ABSTRACT
Adequate dietary intake is important in achieving optimal nutrition and health for people before and during treatment of HIV. Inadequate nutrition causes health issues and fatalities among prisoners. Thus, this study assesses dietary intake and factors affecting food service among male prisoners living with HIV at selected prisons in Kenya. A cross sectional analytical study design was adopted on a sample of 113 male prisoners living with HIV, randomly sampled from 4 prisons. Data collection tools included a structured questionnaire used to collect demographic, 24 h recall and food frequency data. During data analysis, 24 h recall data was analyzed using Nutri-survey software, and further analysis via SPSS software. Results revealed that slightly more than half the prisoners (50.4%) were aged 36-53 years. Primary education was attained by 60.2% and secondary education by 21.2%. Mean dietary intake for macronutrients was: Energy (1815±218 Kcal), Protein (56±12 g), fat (32±6 g), Carbohydrates (322±45 g), Fiber (41±23 g) and PUFA (8±1 g). None attained Recommended Daily Allowances (RDA) for energy, fat and PUFAs. Mean key micronutrients were: Vitamin A (1195.1±812.7), Vitamin B6 (1.9±0.9), Vitamin C (55.7±18.4), Iron (10.2±2.7), Magnesium (488.1±152.3) and Zinc (13.9±6.7). None met RDA for Iron. Therefore, provision of a nutritionally balanced diet in prisons can ensure nutrients adequacy.
Key words: Dietary intake, food service, prisoners living with HIV.
Prisoners are a population that is recognized as vulnerable and socially excluded (Condon et al., 2008). Imprisonment is high in many countries, resulting in overcrowding and increased prevalence of health problems, which should make prison health a priority (van den Bergh et al., 2011). Sub-Saharan Africa is the hardest hit by the HIV epidemic with almost two thirds of all people infected with HIV living in the region. HIV prevalence among prisoners in sub Saharan Africa prisons has been estimated at 2-50 times the prevalence in non-prison populations (UNAIDS/WHO, 2008). The high HIV prevalence in prisons could be attributed to high risk behaviors which include incidences of rape and other forms of non-consensual sex and drug injection (Jürgens et al., 2011). HIV and AIDS is associated with biological and social factors that affect the individual’s ability to acquire, consume and utilize food and these factors lead to poor nutrition status and weight loss, which are both critical in causing morbidity in individuals infected with HIV, resulting in poor quality of life (Hendricks et al., 2008).
Lack of sufficient food has been shown to compromise retention of PLHIV in care and treatment programs, as well as adherence to anti-retroviral therapy (ART) (Maluccio et al., 2015).
Prisoners incarcerated in developing countries have been shown to be vulnerable to dietary deficiencies (Gould et al., 2013). The diet of the prisoners is usually inadequate nutritionally and places them at higher risk of developing acute and chronic nutritional deficiency diseases. However, in some incidences prisoners may benefit from additional food ration from their families and visitors but the majority of prisoners remain nutritionally inadequate (Qadir et al., 2014). Appropriate nutrition should be considered as one of prisoners’ basic human rights, for many of them have poor health. The quantity and quality of food available in a prison helps maintain and improve prisoners’ health, which plays a major role in determining the quality of a prisoner’s life (Gould et al., 2013).
Providing and ensuring safe and healthy food supply in prisons will prevent nutrient deficiency diseases and promote better overall health of prisoners, hence promoting drug adherence (Edwards and Reeve, 2008). Food is a fundamental need and the ability to choose what to eat and to prepare one's own food should be a right for all people, including prisoners and all essential food groups should be represented in sufficient quantities in the food supplied to prisons, so that detainees can benefit from a balanced and varied diet (Kjaer, 2014). Few studies (for example, by Human Rights Watch, 2006) have focused on general prison conditions and prevalence of HIV pandemic; hence, paucity of data on dietary intakes and factors affecting food service of prisoners living with HIV. The aim of this study is to investigate the dietary intake and factors influencing food service of male prisoners living with HIV at selected prisons in Kenya.
