Full Length Research Paper

ABSTRACT
Care quality is a major concern for healthcare settings. Because of its essential place in hospital management, Nurse Manager (NM) is a critical link in the care system. This study aimed to analyse the role and leadership of the NM in the care quality improvement at the Charles de Gaulle Pediatric Teaching Hospital (CHUP-CDG). This was a qualitative and descriptive study. Ten NMs from clinical services selected on a reasoned sampling basis participated in individual semi-structured interviews. Non-participant observations and a documentary review were carried out. Data collection was conducted from August 1st to 31st, 2017 at the CHUP-CDG. A thematic analysis based on the professional practice framework (PPF) of Oldland et al. performed. The NM’s role and leadership nurse covered three of the seven healthcare quality domains of the PPF, namely: (1) Promotion of safety; (2) Positive interpersonal behaviours; (3) Clinical leadership and governance. Four healthcare quality domains are not covered: Management of the environment, evidence-based practice, medical/technical competence, and person-centred care. The NMs of clinical services hold a special place at the CHUP-CDG. Consequently, the success of quality care improvement depends on their involvement and commitment in all the domains of healthcare quality.
Key words: Nurse manager, role, leadership, care quality improvement, hospital, pediatric.
INTRODUCTION
The quality of care is a major concern for healthcare settings (Phaneuf, 2012). As a factor that contributes the most to building confidence in the population (Jacquerye and Chagnon, 1999), it is also the one that gives meaning to healthcare systems (Phaneuf, 2012). As the place of the care user in society has evolved, it has led to its becoming more attentive and more demanding about the quality of care (Compagnon et al., 2013). It relies to a large extent on motivated nurses, judiciously deployed, and who practice in conditions that optimize their work experience (Filion-Côté, 2014). Healthcare managers have a legal and moral obligation to ensure a high quality of patient care and to strive to improve care (Parand et al., 2014). According to Parand et al. (2014), they are in a prime position to mandate policy, systems, procedures, and organisational climates. In a rapidly changing healthcare environment, NMs face significant pressures (Krugman and Sanders, 2016). As key personnel in the care organisation, they play an essential role in the delivery and coordination of care, the prevention of adverse events, and the optimization of health service productivity and patient outcomes (Aiken et al., 2014).
In Burkina Faso, healthcare offered does not always meet the criteria of permanent availability, integration, continuity, comprehensiveness, and satisfaction of the populations, which most often lead to a poor perception of users towards healthcare settings (Ministère de la Santé, 2003). This is why improving the quality of services and healthcare has been and remains a national concern, all the more justified given the numerous complaints from users (Ministère de la Santé, 2016). Several studies document the quality of care and the leadership of nurses. However, NM’s role and leadership in improving the quality of hospital care remains poorly documented. This research aims to analyse the role and leadership of NM in improving the quality of care at CHUP-CDG, based on the PPF of Oldland et al. (2020).
RESEARCH METHODOLOGY
Research design
A qualitative and descriptive study was conducted.
Description of the research context
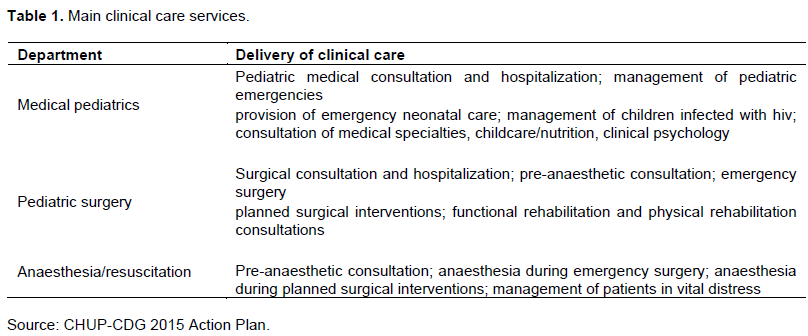
The CHUP-CDG is one of four 3rd level hospitals in Burkina Faso, located in Ouagadougou. As a national referral hospital for pediatric care, it has the mission to (1) offer specialized care to children and adolescents from zero to fourteen years old; (2) ensure the training of students and trainees in various disciplines; (3) develop research activities in its domain of ??expertise and provide its expertise to national and international requests. The CHUP-CDG has several directorates. The directorate of hospitalization and quality of care comprises medico-technical services and clinical services. Clinical services include Medical Pediatrics, Pediatric Surgery, and Anaesthesia/Resuscitation departments which include together the care units following: Infants, Older Children, Infectious Diseases, Pediatric Oncology, Medical Emergencies, Pulmonology and Allergology, Neonatology, External Consultations, Surgical Emergencies, Operating Room, Surgery/Hospitalization, Functional Rehabilitation/Physiotherapy, Anaesthesia and Multipurpose Resuscitation (CHUP-CDG 2015). The study field covers all these care units. The main clinical care services are provided in Medical Pediatrics, Pediatric Surgery, and Anaesthesia/Resuscitation departments (Table 1).
