Full Length Research Paper
ABSTRACT
Considering the importance of nutritional health for people living with HIV, programs delivering nutritional support have been scaled up globally. Among various programs, the Food by Prescription (FBP) program has been implemented in Ethiopia since 2010. This study was undertaken to assess the level of adherence to the FBP program and identify the associated factors among HIV infected adults. Facility-based cross-sectional study design was conducted from May to June 2018 among 481 adult people living with HIV who have been enrolled in the program in 15 public health facilities. The study subjects were selected through a convenient sampling technique and data were collected using a structured interviewer-administered questionnaire. The data were entered and analyzed using Epi Info version 7 and Statistical Package for Social Science version 20 statistical software respectively. Bivariable and multivariable logistic regression were used. More than half 285(59.3) of the study subjects were found to be adherent to the FBP program. The amount of prescribed food, the duration of stay in nutrition program, the practice of sharing the supplement and experiencing of supplement stock out was found to be the most important predictors. The study revealed the level of adherence to the FBP program and identified some of the most important associated factors among adult people living with HIV. Strengthening the counseling component of the program, improving the supply management of the health facilities and linking people living with HIV to the economic strengthening activities should be considered to improve the adherence level of the program.
Key words: Adherence, Food by Prescription Program, adult PLWHA, Ethiopia.
INTRODUCTION
Globally 36.7 million [30.8 million–42.9 million] people were living with HIV in 2016. The Sub-Saharan African region remains the worst affected region in the world accounting for 64% of all people with new HIV infections from the global community (UNAIDS, 2017). In Ethiopia, an estimated 613,000 people were living with HIV in 2017. The HIV prevalence among women and men aged 15-49 in Ethiopia was 0.9% (FHAPCO, 2018).
Considering the fact that nutritional health is essential for people living with HIV/AIDS (PLWHA), programs delivering inputs including nutrition assessment, counseling, therapeutic nutritional rehabilitation, and livelihood support to HIV-infected adults and children have been scaled up globally (Sadler et al., 2012). The current Ethiopian National Nutrition Program also emphasized the importance of providing nutrition support for PLWHA (Ethiopian FMoH, 2016).
Among the various programs that combine nutrition support with HIV programming, the Food by Prescription (FBP) program has been implemented in Ethiopia since 2010. The program consists of a combined package of Nutrition Assessment, Counseling, and Support (NACS) to HIV-infected adults as well as orphans and vulnerable children (OVC) based on specific criteria. Through the program, HIV-infected adults with moderate acute malnutrition (MAM) have been provided with two sachets of Ready to Use Therapeutic Food (RUTF) daily until recovery from malnutrition or for a maximum of three months. Those with severe acute malnutrition (SAM) have been provided with four sachets of RUTF daily until recovery or for a maximum of six months (Sadler et al., 2012).
A longitudinal study was conducted in Sub-Saharan Africa to document the nutrition outcomes of HIV -infected malnourished adults treated with RUTF. The study found out that nutrition therapy provided in conjunction with an early start of ART increases the chances of nutritional recovery in severely malnourished HIV patients (Ahoua et al., 2011). A quasi-experimental study conducted in Ethiopia among PLWHA found out that a significantly better nutrition outcome and greater improvements in functional status among the intervention group (Sadler et al., 2012). A retrospective cohort study conducted at Mekele referral Hospital among patients on HIV/AIDS Care also revealed that 62.2% of patients enrolled in the program were recovered (Maldey et al., 2014). However, challenges such as failure to respond to the nutritional support, a higher level of default and poor adherence were also reported. Sadler and his friends found out that 58.4% of participants who complied with the program protocol did not respond to treatment and 70.6% of participants defaulted from the FBP program (Sadler et al., 2012).
In Mekele Referral Hospital, 29.6% of the program participants were non-respondents, and 5.9% were defaulters with the overall failure rate of 37.6% (Maldey et al., 2014). It was suggested that enhancing the level patient adherence could have a good potential to improve the impact of the program (Sadler et al., 2012).