A cross-sectional analytical study design was done in 2015 in four purposively selected Kenyan male prisons (Naivasha, Nyeri, Meru and Kakamega). The target population was male prisoners living with HIV who were randomly selected. Only respondents who met the inclusion criteria of confirmed HIV positive status, on care and/or treatment, remand awaiting trial or convicted were included in the study. A total of 113 prisoners were sampled. A structured questionnaire was used to collect socio-demographic data. Dietary intake was collected by use of a validated 24-h dietary recall and 7-day food frequency questionnaire (FFQ). The 24-h food recall was used to determine the approximate amounts of nutrients consumed, while the food frequency questionnaire was used to gather information on habitual intake of a range of foods. Dietary data was analyzed by use of Nutri-survey software and exported to SPSS for cross-analysis. The amount of nutrients consumed per day was then compared with the Recommended Daily Allowances (RDAs) to determine dietary adequacy. The food frequency data was analyzed based on seven food groups to determine how often each of the food was consumed in a 7-day period and what proportion of the study population consumed it. Chi-square tests were performed to establish the relationship between categorical variables (socio-demographic and dietary intakes). A p-value Ë‚0.05 was considered significant. Descriptive statistics was used to describe and summarize socio-demographic characteristics data of male inmates living with HIV.
Logistical and ethical considerations
Before embarking on data collection, ethical approval was obtained from the University’s Ethical Review Committee. Research permit was obtained from National Commission for Science Technology and Innovation (NACOSTI). Further, a permit to do research in prison was sought from training and development department at prison headquarters. Verbal and written consent was obtained from the study participants after a thorough explanation of study purpose. Participants were informed that all information and data obtained from them would be kept confidential by use of codes instead of personal identifiers. The researchers ensured that participants received full disclosure and understood the nature and benefit of the study and equitable selection of participants was ensured.
Socio-demographic characteristics of respondents
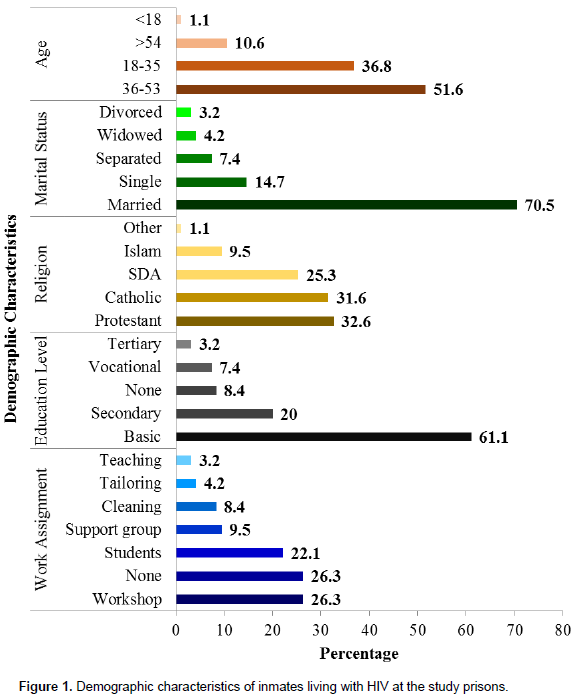
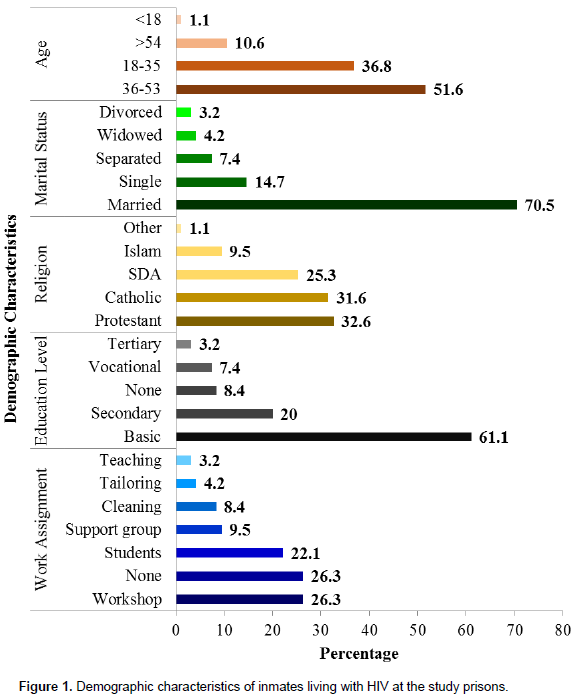
Slightly more than half (51.6%) of the respondents were aged between 36 - 53 years. This group constituted the biggest cohort of those sampled. Results showed that 70.5% of respondents were married, while 14.7% were single. Christianity (Catholic, SDA, and Protestant) was the most common religion, followed by Islam. More than half (61.1%) of the respondents had attained primary school education, followed by secondary education (20%). A meagre 8.0 and 3.0% had attended vocational training and tertiary education respectively (Figure 1). More than half of the prisoners had some duties assigned (51.6%) to them and 23.6% had no work assigned to them.