Description of the theoretical framework
The PPF of Oldland et al. (2020)includes seven healthcare quality domains (Figure 1):
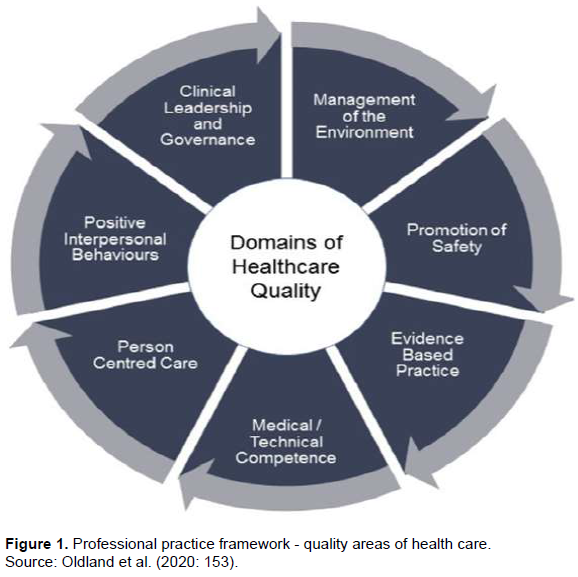
Management of the environment: Encapsulates nurses’ responsibilities to maintain an appropriate, healing physical space in which a health care service is delivered (Oldland et al. 2020).
Promotion of safety: Refers to nurses’ responsibility to provide care that minimizes risks and harm to themselves and service users. It avoids injuries to patients from the care that is intended to help them (WHO 2006).
Evidence-based practice: Involves giving consideration to the best available evidence; the context in which the care is delivered; client preference; and the professional judgment of the health professional (Pearson et al., 2005).
Medical and technical competence: Refers to discipline and context-specific knowledge and psychomotor skills registered nurses need to provide quality healthcare (Oldland et al., 2020).
Person-centred care: Nursing care that takes into account the preferences and cultures of individual service users and their communities (ACSQHC, 2011).
Positive Interpersonal behaviours: Refers to the communication skills, team behaviours, and personal attributes that promote safe and quality healthcare (Oldland et al., 2020).
Clinical Leadership and Governance: Refers to registered nurses’ behaviours that provide direction and support to clients and the healthcare team in the delivery of patient care (Patrick et al., 2011).
Regarding the PPF of Oldland et al. (2020), the elements of NMs’ role and leadership can be categorized into the three domains of healthcare quality following:
i) Promotion of safety: Development and implementation of procedures, protocols, and tasks’ description, follow-up of care traceability, check of technical activities implementation according to standards, methods, and requirements.
ii) Positive interpersonal behaviours: Information and communication management, assessment of professional skills and practices of the staff.
iii) Clinical leadership and governance: Planning of care unit’ activities, decision-making, mobilization and motivation of care teams, implementation of strategies and actions to improve quality, continuous training of staff and supervision of trainees; and building of care unit’s organisational culture.
Population and sampling
The population in this study included NMs working at the CHUP-CDG. Reasoned sampling with a maximum of variation made it possible to target ten NMs of clinical services according to the concordance of their characteristics with the research goal and objectives (sex, seniority, professional experience, diversity of care units). The sampling criteria included NMs with basic training as a nurse or midwife and working for a minimum of two years of seniority as NMs at the CHUP-CDG.
