ABSTRACT
The coexistence of both under nutrition and over nutrition or known as double burden of malnutrition (DBM) is a recent emerging nutritional problem documented in most developing countries. In Ethiopia, though there are various studies documenting the magnitude of under-five children nutritional problem, there is a research gap on DBM among adolescents. To fill the identified gap, the extent of the problem among in-school adolescents was assessed. A school based, cross-sectional study was conducted among 634 high school adolescent students in Arba Minch town, Southern Ethiopia from March 2015 to April 2015. Multi-stage sampling was employed to select the sampled participant. Following the school stratification by ownership as governmental and private, two schools were randomly selected from each category and the number of students were allocated proportionately. A pre-tested structured questionnaire was used to collect socio-demographic and anthropometric measurements. Weight, height, waist circumference and hip circumference measurements were taken from all participants using standard procedures. Data were entered into EPI-info version 7 and analyzed using SPSS, version21. The anthropometric data were converted into nutritional indices using WHO Anthro-Plus software, version 1.0.4. Both bivariate and multivariate analyses were done using multinomial regression model. A total of 406 from the government and 228 from the private schools were enrolled in the assessment. The magnitude of underweight, and overweight and/or obesity were 19.7% (95%CI: 16.5%, 23.2%), and 11.2% (95%CI: 8.7%, 13.7%), respectively. Father educational and occupation status, family size and wealth index were significantly associated with underweight. The odds of being underweight among whose fathers’ had no formal education was 12 times [AOR=12; 95% CI=4 to 34], higher than those whose education level was above secondary. Those from family size of five or less were 80% times less likely to be underweight [AOR=0.2; 95% CI=0.12 to 0.4] than those whose family size was more than 5. Participants whose fathers’ occupation was merchant were 75% times less likely to be underweight than private work [AOR=0.25; 95%CI=0.09 to 0.6]. Wealth index quintile of lowest [AOR=9.4; 95% CI=3 to 29] and second [AOR=5; 95%CI=1.8 to14.9] were 5 times more likely to be underweight than their counterparts. This study revealed the coexistence of double burden of malnutrition among in-school adolescents. Parents’ education, family size and wealth index were some of the predictors which require the collaborative effort of health, education and social affair sectors to avert the prevailing problem in the community.
Key word: Magnitude, double burden of malnutrition, predictors, in-school community, rural Ethiopia.
The double burden of malnutrition (DBM) is an emerging nutritional problem of the coexistence of underweight, and overweight and/or obesity affecting adolescents from both affluent and poor countries. The DBM recognizes that under nutrition early in the life course contributes to an increased tendency for overweigh/obesity in adulthood. At the individual level the most common form of DBM seems to be excess energy consumption and iron deficiency. At the population level women are most affected by DBM, with most countries having more overweight than underweight women (James et al., 2000). The magnitude of overweight and obesity in children is increasing worldwide, and currently 1 child in 10 is overweight or obese (Hazbun et al., 2009). Results of longitudinal study in United State suggest that obese adolescents are likely to stay obese into adulthood and among individuals who were obese as adolescents, incident of severe obesity is 37.1% in men and 51.3% in women (Suchindran et al., 2010). In lower-to middle-income countries, overweight co-exists with underweight and most of them are concentrated in urban areas and presents serious social and psychological impacts (Kelishadi, 2007).
According to the systematic review made in 2014 on global burden of disease, overweight and obesity attributed to 3.4 million deaths, 3.9% of years of life lost, and 3.8% of disability-adjusted life-years worldwide (Ng et al., 2014). In Africa, the DBM has become an emerging public health problem due to the increased access to energy-dense foods consumption and less strenuous jobs resulting into many people having a positive energy balance leading to overweight/obesity indicating a challenge for program and policy-makers in transitional countries (Garenne, 2010; Ziraba et al., 2009). A study conducted on changes in the prevalence of underweight and overweight/obesity in non-pregnant women of reproductive age (ages 15-49), and their main socio-demographic correlates in Addis Ababa using data from 2000, 2005 and 2011 Ethiopian Demographic and Health Surveys, revealed the prevalence of overweight/obesity rose significantly from 16.1 to 20.6%; while underweight decreased from 17.9 to 14.1% between 2000 and 2011 (Yibeltal et al., 2000).
