Cooper et al., 2002). To overcome the tumor angiogenesis, it is needed to regulate the normal concentration of VEGF in the serum. This approach is very helpful in improving the disease status in the patients having benign or metastasized ovarian tumors (Linderholm et al., 2009). Serum VEGF (S-VEGF) concentrations come under the influence of cyto-reductive treatment and it may be better to control VEGF levels in ovarian cancer patients. The survival of ovarian cancer patients do not depend upon this single factor VEGF in the serum (Salgado et al., 1999). VEGF may be transported in the serum by the circulating platelets. So platelets also have an important function in the regulation of VEGF in the serum (Oehler and Caffier, 2000). Ovarian cyst fluid has elevated level of VEGF which hastens the onset of disease towards malignancy. But high concentration of basic fibroblast growth factor (bFGF) has no remarkable function in the progression and succession of ovarian cancer. High level of VEGF in the ovarian cancer patients perform major role via tumor angiogenesis. So, it is an important target for chemotherapeutic agents (Verheul et al., 1997). Highest concentrations of VEGF in the ovarian cyst fluid indicated that the elevated level of VEGF plays important part in the progression and multiplication of ovarian cancer to the distant parts of body (Boss et al., 2001; Qadir and Malik, 2008).
Localized and metastasized tumors are well differentiated by the CA 125 and cystic VEGF in the serum. In ovarian cancer patients, having high level of VEGF, high level of CA 125 was observed in their ovarian cyst fluid. In patients with ovarian epithelial neoplasm, the angiogenesis and augmentation of vascular permeability caused by VEGF indicates for the discharge of the CA 125 antigen into the circulation of patients (Hazelton et al., 1999). There is no association between VEGF and the concentrations of VHL-associated cancers. High level of VEGF is related with the spreading of tumor growth to the distant parts of body.
DISSEMINATED CANCER
Serum VEGF (s-VEGF) may achieve an elevated point in the loco regional or benign tumors and in the metastasized cancers, related to the histological kind of tumors. This high level of VEGF is very important for the metastases of tumors to other areas of the body (Salven et al., 1997). In anemia and intratumoral hypoxia, there is an increased level of VEGF in the serum of patients having stumpy hemoglobin through hypoxia-induced VEGF secretions (Dunst et al., 1999; Qadir et al., 2007; Salven et al., 1999b).
BRAIN TUMOR CYSTS
In the brain tumor cysts, VEGF is released in brain tumors whether benign or malignant. VEGF in brain tumor cyst causes the tumor to progress to the distal parts and makes it malignant (Stockhammer et al., 2000). Metastasized carcinomas progress positively and lead to more severity due to the presence of VEGF and basic fibroblast growth factor in the serum (Lissoni et al., 2001; Weindel et al., 1994). The patients suffering from bacterial meningitis have comparatively low concentration of VEGF in the cyst fluid than those patients with brain tumors. VEGF is found much higher in patients having CM than those having bacterial meningitis (Stockhammer et al., 2000; Takano et al., 1996).
HEAD AND NECK CANCER
VEGF acts as an endocrine growth factor, a positive angiogenic cytokine. As clinical monitoring point of view, it develops solid and definite growth of head and neck cancer and causes the further proceeding of tumor, leads to malignancy condition (Stockhammer et al., 2000). Head and neck cancer may develop very rapidly in the presence of elevated concentration of VEGF due to the proliferation of cancer cells and endothelial cells of head and neck. This high level of VEGF in head and neck cancer is a pin point target for the therapeutic point of view (Riedel et al., 2000).
RENAL CELL CARCINOMA (RCC)
Cancerous cells in the patients suffering from renal cell carcinoma releases VEGF into the blood circulation which may be a crucial factor in the progression and further spreading of renal cell carcinoma. Over expression of VEGF receptor is detected in renal cell carcinoma patients. Chances of survival of patients in renal cell carcinoma will be increased, if VEGF level become low in the serum of patients having renal cell carcinoma (Eisma et al., 1997). In both the localized tumor and malignant tumor, an association has observed between VEGF and tumor cyst fluid (Sato et al., 1999). VEGF performs important role in the spreading of tumor cell growth in the tumor cyst wall, in areas of hyaline cystic degeneration, in stellate reticulated astrocytes around microcysts, in the biphasic squashed and loose areas. VEGF causes the formation of cysts, microcystic pattern, hyaline cystic degeneration, hyaline vessels and vascular proliferation (Demirkiran et al., 2003).