Data collection
Data collection was conducted from August 1st to 31st, 2017 at the CHUP-CDG. It consisted of semi-structured individual interviews, non-participant observations, and a documentary review. The interview guide was pre-tested in a similar hospital and validated by the research team. The interviews have been recorded, and data saturation occurred at the 10th interview. Observation in the situation, free and disengaged, combined with taking notes in a logbook was used. It took place during the working hours of NMs, from 7:30 a.m. to 4:30 p.m., and concerned both the activities and the general behaviour of NMs. The field observation notes and documentary review were written in the logbook.
Data analysis
A textual transcription of interviews was conducted, followed by in-depth reading and description of the data crossed with that of the logbook and the documentary review. Data coding, coding verification, data export, and synthesis were performed using RQDA software. A thematic analysis based on the PPF was performed. A triangulation was performed with official and unofficial documents. Data were categorized according to the domains of the PPF.
Ethical considerations
This research was approved by the Ethics Committee for Health Research of Burkina Faso (deliberation N° 2017-6-088, June 07th, 2017). Permission to collect data was obtained from the CHUP-CDG (authorization N° 2017-000798 -MS/SG/CHUP-CDG/DG/DRH/SRF, May 23th, 2017). Informed consent of NMs was obtained verbally and in writing by the researcher. Interviews verbatim have been coded.
RESULTS
Characteristics of participants
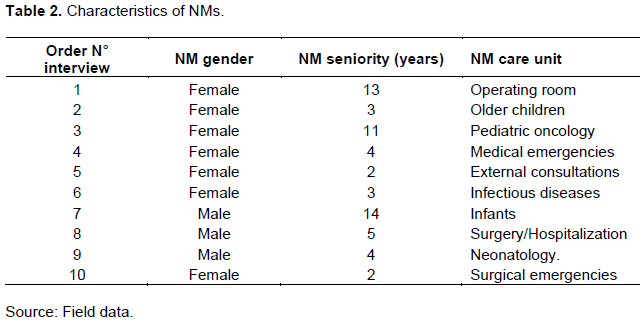
Ten NMs were interviewed. Distribution by gender is three men for seven women. Average seniority in function is six years with extremes of two years and fourteen years (Table 2).
Role and leadership of NMs in improving the quality of care
The analysis of interviews’ results made it possible to gather together the ideas common to NMs while retaining the most significant verbatim. NMs’ activities fall into three healthcare quality domains of the PPF of Oldland et al. (2020): promotion of safety, positive interpersonal behaviours, clinical leadership and governance.
Promotion of safety
Development and implementation of procedures, protocols, and tasks’ description improve the quality of care. The NMs insist on the importance of using these tools. Without having all of them, some NMs claim to have participated in the development of some of these tools. Many NMs have participated in the development of specific care procedures and protocols; however, its implementation is slow to materialize as attested by NM3 (F11):
We do not have all the protocols [...]. Otherwise, there are a lot of protocols, which are not being applied at the moment. However, there are all the same […] types of transmission, mouthwashes, handwashing […]! It is posted, and people are reading but, […] when you pick up somebody washing their hands, you see, it is in front of them, but they do not follow.
Tasks’ description is a description of the activity carried out by an agent in the care unit that takes into account his work environment, including service and any supervision. As a communication tool, it offers the opportunity for staff to interact with their direct supervisor. Interviews reveal that the tasks’ description has not yet been developed by NMs and is not used.
By checking acts notification through documents such as consultation, care, and hospitalization registers, care instructions books, and the patient's file, NMs follow up the care traceability. However, they noted that is not optimal, despite their appeals to the caregivers, as NM1 (F13) attests:
[…] The nurses do not take what it may be doing seriously. Otherwise, their attention has always been drawn to always note what they are doing […]; if it is not noted we will not see workload. […]. We must make an effort in this direction […] to try to promote what we do.
The notification of care acts by the caregivers remains incomplete, in particular, the filling in of the nursing file, an integral part of the patient's file, as indicated by NM3 (F11):
[…] Some nurses write in full; others do not. In the patient's file, there is a nursing file. It must be used. Patients can come in and go out without anything being noted on this file!
According to NMs, technical activities are not always carried out according to standards, methods, and requirements. However, certain conditions that NMs oversee are respected, in particular, compliance with the medical prescription and the care plan.
