Full Length Research Paper
ABSTRACT
Adequate nutrition is vital to children’s growth and development. Globally, about 155 million children were stunted. About half of the child's mortality was related to child malnutrition in developing countries, including Ethiopia. This study aimed to assess the prevalence of stunting, feeding practice, and associated factors among children age 6 to 59 months in Zeway Dugda district in 2019. A community-based cross-sectional study was conducted among 783 children age 06 to 59 months selected with a multistage sampling technique. The data was entered, coded, and summarized using EPI INF-07 statistical software and analyzed by using SPSS version 21. Anthropometric measurements were taken by using calibrated equipment and analyzed with WHO-Anthro version 3.2.2 software. Bivariate and multivariate logistic regression analysis was done to see the association of each category of a variable with the outcome variable. Significance was checked at 95% CI with a p-value <0.05. The prevalence of stunting was 46.2% (of them, 30.4% severely stunted and 15.8% moderately stunted). Only 41% of the children had good IYCF practice as of WHO recommendation. Children’s who born from young age mothers [AOR=2.02, 95% CI (1.37, 2.97)], who were fed breast milk below 24 months [AOR = 1.75, 95% CI (1.18, 2.58)], who were from large family [AOR = 1.57, 95% CI (1.13, 2.19)], whose mother started FANC after 28 weeks of GA [AOR = 2.66, 95% CI (1.04, 6.78)], who were cared with other guardian [AOR = 2.42, 95% CI (1.00, 5.81)], whose weight for height below -2 Z-Score [AOR = 5.76, 95% CI (2.24, 15.58)], and whose MUAC < 125 mm [AOR = 1.71, 95% CI (1.15, 2.53)] were positively associated with stunting. Stunting was a highly prevalent problem with a low level of IYCF practice in the study area. This finding accentuates the need for increasing awareness of mothers about appropriate AMIYCF, family planning utilization, child care practice, early initiation of FANC, and delaying young age birth to prevent stunting.
Key words: Stunting, 6-59 months of age children, adolescent maternal infant young child feeding (AMIYCF), Zeway Dugda Woreda, Ethiopia.
INTRODUCTION
Chronic undernutrition among under-five children is a major public health problem in developing countries including Ethiopia. In Ethiopia, child stunting is one of the most serious public health problems and the highest in the world (UNICEF, Tracking Progress on Child and Maternal Nutrition, UNICEF, New York, 2009; Berihun and Azizur, 2013). Nutritional stunting, which is the height for age below that is expected based on international growth reference, is a very serious type of malnutrition in that it develops slowly through time before it is evident (MOH, 2014). It is attributable to more than half of all child deaths in Ethiopia by raising the risk factors of other childhood illnesses (Fentaw et al., 2013).
Stunting in early life is associated with adverse functional consequences and growth failure during infancy and early childhood is often irreversible, leading to short stature during adolescence and adulthood. Stunting is associated with an elevated risk of child mortality, increased susceptibility to infection, and poor cognitive and psychomotor development (Rah et al., 2010; Victora et al., 2008; Fentaw et al., 2013). The long-term consequences of stunting include deficits in school achievement, reduced work capacity, and adverse pregnancy outcomes. Worldwide, stunting affects nearly one-third of children under 5 years of age, with the prevalence being higher in low-resource countries in sub-Saharan Africa and South Asia (Rah et al., 2010; Victora et al., 2008). Stunting is a multi-factorial phenomenon with a high prevalence in developing countries (Ruel and Menon, 2002; Deconinck et al., 2011; Teshome et al., 2009).
Globally in 2016, 22.9% or 154.8 million children under 5 years of age suffered from child stunting, defined by a low height-for-age (UNICEF, WHO, World Bank Group, 2015). Stunting is measured by a height-for-age z-score of more than 2 standard deviations below the World Health Organization (WHO) Child Growth Standards median (World Health Organization, 2018), showing a restriction of a child’s potential growth (Black et al., 2008). Child stunting can happen in the first 1000 days after conception and is related to many factors, including socioeconomic status, dietary intake, infections, maternal nutritional status, infectious diseases, micronutrient deficiencies, and the environment (Black et al., 2008; Ikeda et al., 2013; Black et al., 2013; Gossaye et al.; 2003)
More than 90% of stunted children in the world have been living in Africa and Asia. An estimated 80% of the world's stunted children lived in just fourteen countries (India, Nigeria, China, Pakistan, Indonesia, Bangladesh, Ethiopia, Democratic Republic of Congo, Philippines, United Republic of Tanzania, Egypt, Kenya, Uganda, and Sudan) (UNICEF, Improving Child Nutrition, 2013). Sub-Saharan Africa and South Asia were the home to three-fourths of the world's stunted children, 40 and 39%, respectively (De-Onis et al., 2012).
In the past decade, Ethiopia has only limited success in reducing the prevalence of child undernutrition. According to the 2016 EDHS reports, 38% of the children are stunted nationally, whereas, 36.5% of the children are stunted with 17.1 severely stunted in the Oromia region (CSA and ICFI, 2016). In 2019, the prevalence of stunting reduced from 51% in 2005 to 37%. The prevalence of wasting also reduced over the same period, from 12 to 7%. Moreover, the percentage of underweight children has consistently decreased from 33 to 21% over these 14 years. Despite improvements in reducing the prevalence of malnutrition, the current rate of progress is not fast enough to reach the World Health Organization's global target for reducing malnutrition by 40% by 2025 (WHO, 2014; Ethiopian Public Health Institute (EPHI) [Ethiopia] and ICF, 2019).
The improvement of stunting, therefore, the main prerequisite for the reduction of high infant and under-five mortality rate, the assurance of physical growth, social and mental development of children as well as academic achievement. To achieve this goal, chronic nutrition should be addressed comprehensively. Therefore, this study was conducted to assess the determinants of chronic undernutrition and the feeding practice of under-five children and provide suggestions to improve the situation in the study area.
MATERIALS AND METHODS
Study area and period
The study was conducted in Ziway Dugda Woreda including Zeway/Batu town, Arsi zone of Oromia regional state, from March-August, 2019. The study area is Ziway Dugda Woreda which is found in the Arsi zone and located at 221 km from Addis Ababa and 46 km from Assela capital city of Arsi zone. According to the 2019 Woreda health office population profile, the Woreda has a total population of 145,471 and 21,821 6-59 months’ children. The Woreda has 2 administrative towns with 28 rural Kebele and has 6 Primary Health Care Unit (PHUC) with 30 health posts (H/P). The area has a low land climate with short rain that occurred between March and April and long rain occurred between July and September. People in the area predominantly grow cash crops such as Wheat, Barley, Maize, Potato, and Teff with some livestock (Ziway Dugda Woreda Health Office, 2019).
Study design and population
A quantitative community-based cross-sectional study was conducted among all randomly selected children 06 - 59 months of age who lived with their mothers or caregivers in the sampled kebeles of Ziway Dugda Woreda and available during the study period.
Method of sampling
The sample size was calculated using a single population proportion formula by the estimated prevalence of 33.3%, [taken from the study conducted on the prevalence of stunting among children in Southwest Ethiopia (Teferi et al., 2016)] with 5% marginal error (d) and confidence interval of 95% (Z α/2= 1.96). Based on these assumptions, the sample size was 341 calculated with the formula as follows:
and we considered design effect = 2, because of Multi-Stage sampling technique was applied in the study. Therefore, we multiply the sample size with 2 =341×2 = 682 and allowance for possible non-response rate of 10% makes the final sample size; 10% × 682 = 68. So, the total sample size for this research was 750. Regarding the sampling process, the study employed a multi-stage sampling scheme using stratified and simple random. First, the study area was stratified into urban and rural kebeles and then a total of 10 kebeles were randomly selected; one from urban and nine from the rural kebeles considering agro-ecological areas. After the selected kebele determined, the households in the selected kebeles with children age 6 - 59 months were identified through house-to-house visits by the research assistants. A sampling frame was prepared by registering all the identified eligible children age 6 - 59 months in each kebele and provided study code. Then, the probability proportional to size (PPS) sampling technique was applied to determine the number of households with children age 6 - 59 months per selected kebele. Finally, a simple random sampling technique was used to select the required number of children age 6 - 59 months per each kebele among those who fulfill inclusion criteria.