However, a study conducted in Addis Ababa City revealed a low level of adherence (36.3%) among the program participants (Kebede and Haidar, 2014). To improve the success of the FBP program, the identification of programmatic challenges could have overriding importance. Therefore, the current study was undertaken to assess the adherence dimension of the FBP program and to identify factors that affect theadherence level of adult PLWHA in Addis Ababa City.
MATERIALS AND METHODS
Study setting and population
This study was conducted in Addis Ababa City. Based on the 2017 population projection of the Central Statistical Agency (CSA), the city administration has a total population of 3, 433,999, out of which 1624,999 were males and 1,809,000 females (FDRE-CSA, 2013). The City Administration comprises 13 public hospitals, 35 private hospitals, 2 charity hospitals, 96 health centers, and 723 clinics. According to the 2017/18 report of the City Administration Health Office, 89,033 PLWHA have been receiving ART care and related support. Addis Ababa is one of the regions in Ethiopia, where FBP is being implemented in public health centers and hospitals. At the time of the study, 60 public health facilities have been providing the program for 4,325 adult PLWHA who are usually poor and demand the assistance of the government to ensure their good nutrition and health.
For the study, all adult PLWHA who have been enrolled in the FBP program for at least one month in the selected public health facilities were included. The study excluded pregnant and lactating PLWHA and those who were unable to communicate due to illness.
Study design, sample size, and sampling procedures
The facility-based cross-sectional study design was conducted in selected public health facilities from May to June 2018 among adult PLWHA who have been enrolled in the FBP program at the selected public health facilities of Addis Ababa city. The sample size for the study was determined by using a single population formula considering a 36.3% adherence level taken from a similar study conducted in Addis Ababa city (Kebede and Haidar, 2014). Α marginal error of 5%, design effect of 1.5 for the use of multistage cluster sampling and 10% of non-response were assumed in the sample size calculation. After making an allowance for a finite population correction factor, 497 adult PLWHA were required from the selected public health facilities.
Multi-stage cluster sampling techniques were used in the selection of the health facilities. In the first stage of the sampling process, from the 10 sub-cities of the Addis Ababa city administration, four sub-cities were selected randomly using the lottery method. The selected sub-cities included Bole, Yeka, Gullele and Kirkos Sub Cities. In the second stage, three public health centers that were selected randomly and all the available public hospitals were included from each of the selected Sub Cities. Accordingly, 12 health centers and three hospitals were included in this study. The calculated sample size was allocated to the health facilities based on Probability Proportional to Size (PPS) techniques using the registered number of adult PLWHA who have been enrolled in the FBP program in the selected facilities. The study subjects were selected through convenient sampling technique in a consecutive manner.
Data collection method, tools, and personnel
A structured interviewer-administered questionnaire was used for data collection. The questionnaire was first developed in English and then translated into the local language (Amharic). It was back-translated to English to ensure the consistency of the translation and reviewed by local experts before the data collection. The questionnaire has four sections. The first section was used to collect data on socio-demographic issues. The second section dealt with the care that PLWHA have been given at the health facilities (follow up, nutritional counseling and appetite taste). Questions that assessed the utilization of the RUTF supplied through the FBP program and the related questions were also included in this section. The third section was intended to assess the food insecurity situation of the households, which, was measured using the Household Hunger Scale (HHS). The scale consisted of six occurrence questions covering a recall period of four weeks. By counting the number of “no” responses of the study subjects, their households were categorized into three independent groups. Study subjects with a score of 0-1 were considered to have little to no hunger in households. Study subjects with a score of 2-3 were considered to have moderate hunger in the households while those with a score of 4-6 were considered to have severe hunger in households (Ballard T. et al., 2011). According to USAID guidelines for measuring the household food security situation, households with a severe or moderate level of hunger were categorized as food-insecure households (Gary et al., 2000).