Positive interpersonal behaviours
Information and communication management boils down to the dissemination of memos from hospital management, internal information within the care unit and between NMs, and interpersonal and inter- NMs communication, as evidenced by NM3 (F11):
[…] We try to convey to staff whatever information we receive from the hierarchy. Memos are posted […]. We have a fleet, with the NM and the hierarchy. Between NMs we can call each other and also with some departments such as Emergencies, Ambulance, Maintenance. […]. There are monthly meetings, extraordinary meetings when there is urgent information to give.
Professional skills assessment is annual and consists of awarding a score to the agent during an individual and concerted interview between him and the NM. According to NMs, it is an administrative formality that does not allow an objective assessment of professional skills because it is not based on a contract of objectives previously assigned to the agent. What NM1 (F13) reports:
We could have improved that by setting objectives in advance and then follow up with staff to see if indeed those objectives were achieved at the end of the year before writing them down. This is not a good assessment of skills; at the beginning, there was no contract of objectives assigned to the staff!
Professional practices represent all health care, prevention, and education activities. To assess it consists of measuring the gap between these practices and benchmark behaviours. In the care unit, the assessment is limited to the routine observation of NMs and the correction of any observed deviations. For many NMs, the lack of validated assessment tools does not allow assessment of professional practices that could improve the quality of care. According to NMs, it is also essential that their role in its implementation be affirmed by hospital management. Health personnel should be sensitized too in order to reduce possible resistance.
Clinical leadership and governance
Activities’ planning consists of planning working time, on-call duty, and staff leaves. It is also about updating the care schedule, on-call book, care instructions book, and developing the micro-plan for the care unit which, along with micro-plans from other care units will be used to develop the hospital's action plan. It is fully ensured by NMs, and its impact on improving the quality of care has been underlined. From the development of the micro plan to the validation of the hospital action plan, the involvement of NMs is effective, and its participation is active, as attested to by NM5 (F2):
We do the first draft, […] we submit it to the head of the unit, and afterwards, together with the staff of the unit, we still try to rework it, and what they propose […], we take into account before submitting it, the micro plan, to hospital management.
Decision-making in the care unit is mostly collective. It focuses on communication, consultation, and involvement of the personnel, with Chief Medical Officer (CMO) approval. According to NMs, important decisions are often taken during staff meetings and care transmissions.
The NMs mobilize and motivate care teams to carry out activities by using group facilitation, communication, active listening and receptivity to personnel expectations, and recognition of work well done. This aims to create a work climate conducive to improving care quality. The NM presence among the personnel, her participation in social events for the care team members, and the initiation of recreational activities strengthen the group cohesion, as highlighted by NM7 (M14):
It is group animation, communication, presence, [...] in the group, in the field with the staff. Other sources of motivation are especially social actions. When there is an unfortunate or happy event with an agent, we must immediately mobilize others so that we can make home visits; this is very important. It helps to motivate the staff!
Quality improvement actions are being implemented following the adoption of strategies to resolve dysfunctions and improve the quality of patient care, as pointed out by NM3 (F11):
Together with the hygiene department, we have set dates for the disinfection of patients’ rooms, […] once a month, our rooms are disinfected, and we have also been able to install handwash basins in front of each hospital ward. […] All entering should wash their hands before entering in care room. Since, […] a clear improvement, in terms of hygiene. […] Many children fell into the aplastic infection, but since we started, it has been okay!
The interaction between care teams during meetings promotes the better implementation of strategies and efficiency of the coordination of quality improvement actions. These strategies and actions are taken in consultation with the CMO and the staff.
Provided by the NM and the CMO, continuous training took place during medical visits, clinical staffs, care transmissions, and through exchanges and discussions on previously prepared topics presented at the meetings of the care unit. Feedback of training workshops by NMs or agents is also a moment of continuous training for the staff. According to some NMs, although important, this role is not often seen as a priority by hospital management. In order to strengthen continuous training, NM8 (M5) suggests advanced training courses, inter-hospital exchanges, and training workshops. To accomplish its training mission, CHUP-CDG receives medical trainee students from two universities, nursing trainee students, and hospital hygiene technician trainee students from the National School of Public Health and private health schools. NMs mainly provide supervision for nurse trainees and hospital hygiene technician trainees, in collaboration with the care unit staff. They support them in achieving internship objectives, follow up learning, and participate in the internship assessment. The involvement of NMs in the coaching is active, despite the plethora of trainees which does not allow effective coaching; as evidenced by NM2 (F3):
[…] supervisor must really have a very strong eye on the trainees. The workforce is so bloated that when they come, they think this is a place to go, play and you go! When you are a little staring and feel that you are getting involved too, you have to get involved, don't be Major [...] in office; you have to be on the field with them, to supervise them!