SOFT-TISSUE SARCOMA
Tumor-induced angiogenesis is mostly caused by VEGF and basic fibroblast growth factor. As an outcome of histological testing and by tumor grading, it is concluded that the elevated concentrations of VEGF and basic fibroblast growth factor (bFGF) detected in patients distress from soft tissue sarcoma. This higher level of both of these growth factors leads to the progression of cancerous cells whether it is malignant or nonmalignant circumstance (Graeven et al., 1999; Qadir et al., 2006).
ANEMIA AND ELEVATION OF VEGF
VEGF is regulated by a major stimulus that is tissue hypoxia. Due to impairment of tissue oxygenation, anemia has impact on angiogenesis which ultimately affect the tumor growth because angiogenesis provides nutritive support to the progression of tumor cells whether it is benign or malignant. Testing on patients suffering from malignant tumor showed elevated levels of VEGF as compared to those with nonmalignant diseases. Due to decreased hemoglobin level, there will be increase in VEGF in the serum of metastasized tumor patients. When hemoglobin level changes under erythropoietin treatment then there will be normalization in the VEGF level. This has indicated that anemia might have an important role in the progression and propagation of tumor growth (Dunst et al., 2002).
The emergence of resistance and tolerance to the existing drugs has created a decreased efficacy of these drugs in use. This problem has been tried to be overcome by increasing the drug delivery to the target site by the use of polymers (Khalid et al., 2009; Hussain et al., 2011) or through nanotechnology (Naz et al., 2012; Ehsan et al., 2012), synthesis of new drugs, either by the use of proteomics (Qadir, 2011; Qadir and Malik, 2011), or synthesis from lactic acid bacteria (Masood et al., 2011), or marine microorganisms (Javed et al., 2011). However, nowadays, the trend is being changed from synthetic drugs to the natural drugs either from plants or microbes to control the diseases. The natural products are constantly being screened for their possible pharma-cological value particularly for their anti-inflammatory (Qadir, 2009), hypotensive (Qadir, 2010), hepatoprotec-tive (Ahmad et al., 2012; Ali et al., 2013), hypoglycaemic (Nisa et al., 2009; Qadir and Malik, 2010), amoebicidal (Asif and Qadir, 2011), anti-fertility, cytotoxic, antimicro-bial (Amin et al., 2012), spasmolytic, bronchodilator (Janbaz et al., 2013a), antioxidant (Janbaz et al., 2012), anti-diarrheal (Janbaz et al., 2013b) and anti-cancer properties. With the passage of time and advancement in science and technology, new management tools have been emerged for the control of different diseases including cancer. Anti-VEGF therapies are important in the treatment of certain cancers and in age-related macular degeneration. They can involve monoclonal antibodies such as bevacizumab (avastin), antibody derivatives such as ranibizumab (lucentis), or orally-available small molecules that inhibit the tyrosine kinases stimulated by VEGF: lapatinib (tykerb), sunitinib (sutent), sorafenib (nexavar), axitinib, and pazopanib.
CONCLUSION
The collected data show that in various tumors whether locally invasive or metastasize to distal parts, there are elevated levels of VEGF in blood through angiogenesis, which leads to progression of cancer. Anti-VEGF therapies are important in the treatment of certain cancers.