The adherence of the study subjects to the FBP program was assessed in the fourth section of the questionnaire. Adherence was measured based on the study subject’s self-report using the Modified Morisky Scale (MMS). The scale consists of six items with "Yes" or "No" response. Three of the items in the scale were intended to measure the motivation domain of adherence intention while the remaining three items were intended to measure the knowledge domain of adherence intention. The items provide a scoring range of 0 to 3 for each of the motivation and knowledge domains. The score of 0 to 1 and >1 were considered to have low or high for each of the domains. Based on the scoring, the study subjects were then categorized into one of the four distinct adherence intention quadrants which take in to account the knowledge level (high or low) and motivation status (high or low). Study subjects categorized under quadrant IV were considered to have a high level of adherence (high knowledge/high motivation)( Case Management Society of America, 2006). To collect the data, 15 experienced nurses were recruited and trained for two days to ensure uniform data collection. Three trained public health experts were also deployed to supervise the data collection. The data collection was strictly followed by the supervisor and the investigators. One week before the actual data collection, the questionnaire was pre-tested on 5% of the sample in two health facilities that were not be included in the study. Minor modifications were made on the questionnaires based on the pretest findings.
Data processing and analysis
Two independent data clerks entered the data into Epi Info version 7 statistical software. For data analysis, we used the Statistical Package for Social Science (SPSS) version 20 statistical software. Descriptive statistics were conducted to summarize the characteristics of the study subjects. Bivariable logistic regression was employed to examine the independent associations between the outcome variables (adherence) and each of the independent factors. Variables having a significant association with the outcome variables were recruited for the multivariable logistic regression model that could control the effect of potential confounders. The finding of the final model was expressed as Adjusted Odds Ratios (AOR) with 95% Confidence Intervals (CI).
Ethical consideration
The Institutional Review Board (IRB) of the Bahir Dar University, Faculty of Food and Chemical Engineering approved the research protocol. An official letter of cooperation was written to Addis Ababa City Administration Health Office and each of the selected health facilities. All study subjects were asked for their written informed consent after given a detail explanation about the study.
RESULTS AND DISCUSSION
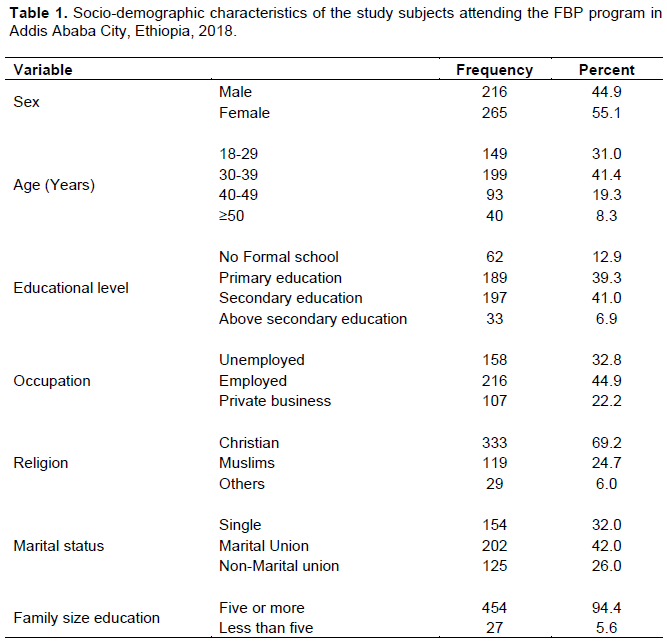
A total of 481 study subjects participated in the study making a response rate of 96.8%. More than half of the study subjects 265 (55.1%) were females and 19 (41.4%) of them were in the age group of 30 to 39 years. One hundred ninety-seven (41.0%) of the study subjects completed secondary education and 216 (44.9%) of them were employed. More than two-third 333 (69.2%) of the study subjects were Christian by religion and 202 (42.0 %) were in marital union. Hundred fifty-four (94.4%) study subjects reported that more than five people were living in their households (Table 1).