Dietary intake
Macronutrient intake
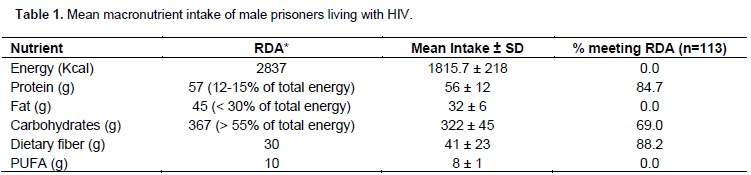
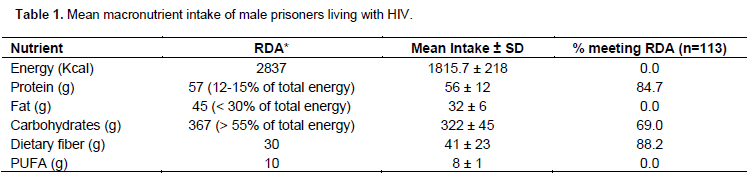
Assessment of macronutrients intake showed a mean energy intake of 1815.7 ± 218 Kcal. per day, and mean carbohydrates intake of 322 ± 45 g per day per prisoner. Recommended daily allowance (RDA) for protein was met by 84.7% of the respondents, while carbohydrates and dietary fiber requirements were met by 69.0% and 88.2% of the respondents respectively. None of the respondents met the RDA for energy, fat and PUFAs (Table 1).
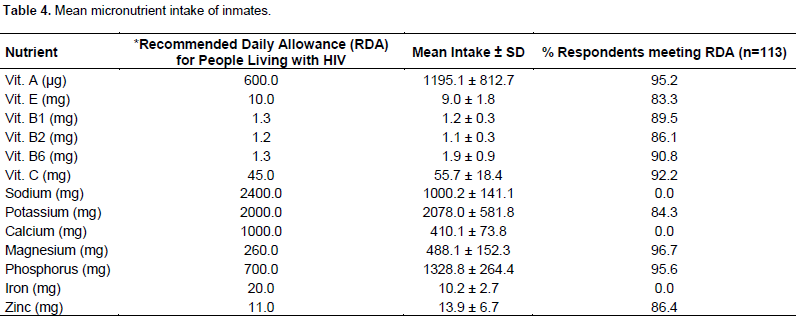
Macronutrient intake by prison
The study further established macronutrients intake per prison using data from the 24 h food recall (Table 3). The study established that in specific prisons, none of the prisoners met the energy, fat and PUFA RDA. The study also ascertained that it was only Naivasha and Kakamega prisoners that met their RDA for protein, carbohydrates and fiber at 100%. Only 68.7 and 39.4% of prisoners in Meru and Nyeri respectively met RDA for protein, with only 72.4 and 79.5% in the same prisons meeting Fiber RDA.
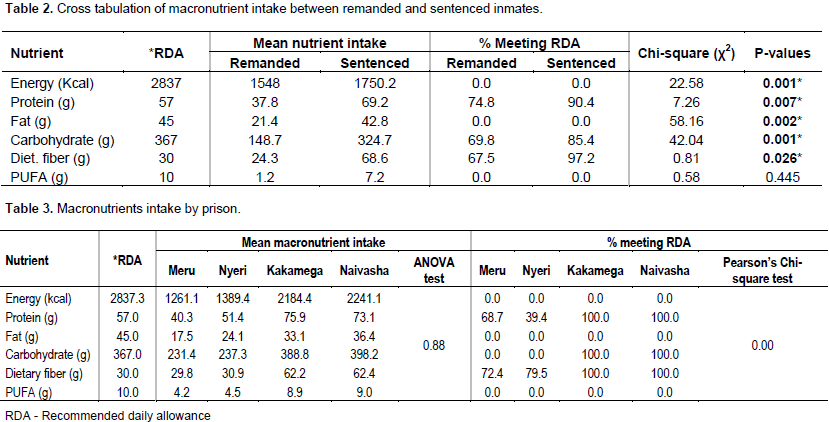
Dietary intake between remanded and sentenced inmates
The study established that remanded and sentenced inmates had different food ration prescriptions. The intakes were therefore evaluated to ascertain whether any significant difference existed (Table 2). Evaluation uncovered significant associations (P<0.05) between dietary intake and nature of custody, although neither of the two categories met RDA requirements for energy, fat or PUFAs.