REFERENCES
|
Adams J, Carder PJ, Downey S, Forbes MA, MacLennan K, Allgar V, Kaufman S, Hallam S, Bicknell R, Walker JJ, Cairnduff F, Selby PJ, Perren TJ, Lansdown M, Banks RE (2000). Vascular endothelial growth factor (VEGF) in breast cancer: comparison of plasma, serum, and tissue VEGF and microvessel density and effects of tamoxifen. Cancer Res. 60:2898-2905. Pubmed |
||||
| Ahmad M, Mahmood Q, Gulzar K, Akhtar MS, Saleem M, Qadir MI (2012). Anti-hyperlipidaemic and hepatoprotective activity of Dodonaea viscosa leaves extracts in alloxan-induced diabetic rabbits (Oryctolagus cuniculus). Pak. Vet. J. 32:50-54. | ||||
|
Ali M, Qadir MI, Saleem M, Janbaz KH, Gul H, Hussain L, Ahmad B (2013). Hepatoprotective potential of Convolvulus arvensis against paracetamol-induced hepatotoxicity. Bangladesh J. Pharmacol. 8:300-304. Crossref |
||||
|
Ameen S, Qadir MI, Ahmad B (2012). Pharmacogenomic approaches in the treatment of breast cancer by tamoxifen. Pak. J. Pharm. Sci. 25:469-476. Pubmed |
||||
| Amin N, Qadir MI, Khan TJ, Abbas G, Ahmad B, Janbaz KH, Ali M (2012). Antibacterial activity of Vacuum liquid chromatography (VLC) isolated fractions of chloroform extracts of seeds of Achyranthes aspera. J. Chem. Soc. Pak. 34:589-592. | ||||
| Asif MA, Qadir MI (2011). Molecular approaches for development of malarial vaccines. Rev. Pharmacol. 4:276-278. | ||||
|
Benoy I, Salgado R, Colpaert C, Weytjens R, Vermeulen PB, Dirix LY (2002). Serum interleukin 6, plasma VEGF, serum VEGF, and VEGF platelet load in breast cancer patients. Clin. Breast Cancer 2:311-315. Crossref |
||||
|
Berezov TT, Ovchinnikova LK, Kuznetsova OM, Karabekova ZK, Vorotnikov IK, Tuleuova AA, Katunina AI, Dvorova EK (2009). Vascular endothelial growth factor in the serum of breast cancer patients. Bull. Exp. Biol. Med. 148:419-424. Crossref |
||||
|
Berns EM, Klijn JG, Look MP, Grebenchtchikov N, Vossen R, Peters H, Geurts-Moespot A, Portengen H, van Staveren IL, Meijer-van Gelder ME, Biker B, Sweep FC, Foekens JA (2003). Combined vascular endothelial growth factor and TP53 status predicts poor response to tamoxifen therapy in estrogen receptor-positive advanced breast cancer. Clin. Cancer Res. 9:1253-1258. Pubmed |
||||
|
Boss EA, Massuger LF, Thomas CM, Geurts-Moespot A, Boonstra H, Sweep CG (2001). Vascular endothelial growth factor in ovarian cyst fluid. Cancer 91:371-377. Crossref |
||||
|
Colleoni M, Rocca A, Sandri MT, Zorzino L, Masci G, Nolè F, Peruzzotti G, Robertson C, Orlando L, Cinieri S, de BF, Viale G, Goldhirsch A (2002). Low-dose oral methotrexate and cyclophosphamide in metastatic breast cancer: antitumor activity and correlation with vascular endothelial growth factor levels. Ann. Oncol. 13:73-80 Crossref |
||||
|
Cooper BC, Ritchie JM, Broghammer CL, Coffin J, Sorosky JI, Buller RE, Hendrix MJ, Sood AK (2002). Preoperative serum vascular endothelial growth factor levels: significance in ovarian cancer. Clin. Cancer Res. 8:3193-3197. Pubmed |
||||
|
Coskun U, Günel N, Toruner FB, Sancak B, Onuk E, Bayram O, Cengiz O, Yilmaz E, Elbeg S, Ozkan S (2003). Serum leptin, prolactin and vascular endothelial growth factor (VEGF) levels in patients with breast cancer. Neoplasma 50:41-46. Pubmed |
||||
|
Cubo T, Padilla D, de la Osa G, Palomino T, García M, Pardo R, Martín J, Arévalo E, Hernández J (2004). Serum vascular endothelial growth factor levels in patients with colorectal cancer and its prognostic significance. Med. Clin. 122:201-204. Crossref |
||||
|