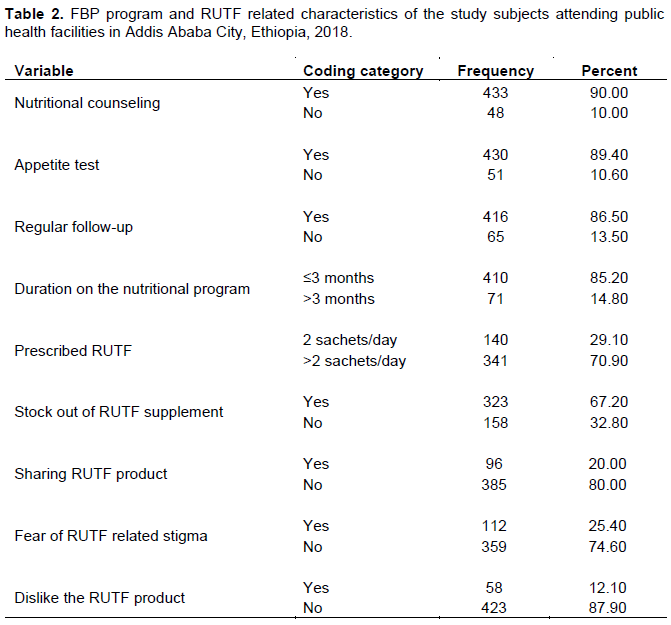
Almost all 433(90.0%) of the study subjects received nutritional counseling and 430(89.4%) of them were tested for their appetite when they were first prescribed the RUTF. A very great proportion of the study subjects 416(86.5%) had a regular follow-up for progress check and collection of the prescribed RUTF. Four hundred ten (85.2%) study subjects stayed on the nutritional program for the duration of three or fewer months and for 341(70.9%) of the study subjects, more than two sachets of RUTF were prescribed per day. More than two-thirds of the subjects 323(67.2%) experienced the stock out of RUTF supplement in the facility. Ninety-six (20%), 112 (25.4%) and 58 (12.1%) of the study subjects reported the practice of sharing RUTF, fear of RUTF related stigma and disliking RUTF product respectively (Table 2).
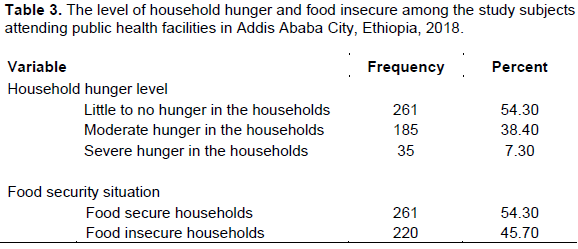
Based on the HHS, 261(54.2%), 185(38.4%), and 35(7.3%) of the study subjects were found to have little to no hunger, moderate hunger and severe hunger in their households respectively. According to USAID guidelines for measuring household food security using HHS, nearly half 220(45.7%) of the households with a severe and moderate level of hunger were considered as food insecure households (Table 3).
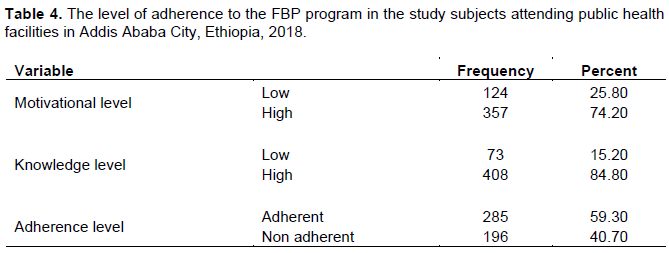
Regarding the motivation and knowledge domains of the study subjects that were used to measure the level adherence to the FBP program, a quarter 124(25.5%) of the study subjects had a low level of motivation, and nearly one-fifth 73(15.2) of them had a low level of knowledge. Accordingly, more than half 285(59.3) of the study subjects were found to be adherent to the FBP program (Table 4).