Data collection
A structured and pre-tested questionnaire was used to assess the socio-demographic characteristics, maternal obstetric and birth care service-related characteristics, maternal and IYCF practice-related characteristics, and health care and environmental health-related characteristics. The dietary diversity questionnaire adapted from literature (that is, 2010 WHO IYCF Indicator guideline) (WHO, IFPRI, Davis UC, USAID, FANTA, 2010) and developed based on the study variables.
Data collections were conducted by trained data collectors. Eight data collectors from health workers and one supervisor participated in the data collection process. Before data collection, the data collectors and supervisors were trained for three days on the purpose of the study as well as the technique of data collection on how to conduct the interview and supervision based on questionnaires. Besides, they were trained on anthropometric measurement, dietary intake assessment, and dietary diversity of a given food, etc. Also, the trained data collectors were trained on how to interview and take the anthropometric measurement and the necessary feedback given by the principal investigator.
Regarding the data collection process, first, the data collectors determined the sample size of each stratum and selected study subject by using a simple random sampling technique. Then, the data collector went to selected households and introduced themselves to the study subject and explained the purpose of the study and the ethical issue (that is, confidentiality). Finally, after assured the willingness of the study subject, the trained data collectors conducted the data based on a pre-tested and structured questionnaire.
Data on dietary diversity and frequency of foods taken were assessed by using an adopted structured questionnaire. Dietary diversity score (DDS) were collected and calculated as the sum of the number of the different food source of items in the complimentary food consumed by the children before the assessment from the total study participants. The food frequency questionnaire was used to ascertain the frequency of consumption of certain foods on the list daily. In this study, a total of 7 food items were considered (that is, FG1- grain, roots and tubers, FG2- Legumes and nuts, FG3- Diary products (milk, yogurt, and cheese), FG4-Flesh (meat, fish, poultry, and liver/organ meat), FG5-egg, FG6- vitamin A-rich fruits and vegetables, and FG7-Other fruits and vegetables). Finally, we analyzed the dietary diversity status as of recommendation of IYCF, those children who take a complementary food containing 4 and more food source we considered the children have good dietary diversity (WHO, IFPRI, Davis UC, USAID, FANTA, 2010).
Anthropometric data were collected through the measurement of the length/height of all children. Measurement of length was done in a lying position with a wooden board for children age 6-24 months and measurement of height for children above two-year stature was measured in a standing position in centimeters to the nearest of 1 cm. WHO-Anthro version 3.2.2 software was used to convert the anthropometric measures; height/length and age values into Z-scores of the indices; Height-for-Age (HAZ), considering sex using WHO 2006 standards. A low height-for-age, below-2SD of the reference population indicates stunting, but below -3SD indicates severely stunting. Counter checking a daily filled questionnaire on regular supervision was done by the supervisor and corrected accordingly (World Health Organization, 2018).
Data quality control
The questionnaire was prepared in English and translated from English to Oromifa language and re-translated back to English to check the consistency. Based on the residence of the study populations, the Oromifa version was used for data collection. Three-days training was given for data collectors and supervisors on methods of data collection. Data were checked in the field to ensure that all the information was properly collected and recorded. Before the actual data collection, the tool was pretested on 5% of the sample size in other kebele where the study was not undertaken to check the reliability and modification was done on the tools. The questionnaire was checked daily for completeness during data collection and data were cleaned and coded before data entry. Data analysis was started by sorting and performing quality control checkups on the field. The pre-tested data was not included in the main data. Data validity and reliability were maintained through close supervision of the data collection process by the supervisor and investigators.
Data processing and analysis
Data were entered, cleaned, and edited using EPI INF-07 statistical software and then exported to SPSS version 21.0 for further analysis. The frequency of each variable was calculated to check for accuracy, outliers, consistency, and missed values. The proportion of undernutrition was determined. Crude and adjusted odds ratios were computed for each explanatory variable to determine the strength of association and control confounders. The p-value < 0.25 was taken as a cut-off point to select variables for the multivariable logistic regression models. The final model was built using backward elimination. The p-value of less than 0.05 was considered statistically significant. Multi-collinearity between independent variables was also checked and the finding was not present.
Anthropometry: Measurement of the variation of physical dimensions and the gross composition of the human body at different age levels and degrees of nutrition by weight-for-age, height-for-age, and weight-for-height (Gibson and Ferguson, 1999).
Bottle-feeding: Proportion of children 0-23 months of age who are fed with a bottle.
Colostrum: It is the first yellow milk that helps to expel the baby’s first dark stool.
Complimentary food: Foods that are required by the child, after six months of age, in addition to sustained breastfeeding.
Diarrhea: Diarrhea is defined as a child having three or more loose or watery stools per day.
Dietary practice: Eating habits of the children.
Exclusive breast feeding: Proportion of infants less than 6 months of age feeding only breast milk for the 1st six months from own mother or a wet nurse, or expressed breast milk, and no other liquids or solids except recommended medications.
Family size: Refers to the total number of people living in a house during the study period except for temporal relative residence.
Malnourished: A child will be labeled as malnourished if any of the nutritional assessment indices weight for height, weight for age, or height for age is below the cut-off point whose Z-score < -2.
Minimum dietary diversity: Proportion of children 6-23 months of age who received the number of food groups over the 24 h recall period within their complementary food. It was analyzed by summing the kinds of food groups received by children over the 24 h recall period called DDS.
(1) If the proportion of children 6-23 months of age who received foods from less or equal 3 food groups over a 24-h recall period, they were classified under the lowest dietary diversity.
(2) If the proportion of children 6-23 months of age who received foods from 4 or more food groups over a 24-h recall period, they were classified under High Dietary diversity.
Minimum meal frequency: Proportion of breastfed and non-breastfed children age between 6 and 23 months who receive solid, semi-solid, or soft foods (but also including milk feeds for non-breastfed children) the minimum number of times or more.
Minimum acceptable diet: Proportion of children 6-23 months of age who receive a minimum acceptable diet (apart from breast milk).
Optimal infant young child feeding/nutrition: The proportion of infants exclusively breastfed for the first six months of life to achieve optimal growth, development and health. Thereafter, to meet their evolving nutritional needs, infants should receive safe and nutritionally adequate complementary foods while breastfeeding continues for up to two years of age or beyond (WHO, UNICEF, 2003; MOH, 2014).
Pre-lacteal feeds: Giving other fluids or foods to the baby before the initiation of breastfeeding.
Stunting: A child was defined as stunted if the height for the age index was below -2 SD of the median of the standard curve. Severe stunting was diagnosed if height for the age index was below -3 SD (World Health Organization, 2018; Victora et al., 2008; MOH, 2014).
Timely initiation of breastfeeding: The initiation of breastfeeding immediately or within 1 h after delivery. It also includes the provision of colostrum and avoidance of pre-lacteals such as water, other liquids, and ritual fluids.
Wasting: Nutritional deficient state of recent onset related to sudden food deprivation or mal-absorption utilization of nutrients which results in weight loss. It is defined as wasting if the weight-for-height index was below-2SD from the NCHS/WHO median value and MUAC <125 mm. Severe wasting was diagnosed if the weight-for-height index was below -3 SD or MUAC <110 mm (CSA and ICFI, 2016; MOH, 2014).