Prioritizing one extreme of malnutrition over the other is difficult on a limited budget, but under nutrition, especially in children below the age of 5 years continues to be the main focus of research and health care spending. Overweight and obesity particularly in adolescents receives very little attention, and is difficult to quantify accurately in this age group due to rapid changes in best to deal with it. Examination of the two extremes of malnutrition in adolescents may provide insight into the growth and development, and a lack of consensus over which definition to use. As a result, there is limited understanding of the problem of dual burden and how nature of dual burden and how to direct prevention strategies, both for the immediate problem of adolescent underweight, and the rapidly increasing problem of adolescent overweight. Although several studies have been conducted on child malnutrition in Ethiopia (Yohannes et al., 2017; Megabiaw and Rahman, 2013; Amare et al., 2016), there is a research gap on the coexistence of the double burden of malnutrition among adolescents which presumably is central to the success of many public health agendas, including the Millennium Development Goals aiming to reduce child and maternal mortality and non-communicable diseases (World Health Organization, 2009; Organization, 2009). This study has attempted to fill the identified gap and provided evidences for some program initiatives.
Study design and population
Across-sectional study was conducted among in-school adolescents from March, 2015 to April, 2015 in Arba Minch town which is the capital city of GamoGofa zone and Arba Minch Zuria wereda, Southern Nation, Nationality and Peoples Region (SNNPR). Arba Minch is about 430 km South of Addis Ababa with a total area of 12, 581.4 km2 and has a highland and lowland areas characterized by an average annual rain fall of 1166 and 900 mm, respectively. According to the 2007 census, the town has a total population of 74,879 (Garenne, 2010)and nine high schools of which five were governmental (N=4036) and four were private (N=2267) schools with a total number of 6303 students enrolled in both categories of the school at the time of the study. Two schools from government namely Arba Minch (N=1085) and Chamo (N=1035); and the same number from private schools called Rohobot (N=210); Hibret (N=176) were randomly selected and the number of students required in each school was allocated proportionately.
Ethical consideration
An ethical clearance and official letter was obtained from the Research and Ethics Committee of School of Public Health, Addis Ababa University. Permission was secured from Arba Minch education office and the respective schools. Assent was obtained from children’s family through school director for participants below the age of 18 years and verbal consent was also obtained for willingness of adolescents aged 18 years and above and the right to withdraw from the study at any time was also communicated to all participants. All the interviews and anthropometric measurement
Were conducted in a private place by same sex interviewers. All were informed the data collection procedures have no harm and debriefed on the outcome of the anthropometric measurements.
Sample size determination and allocations
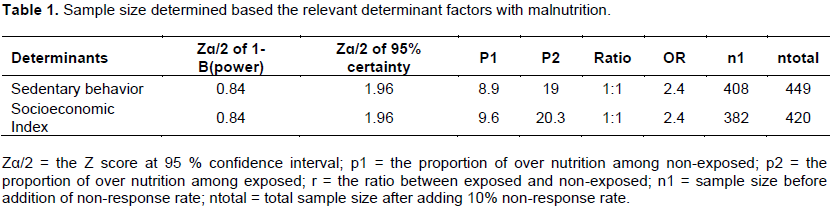
The required sample size was determined using single and two population formula to accommodate the objectives of the study. To determine the double burden of malnutrition (DBM) a magnitude of 15.0% of overweight (Teshome et al., 2013) and 20% of underweight (Cordeiro et al., 2012) with level of significance = 0.05; Marginal of error (d) = 0.04; Power of 80.0% and non-response rate= 10% yielded 337 and 423, respectively while to determine the determinants for DBM, proportion of two explanatory variables (sedentary behavior and wealth index proportions) identified for DBM in Hawasa study (Teshome et al., 2013) were used to estimate the respective sample sizes using the formula for comparisons of proportions and the estimated sample sizes are summarized in Table 1. With the inclusion of a design effect of 1.5 to the larger sample size calculated for the different study objectives the final sample reached 634, and allocated proportionately across the four schools randomly selected. To select the study participant, the schools were first stratified by ownership as governmental and private schools (Grades 9 and 10). The randomly selected schools from government and private schools were assigned the required number of students proportionately. Two sections from each grade of the respective schools were included and the total number of student allocated according to their grade level was 208, 198, 124 and 104 in Arba Minch, Chamo, Rohobot and Hibret, respectively.
Data collection
All regular students in apparent health that were present during the study period were enrolled in each section until the required sample size for the respective schools were reached. Data were collected using structured questionnaire adapted from the Global Physical Activity Questionnaire (GPAQ) Analysis Guide (Bull et al., 2009) and WHO steps instrument for chronic disease risk surveillance (WHO, 2012) and standard CDC anthropometric measurement protocols.