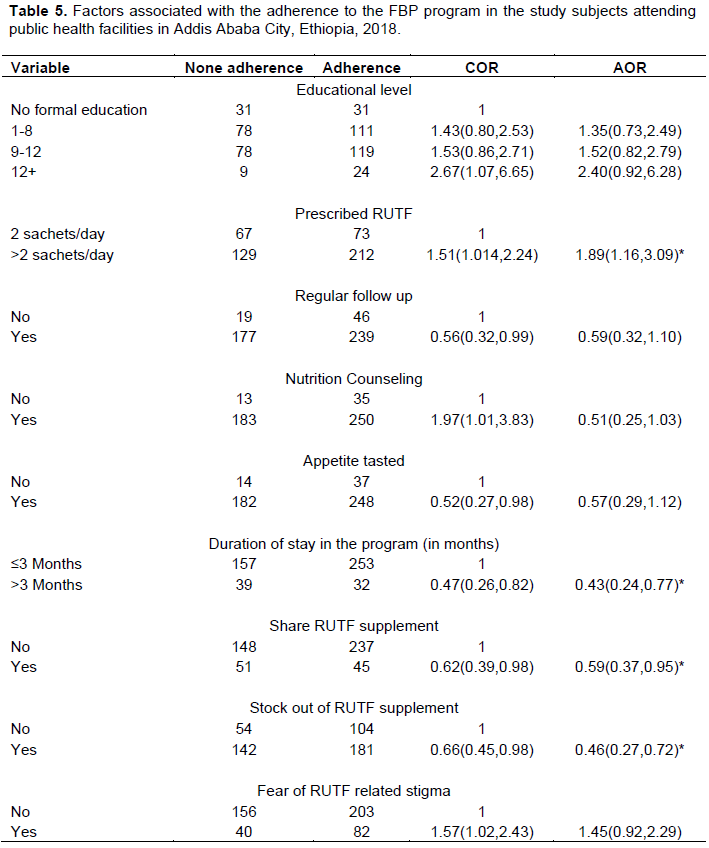
Based on the finding of the multivariable binary logistic regression analysis model, study subjects who took more than two sachets of prescribed RUTF per day were 89.6% (AOR = 1.89; 95 % CI = 1.16–3.09) more likely to be adherent compared to those who took two sachets. Study subjects who stayed for more than three months in the nutritional program and practiced sharing prescribed RUTF were 57% (AOR = 0.43; 95 % CI = 0.24–0.77) and 41% (AOR 0.59; 95% CI= 0.37 to 0.95) respectively less likely to be adherent compared to the reference group. Similarly, study subjects who experienced the stock out of RUTF supplement in the facility were 54% (AOR=0.46; 95% CI =0.27-0.72) less likely to adhere compared to their counter groups (Table 5).
DISCUSSION
The study revealed the level of adherence to the FBP program and identified some of the most important associated factors among adult PLWHA who had been receiving care from the public health facilities in Addis Ababa City, Ethiopia. It was found out that the self-reported level of adherence was 285(59.30%). The observed level of adherence in this study is higher than the previous study conducted in the study area where 36.3% of the PLWHA were found to be adherent to the FBP program (Kebede and Haidar, 2014). However, the equivalent finding was reported from Senegal where the rate of RUTF consumption compared to the prescribed amount was approximately 50% among the study subjects (Cames et al., 2017). A qualitative study conducted in Kenya also revealed that half of malnourished AIDS adult patients failed to consume the daily prescription of RUTF (Dibari et al., 2011). The taste of the product and associated nausea and vomiting, diet monotony and clinical conditions associated with HIV were found to be some of the factors that reduced the daily consumption of the RUTF based on the prescribed level (Dibari et al., 2011; Olsen et al., 2013).
This study also revealed a statistically significant association between the duration of the study subjects stayed on the FBP program and the level adherence. Study subjects who stayed on the nutritional program for more than three months were 57% less likely to be adherent compared to those who stayed for less than three months. This finding was supported by a similar study conducted in Addis Ababa health facilities that showed adult PLWHA who had been consuming the RTUTF for more than four months were less likely to adhere (Kebede and Haidar, 2014). In a study conducted in Vietnam, a trend was noted in the consumption of the RUTF (Plumpy’Nut) from the first week to the second week of the regimen where the mean number of servings consumed decreased significantly from week 1 to week 2 (Wieringa FT. et al., 2013). The observed level of poor adherence among patients who stayed in the nutritional program for an extended duration may be related to the fact that patients could become fed up taking and consuming the prescribed food due to the longer duration (Kebede and Haidar, 2014). Furthermore, for patients with SAM, a relatively greater amount of RUTF (four sachets of RUTF daily) has been ordered for longer duration typically until recovery or for six months (Gerberg and Stansbury, 2010).