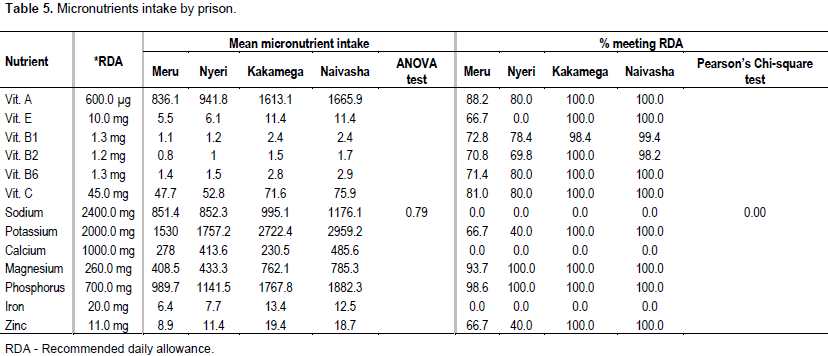
Dietary intake for micronutrients
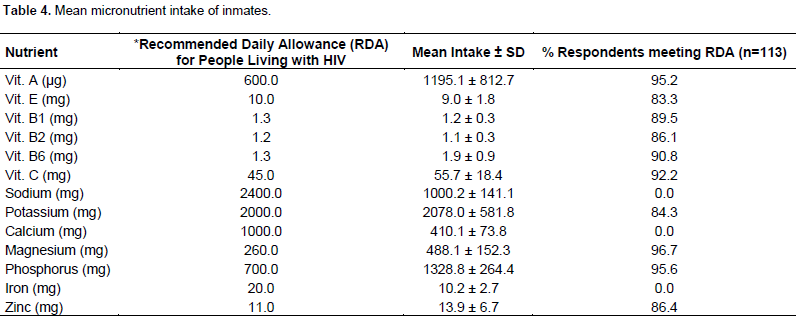
Micronutrients through 24-h food recall revealed that the RDA for Vitamin A, B6, C, Magnesium and Phosphorus was met by over 90% of the respondents. While Vitamin E, B2, Potassium and Zinc was equally met by a high number of prisoners, 84.3 and 86.4% respectively. However, none of the respondents met the RDA for Sodium, Calcium and Iron in the 24-h food recall conducted (Table 4).
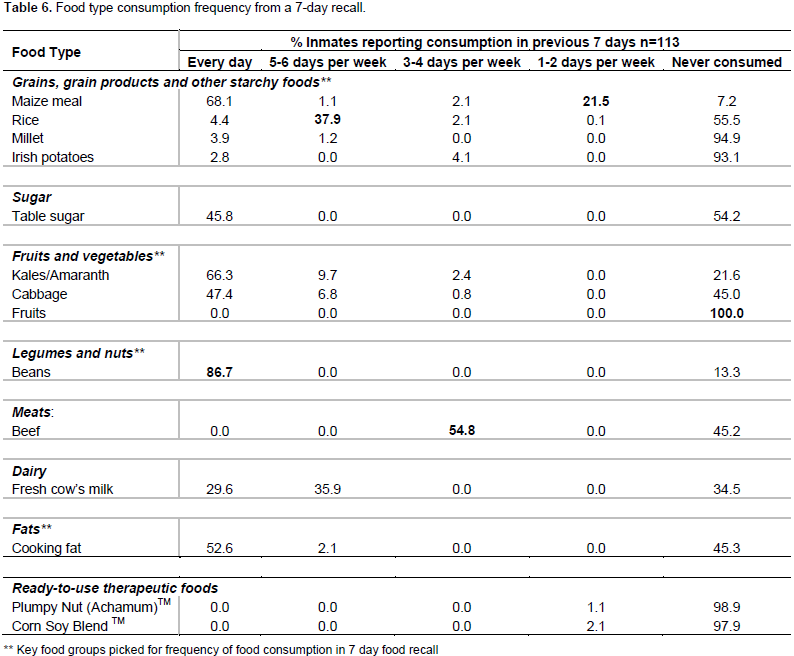
Micronutrient intake by prison
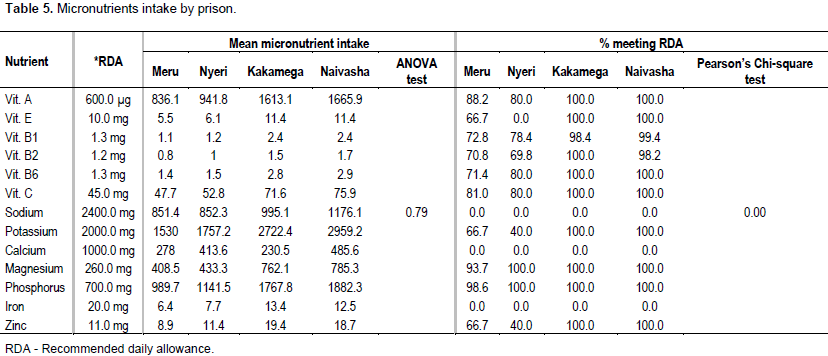
Micronutrients intake by respondents per prison was determined using data from the 24-h food recall (Table 5). The study showed that inmates at Kakamega and Naivasha prisons met their RDA for Vitamin A, E, C and B6. Respondents in the two prisons also met RDA for Potassium, Magnesium, Phosphorus and Zinc. However, not all the prisoners in the four prisons met the RDA for Vitamin B1 (Meru 72.8%, Nyeri 78.4%, Kakamega 98.5% and 99.4%). Naivasha prisoners met the RDA for Vitamin B2 unlike Meru, Nyeri and Kakamega prisons that did not have all their prisoners meet the RDA at 70.8, 69.8 and 98.2% respectively. Nyeri prisoners met RDA for Vitamin B6, Magnesium and Phosphorus while none of the prisons met the RDA for Sodium, Calcium and Iron. Meru and Nyeri prisoners did not fully meet the RDA for most of the micronutrients except for Vitamin B6, Magnesium and Phosphorus at Nyeri prison only, but not Meru. At Meru prison, none of the micronutrient’s RDA was met by all the respondents and were all below 100% with highest being Vitamin A at 88.2%, Magnesium 93.7% and Phosphorus at 98.6%. Nyeri prison had the lowest number of prisoners who attained RDA for Vitamin E, B2 and Potassium (Table 5).
Food consumption
Seven day food frequencies of inmates
The food frequency was based on 7 food groups (Table 6) and at least a food item from each group was consumed daily in the previous 7 days with the exception of beef and fruits. Beef was served to the inmates three times per week, but no fruits were consumed. Intake of supplementary foods (SF) (Achamum-2.1% and CSB-2.1%) was reported by some inmates at Naivasha and Nyeri GK prisons. The SF had been provided as a donation from Kenya Prisons Service headquarters.
Frequently consumed food
Beans were the most frequently consumed food type (86.7%), sometimes twice a day. The other most consumed foods were Kales at 66.3% and Maize meal at 68.1%. Milk was not consumed at all by 29.6% of the respondents while 47.4% did not consume cabbages. Table sugar and cooking fat consumption were reported by 45.8% and 52.6% respectively of the respondents. The prisoners reported having consumed Achamum and Corn Soy Blend porridge once in the week.