Wealth Quintile: Net asset of the household (that is, the value of all the property, possessions, and money that the household has).
Underweight: Refers to a deficit and is defined as underweight if the weight-for-age index was below the -2 SD from the NCHS/WHO reference of the median of the standard curve. A severely underweight was diagnosed if weight-for-age was below-3 SD (CSA and ICFI, 2016; MOH, 2014).
RESULTS
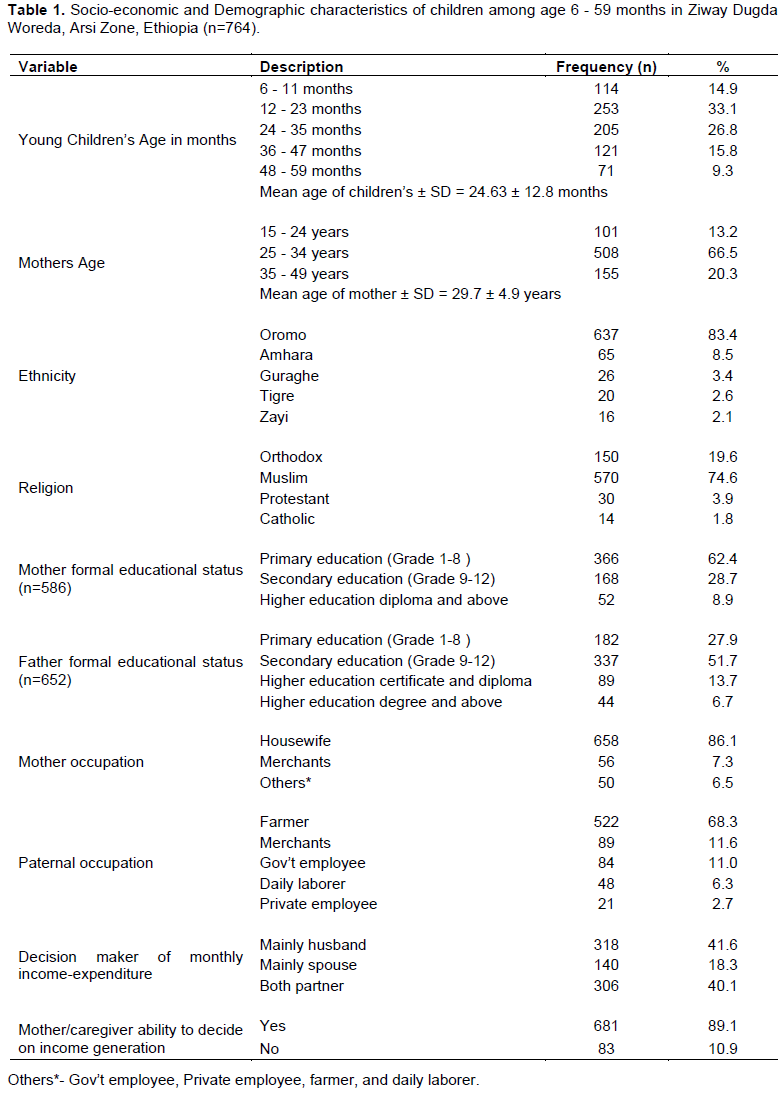
A total number of 750 children age 6 - 59 months were involved in this study who fulfilled the inclusion criteria, with the response rate of 764 (98.2%). Among all respondents, most 733 (95.9%) of the children lived in the male-headed household (Table 1).
Socio-economic and demographic characteristics
Of all 764 children in the study, 384 (50.3%) were male and 253 (33.1%) were found in the age group 12-23 months. The mean age of the participants was 24.63 ± 12.81 months. More than half 508 (66.5%) of the study participant's mothers' age was found in the age range of 25 to 34 years. The mean age of the study participant’s mother was 29.7 ± 4.9 years. Regarding ethnicity and religion, the majority of the study subjects were from the Oromo ethnic group and Muslim religion follower families, which accounts for 673 (83.4%) and 750 (74.6%), respectively. Six hundred and sixty-one (86.5%) parents of the participant were currently married, and 103 (13.5%) parents' marital status was reported to be divorced and widowed (Table 1).
About the formal educational status of the family of study subjects, about two-thirds of the mother 586 (76.7%) and fathers 652 (85.3%) had formal education. Out of them, more than half of children's mothers 366 (62.4%) and 337 (51.7%) fathers completed primary and secondary education, respectively. Similarly, the majority of the mothers 658 (86.1%) and fathers 522 (68.3%) were housewives and farmers in their occupation, respectively (Table 1).
Regarding the family size of the study subject households, the majority of the participants 443 (58.0%) lived in households of less or equal to five family size, but the remaining 42% of them lived in households of six and above family size. The mean family size ± SD of the study subject households was 5.47 ± 1.95. However, most of the study subjects 699(91.5%) had one to two under-5 children in their households, but only a few 65 (8.5%) of them had a maximum of four under-5 children. About the wealth status of the households of study subjects, the majority 356 (46.7%) and 343 (45.3%) of the study participants were present on the second and third quintiles of wealth status. Whereas, only 27 (3.5%) and 34 (4.5%), of the study participants were left on the highest and lowest quintiles of wealth status, respectively.
Maternal obstetric, child health care, and environmental-related characteristics
The majority of the age of mothers at first pregnancy and when the youngest children born were present in the age range of 20 - 24 and 25 - 29 years, respectively. The mean age of them was 21.4 ± 3.8 and 27.8 ± 4.9 years, respectively. More than half of the study participant's mothers, 444 (66.5%) started FANC visits at 16 - 28 weeks of gestational age. The mean GA of mothers of study subjects started FANC visit at 16 ± 4.1 weeks. However, only 211 (31.3%) of the mothers had four and more FANC visits as recommendations of WHO. More than one-third of mothers, 324 (42.4%), had a pre- pregnancy weight of 55 - 64 kg during the last pregnancy and followed by a mother who weighed 40 - 54 kg that accounts for 262 (34.3 kg) (Table 2).