However, these patients usually have an advanced disease progression and increased morbidity which affects their eating behavior and reduces their swallowing capacity that potentially leads to the lower level of adherence to the nutritional support program (Dibari et al., 2011). The study subjects who took more than two sachets of prescribed RUTF per day were 89% more likely to be adherent compared to those who took two sachets RUTF. This finding is contradicting with other studies that reported more non-adherence among patients prescribed with more than 2 sachets/day (Kebede and Haidar, 2014, Dibari, 2008).
According to the Ethiopian National guideline, four sachets of RUTF have been recommended for a maximum of six months (relatively longer duration) for PLWHA with SAM who usually have an advanced disease progression, increased morbidity and associated feeding difficulty as discussed above (Ethiopian FMoH, 2008). The frequently reported compliant of the PLWHA about the product such as the taste and the related occurrences of nausea and vomiting (Dibari et al., 2011) should also be taken in to account while interpreting this finding until a more informative study finding is available from the scientific community.
According to a study conducted in rural Malawi, the prescribed RUTF had been shared among all family members (Rodas-Moya et al., 2015). A review finding of the Kenyan FBP Program showed that sharing RUTF ration with other household members was common (Food and Nutrition Technical Assistance, 2009). The study conducted in Addis Ababa City also reported sharing the product with children and with other HIV-infected friends (Kebede and Haidar, 2014). The practice of sharing the RUTF with household members was also reported from similar studies conducted elsewhere (Gerberg and Stansbury, 2010; Dibari et al., 2011; Cames et al., 2017). The scarcity of food at the level of households, poverty, household food insecurity, and cultural issues are among the reasons behind sharing RUTF (Rodas-Moya et al., 2015; Food and Nutrition Technical Assistance, 2009; Kebede and Haidar, 2014). The practice of sharing the prescribed RUTF among PLWHA was found to be closely linked with-the compliance to the FBP program as per the finding of a qualitative investigation of adherence to nutritional therapy in malnourished adult AIDS patients in Keny (Dibari et al., 2011). It was also reported that non-adherence due to the sharing of food at home was considered by clients to be the single most important contributor to inadequate intake (Food and Nutrition Technical Assistance, 2009).
Similar to most of the available literature, this study also revealed the practice of sharing the RUTF was an important predictor of adherence where study subjects who shared the prescribed RUTF were 41% less likely to adhere to the FBP program. PLWHA who experienced stock out of RUTF supplement in the health facilities were 54% less likely to adhere to the program. In line with our findings, a similar finding was reported indicating that the delay in distributing the food to the health facilities could have an effect on the adherence level of the PLWHA (Kebede and Haidar, 2014). In Kenya, factors related to the design of the FBP program were also identified to be one of the two important factors that limit the compliance of PLWHA to the RUTF-based protocol (Dibari et al., 2011).
The limitations of this study included that some of the important variables such as the nutritional status of PLWHA, their clinical condition and the change in their weight; health and quality of life that could have been more informative to understand the success and the challenges of FBP program were not included in the study. Measuring the adherence level of the study subjects by a single method of self-reporting was also another limitation. Furthermore, due to the cross- sectional nature of the study establishing the causal relationship between significant variables and the level of adherence could be difficult.