Factors that determine food service
Through focus group discussions, factors that determine food service were established and how each contributed to the food service status at the prisons. These included; morbidity status, prison set menu (ration), food preparation and hygiene, food distribution among prisoners, diet prescriptions, seasonality and market prices, prison’s administration initiatives, prisoners’ population at a time. These factors in one way or another informed the decision regarding food service in the study prisons.
Demographic and socioeconomic characteristics of inmates in the study prisons
Social determinants of health are wider set of forces and systems that shape the conditions of life. These include demographic, socioeconomic characteristics, religion, marital status and health outcomes whose influence has notable impact (WHO, 2010). Socioeconomic status (SES) is often measured as a combination of education, income and occupation. It is commonly conceptualized as the social standing or class of an individual or group. Furthermore, an examination of SES as a gradient or continuous variable reveals inequities in access to and distribution of resources. In this study, majority of respondents’ age was between 36 - 53 years. More than half were married and had attained primary education. Christianity was the most dominant followed by Islam. The results of this study concurs with one by Thapa et al. (2015) in Nepal prisons that found the mean age of the population to be 36.2 years and majority married.
Similarly, a higher number of prisoners in Nepal had completed primary level education and Christianity was one of the majority religions after Hinduism and Buddhism, followed by Islam hence this concurs with this study. HIV is a disease that strongly relates with social and economic inequity and it affects those of lower socioeconomic status at a disproportionately high rate. Furthermore, SES is a key factor in determining the quality of life for individuals after they are affected by the virus. Those with fewer resources are often left with limited treatment options. In Kenyan prisons, the demographic and socioeconomic factors may not influence dietary intake as prisoners have no influence on the already set menu and no food is allowed in the prison from family members. Religion likewise did not dictate what a prisoner ate or did not eat because of limited food choices available within the prisons.