Demirkiran F, Kumbak B, Bese T, Arvas M, Benian A, Aydin S, Uzun H, Sanioglu C, Aydinli K, Kösebay D (2003). Vascular endothelial growth factor in adnexal masses. Int. J. Gynaecol. Obstet. 83:53-58. Crossref |
||||
|
Dunst J, Becker A, Lautenschläger C, Markau S, Becker H, Fischer K, Haensgen G (2002). Anemia and elevated systemic levels of vascular endothelial growth factor (VEGF). Strahlenther Onkol. 78(8):436-441. Crossref |
||||
|
Dunst J, Pigorsch S, Hansen G, Hintner I, Lautenschläger C, Becker A (1999). Low hemoglobin is associated with increased serum levels of vascular endothelial growth factor (VEGF) in cancer patients. Strahlenther Onkol. 175:93-96 Crossref |
||||
| Ehsan O, Qadir MI, Malik SA, Abbassi WS and Ahmad B (2012). Efficacy of nanogold-insulin as a hypoglycemic agent. J. Chem. Soc. Pak. 34:365-370. | ||||
|
Eisma RJ, Spiro JD, Kreutzer DL (1997). Vascular endothelial growth factor expression in head and neck squamous cell carcinoma. Am. J. Surg. 174:513-517. Crossref |
||||
| Foekens JA, Peters HA, Grebenchtchikov N, Look MP, Meijer-van Gelder ME, Geurts-Moespot A, van der Kwast TH, Sweep CG, Klijn JG (2001). High tumor levels of vascular endothelial growth factor predict poor response to systemic therapy in advanced breast cancer. Cancer 61:5407-5414. | ||||
|
Gasparini G, Toi M, Gion M, Verderio P, Dittadi R, Hanatani M, Matsubara I, Vinante O, Bonoldi E, Boracchi P, Gatti C, Suzuki H, Tominaga T (1997). Prognostic significance of vascular endothelial growth factor protein in node-negative breast carcinoma. J. Natl. Cancer Inst. 89:139-147. Crossref |
||||
|
Graeven U, Andre N, Achilles E, Zornig C, Schmiegel W (1999). Serum levels of vascular endothelial growth factor and basic fibroblast growth factor in patients with soft-tissue sarcoma. J. Cancer Res. Clin. Oncol. 125:577-581. Crossref |
||||
|
Granato AM, Nanni O, Falcini F, Folli S, Mosconi G, De Paola F, Medri L, Amadori D, Volpi A (2004). Basic fibroblast growth factor and vascular endothelial growth factor serum levels in breast cancer patients and healthy women: useful as diagnostic tools? Breast Cancer Res. 6:R38-45. Crossref |
||||
|
Hazelton D, Nicosia RF, Nicosia SV (1999). Vascular endothelial growth factor levels in ovarian cyst fluid correlate with malignancy. Clin. Cancer Res. 5:823-829. Pubmed |
||||
|
Heer K, Kumar H, Read JR, Fox JN, Monson JR, Kerin MJ (2001). Serum vascular endothelial growth factor in breast cancer: its relation with cancer type and estrogen receptor status. Clin. Cancer Res. 7:3491-3494. Pubmed |
||||
| Hussain A, Khalid SH, Qadir MI, Massud A, Ali M, Khan IU, Saleem M, Iqbal MS, Asghar S, Gul H (2011). Water Uptake and Drug Release Behaviour of Methyl Methacrylate-co-itaconic acid [P(MMA/IA)] Hydrogels Cross-linked with Methylene Bis-acrylamide. J. Drug Deliv. Sci. Tech. 21:249-255. | ||||
|
Hyodo I, Doi T, Endo H, Hosokawa Y, Nishikawa Y, Tanimizu M, Jinno K, Kotani Y (1998). Clinical significance of plasma vascular endothelial growth factor in gastrointestinal cancer. Eur. J. Cancer 34:2041-2045. Crossref |
||||
| Janbaz KH, Jan A, Qadir MI, Gilani AH (2013a). Spasmolytic, bronchodilator and vasorelaxant activity of methanolic extract of Tephrosia purpurea. Acta. Pol. Pharm. 79:261-269. | ||||
|
Janbaz KH, Nizsar U, Ashraf M and Qadir MI (2012). Spasmolytic, bronchodilator and antioxidant activities of Erythrina superosa Roxb. Acta. Pol. Pharm. 69:1111-1117. Pubmed |
||||
|