The measurement was conducted in a private place by an interviewer of the same sex. Three trained females and three males with BSc in public health, and 2 supervisors qualified with masters of public health with relevant experience were recruited and trained for two days on the method of the data collection. The training addressed issues such as the content of the questionnaire, basic interviewing skills, and taking anthropometric measurements.
Weight was measured by a digital scale to the nearest 0.1 kg, without shoes and minimum clothes while height was measured with portable stadiometer to the nearest 0.1 cm. The study participants stood upright on bare feet, with heels together, and buttocks and back touching the meter rule. Single measurements were taken in each case.
Waist circumference was measured to the nearest 0.1 cm with a non-elastic standard measurement tape. The measurement was taken parallel to the floor at the umbilical level, with study participants wearing no cloth around the waist area after expiration.
Hip circumference was measured as standing inter-trochanteric girth according to the WHO guidelines. Hip circumference (cm) was measured at the widest point around the greater trochanter to the nearest 0.1 cm.
Data quality management
To maintain the quality of the data, two days training was given to data collectors on the objective of the study, measurement procedures and ethical issues. The questionnaires were developed in English and then translated in to Amharic and review made for consistency of translation of the language. Pretest and demonstration of instrument was performed on 5% of the sample from nearby Arba Minch town of Merab Abaya high school. The collected data were checked for completeness and consistencies by the supervisors and the investigator. The scales were regularly checked and adjusted to zero after each measurement.
Data analysis procedures
Data collected were checked for completeness, coded, and entered using Epi-Info version 7 then exported to SPSS version 21 for cleaning and analysis. For computing the magnitude of malnutrition the data were exported to WHO-Anthro plus software version 1.0.4 and BMI for age and cut off points using WHO growth reference 2007, Mean and standard deviation (SD) were calculated. Accordingly, students were classified as under-weight when the BMI-for-Age Z-score (BAZ) was below minus 2SD; normal when BAZ was between minus 2SD and +1SD; overweight when BAZ was between +1SD and +2SD and Obese when BAZ was greater than +2SD. Waist-to-hip ratio (WHR) was calculated by dividing the waist size by the hip size.