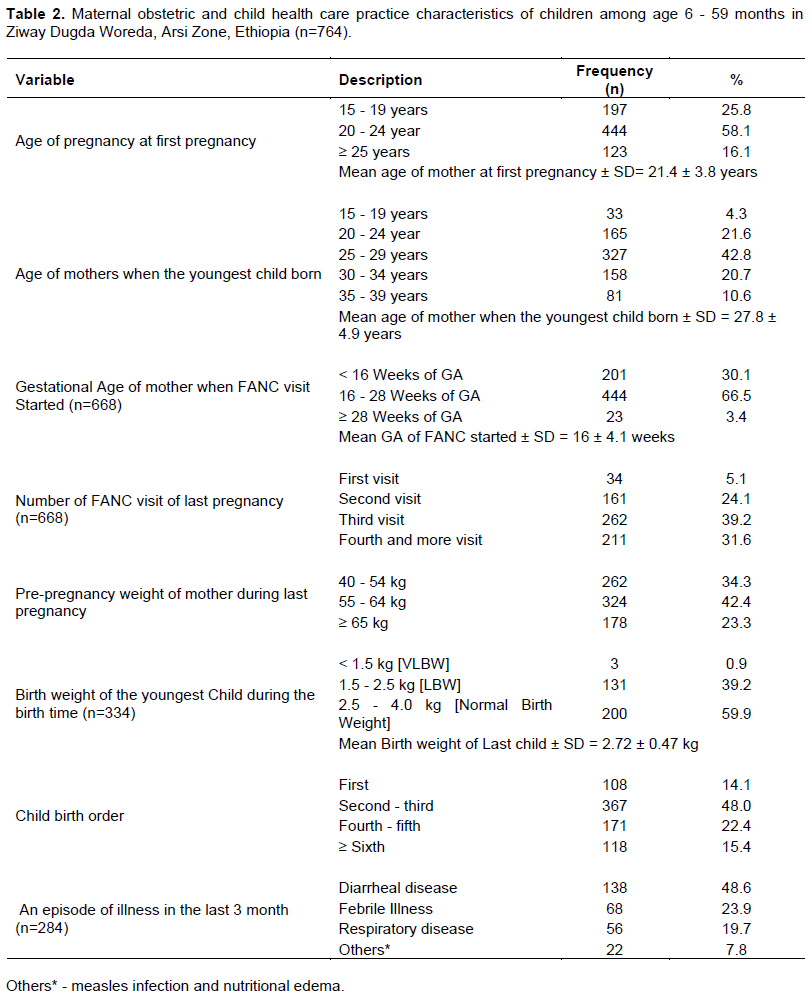
More than two-thirds of the mothers of study participants 614 (80.4%) had birth preparedness and complication readiness plan during the last pregnancy, whereas 150 (19.6%) of the mothers did not have the plan of preparedness. Even though the majority of mothers had birth preparedness and complication readiness plan, 41.8% of the mothers had their youngest child in their home with the help of traditional birth attendants, but 58.2% of the mothers had their youngest child in a health facility. About three-fourth of the youngest children 580 (75.9%) were term birth child (36 - 42 weeks GA of pregnancy); whereas 81 (10.6%) and 103 (13.1%) of the youngest children were a pre-term birth child (< 36 weeks GA of pregnancy) and post-term birth child (≥ 42 weeks GA of pregnancy), respectively. Among those children who weighed during the birth time “334”, the majority of the children 200 (59.9%) had normal birth weight and followed by low birth weight 131 (39.2%), but only 3 (0.9%) of them were very low birth weight babies. The mean birth weight of the youngest children was 2.72 ± 0.47 kg. Regarding birth order and birth spacing between children, nearly half of the children (48%) were present in the second and third birth order, and 648 (84.8%) of the study subjects mothers had good birth spacing as of WHO recommendation, that is, 2 years and above (Table 2).
About child care service, most of the children 738 (96.6%) received their vaccination timely. Out of them, the majority of the children 601 (81.4%) were fully immunized during their infancy age; whereas, the remaining 89 (12.1%) and 48 (6.5%) of the children were present on immunization schedule and not fully immunized, respectively. Also, 588 (77.0%) of the study subjects took vitamin A supplementation during National Immunization Days (NID), whereas the remaining 176 (23%) of them did not take vitamin A supplementation. Among all study participants, about one-third of the children 284 (37.2%) had a history of illness in the last 3 months. Out of them, 138 (48.6%) had an episode of diarrheal disease. The health facility was the major usual treatment place of sick children, which accounts for 199 (70.1%), whereas 29.9% of the sick children used home-based treatment and traditional therapy. One hundred and forty-four of the sick children (50.7%) visited health institutions for less than or equal to 2 times per the last 3 months (Table 2).
Regarding maternal health care, the majority of the children's mother 640 (83.8%) had awareness about the family planning method that was used for limiting the number of children in the family. In line with this, more than one-third of the study subject's mothers 607 (79.5%) had a history of family planning utilization. Among them, injectable (Depo-Provera), 267 (44.0%) and implant (Implanon Next®), 251 (41.3%) were the major family planning methods used by the mother, but the remaining 20.5% of the mothers have used pills, IUCD, and a condom as a method of family planning.
About the main source of drinking water of the households of the children, only 346 (45.3%) of the children had improved sources of water, such as public tab/stand tabs (26.6%) and protected spring water (18.7%); whereas the majority of the study subject households, 418 (54.7%) were not having improved source of water, such as private hand wells, unprotected spring, and river/pond water. Similarly, a small number of households of the children had improved toilet facilities (13.6%) and improved waste management (39.5%) to maintain environmental healthiness (Table 2).
Maternal and infant young child feeding practice-related characteristics
Regarding the responsible caretaker of the children, more than two-thirds of the children 679 (88.9%) were cared for by their mothers; whereas, 85 (11.1%) of the children were cared for by their grandmothers, sisters, and domestic workers.
According to WHO recommendation of optimal breastfeeding related to IYCF, the majority of the children initiated breastfeeding within hours of delivery 545 (71.3%), fed exclusive breastfeeding for 6 months 514 (67.3%), and breastfeed for a maximum duration of 24 months or more 593 (77.6%). More than half of the children, 431 (56.4%) were fed a minimum frequency breastfeeding day and night which is greater than or equal to 10 times per 24 h. Even though one-third of the mothers, 219 (28.7%) were not timely initiated breastfeeding as of recommendation, the majority of the study subjects' mothers, 659(86.3%) were given their colostrum (Table 3).
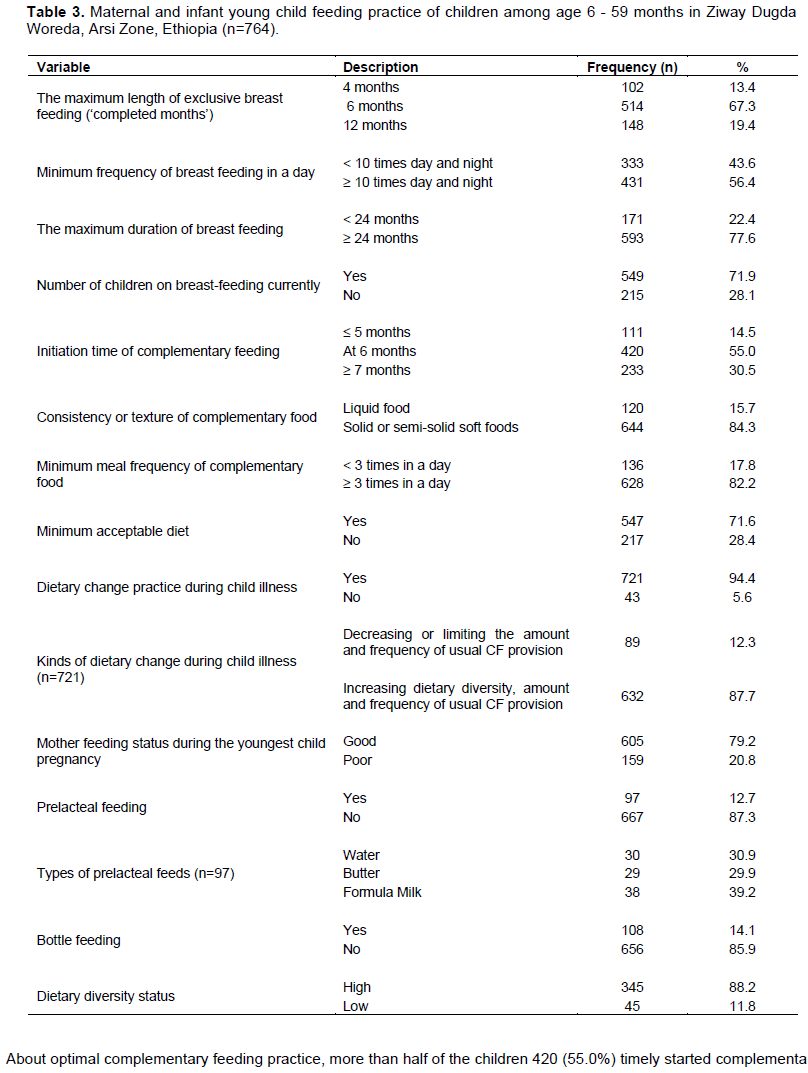
About optimal complementary feeding practice, more than half of the children 420 (55.0%) timely started complementary feeding at 6 months; whereas, the rest 45% of the participants started earlier before 6 months and lately at seven or more months contrary to WHO recommendation time of initiation. Also, the majority of the children, 674 (88.2%) and 644 (84.3%) took the highest dietary diversity foods and solid or semi-solid soft foods, respectively. Among those children who had high dietary diversity status, male children 346 (45.3%) had slightly higher dietary diversity status than that of female children, 328 (42.9%). Six hundred and twenty-eight (82.2%) of the children take a minimum meal frequency of complimentary food, that is, greater than or equal to 3 times a day. But, only 547 (71.6%) of the children take a minimum acceptable diet as the recommendation of IYCF. During the illness time of the children, most 721 (94.4%) of the mothers practiced dietary change intake of the children. Out of them, the majority 632 (87.7%) of the study participant mothers/caretakers have increased the dietary diversity, amount, and frequency of usual complimentary food provision; whereas, the remaining 89 (12.3%) decreased or limited the amount and frequency of usual complementary feeding provision (Table 3).