Dietary intake
Nutritional needs of PLHIV are influenced by several factors including age, physiological changes, level of physical activity and an individual’s clinical state of health (including the metabolic rate and viral load count). The human body expends energy, even when resting. Infections, including HIV and AIDS, increase the body’s energy needs depending on the severity of the infection. Basically, PLHIV’s energy needs increase with the progression of the disease, especially during episodes of opportunistic infections. The fundamental concerns are to maintain a balance of foods from each food group, and to consume a variety within each food group daily. This study’s findings revealed that none of the respondents met the RDA for energy for a male adult living with HIV, Fat and PUFA. More than three quarters of the prisoners met the RDA for protein and dietary fiber with fewer meeting that of carbohydrates. However, a study done in selected prisons in Tanzania by Mwakyoso (2013) revealed that energy intake for prisoners living with HIV was high above the WHO recommended daily allowances but protein intake was below RDA.
Another related study in Papua New Guinea found out that energy intake for prisoners was below the recommended daily allowance (Gould et al., 2013) while another in UK also revealed that energy intake for prisoners was within the recommended daily allowances, protein above and carbohydrates within the RDA (Edwards and Reeve, 2008). This could be explained by the fact that Kenyan prisons hold population capacities that are higher than recommended with an occupancy level of 343.7% (Walmsley, 2008). This makes food service difficult because standard measure of food is not guaranteed. Due to these high populations, a prisoner is forced to eat what ‘falls’ in their plate regardless of the amount. According to the prison Menu, prisoners took only 3 meals in a day, hence it is common knowledge that many energy gaps in a person living with HIV are filled by snacks in between meals. In this study, protein intake was below the RDA despite daily consumption of beans, milk and meat thrice a week. Similarly, carbohydrates, fat and PUFAs consumption was below the recommended daily allowance and this could have been contributed by the amounts of these foods taken at a given serving and lack of variety.
In all the prisons, the only cereals consumed were maize, rice and millet which was being consumed by few prisoners who were on special diet as per prison standards. High dietary fiber above the recommended daily allowance in the 3 GK prisons could be attributed to the use of whole meal maize flour in all the 3 meals in a day. This concurs with a study in Australian prisons where fiber intake was more than adequate (Williams et al., 2009). Fat in prison was not cooked with food but boiled and distributed differently to prisoners. The amounts were very small to meet the RDA, e.g. in one prison, 330 g of fat was shared among 175 prisoners, which translates to approximately 2 g in a meal per person. The intake of vitamin E that is fat soluble in this study was below the average as per the recommended daily allowance, which concurs with a study in Papua New Guinea (Gould et al., 2013). Findings from this study were that Vitamin B2 was within the recommended levels, whereas Vitamins A, B6 and C were above the RDA hence similar with those of a research done by William et al. (2009) in Australian prisons. However, this study differed with the study in Papua New Guinea whose findings were that vitamin A, riboflavin, vitamin C was below the RDA (Gould et al., 2013).
In this study, Potassium, Phosphorus, Zinc and Magnesium were above the estimated RDA and these results concur with findings from a related study in England by Edwards and Reeve (2008). Sodium, Calcium and Iron were found to be lower than RDA in this study; findings that concurs completely with a study by Gould et al. (2013) in Papua New Guinea prisons. Low failure to meet the RDA for Calcium in Kenyan prisons could be associated with low consumption of milk and bone soup in prisons. The study noted that not all prisons provided milk for prisoners living with HIV and those that provided it was not equally distributed among the intended population. Bone soup was not equally available to all the prisoners because it was not adequate and still it was not specific to prisoners living with HIV. Iron rich foods in prison equally were not adequately taken hence levels below RDA. Meat was taken 3 times a week, vegetables daily and yet the 24-h food recall revealed low Iron intake.
Many prisoners ended up being served with vegetable soup instead of the vegetables because of the large prison population and the quick food service exercise whereby only what the spoon scooped was served regardless of the quantity. The fundamental concerns in HIV are to maintain a balance of foods from each food group, and to consume a variety within each food group daily. In this study none of the respondents met the RDA for energy for a male adult living with HIV, Fat and PUFA. More than three quarters of the prisoners met the RDA for protein and dietary fiber with fewer meeting that of carbohydrates. This makes food service difficult because standard measure of food is not guaranteed. Due to high populations, a prisoner is forced to eat what ‘falls’ in their plate regardless of the amount. According to the prison menu, prisoners took only 3 meals in a day, hence it is common knowledge that many energy gaps in a person living with HIV are filled by snacks in between meals.