A waist-to-hip ratio of 0.85 or greater for females and 0.90 or greater for male is the increased risks for heart disease and other ailments connected with being overweight whereas a waist-to-hip ratio of less than 0.90 for male and less than 0.85 for women, is considered as low risk (De Onis et al., 2007).
To explore the association between independent and outcome variables, crude odds ratio with 95% C.I was constructed using bivariate analysis. Multinomial logistic regression analysis was also used to determine the factors associated with extremes of malnutrition since the outcome variable has more than two categorical variables. Accordingly, adjusted odds ratios (AORs) with 95% CIs were estimated. All variables in the bivariate analysis were taken to the multinomial logistic regression model. Principal component analysis (PCA) was done to determine the wealth index in five categories. In all analyses, P< 0.05 was considered to be statistically significant.
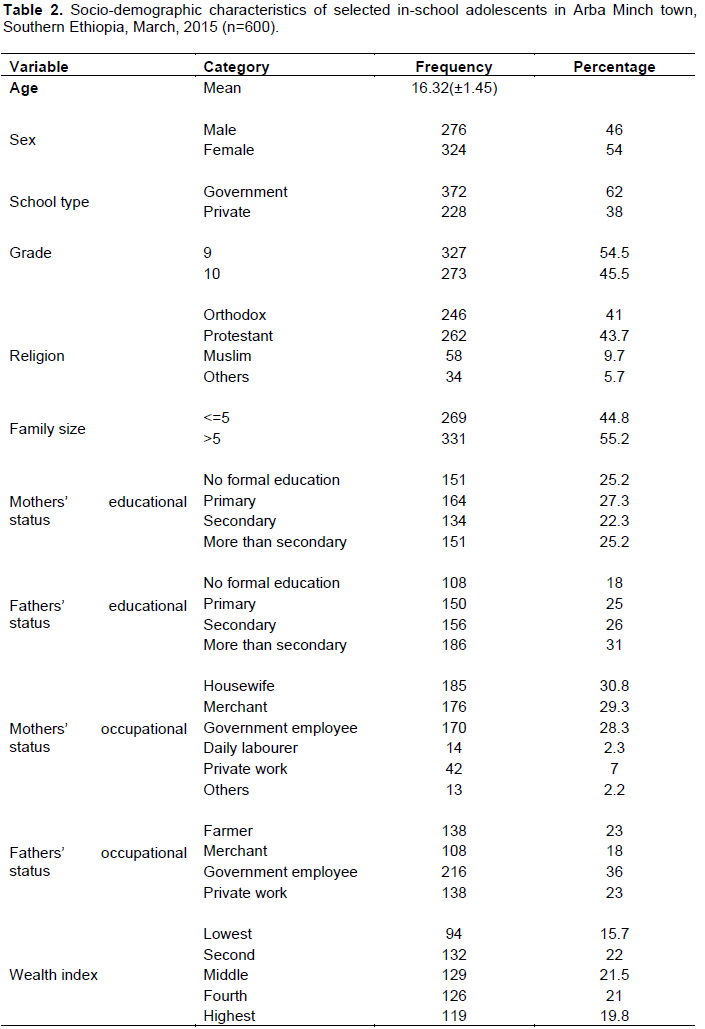
Of the 634 sampled students, 600 of them participated making the response rate 94.6%. Of these, 372 (62%) were from government and 228 (38%) were from private schools. The mean (±SD) age of the respondents was 16.32(±1.45) years ranging from 14 to 19 years. The majority (77.5%) reside in urban, 262 (43.7%) were protestant by religion. Of the 600 participants, 327 (54.5%) were grade nine and 273(45.5%) were grade 10 students. Educational status of parents’ of the participants revealed that 151(25.2%) mothers and 108(18%) fathers had no formal education. Over half (55.2%) were living in the family size of more than five. Slightly over one-third (36%) of participants fathers was government employee and 185 (30.8%) of mothers were housewives. As for wealth index quintile, 132(22%) and 129(21.5%) of them were from second and middle socio economic index category, respectively (Table 2).
Magnitude of malnutrition
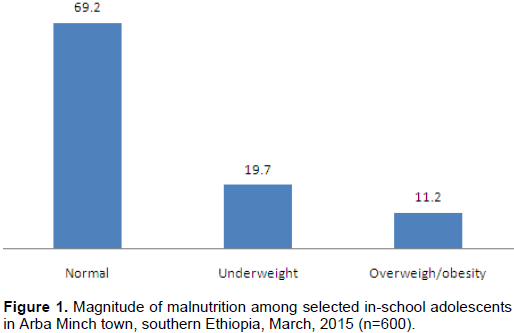
The overall proportion of underweight and overweight/obesity determined by BMI status was 19.7% (95%CI: 16.5%, 23.2%) and 11.2% (95%CI: 8.7%, 13.7%), respectively (Figure 1).
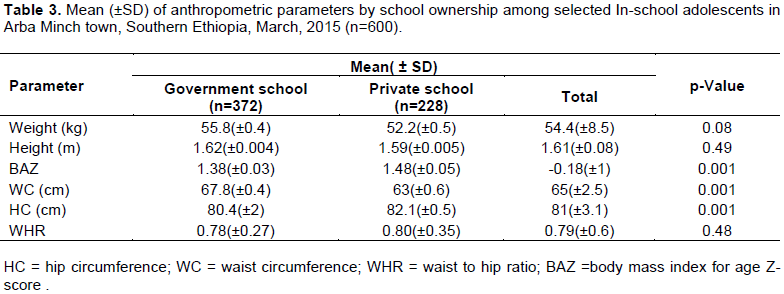
The mean Body mass index for age Z-score (BAZ) and hip circumference (HC) was significantly higher among private than the government schools while the mean WC was significantly higher in government than private schools. There were no significant differences in mean height, weight and waist hip ratio (WHR). The overall mean value of WHR for both schools was 0.79 cm which shows low risk for developing heart disease and other ailments connected with being overweight (Table 3).