Contrary to WHO IYCF recommendation, a few numbers of children 97 (12.7%) take cultural pre-lacteal food before breast milk initiation. Out of them, 30.9 and 29.9% of the children were allowed water and butter, respectively. Also, 108 (14.1%) of the children were bottle feeders during the young infancy period (Table 3).
Among plant-based food, 539 (70.5%) and 702 (91.9%) of the study participant mothers/caretakers reported that they provide “grains, roots, and tubers”, and “legumes and nuts” based complementary foods to their children in the previous 24 h, respectively. Besides, 518 (67.8%) and 671 (87.8%) of the study participant mothers/ caretakers also reported that they were given a complementary food to their children prepared from a source of “other fruits and vegetables” and "vitamin-A-rich fruits and vegetables" in the previous 24 h, respectively (Figure 1).
Among animal-based foods, 617 (80.8%), 531 (69.5%), and 611 (80.0%) of the study participant mothers/ caretakers reported that they were given a complimentary food prepared from a source of dairy product (milk, yogurt, cheese), flesh foods (meat, fish, poultry, and liver/organ meats), and egg, respectively (Figure 1).
Regarding the overall infant young child feeding practice, more than half, 50.8 and 76% of the study participant had good optimal breastfeeding practice and complementary feeding practice, respectively. Even though the majority had good optimal breastfeeding and complementary feeding practice, only 41% of the respondents reported that their children had good infant young child feeding practice as of WHO IYCF recommendation.
Nutritional status of children age 6-59 months
WHO Anthro-plus 2006 was used to generate z-score values for weight-for-age, height-for-age, and weight-for-height. In the analysis stunting, wasting, and underweight were defined as having a Z-Score below -2 SD of the WHO standards.
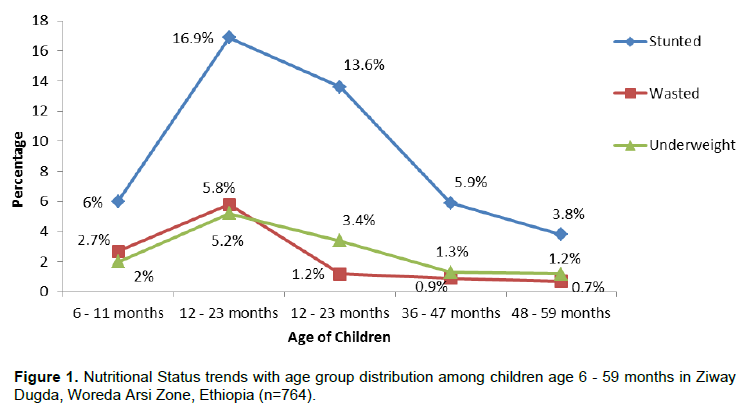
The prevalence of stunting among children of 6-59 months in the study area was 46.2% (42.7-49.7; 95% CI). Of them, 232 (30.4%) and 121 (15.8%) of the children were severely stunted and moderately stunted, respectively. In age distribution, from those stunted children, a higher percentage of stunted children were present in the age group of 12 - 23 months, 129 (16.9%), and followed by 24 - 35 months, 104 (13.6%) (Figure 1).
The prevalence of wasting among children of 6-59 months in the study area was 11.5% (9.4 - 14.0; 95% CI). Of them, 30 (4.0%) and 56 (7.5%) of the children were severely wasted (SAM) and moderately wasted (MAM), respectively. In age distribution, from those wasted children, a higher percentage of wasted children were present in the age group of 12 - 23 months, 43 (5.8%), and followed by 6 - 11 months, 20 (2.7%) (Figure 1).
The prevalence of underweight among children of 6-59 months in the study area was 13.1% (10.9 - 15.7; 95% CI). Of them, 37 (4.8%) and 63 (8.2%) of the children were severely underweight and moderately underweight, respectively. In age distribution, from those under-weighted children, a higher percentage of underweight children were present in the age group of 12 - 23 months, 40 (5.2%), and followed by 24 - 35 months, 26 (3.4%) (Figure 1).
Association of stunting with associated factors of study participants
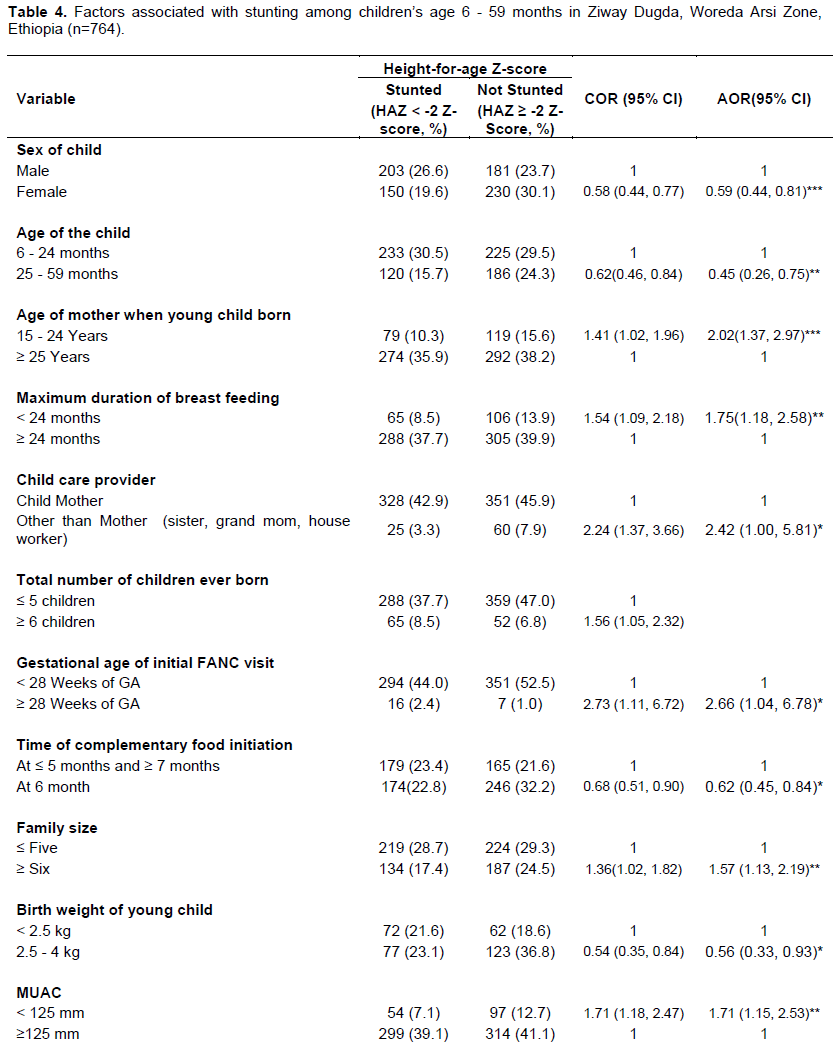
In the study, thirteen variables had a significant association with stunting in bivariate analysis with a p-value of <0.25, but only one variable did not have a significant association with multivariate logistic regression analysis. However, the finding of the study indicated that sex of the child, child age, age of the mother when a child was born, the maximum length of breastfeeding, child care provider, gestational age of initial FANC visit, time of complementary food initiation, family size, birth weight of the young child, wasting status (weight-for-height z-score), underweight status (weight-for-age z-score), and malnutrition status (MUAC) were identified as determinants of stunting among children in the study area in the multivariate logistic regression analysis.