Janbaz KH, Qadir MI, Ahmad B, Sarwar A, Yaqoob N, Masood MI (2012). Tuberculosis – Burning Issues: Multi-Drug Resistance and HIV-Coinfection. Critical Rev. Micro. 38:267–275. Crossref |
||||
| Janbaz KH, Qadir MI, Jan A, Gilani AH (2013b). Anti-diarrheal activity of methanolic extract of Tephrosia purpurea. Acta. Pol. Pharm. 79:345-347. | ||||
|
Javed F, Qadir MI, Janbaz KH, Ali M (2011). Novel drugs from marine microorganisms. Crit. Rev. Micro. 37:245-249. Crossref |
||||
|
Karayiannakis AJ, Syrigos KN, Zbar A, Baibas N, Polychronidis A, Simopoulos C, Karatzas G (2002). Clinical significance of preoperative serum vascular endothelial growth factor levels in patients with colorectal cancer and the effect of tumor surgery. Surgery 131:548-555. Crossref |
||||
| Khalid SH, Qadir MI, Massud A, Ali M, Rasool MH (2009). Effect of degree of cross-linking on swelling and drug release behaviour of poly (methyl methacrylate-co-itaconic acid) [P(MMA/IA)] hydrogels for site specific drug delivery. J. Drug Deliv. Sci. Tech. 19:413-418. | ||||
|
Kim BC, Han SI, Lim SC (2009). Interpretation of Pin-1 and VEGF-C expression in breast infiltrating duct carcinoma. Oncol. Rep. 22:1381-1390. Pubmed |
||||
|
Kraft A, Weindel K, Ochs A, Marth C, Zmija J, Schumacher P, Unger C, Marmé D, Gastl G (1999). Vascular endothelial growth factor in the sera and effusions of patients with malignant and nonmalignant disease. Cancer 85:178-187 Crossref |
||||
|
Linderholm BK, Hellborg H, Johansson U, Elmberger G, Skoog L, Lehtiö J, Lewensohn R (2009). Significantly higher levels of vascular endothelial growth factor (VEGF) and shorter survival times for patients with primary operable triple-negative breast cancer. Ann. Oncol. 20:1639-1646 Crossref |
||||
|
Lissoni P, Malugani F, Bonfanti A, Bucovec R, Secondino S, Brivio F, Ferrari-Bravo A, Ferrante R, Vigoré L, Rovelli F, Mandalà M,Viviani S, Fumagalli L, Gardani GS (2001). Abnormally enhanced blood concentrations of vascular endothelial growth factor (VEGF) in metastatic cancer patients and their relation to circulating dendritic cells, IL-12 and endothelin-1. J. Biol. Regul. Homeost. Agents 15:140-144. Pubmed |
||||
|
Lowery AJ, Sweeney KJ, Molloy AP, Hennessy E, Curran C, Kerin MJ (2008). The effect of menopause and hysterectomy on systemic vascular endothelial growth factor in women undergoing surgery for breast cancer. BMC Cancer 8:279. Crossref |
||||
|
Manders P, Beex LV, Tjan-Heijnen VC, Span PN, Sweep CG (2003). Vascular endothelial growth factor is associated with the efficacy of endocrine therapy in patients with advanced breast carcinoma. Cancer 98:2125-2132. Crossref |
||||
|
Masood MI, Qadir MI, Shirazi JH, Khan IU (2011). Beneficial effects of lactic acid bacteria on human beings. Crit. Rev. Micro. 37:91-98. Crossref |
||||
| Naz S, Qadir MI, Ali M, Janbaz KH (2012). Nanotechnology for imaging and drug delivery in cancer. J. Chem. Soc. Pak. 34:107-111. | ||||
| Nisar L, Qadir MI, Malik SA, Tabassum N (2011). Characterization of the immunodominant regions within gp41 of env gene of HIV in Pakistan. J. Chem. Soc. Pak. 33:545-548. | ||||
|
Oehler MK, Caffier H (2000). Prognostic relevance of serum vascular endothelial growth factor in ovarian cancer. Anticancer Res. 20(6D):5109-5112. Pubmed |
||||
| Qadir MI (2009). Medicinal and cosmetological importance of Aloe vera. Int. J. Nat. Ther. 2:21-26. | ||||
| Qadir MI (2010). Medicinal values of ginger. Int. J. Nat. Ther. 3:19-22. | ||||
|
Qadir MI (2011). Qadirvirtide. Pak. J. Pharm. Sci. 24:593-595. Pubmed |
||||