Factors associated with double burden of malnutrition
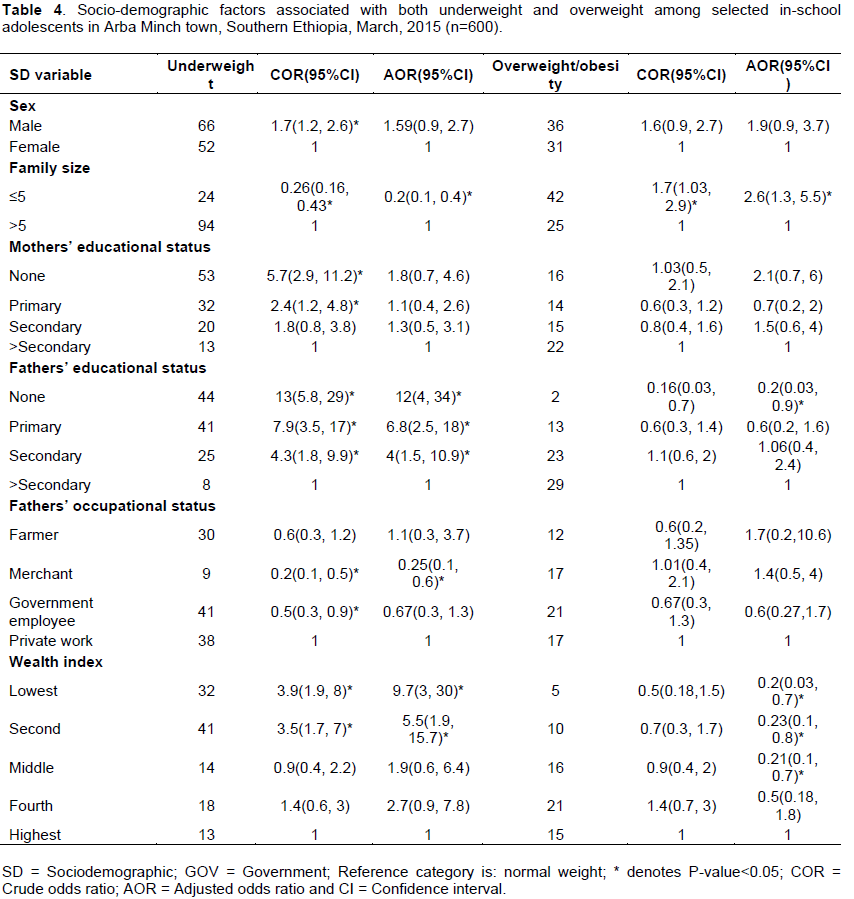
As shown in Table 4, sex, family size, parents’ education, fathers’ occupational and wealth index were significantly associated with the level of underweight. Being male was 1.7 times more likely to be underweight than girls [COR=1.7; 95%CI=1.2 to 2.6]. Respondents from family size of ≤5 were 74.0% times less likely to be underweight than the referent groups [COR=0.26; 95%CI= 0.16 to 0.43]. The odds of being underweight was 13 times more likely among respondents whose father educational status had no formal education [COR=13; 95% CI=5.8 to 29]; whose mother had no formal education were also 5.7 times more likely [COR=5.7; 95% CI= 2.9to11.2] to be underweight and those participants from lowest wealth index were 4 times more likely [COR=3.9; 95% CI= 1.9 to 8] to be underweight than the referent groups. Similarly father occupation of being merchant were 20.0% less [COR=0.2; 95% CI=0.1 to 0.5] and government employee were 50.0% less likely [COR=0.5; 95% CI= 0.3 to 0.9] to be underweight their counterparts. Nonetheless, the above associations were retained only for father education and occupation, family size and wealth index after controlling the confounding effect of other variables. The odds of being underweight among participants whose fathers’ had no formal education was 12 times more [AOR=12; 95% CI=4 to 34]; respondents whose family size of five or less were 80.0% times less [AOR=0.2; 95% CI= 0.12 to 0.4]; those whose fathers’ occupation was merchant were 75.0% times less [AOR=0.25; 95%CI=0.09 to 0.6] and wealth index quintile of lowest [AOR=9.4; 95% CI=3 to 29] and second [AOR= 5; 95%CI= 1.8 to14.9] were likely to be underweight than their counterparts.