NM’s leadership was used to improve the quality of care and excellence in the CHUP-CDG through the building of organisational culture. It emerges out of interviews, respect, and humanism towards the patient, communication, active listening, and respect for working hours, work attendance, example, professional skills, and accountability. According to NMs, they work in building the care unit’s organisational culture.
DISCUSSION
This research aims to analyse NM’s role and leadership in improving the quality of care. More than ever, the rapidly changing healthcare environment demands highly refined management skills and exceptional leadership (Sullivan, 2012).
Summary of the main findings
Based on the PPF of Oldland et al. (2020)(Figure 1), the elements of NMs roles in the CHUP-CDG cover three of the seven healthcare quality domains: (1) promotion of safety, (2) positive interpersonal behaviours, and (3) clinical leadership and governance.
Promotion of safety
The follow-up of care traceability is ensured by NMs, which allows them to monitor the notification of the care activities implementation and to make caregivers aware of the need to notify all care acts. Most care procedures and protocols are not developed, so care administration is not standardized. The task’s description is not developed, so workstations clearly defining the tasks of staff are not described. Without the task’s description and systematic use of care procedures and protocols, checking of technical activities implementation according to standards, methods, and requirements is not effective.
Positive interpersonal behaviours
Information and communication management is effective in the care unit. It allows NMs to coordinate work and organise staff for delivering continuous care. Assessment of the professional practices of the staff is not effective. Also, the assessment of professional skills made is not objective because it is not based on a contract of objectives previously assigned to the staff. This context does not help to improve the quality of care.
Clinical leadership and governance
The planning of activities is carried out by NMs, which promotes care continuity and service permanence. By mobilizing several elements belonging to their leadership in decision-making, they involve the staff. That creates a friendly, constructive, and productive working climate, favourable to better inter-professional collaboration and good coordination of care activities. They mobilize and motivate the care teams to carry out activities that creates a relationship of trust and group cohesion. These conditions are conducive to personnel adherence to the implementation of quality actions. The implementation of quality improvement strategies and actions ensured by NMs in collaboration with the staff is effective and productive. Continuous training of staff and supervision of trainees provided by NMs helps to strengthen the knowledge, skills, and professional practices of staff, as well as the learning of trainees. Promotion of values, attitudes, conduct, principles, and rules by NMs participate in building the care unit’s organisational culture.
Comparison of results with the literature
As an integrative entity of hospital activity, the care unit is a strategic location within the hospital. It is both the closed field of the care function-oriented according to a coordinated division of labour and the space open to all the professional, functional, and administrative interfaces of the overall hospital organisation (Ait Chitt, 2006). The commitment and work of hospital managers can influence clinical outcomes, processes, and performance of quality and safety (Parand et al., 2014).
Promotion of safety
Nurses play a central role in providing safe and high-quality care, and NMs are an integral part of this process as managers and leaders within organisations (Weiss and Tappen, 2015). NM’s role in the development and implementation of protocols, procedures, and tasks description is essential in improving the quality of care. As pointed out by McFadden et al. (2006), the development of procedures is part of a strategy to improve the quality of care by bringing about positive changes. The standardization of practices also contributes to this (HAS, 2014). NCUM is a key player in ensuring the quality of care (Karna, 2012). Our results differ from those of Coulon (2011)who showed very frequent follow-up of control and compliance with treatment protocols. According to Crommelynck et al. (2013), turning of data collection and processing into actionable information is gaining more and more importance, hence the need for care traceability follow-up. As indicated by Coulon (2011), NM occupies a unique place in the “world of care”. She no longer heals but supervises (world of control) under the responsibility of doctors (world of treatment). Check of technical activities implementation according to standards, methods, and requirements consists of daily follow-up of the work execution by the caregivers and is mainly the responsibility of local managers (Jounin and Wolff, 2006).