CONCLUSION AND RECOMMENDATION
In conclusion, the present study found out that the self-reported level of adherence to the FBP program among PLWHA who had been receiving care from the selected public health facilities of Addis Ababa City was 285(59.3%). The amount of prescribed RUTF, the duration of stay in a nutritional program, the practice of sharing of RUTF supplements and having the experience of RUTF supplement stock out were found to be the most important predictors of adherence. Capacity strengthening on the counseling component of the NACS service at the level of health facilities could be important to address some of the identified important predictors of adherence such as the practice of sharing the RUTF. The supply management of the health facilities should also be improved to ensure sustainable availability of RUTF in all health facilities to regularly supply to the needy PLWHA based on the recommended protocol and to prevent stock out. Linking PLWHA to the economic strengthening activities needs concentrated attention of all concerned bodies. It might help to address the practice of sharing RUTF, which is usually associated with poverty and household food insecurity.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Ahoua L, Umutoni C, Huerga H, Minetti A, Szumilin E, Balkan S (2011). Nutrition outcomes of HIV-infected malnourished adults treated with ready-to-use therapeutic food in sub-Saharan Africa : a longitudinal study. Journal of International AIDS Society 14(1):2. |
|
|
Ballard T, Coates J, Swindale A, Deitchler M (2011). Household Hunger Scale : Indicator Definition and Measurement Guide. Washington, DC: Food and Nutrition Technical Assistance II Project, FHI 360. |
|
|
Cames C, Varloteaux M, Have NN, Diom AB (2017). Acceptability of Outpatient Protocols in HIV-Infected Senegalese Children and Adolescents Within the MAGGSEN Cohort Study. The Pediatric Infectious Disease Journal 38(1):27-36. |
|
|
Dibari F (2008). Operational aspects of therapeutic nutritional rehabilitation for HIV/TB patients: the use of Ready To Use Therapeutic Foods. In: 39th Union World Conference on Lung Health. Paris, France. |
|
|
Dibari F, Bahwere P, Gall I Le, Guerrero S, Mwaniki D, Seal A (2011). A qualitative investigation of adherence to nutritional therapy in malnourished adult AIDS patients in Kenya. Public Health Nutrition 15(2):316-23. |
|
|
Ethiopian FMoH (2008). Ethiopian Guide to Clinical Nutrition Care for Children and Adults Living with HIV. Addis Ababa, Ethiopia. |
|
|
Ethiopian FMoH (2016). National Nutrition Program 2016-2020. Addis Ababa, Ethiopia. |
|
|
FDRE-CSA (2013). Population Projection of Ethiopia for All Regions At Wereda Level from 2014-2017. Addis Ababa, Ethiopia. |
|
|
FHAPCO (2018). HIV Prevention in Ethiopia National Road Map 2018 - 2020. Addis Ababa, Ethiopia. |
|
|
Food and Nutrition Technical Assistance II Project FANTA-2, FHI 360 (2009). Review of Kenya's Food by Prescription Program. Washington, DC. |
|
|
Gary B, Mark N, Cristofer P, William H, John C (2000). Guide to Measuring Household Food Security, Revised 2000. Alexandria VA. |
|
|
Gerberg L, Stansbury JP (2010). Food by prescription in Kenya. Arlington, VA. |
|
|
Kebede MA, Haidar J (2014). Factors influencing adherence to the food by prescription program among adult HIV positive patients in Addis Ababa . Infectious Diseases of Poverty 3(20). |
|
|
Maldey B, Haile F, Shumye A (2014). AIDS and Clinical Outcome of Ready to Use Food Therapy among Patients on HIV / AIDS Care in Mekelle Hospital, Northern Ethiopia : Retrospective Cohort Study. Journal of AIDS and Clinical Research 5(1):268. |
|
|
Olsen M, Tesfaye, Kæstel, Friis, Holm (2013). Use, perceptions, and acceptability of a ready-to-use supplementary food among adult HIV patients initiating antiretroviral treatment: a qualitative study in Ethiopia. Patient Prefer Adherence 7:481-8. |
|
|
Rodas-Moya S, Kodish S, Grede N, Pee S de (2015). Preferences for food and nutritional supplements among adult people living with HIV in Malawi. Public Health Nutrition. |
|
|
Sadler K, Bontrager E, Rogers B, Coates J, Ghosh S, Kidane Y (2012). Measuring the Impact and Cost-Effectiveness of Prescribed Food on Recovery from Malnutrition and HIV Disease Progression Among HIV + Adult Clients in Ethiopia. Feinstein International Center, Friedman School of Nutrition Science and Policy. Boston, USA. |
|
|
UNAIDS, UNAIDS DATA (2017). Avenue Appia, Geneva, Switzerland. |
|
|
Wieringa FT, Hoang M, Brown M, Maalouf-manasseh Z, Berger J (2013). Acceptability of Two Ready-to-Use Therapeutic Foods among HIV- Positive Patients in Vietnam. Washington, DC. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