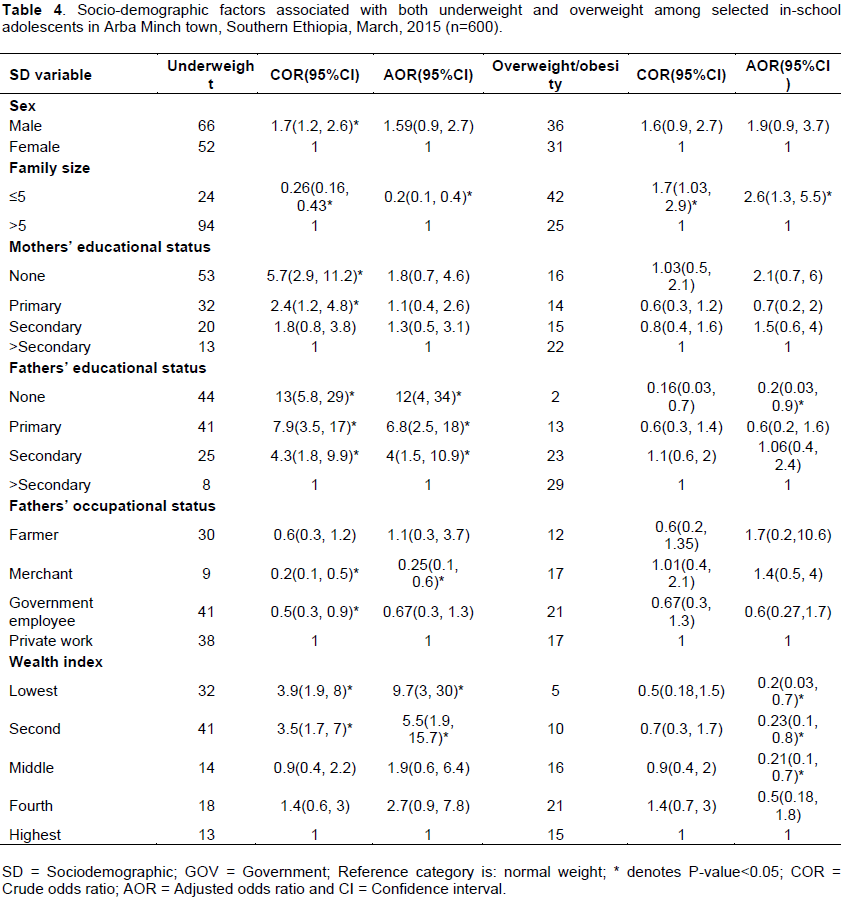
Similarly, family size, school type and grade level weresignificantly associated with overweight and/or obesity. Government school respondents were 60% times less likely to be overweight/obesity than private schools [COR=0.4; 95%CI=0.2 to 0.7]. The odds of being overweight/obesity is twice more among grade 9 students than grade 10[COR=2; 95% CI=1.1, 3.6)]. Participants from family size of 5 or less were 1.7 times more likely to be overweight than of family size more than 5[COR=1.7; 95%CI=1.03 to 2.9].
After controlling for the confounding effect of family size, wealth index quintile of lowest, second and middle, fathers’ education level of no formal education, mother occupation of being housewife and being grade 9 students remained significantly. Respondents whose family size of five or less were 2.6 times more [AOR=2.6;95%CI=1.3 to 5.5]; whose fathers’ had no formal education was 80% times less [AOR=0.2; 95% CI=0.03 to 0.9] whose mothers’ were housewives was 90% times less [AOR=0.1; 95% CI=0.01 to 0.8] wealth index quintile of lowest [AOR=0.2; 95% CI=0.03 to 0.7], second [AOR= 0.23; 95%CI= 0.1 to 0.8] and middle [AOR= 0.21; 95%CI=0.1 to 0.7] likely to be overweight and/or obesity than their counterparts (Table 4).
The present study revealed the coexistence of underweight and overweight/obesity in the studied in-school communities and concordant with various studies documented elsewhere (Teshome et al., 2013, Ene-Obong et al., 2012, Motlagh et al., 2011, Alemu et al., 2014).
Nevertheless, when the present study is compared with the Gondar findings (11.2% vs 5.9%), the present finding is higher (Gebregergs et al., 2013) probably due to seasonality effect and the cut-off points used to classify malnutrition in the present study is different (BMI-for-Age).
The odds of being underweight among adolescents whose fathers’ had no formal education attended, primary and secondary education were higher than those education level was above secondary, respectively; and concurs with previous study findings from northern Ethiopia (Dessalegn, 2015). Nevertheless, when compared with Hawassa and Addis Ababa the finding is different (Teshome et al., 2013, 2009). This difference observed in this study might be explained by the fact that fathers who had better education had better job opportunity which could lead to higher income and a better opportunity for food consumption. In addition to this, educated fathers had better nutritional awareness as well as better caring of children.
In this study, respondents whose family size of five or less were observed to be less likely to be underweight at the same time (double burden) more likely to be overweight and/or obesity than those whose family size was greater than five. This finding is comparable to the study done in Addis Ababa and among Adolescents in Osun State, Nigeria (Alemu et al., 2014, Funke, 2008), where both documented the coexistence of underweight and overweight/ obesity.