Positive interpersonal behaviours
Information and communication occupy a central place in the care unit’s management. Communicating optimally means being available and attentive as well as showing consistency and respect towards the staff (Moulin, 2012). In this regard, the role of NMs is effective. This result is similar to that of Djoumbé (2008), who reveals that NMs provide staff with information on the problems, actions, and performance of the care unit. The author highlights the holding of service meetings and clinical staffs among the communication mechanisms that aims for information and discussion with care teams. According to ANAES (2002), the assessment methods of professional practices make it possible to measure the conformity of practices with accepted references, to observe deviations, to analyse its causes, and to implement corrective actions. Assessment of professional skills and practices of the staff is not meaningful although it is necessary for the clinic because it makes it possible to "develop a knowledge of how to act in a situation" (Aiguier and Cobbaut, 2016).
Clinical leadership and governance
The manager's influence in an organisation is most evident in his leadership role (Mintzberg, 2004). It is recognized that NM’s leadership is an important component that fosters the professional practice environment for the staff (Beaudet, 2008). Evidence suggests that NM’s leadership has a direct impact on the performance of hospital nursing care units (Casida and Parker, 2011). According to Sullivan and Decker, quality of care is directly proportional to the quality of leadership. Effective clinical leadership is offered as the key to a healthy, functional, and supportive work environment for nurses (Mannix et al., 2013). So, effective nurse leaders are vital to accomplishing the goal of a healthy work environment (Blake, 2012). The NMs must deploy their leadership to develop the potential of the care teams, use their capacities for observation and analysis of situations, be able to make concerted decisions and work collaboratively for continuous quality improvement (ACQ). Through their leadership, they can influence practices that either promote or decrease patient safety (Merrill, 2015). The NM’s role in activities planning and staffing is essential to improving the quality of care. Crossan (2003)indicates that the levels of involvement and participation in the development of strategic planning vary from individual to others. The leadership of NMs in improving the quality of care through decision-making is effective at the CHUP-CDG. They take into account the ideas and suggestions of the care teams. This way of working develops their ability to take initiatives, their motivation, promotes teamwork and favours the quality of the climate (Moulin, 2012). In terms of patient care organisation and care unit’s performance, the contribution of NMs is significant (Coulon, 2011). At the CHUP-CDG, the mobilization, and motivation of care teams are effective. Evoking the essential role of team mobilization recognized by care unit managers in an AQC approach, Djoumbé (2008)finds it marginal for some NMs. Our results differ from those of Djoumbé (2008).
According to Parand et al. (2014), the managers’ work can influence clinical outcomes, processes, and performance in terms of quality and safety. Improvement actions are corrective actions initiated and implemented by NMs in collaboration with the staff and the CMO in order to improve the quality of care. As part of the continuous training of staff and the supervision of trainees, NM’s role is essential in improving the quality of care. The NM’s role as trainer, teacher, and resource person for staff and trainees appears in this context (Hubinon, 2004). Continuous trainee aims to acquire personal, professional, and social knowledge and skills that complement or reinforce recognized basic training. The promotion of a quality culture is essential for improving the quality of care. It requires adhesion, mobilization, active participation, and empowerment of staff and relies on internal communication, discussions, and regular meetings (HAS, 2014). As leaders, NMs demonstrate the profession’s values ??and standards, while creating an empowering environment for the staff (Weiss and Tappen, 2015).
Implications for research and practice
It is widely recognized that developing the role and leadership of NM contributes to growth towards improved performance (Krugman and Sanders, 2016). This research reveals that the role and leadership of NMs at CHUP-CDG do not cover four of the seven healthcare quality domains of the PPF of Oldland et al. (2020): Management of the Environment, Evidence-Based Practice, Medical/Technical Competence and Person-Centred Care. Based on this PPF, more in-depth research could be considered to assess the quality of care provided at CHUP-CDG. From a practice perspective, a definition of NM’s roles taking into account the four domains not covered could help improve the quality of care. As Sullivan (2012)points out, NMs need a very different set of knowledge and skills from those required in the practice of nursing, but few nurses have the necessary education or training to become managers. This research could enlighten early hospital managers and decision-makers on the need to develop high-quality, competency-based education and training programs for NMs in order to strengthen ACQ. These programs must be adapted to their context of clinical and managerial practice and target their learning needs (Kakyo and Xiao, 2017).