| Qadir MI, Malik SA (2009). Effect of Eugenia jambolana leaves extracts on blood glucose levels of experimental diabetic rabbits. Pharmacologyonline 3:829-835. | ||||
| Qadir MI, Malik SA (2010). Anti-diabetic activity of inorganic metals Eugenia jambolana Lam. (Myrtaceae) flowers. Pharmacologyonline 2:979-985. | ||||
|
Qadir MI, Malik SA (2011). Genetic variation in the HR region of the env Gene of HIV: A perspective for resistance to HIV fusion inhibitors. AIDS Res. Hum. Retrovir. 27:57-63. Crossref |
||||
|
Quaranta M, Daniele A, Coviello M, Venneri MT, Abbate I, Caringella ME, Di Tardo S, Divella R, Trerotoli P, Di Gennaro M, Schittulli F, Fransvea E, Giannelli G (2007). MMP-2, MMP-9, VEGF and CA 15.3 in breast cancer. Anticancer Res. 27(5B):3593-600. Pubmed |
||||
|
Riedel F, Götte K, Schwalb J, Wirtz H, Bergler W, Hörmann K (2000). Serum levels of vascular endothelial growth factor in patients with head and neck cancer. Eur. Arch. Otorhinolaryngol. 257:332-336. Crossref |
||||
|
Saleem M, Qadir MI, Perveen N, Ahmad B, Saleem U, Irshad T, Ahmad B (2013). Inhibitors of apoptotic proteins: New targets for anti-cancer therapy. Chem. Biol. Drug Desi. 82:243-251. Crossref |
||||
|
Salgado R, Vermeulen PB, Benoy I, Weytjens R, Huget P, Van Marck E, Dirix LY (1999). Platelet number and interleukin-6 correlate with VEGF but not with bFGF serum levels of advanced cancer patients. Br. J. Cancer 80:892-897. Crossref |
||||
|
Salven P, Mänpää H, Orpana A, Alitalo K, Joensuu H (1997). Serum vascular endothelial growth factor is often elevated in disseminated cancer. Clin. Cancer Res. 3(5):647-651 Pubmed |
||||
|
Salven P, Orpana A, Joensuu H (1999a). Leukocytes and platelets of patients with cancer contain high levels of vascular endothelial growth factor. Clin. Cancer Res. 5:487-491. Pubmed |
||||
|
Salven P, Perhoniemi V, Tykkä H, Mäenpää H, Joensuu H (1999b). Serum VEGF levels in women with a benign breast tumor or breast cancer. Breast Cancer Res. Treat. 53:161-166. Crossref |
||||
|
Sato K, Tsuchiya N, Sasaki R, Shimoda N, Satoh S, Ogawa O, Kato T (1999). Increased serum levels of vascular endothelial growth factor in patients with renal cell carcinoma. Jpn. J. Cancer Res. 90:874-879. Crossref |
||||
|
Stockhammer G, Obwegeser A, Kostron H, Schumacher P, Muigg A, Felber S, Maier H, Slavc I, Gunsilius E, Gastl G (2000). Vascular endothelial growth factor (VEGF) is elevated in brain tumor cysts and correlates with tumor progression. Acta Neuropathol. 100:101-105. Crossref |
||||
|
Takano S, Yoshii Y, Kondo S, Suzuki H, Maruno T, Shirai S, Nose T (1996). Concentration of vascular endothelial growth factor in the serum and tumor tissue of brain tumor patients. Cancer Res. 56:2185-2190. Pubmed |
||||
|
Tuttle RM, Fleisher M, Francis GL, Robbins RJ (2002). Serum vascular endothelial growth factor levels are elevated in metastatic differentiated thyroid cancer but not increased by short-term TSH stimulation. J. Clin. Endocrinol. Metab. 87:1737-1742. Crossref |
||||
|
Verheul HM, Hoekman K, Luykx-de Bakker S, Eekman CA, Folman CC, Broxterman HJ, Pinedo HM (1997). Platelet: transporter of vascular endothelial growth factor. Clin. Cancer Res. 3:2187-2190. Pubmed |
||||
|
Weindel K, Moringlane JR, Marmé D, Weich HA (1994). Detection and quantification of vascular endothelial growth factor/vascular permeability factor in brain tumor tissue and cyst fluid: the key to angiogenesis? Neurosurgery 35:439-448. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