Students whose fathers’ occupation was merchant showed to be less likely to be underweight than whose family were private workers and the finding is consistent with the study in Tanzania and Palestinian participants (Cordeiro et al., 2012, Massad et al., 2012) and attributed to better income of merchants.
Wealth index quintile of lowest and second were positively associated with underweight while respondents who were food secure were negatively associated with underweight in the present study which concurs with the previous studies of Tanzania and Palestine (Cordeiro et al., 2012; Massad et al., 2012).
In this study, wealth index quintile of lowest, second and middle, fathers’ education level of no formal education and mother occupation of housewife were negatively and significantly associated with overweight and/or obesity. This finding is in line with a study done in South Africa (Kruger et al., 2006); which reported the least overweight/obese children’s among parents who were employed as domestic/housewife workers, while more overweight/obese children’s among parents who had professional/business occupations (higher incomes) or self-employed in the informal sector. In contrast the Korean study documented high economic status as a protective factor for overweight which was different from our findings (Noh et al., 2014) and could be attributed to excess fat dense foods consumption which is considered as a sign of healthiness and a common experience among higher income family leading to weight gain. On the contrary, developed countries considered overweight as a disease and it is those families from low socioeconomic status that are consuming fat dense foods because of its accessibility.
Being grade 9 student was positively and significantly associated with overweight and/or obesity compared to grade 10. Nevertheless, studies from Hawassa (Teshome et al., 2013) and Addis Ababa (Alemu et al., 2014) showed no significant difference among grade level. The difference observed in the present study might be associated to more awareness of physical exercise of grade 10 students than grade 9; and another probable reason might be also due to the adolescent growth spurt sometimes occurring at an earlier age which could lead to increased adiposity.
Strength and limitations
This study in addition to weight and height, waist circumference and hip circumference was measured to address the central adiposity by WHR. Multinomial logistic regression model was also used to reduce the effect of error. Nonetheless, there were limitations like; variables which can affect malnutrition such as parental weight status, nutritional knowledge, dietary intake and disease status of the participants which were not addressed in this study. Other than this, identification of temporal relationship, seasonal variation for food insecurity measurement is acknowledged as limitation of the study.
This study revealed the coexistence of underweight and overweight and/or obesity among in- school adolescents from rural Ethiopia. Parental education and occupational status, family size and wealth index were the significant predictors attributed to the extremes of malnutrition. Thus, actions targeting the identified predictors are necessary to improve nutrition situation of the in-school community by the stakeholders which include health and education sectors through family planning and nutrition related education.
The authors have not declared any conflict of interests.
REFERENCES
|
Alemu E, Atnafu A, Yitayal, M, Yimam K (2014). Prevalence of overweight and/or obesity and associated factors among high school adolescents in Arada Sub city, Addis Ababa, Ethiopia. J. Nutr. Food Sci. 4:2.
Crossref
|
|
|
|
Amare D, Negesse A, Tsegaye B, Assefa B, Ayenie B (2016). Prevalence of undernutrition and its associated factors among children below five years of age in Bure town, west Gojjam zone, amhara national regional state, northwest Ethiopia. Adv. Public Health 2016:7145708.
Crossref
|
|
|
|
|
Bull FC, Maslin TS, Armstrong T (2009). Global physical activity questionnaire (GPAQ): nine country reliability and validity study. J. Phys. Act. Health. 6:790-804.
Crossref
|
|
|
|
|
Cordeiro LS, Wilde PE, Semu H, Levinson FJ (2012). Household food security is inversely associated with undernutrition among adolescents from Kilosa, Tanzania. J. Nutr. 142:1741-1747.
Crossref
|
|
|
|
|
De Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J (2007). Development of a world health organization (WHO) growth reference for school-aged children and adolescents Bull. World Health Organ. 85(9):660-667.
Crossref
|
|
|
|
|
Ene-Obong H, Ibeanu V, Onuoha N, Ejekwu A (2012). Prevalence of overweight, obesity, and thinness among urban school-aged children and adolescents in southern Nigeria. Food Nutr. Bull. 33:242-250.
Crossref
|
|
|
|
|
Funke OM (2008). Prevalence of underweight: A matter of concern among adolescents in Osun State, Nigeria. Pakistan J. Nutr. 7:503-508.
Crossref
|
|
|
|
|
Garenne M (2010). Urbanisation and child health in resource poor settings with special reference to under-five mortality in Africa. Arch. Dis. Child. 95:464-468.