Limitations and strengths of the research
The results of this research must be viewed in light of three limitations. The first relates to the subjectivity that could taint the collection of data based on the perception of NMs as well as the subjective interpretation of the results and source of bias. In order to reduce it, the "method overlap" principle through the use of several investigative techniques during data collection (Ferréol, 2002)was applied. The 2nd is related to the Hawthorne effect. In order to reduce it, the reason for the investigation was communicated to NMs, without revealing that they will be under observation, and we have developed a practice of reflexivity. The 3rd is related to the small number of analysis cases which could limit results transferability. However, with the varied sample, detailed case studied descriptions (Table 1), and in-depth exploration considering the context, the results could be transferred to other similar teaching hospitals.
This research work has strengths that should be highlighted. To our knowledge, it is one of the first to explore the role and leadership of NMs in improving the quality of care in teaching hospitals in Burkina Faso. As a pioneer, it could prove useful for similar research projects in other teaching hospitals. The use of triangulation of sources and methods (Polit and Beck, 2012)in order to limit biases relating to the collection (Miles and Huberman, 2003)made it possible to verify that the data represented reality. The researcher ensured the conclusions’ accuracy with interviewees by ensuring an agreement degree between meaning attributed by the researcher and its plausibility in the eyes of the subjects. His interpretation was compared to similar researches.
CONCLUSION
New challenges for hospitals are to maximize the satisfaction of nurses and their involvement in the organisation, so that they provide care that meets quality requirements while ensuring patient satisfaction; doing this in a more participatory management method, based on the mobilization and empowerment of nurses (Hubinon and Grimmiaux, 2002). A NM’s contribution is capital to addressing these challenges, given the place and strategic position she occupies in hospital management. Effective clinical and managerial leadership of NM could be a source of satisfaction for patients and users of healthcare and services; motivation and accountability for providers and care teams; excellence, visibility, and prestige for the hospital.
CONFLICT OF INTERESTS
The authors ave not declared any conflict of interests.
ACKNOWLEDGMENTS
We thank Dr Félicité Wendin-manegdé Nana, Quality specialist, Public health researcher, Director of Care quality and patient safety, for her teachings in Care Quality Management and in Quality Planning at the IFRISSE. We thank Mrs. PAFADNAM / SANA Fatou for her moral support. Finally, we thank the “Institut de Formation et de Recherche Interdisciplinaires en Sciences de la Santé et de l’Education” in Ouagadougou, Burkina Faso for its assistance.
REFERENCES
|
ACSQHC (2011). Australian Safety and Quality Framework for Health Care: Getting Started Guide for The Healthcare Team. |
|
|
Aiguier G, Cobbaut JP (2016). Chapitre 1. Le tournant pragmatique de l'éthique en santé?: enjeux et perspectives pour la formation.Journal international de bioéthique et d'éthique des sciences 27(1-2):17-40. |
|
|
Aiken, Linda H, Douglas M Sloane, Luk Bruyneel, Koen Van den Heede, Peter Griffiths, Reinhard Busse, Marianna Diomidous (2014). "Nurse Staffing and Education and Hospital Mortality in Nine European Countries: A Retrospective Observational Study.The Lancet 383(9931):1824-1830. |
|
|
Ait Chitt H (2006). Références de management?: vers la gestion de l'unité des soins. |
|
|
ANAES (2002). Principes de mise en œuvre d'une démarche qualité en établissement de santé.Agence Nationale d'Accréditation et d'Évaluation en Santé. |
|
|
Beaudet G (2008). Relation entre le ratio infirmières-patients, la composition des équipes soignantes et la perception de l'environnement de pratique des infirmières. Montréal: Université de Montréal. |
|
|
Blake N (2012). Practical Steps for Implementing Healthy Work Environments. AACN Advanced Critical Care 23(1):14-17. |