Sex of the child and underweight status (weight-for-age z-score) had a highly significant association with stunting, that is, the odds of experiencing stunting was lesser among female children than that of male children/those children who had female sex were 41% less likely to be affected with stunting than those of male children [AOR=0.59, 95% CI (0.44, 0.81)], and those children who are not underweight (WAZ ≥ -2 Z-score) was 99.92% less likely to be affected with stunting than those of underweight children (WAZ < -2 Z-score) [AOR = 0.07, 95% CI (0.02, 0.30)]. Also, the age of the mother when a child born and wasting status (Weight-for-Height Z-score) also had a highly significant association with stunting, that is, those children born from a mother of age between 15 and 24 years were 2.02 times more likely to be affected with stunting than those children born from a mother age ≥ 25 years [AOR=2.02, 95% CI (1.37, 2.97)] and those children who are wasted (WHZ < -2 Z-score) were 5.76 times more likely to experience stunting than those children who are not wasted (WHZ ≥ -2 Z-score) [AOR = 5.76, 95% CI (2.24, 15.58)] (Table 4).
.png)
Moreover, child age, the maximum length of breast feeding, family size, and MUAC had a very significant association with stunting, that is, those children whose age range between 25 and 59 months were 55% less likely to be affected with stunting than that of children whose age between 6 and 24 months [AOR = 0.45, 95% CI (0.26, 0.75)]; those children who were fed breast for less than 24 months were 1.75 times more likely to be affected with stunting than that of children breast feed for greater or equal to 24 months [AOR = 1.75, 95% CI (1.18, 2.58)]; those children who are from greater or equal to 6 family size households were 1.57 times more likely to be affected with stunting than that of children who are from less or equal to 5 family size households [AOR = 1.57, 95% CI (1.13, 2.19)]; and those children whose MUAC < 125 mm were 1.71 times more likely to be affected with stunting than that of children whose MUAC ≥ 125 mm [AOR = 1.71, 95% CI (1.15, 2.53)] (Table 4).
Furthermore, gestational age of initial FANC visit, time of complementary food initiation, child care provider, and birth weight of young child had a significant association with stunting, that is, those children who started complementary feeding timely at 6 months and whose birth weight between 2.5 and 4 kg were 0.56, and 0.62 times less likely to be with stunting than those of children who started complementary feeding early or lately and with weight below 2.5 kg [AOR = 0.56, 95% CI (0.33, 0.93)] and [AOR = 0.62, 95% CI (0.45, 0.84)], respectively. Whereas, those children whose mother started FANC visit after 28 weeks of GA and those children who cared with other than mothers were 3.08 and 2.42 times more likely to be affected with stunting than that of children mothers who started FANC before 28 weeks of gestation and children who cared with own mother [AOR = 2.66, 95% CI (1.04, 6.78)] and [AOR = 2.42, 95% CI (1.00, 5.81)], respectively (Table 4).
DISCUSSION
Nutritional stunting, which is the height for age below that is expected based on international growth reference, is a very serious type of malnutrition in that it develops slowly through time before it is evident.
This study intended to assess the prevalence of stunting and associated factors among 6-59 month children in Zeway Dugda district. The prevalence of stunting in this study area was 46.2% (42.7-49.7; 95% CI) (that is 30.4% severely stunted and 15.8% moderately stunted). This study finding was almost comparable with studies conducted in Hidabu Abote districts of North Shewa of Oromia (47.6%) (Mengistu et al., 2013), in Bule Hora district (47.6%) (Mandefro et al., 2015) and Ataye town (48.4%) (Moges et al., 2019). However, the prevalence was higher than the study conducted in Sodo Zuria district (24.9 with 7.9% being severely stunted) (Dake et al., 2019), Shey Bench district of Southwest of Ethiopia (33.3%) (Teferi et al., 2016), Areka town (33.2%) (Desalegn et al., 2016), Hossana town (35.4%) (Beminet et al., 2015). On the other hand, the finding was lower than the study done in Lalibela town (51.1%) (Yalew, 2014), Wondo Genet Woreda (50.3%) (Woldie et al., 2015), Dabat district (64.5% with 37.7% and 26.8% being moderately and severely stunted, respectively) (Tariku et al., 2017). The variation in prevalence might be due to the difference in the socio-demographic, agro-ecological, and economical characteristics, sample size variation, and child feeding practice of the participants in the study area. From other countries, the finding was also higher compared with studies done in countries in Nigeria (29%)(Etim et al., 2017), Tanzania (35.5%) (Chirande et al., 2015), and Bangladesh (39.3%) (Das and Gulshan, 2017).
Like many other study findings, this study documented that the odds of being stunted was higher for males as compared to females. This finding was consistent with other study findings from Ethiopia (in Ataye), Nigeria, Tanzania, and Uganda where males have a higher risk of being stunted (Moges et al., 2019; Etim et al., 2017; Chirande et al., 2015; Bukusuba et al., 2017). On the other hand, our finding was different from other study findings from Ethiopia like Sodo Zuria district and Mehrabete Woreda, which reported that females had a higher chance of being stunted (Dake et al., 2019; Shiferaw et al., 2018). This may be due to cultural issues, gender preference, and differential feeding practice.
The age of the mother when a child born was one of the factors highly significantly associated with stunting in the study area. Comparing with those children born from a mother of age ≥ 25 years when their child was born, a child who was born from a mother of age 15 to 24 years was more likely to be stunted. This might be due to incomplete growth spurt mothers and inappropriate maternal nutrition practice during pregnancy time and lactation period among mothers age 15 - 24 years. Because of this, the mother might not fulfill the nutrient and energy needs of the child and as well for her body. Whereas, children whose ages between 6 and 24 months were more likely to be affected with stunting than that of children whose ages between 25 and 59 months. Our study finding was incomparable with the study findings of Geberselassie et al. (2018), Hana Moges et al. (2019), and Dake et al. (2019), which reported that those children whose age between 25 and 59 months had a higher chance of being stunted. Our study findings go with the trend of stunting peaks for each group of children age up to 35 months and then decline for children 36 to 47 months of age. The possible reason for more chance of being stunting in infant and young child period in our study area might be inappropriate complementary feeding practice and introducing children directly to household diet rather than well prepared complementary food provision. The other reason could be because stunting is chronic malnutrition and is commonly manifested after long-term nutritional deprivation.
The maximum duration of breastfeeding of the children were the other significant factors associated with stunting. Those children who had to breastfeed for less than a 24-month duration were more likely to be stunted than that of children who breastfeed up to 24 months of age and beyond. This finding was comparable with WHO IYCF's recommendation to fulfill the nutrient and energy needs besides with complimentary food (WHO, IFPRI, Davis UC, USAID, FANTA, 2010; Solomon et al., 2019). But, our finding was inconsistent with the study done in Hossana town, which reported that children who had to breastfeed for more than 24 months long were more likely to be stunted than children who breastfeed for less than 12 months long (Beminet et al., 2015). This variation might be due to poor awareness of IYCF practice and cultural variation. Also, children who started complementary food before and after 6 months were more likely to be stunted than that of children who initiated timely at 6 months. This study finding is in agreement with the study conducted in Shay Bench district and Merhabete Woreda (Teferi et al., 2016; Shiferaw et al., 2018). This might be due to inappropriate timing for introducing complimentary food to a child that may affect the nutritional status of the children as a result of immature digestive and immune systems. And also, introducing supplements earlier before 6 months, especially under unhygienic conditions, could be a predisposing factor for infection and it leads to malnutrition.