Crossref
|
|
|
|
|
Gebregergs G, Yesuf M, Beyen T (2013). Overweight and obesity, and associated factors among high school students in gondar town, North West Ethiopia. J. Obes. Wt Loss. Ther. 3:2.
|
|
|
|
|
Hazbun OM, Azcona C, Martínez JA, Martí A (2009). Management of overweight and obesity in adolescents: an integral lifestyle approach. Actividad Dietética 13:153-160.
Crossref
|
|
|
|
|
James W, Norum K, Smitasiri S, Swaminathan M, Tagwireyi J, Uauy R (2000). Ending Malnutrition by 2020: an Agenda for Change in the Millennium: Final Report to the ACC/SCN by the Commission on the Nutrition Challenges of the 21st Century. Supplement to the Food and Nutrition Bulletin. 2000 September. Food Nutr. Bull. P 21.
|
|
|
|
|
Kelishadi R (2007). Childhood overweight, obesity, and the metabolic syndrome in developing countries. Epidemiol. Rev. 29:62-76.
Crossref
|
|
|
|
|
Kruger R, Kruger HS, Macintyre UE (2006). The determinants of overweight and obesity among 10- to 15-year-old schoolchildren in the North West Province, South Africa - the THUSA BANA (Transition and Health during Urbanisation of South Africans; BANA, children) study. Public Health Nutr. 9:351-358.
Crossref
|
|
|
|
|
Massad S, Deckelbaum RJ, Gebre-Medhin M, Holleran S, Dary O, Obeidi M, Bordelois P, Khammash U (2012). Double burden of undernutrition and obesity in Palestinian Schoolchildren: a cross-sectional study. Lancet 380:S5-S6.
Crossref
|
|
|
|
|
Megabiaw B, Rahman A (2013). Prevalence and determinants of chronic malnutrition among under-5 children in Ethiopia. Int. J. Child Health Nutr. 2:230-236.
Crossref
|
|
|
|
|
Motlagh ME, Kelishadi R, Amirkhani MA, Ziaoddini H, Dashti M, Aminaee T, Ardalan G, Mirmoghtadaee P, Keshavarz S, Poursafa P (2011). Double burden of nutritional disorders in young Iranian children: findings of a nationwide screening survey. Public Health Nutr. 14:605-610.
Crossref
|
|
|
|
|
Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, Mullany EC, Biryukov S, Abbafati C, Abera SF (2014). Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384:766-781.
Crossref
|
|
|
|
|
Noh JW, Kim YE, Park J, Oh IH, Kwon YD (2014). Impact of parental socioeconomic status on childhood and adolescent overweight and underweight in Korea. J. Epidemiol. 24:221-229.
Crossref
|
|
|
|
|
Suchindran C, North KE, Popkin BM, Gordon-Larsen P (2010). Association of adolescent obesity with risk of severe obesity in adulthood. JAMA 304:2042-2047.
|
|
|
|
|
Teshome T, Singh P, Moges D (2013). Prevalence and associated factors of overweight and obesity among high school adolescents in urban communities of Hawassa, Southern Ethiopia. Curr. Res. Nutr. Food Sci. J. 1:23-36.
Crossref
|
|
|
|
|
World Health Organization, (WHO) (2009). Global health risks: mortality and burden of disease attributable to selected major risks.
|
|
|
|
|
World Health Organization, (WHO) (2012). Steps instrument for chronic disease risk surveillance. 2012.
|
|
|
|
|
Yibeltal T, Charles T, Uriyoan C (2000). The Rising Overweight-obesity and Its Socio-Demographic Correlates in Addis Ababa.Ethiopia. 2011 pp. 1-14.
|
|
|
|
|
Yohannes Z, Behailu T, Mekonnen A, Teshome M, Yeshitila S (2017). Malnutrition and associated factors among under five children (6-59 Months) At Shashemene Referral Hospital, West Arsi Zone, Oromia, Ethiopia. Curr. Pediatr. Res. 21(1):172-180.
|
|
|
|
|
Zeleke A (2009). Prevalence of childhood and adolescent overweight and obesity among elementary school students in Addis Ababa: Double burden of malnutrition in Ethiopia. Available at:
View
|
|
|
|
|
Ziraba AK, Fotso JC, Ochako R (2009). Overweight and obesity in urban Africa: A problem of the rich or the poor? BMC Public Health. 9:465.
Crossref
|
|