Factors that determine food service
In this study, several factors played a role in determining diet and food service in all the prisons. These factors were uniform across the four prisons. They included:
Morbidity status: This led to elimination/inclusion of irritating food and prescribed food respectively. According
to a study in a Texas prison, prison inmates’ exhibited poorer overall health status than the general population, which in turn affected their feeding, and thereafter nutrition status (Baillargeon et al., 2007).
Food preparation and hygiene: In all the prisons, food was prepared by selected prisoners. Many inmates and wardens felt that hygiene was poor and food was not washed as it should hence this could have been a contributing factor to some illnesses reported in this study, e.g. diarrhea and typhoid. This concurs with a study in US which noted that most food contamination through unhygienic conditions occur at large food service area resulting in food-borne diseases (Judy et al., 2007).
Food distribution among prisoners: Food distribution in prison was dependent to some extent on the length of stay in the prison. This could in turn affect the nutritive value of food and consequently the nutrition status. This study concurs with one in a Cote d’Ivoire prison, whose findings were that penal rations did not provide the necessary nutrient intake recommended according to international standards and this varied among prisoners (Ahoua et al., 2007). A study in the US found that it was impracticable to vary the quantities for each individual according to his need in a prison set up (Carpenter, 2006).
Seasonality and market prices: This factor played a major role in prisons the same as in the general population, especially vegetables used in prison dependent on seasonality. For example, some prisons served cabbage while others served kales depending on what was in season and low priced in that region. This concurs with a study in US which suggested that the higher cost of healthier foods could be a deterrent to eating healthier among populations (Story et al., 2008). This can be explained better in this study by the fact that there is no much diet diversification in prisons, which is majorly attributed to budgetary constraints.
Prison’s administration initiatives and set menu: Kenya’s prisoners do not have an alternative diet apart from the prison diet unlike Western prisons where inmates are allowed to buy food from prison canteens. This therefore left them at the mercies of the prison administration to improve on quality and diversity of their diets. Despite few modifications on the diet, there were set prison menus that must be strictly followed. These finding concur with a study in England that prisoners were often prevented from making healthy choices by the prison setting and barriers exist within the prison setting, which limited the ability of prisoners to maintain and improve their health and more specifically nutrition status (Condon et al., 2007). These finding however differed from a study in the UK which noted that UK prison menu had over the years changed from Ration Scale to a pre-select menu system (Edwards and Reeve, 2008). In Kenya, the Ration Scale was strictly in use as per the laid down rules and regulations.
Prisoners’ population at a time and diet prescriptions: All the 4 prisons had a population higher than the set limit for prisoners, which was not unique as this is common in most prisons all over the world. This made it difficult to serve food equally to every prisoner hence some ended up with more or less than the other. Some even ended up missing on a type of food because of the haste of the exercise and high number of people who shared the same food. For example, some ended up with vegetable soup without the vegetables or beans soup without the beans. This study concurs with a study in Cote d’Ivoire, which found that penal rations were inadequate and therefore systematic food supplementation with vitamins and micronutrients should be considered (Ahoua et al., 2007).
Article 43 of the constitution establishes Kenyans’ right “to be free from hunger and have adequate food of acceptable quality”. This aspect also applies to prisoners who are citizens of the country. Prisoners feed on only 3 meals a day hence difficult to meet the nutritional requirements of a person living with HIV. Normally, the energy requirements of a PLHIV are filled by 2 extra snacks in a day, which is lacking in these prisons. Food service in this study was determined by several factors which are constant and did not allow for a lot of flexibility. This study showed that food provided by the prison authorities was the major dietary source for majority of prisoners. Regarding the quality of food, majority of inmates complained of uneven portions and some not even getting particular foods at all. However some prisons must be commended for their initiative to provide additional food items besides the existing set menu.
Prison management should consider increasing nutritional balance and choice of food provided by the kitchen through dietary diversity since there is no food allowed from outside. The study noted low intakes of important micronutrients e.g. Iron, Calcium and Sodium hence supplementation can also be considered.
RECOMMENDATIONS FOR POLICY
1. The Ministry of Health should formulate policies that address nutritional requirements of prisoners as part of the Most At Risk Populations (MARPs) and that of interior and coordination of national government provide the resources required for implementation.
2. The prison administration should review the existing menu to ensure recommended dietary allowances for all nutrients are met which was not the case at the time of study.
The authors are thankful to the respondents for their time and willingness to participate in this study and also appreciate the prison administration for their support during the study period.