The family size of the study subject was the other variable that showed a very significant association with stunting. That means children who had family size greater than or equal to six were more likely to be stunted than those who had less or equal to five family members. Our finding was consistent with other studies done by Desalegn et al. (2016) and Geberselassie et al. (2018). This could be because families with more children are more stretched economically and cannot feed themselves well and face difficulty in providing the daily nutrition requirements for proper child physical development. This means as the size of a family increases resources is scarce for household consumption, especially food, and healthcare which ultimately leads to stunted growth. Furthermore, parents with more children generally lack adequate time to pay proper attention to the need of each child.
Mothers’ gestational age of initial FANC visit also showed significant association with child stunting. A child's mother who started FANC visit at a gestational age of greater or equal to 28 weeks during pregnancy was more likely to be stunted than that of children mothers who started FANC visit earlier before 28 weeks of gestation. This might be because, maternal nutritional and health status before, during, and after pregnancy influences a child's early growth and development beginning in utero and contributes importantly to the risk of stunting. Maternal undernutrition contributes to fetal growth restriction, which increases the risk of neonatal deaths and, for survivors, of stunting by 2 years of age (Black et al., 2008; Solomon et al., 2019). However, the appropriate time of FANC initiation of the mother is a great opportunity to improve the nutritional status of the fetus and as well the mother to reduce the incidence of stunting (Tadesse et al., 2016).
Birth weights of a young child were the other determinant factors for stunting in this study. Children who had born with low/small birth weight children were more likely to develop stunting than normal birth weight children. This finding was consistent with the study done in Hossana Town, Guto Gida District, Bangladesh, and Kenya (Beminet et al., 2015; Adeba et al., 2014; Kamal, 2011; Abuya et al., 2012). This might be due to the mother’s nutritional and health status before and during pregnancy which determined the size of the child during the intra-uterine period and birth outcome of the child. And also after birth, those low birth weight children were frequently predisposed to infection during infancy and childhood life which leads to malabsorption of nutrients in their body and favors stunting.
Child care provider during feeding is also the other risk factors that lead to stunting. This implies those children who cared with other than their mother was more likely to develop stunting. This might be low awareness, missing own mother, insensitive and inappropriate IYCF practice, and poor attention provision to the children. Also, those children whose anthropometric results of MUAC less than 125 mm and ‘WHZ and WAZ’ below -2 Z-score were more likely to be stunted than that of children whose anthropometric measurements of MUAC ≥ 125 mm, and ‘WHZ and WAZ’ greater or equal to -2 Z-score. This indicated that being stunting and underweight might lead to stunting if the deprivation of nutrient prolonged.
CONCLUSION
The overall prevalence of stunting in Zeway Dugda district was higher with low IYCF practice as compared to national prevalence and WHO recommendation and thus represents an important public health concern. Sex of the child, age of the child, age of the mother when a child was born, the maximum duration of breastfeeding, child care provider, gestational age of initial FANC visit, time of complementary food initiation, family size, birth weight of the young child, wasting status, underweight status and malnutrition status (low MUAC) were significantly associated factors for stunting. Stunting was found to be a result of maternal, socio-demographic, and child individual factors. These findings are of great importance because they identify potential actions that can be used to improve the nutritional status of the children. Immediate interventions targeted to community-based management of chronic malnutrition might be appropriate to manage stunting which is an indication of chronic malnutrition in the study. Prevalence of undernutrition may be due to inadequate infant young child and maternal feeding practice, therefore nutrition education on dietary diversity, feeding practice, and family planning should be provided. Special attention should be given to the adult literacy program to promote adequate feeding practice and to curb chronic nutritional problems. A community-based nutrition program should be strengthened as well as further study should be carried out to explore additional factors that might not be included in this study. Also, a strong nutrition-specific and sensitive intervention should be implemented in the study area with a special focus on supporting housewives, promoting family planning, and education on child feeding and nutrition. Moreover, it requires collaborative activity from national and regional health offices to reduce the burden of stunting. Furthermore, it requires the promotion of better child and maternal caring practices as well as further research in child-caring practices and dietary assessments.
ETHICAL APPROVAL
The study was approved by the Institution Review Board (IRB) of Adama General Hospital and Medical College. A letter of permission was taken from the Administration of Ziway Dugda Woreda Health Office from departments of public health. Consent was obtained from every relevant authority in the Woreda and assent was taken from every participant. Privacy and confidentiality were maintained throughout the study period by excluding personal identifiers from the data collection form. For malnourished children during the assessment, we were given health education on nutrition and building linkage to the organization that can manage the case and CBN program of the Woreda.
CONFLICT OF INTERESTS
The authors have not declared any conflict interests.
ACKNOWLEDGEMENTS
The authors thank the Institution Review Board (IRB) of Adama General Hospital and Medical College for their proper review and approval of this paper. They thank all respective departments of the college and Woreda officials for their support and permission to conduct this study and data collectors and participants.
REFERENCES
|
Abuya BA, Ciera J, Kimani-Murage E (2012). Effect of mother's education on child's nutritional status in the slums of Nairobi. BMC Pediatr 12(1):1-10. |
|
|
Adeba A, Garoma S, Gemede HF, Garoma W (2014). "Prevalence of stunting and associated factors of children among 6-59 months age in Guto Gida District, East Wollega Zone, Oromia, Ethiopia Prevalence," 29. |
|
|
Beminet M, Amsalu F, Solomon M, Feleke D (2015). Magnitude of Stunting and Associated Factors among 6-59 Months Old Children in Hossana Town, Southern Ethiopia. Journals of Clinic Research Bioethics 6(1):1. |
|
|
Berihun M, Azizur R (2013). 'Prevalence and Determinants of Chronic Malnutrition among Under-5 Children in Ethiopia'. International Journal of Child Health and Nutrition 2(3):230-236. |
|
|
Black RE, Allen LH, Bhutta ZA, Caulfield LE, Onis M de, Ezzati M (2008). Maternal and child under nutrition: global and regional exposures and health consequences. Lancet 371(9608):243-60. |
|
|
Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, Onis M De, Uauy R (2013). Maternal and child undernutrition and overweight in low-income and middle-income countries. The Lancet 382(9890):427-451. |
|
|
Bukusuba J, Kaaya AN, Atukwase A. (2017). Predictors of stunting in children aged 6 to 59 months: a case-control study in Southwest Uganda. Food Nutr Bull 38(4):542-53. |
|
|
Chirande L, Charwe D, Mbwana H, Victor R, Kimboka S, Issaka AI, Agho KE (2015). Determinants of stunting and severe stunting among under-fives in Tanzania: evidence from the 2010 cross-sectional household survey. BMC Pediatrics 15(1):1-13. |
|
|
CSA and ICFI (2016). Ethiopia Demographic and Health Survey 2016: Key Indicators Report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA. CSA and ICF. |
|
|
Dake SK, Solomon FB, Bobe TM, Tekle HA, Tufa EG (2019). Predictors of stunting among children 6- 59 months of age in Sodo Zuria District, South Ethiopia: a community based cross-sectional study. BMC Research Note 5(1):1-7. |
|
|
Das S, Gulshan J (2017). Different forms of malnutrition among under five children in Bangladesh: a cross sectional study on prevalence and determinants. BMC Nutrition 3 (1):1-12. |
|
|
Deconinck BP, Diene SM, Bernardo D, Adou P (2011). Summary Report by Hedwig; Community-Based Management of Acute Malnutrition Implementation in West Africa. |
|
|
De-Onis M, Brown D, Blossner M, Borghi E (2012). Levels and Trends in Child Malnutrition. UNICEF-WHO-The World Bank Joint Child Malnutrition Estimates, UNICEF, New York, NY,USA. |
|
|
Desalegn D, Egata G, Halala Y (2016). Prevalence of stunting and associated factors among children aged 6 to 59 months in Areka town, Wolaita Zone, Southern Ethiopia. Journal of Medicine, Physiology and Biophysics Vol. 21. |
|
|
Ethiopian Public Health Institute (EPHI) [Ethiopia] and ICF (2019). Ethiopia Mini Demographic and Health Survey 2019: Key Indicators. Rockville, Maryland, USA: EPHI and ICF. |
|
|
Etim KD, Ejemot-Nwadiaro RI, Kalu RE (2017). A study of malnutrition-dependent factors among under-five children in Ekureku Community, Abi Local Government Area of Cross River State, Nigeria. Journal of Advances in Medicine and Medical Research, pp. 1-10. |
|
|
Fentaw R, Bogale A, Abebaw D (2013). 'Prevalence of child malnutrition in agro-pastoral households in Afar Regional State of Ethiopia' Nutrition Research and Practice 7(2):122-131. |
|
|
Geberselassie SB, Abebe SM, Melsew YA, Mutuku SM, Wassie MM (2018). Prevalence of stunting and its associated factors among children 6-59 months of age in Libo-Kemekem district, Northwest Ethiopia; A community based cross sectional study. PLoS One 13(5). . |
|
|
Gibson RS, Ferguson FL (1999). An interactive 24-Hour recall for assessing the adequacy of iron and zinc intakes in developing countries. Washington D.C.: ILSI Press. |
|
|
Gossaye Y, Deyessa N, Berhane Y, Ellsberg M, Emmelin M, Ashenafi M, Alem A, Negash A, Kebede D, Kullgren G, Hogberg U (2003). "Butajira Rural Health Program:Women's health and life events study in rural Ethiopia 17(2):1-51. |
|
|
Ikeda N, Irie Y, Shibuya K (2013). Determinants of reduced child stunting in Cambodia: analysis of pooled data from three demographic and health surveys. WHO 91(5):341-349. |
|
|
Kamal SM (2011). Socio-economic determinants of severe and moderate stunting among under-five children of rural Bangladesh. Malaysian Journal of Nutrition 17(1). |
|
|
Mandefro A, Mekitie W, Mohammed T, Lamessa D (2015). Prevalence of undernutrition and associated factors among children aged between six to fifty nine months in Bule Hora district, South Ethiopia. BMC Public Health 15(1):1-9. |
|
|
Mengistu K, Alemu K, Destaw B (2013). Prevalence of malnutrition and associated factors among children aged 6-59 months at Hidabu Abote District, North Shewa, Oromia Regional State. Journal of Nutritional Disorders and Therapy 1(1):1-5. |
|
|
Moges H, Alemayehu D, Redi H, Gebeyehu Y, Dires A, Gedamu S (2019). Prevalence and Associated Factors of Stunting Among Children Aged Six Month - Five Year in Ataye Town, Northeast Ethiopia. International Journal of Nutrition Nutrition and Food Sciences 8(6):86-92. |
|
|
MOH (2014). Comprehensive Adolescent, Maternal, Infant and Young Child Nutrition. In MOHE, Facilitator Guide. Addis Ababa. |
|
|
Rah JH, Akhter N, Semba RD, De Pee S, Bloem MW, Campbell AA, Kraemer k (2010). Low dietary diversity is a predictor of child stunting in rural Bangladesh. European Journal of Clinical Nutrition 64(12):1393-1398. |
|
|
Ruel MT, Menon P (2002). Child feeding practices are associated with child nutritional status in Latin America: innovative uses of the Demographic and Health Surveys". Journal of Nutrition 132(6):1180-1187. |
|
|
Shiferaw A, Bereket G, Rajalakshmi M, Masresha A, Yohannes MA (2018). Stunting and Its Determinants among Children Aged 6-59 Months in Merhabete woreda, Northern Shewa Ethiopia: A Cross-Sectional Study. Hindawi Journal of Nutrition and Metabolism, page 8 |
|
|
Solomon D, Kebede Z, Bogale F, Ababor S, Ararso D, Woldie E, Getachew T, Mideksa S, Gebreyohannes Y, Hailu T, Kebede A. (2019). Reducing Stunting in Ethiopia: -From Promise to Impact: Evidence-Informed Policy Brief. Addis Ababa, Ethiopia. |
|
|
Tadesse M, Getabil F (2016). Factors Associated with Stunting of Under-Five Children in Ethiopia. |
|
|
Tariku A, Biks GA, Derso T, Wassie MM, Abebe SM (2017). Stunting and its determinant factors among children aged 6-59 months in Dabat District, northwest Ethiopia,. Italian Journal of Pediatrics 43(1):1-9. |
|
|
Teferi MB, Hassen HY, Kebede A, Adugnaw E, Gebrekrstos G, Guesh M (2016). Prevalence of Stunting and Associated Factors among Children Aged 06-59 Months In Southwest Ethiopia: A Cross-Sectional Study.. Journal Nutrition Health Food Science 4(6):1-6. |
|
|
Teshome B, Kogi-Makau W, Getahun Z, Taye G (2009). Magnitude and determinants of stunting in children underfive years of age in food surplus region of Ethiopia: the case of west gojam zone. Ethiopian Journal of Health Development 23(2):99-106. |
|
|
UNICEF, WHO, World Bank Group (2015). Levels and trends in child malnutrition.UNICEF/WHO/World Bank Group joint child malnutrition estimates. Key findings of the 2017 edition. Geneva. Retrieved January 22, 2018. |
|
|
UNICEF. Division of Communication (2009). Tracking Progress on Child and Maternal Nutrition. UNICEF, New York. |
|
|
UNICEF (2013). Improving Child Nutrition. The Achievable Imperative for Global Progress, United Nations Children's Fund 1-114. |
|
|
Victoria CG, Adair L, Fall C, Hallal PC, Martorell R, Richter L, Sachdev HS (2008). "Maternal and child under nutrition: consequences for adult health and human capital,". The Lancet 371(9609):340-357. |
|
|
WHO, IFPRI, Davis UC, USAID, FANTA (2010). Indicators for assessing infant and young child feeding practices part 2 measurements. Geneva,Sewizerland, World Health Organization. |
|
|
WHO, UN (2016). Habitat for a better urban future. Global report on urban health: equitable, healthier cities for sustainable development. World Health Organization. Geneva. |
|
|
WHO, UNICEF (2003). Global Strategy for Infant and Young Child Feeding. |
|
|
World Health Organization (WHO) (2014). Global health observatory (GHO) country statistics, Ethiopia. |
|
|
Woldie YT, Belachew T, Hailu D, Teshome T, Gutema H (2015). "Prevalence of stunting and associated factors among under five children in Wondo Genet Woreda, Sidama Zone, Southern Ethiopia,". International Journal of Medical and Health Sciences Research 2(2):36-49. |
|
|
World Health Organization (WHO) (2006). Standards for Maternal and Neonatal Care. Geneva: World Health Organization (WHO). Multicentre Growth Reference Study Group. 2006. . WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Height and Body Mass Index-for Age:Methods and Development. Geneva, Switzerland: WHO. |
|
|
World Health Organization (WHO) (2018). The WHO Child Growth Standards. Retrieved January 22, 2018, |
|
|
Yalew BM (2014). "Prevalence of malnutrition and associated factors among children age 6-59 months at lalibela town administration, North Wollo Zone, Anrs, Northern Ethiopia,". Journal of Nutritional Disorders and therapy 4(1):132. |
|
|
Ziway Dugda Woreda Health Office (2019). Background information or profile of Ziway Dugda Woreda. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