REFERENCES
|
Adams EJ, Grummer-Strawn L, Chavez G (2003). Food insecurity is associated with increased risk of obesity in California women. J. Nutr. 133(4):1070-1074.Ahoua L (2007). Outbreak of beriberi in a prison in Côte d'Ivoire. Food Nutr. Bull. 28(3):283-290.
|
|
|
|
Baillargeon J, Black SA, Pulvino J, Dunn K (2007). The Disease Profile of Texas Prison Inmates. Annals Epidemiol. 10(2):74-80.
Crossref
|
|
|
|
|
Carpenter KJ (2006). Nutritional studies in Victorian prisons. J. Nutr. 136(1):1-8.4.
|
|
|
|
|
Condon L, Hek G, Harris F (2008). Choosing health in prison: Prisoners' views on making healthy choices in English prisons. Health Educ. J. 67(3):155-166.
Crossref
|
|
|
|
|
Condon L, Hek G, Harris F, Powell J, Kemple T, Price S (2007). Users? views of prison health services: a qualitative study. J. Adv. Nurs. 58(3):216-226.
Crossref
|
|
|
|
|
Edwards JS, Hartwell HJ, Reeve WG, Schafheitle J (2007). The diet of prisoners in England. Bri. Food J.109(3):216-232.
Crossref
|
|
|
|
|
Gould C, Tousignant B, Brian G, McKay R, Gibson R, Bailey K, Venn BJ (2013). Cross-sectional dietary deficiencies among a prison population in Papua New Guinea. BMC Int. Health Human Rights 13(1):21.
Crossref
|
|
|
|
|
Hendricks KM, Mwamburi DM, Newby PK, Wanke CA (2008). Dietary patterns and health and nutrition outcomes in men living with HIV infection. Am. J. Clin. Nutr. 88(6):1584-1592.
Crossref
|
|
|
|
|
Human Rights Watch (2006). Human Rights Watch | HIV/AIDS in Prisons. Available at:
View.
|
|
|
|
|
Judy D. Greig, Ewen C.D. Todd, Charles A. Bartleson, Barry S. Michaels (2007). Outbreaks Where Food Workers Have Been Implicated in the Spread of Foodborne Disease. Part 1. Description of the Problem, Methods, and Agents Involved. Available at:
View
|
|
|
|
|
Jürgens R, Nowak M, Day M (2011). HIV and incarceration: prisons and detention. J. Int. AIDS Soc.14(1):26.
Crossref
|
|
|
|
|
Kjaer Minke L (2014). Cooking in prison – from crook to cook. Int. J. Prisoner Health 10(4):228-238.
Crossref
|
|
|
|
|
Maluccio JA, Palermo T, Kadiyala S, Rawat R (2015). Improving Health-Related Quality of Life among People Living with HIV: Results from an Impact Evaluation of a Food Assistance Program in Uganda. PloSOne 10(8):e0135879.
Crossref
|
|
|
|
|
Mwakyoso ML (2013). Nutritional assessment of prisoners living with HIV/AIDS in selected prisons in Tanzania (Doctoral dissertation, Sokoine University of Agriculture.) Qadir M, Murad R, Qadir A, Mubeen SM (2014). Prisoners in Karachi–A Health and Nutritional Perspective. Annals Abbasi Shaheed Hospital Karachi Medical Dental College19(2).
|
|
|
|
|
Thapa R, Amatya A, Pahari DP, Bam K, Newman MS (2015). Nutritional status and its association with quality of life among people living with HIV attending public anti-retroviral therapy sites of Kathmandu Valley, Nepal. AIDS Res. Ther. 12(1):1.
Crossref
|
|
|
|
|
UNAIDS/WHO (2008). Report on the Global AIDS epidemic.
|
|
|
|
|
Van den Bergh BJ, Gatherer A, Fraser A, Moller L (2011). Imprisonment and women's health: concerns about gender sensitivity, human rights and public health. Bull. World Health Organization 89(9):689-694.
Crossref
|
|
|
|
|
Walmsley R (2008). World prison population list, 8th edition. London: International Centre for Prison Studies; (2008). Available at:
View
|
|
|
|
|
Williams P, Walton K, Hannanâ€Jones M (2009). Prison foodservice in Australia –systems, menus and inmate attitudes. J. Foodservice 20(4):167-180.
Crossref
|
|
|
|
|
World Health Organization (WHO) (2010). Discussion Paper Series on Social Determinants of Health No. 2, Geneva, Switzerland. P 24.
|
|
. Evaluation uncovered significant associations (P<0.05) between dietary intake and nature of custody, although neither of the two categories met RDA requirements for energy, fat or PUFAs.)