|
|
Casida J, Parker J (2011). Staff Nurse Perceptions of Nurse Manager Leadership Styles and Outcomes: Nurse Manager Leadership Styles and Outcomes.Journal of Nursing Management 19(4):478-486. |
|
|
CHUP-CDG (2015). Plan d'action 2015 du Centre Hospitalier Universitaire Pédiatrique Charles de Gaulle.Document inédit. |
|
|
Compagnon L, Philippe B, Jean-François H, Bertrand S, Christian G, Yves Z, Claude P (2013). Définitions et descriptions des compétences en médecine générale. Exercer La Revue Française De Médecine Générale 24(108):148-155. |
|
|
Coulon R (2011). Cadres de santé, gestion des soins et contrôle de gestion. Cahier du FARGO. |
|
|
Crommelynck Anja, Katelijn D, David L (2013). L'organisation et le financement des hôpitaux. |
|
|
Crossan F (2003). Strategic Management and Nurses: Building Foundations. Journal of Nursing Management 11(5):331-335. |
|
|
Djoumbé E (2008). Le rôle de l'infirmier-chef de l'unité dans l'amélioration continue de la qualité.Rabat, Maroc: Institut de Formation aux Carrières de Santé. |
|
|
Ferréol G (2002). Dictionnaire de sociologie. 3rd ed. Paris: Armand Colin. |
|
|
Filion-Côté M (2014). Les conceptions et préférences des infirmières quant aux modalités de l'organisation de leur travail. Montréal, Québec: Université de Montréal. |
|
|
HAS (2014). Manuel de certification des établissements de santé V2010. Haute Autorité de Santé. |
|
|
Hubinon M (2004). Management des unités de soins: de l'analyse systémique à l'évaluation de la qualité. Bruxelles: De Boeck. |
|
|
Hubinon M, Grimmiaux V (2002). Les indicateurs du département infirmier pour une gestion prévisionnelle. |
|
|
Jacquerye A, Chagnon M (1999). La qualité des soins: implantation, évaluation, accréditation. Sciences infirmières. Paris: Maloine. |
|
|
Jounin N, Wolff L (2006). Entre fonctions et statuts, les relations hiérarchiques dans les établissements de santé. Recherche 32. Noisy-le-Grand: Centre d'études de l'emploi. |
|
|
Kakyo TA, Xiao LD (2017). Nurse Managers' Experiences in Continuous Quality Improvement in Resource?poor Healthcare Settings. Nursing and Health Sciences 19:244-249. |
|
|
Karna M (2012). Infirmière-chef?: acteur clé pour assurer la qualité et la sécurité des soins. Montréal, Québec: Université de Montréal. |
|
|
Krugman ME, Sanders CL (2016). Implementing a Nurse Manager Profile to Improve Unit Performance. The Journal of Nursing Administration 46(6):345-351. |
|
|
Mannix J, Lesley W, John D (2013). Attributes of Clinical Leadership in Contemporary Nursing: An Integrative Review. Contemporary Nurse 45(1):10-21. |
|
|
McFadden KL., Gregory NS, Charles RG (2006). Exploring Strategies for Reducing Hospital Errors. Journal of Healthcare Management 51(2):123-135. |
|
|
Merrill KC (2015). Leadership Style and Patient Safety: Implications for Nurse Managers. The Journal of Nursing Administration 45(6):319-324. |
|
|
Miles MB, Huberman AM (2003). Analyse des données qualitatives. 2nd ed. Bruxelles: De Boeck & Larcier s.a. |
|
|
Ministère de la Santé (2003). Programme National d'Assurance Qualité en Santé. Burkina Faso. |
|
|
Ministère de la Santé (2016). Guide de formation sur la stratégie 5S-Kaizen-TQM?: étape 5S. Burkina Faso. |
|
|
Mintzberg H (2004). Le management?: Voyage au centre des organisations. 2nd ed. Paris: Éditions d'Organisation. |
|
|
Moulin G (2012). La résistance au changement?: de quelle manière l'infirmier en chef peut-il y faire face.Tournai: École d'Enseignement et de Promotion Sociale de la communauté française. |
|
|
Oldland E, Mari B, Alison MH, Bernice R (2020). A Framework of Nurses' Responsibilities for Quality Healthcare: Exploration of Content Validity.Collegian 27(2):150-163. |
|
|
Parand ASD, Renz A, Vincent C (2014). The Role of Hospital Managers in Quality and Patient Safety: A Systematic Review. BMJ Open 4(9):e005055-e005055. |
|
|
Patrick A, Heather K. Spence L, Carol W, Joan F (2011). Developing and Testing a New Measure of Staff Nurse Clinical Leadership: The Clinical Leadership Survey: Leadership and Management in Mental Health Nursing.Journal of Nursing Management 19(4):449-460. |
|
|
Pearson A, Rick W, Anthea C, Craig L (2005). The JBI Model of Evidence-Based Healthcare. International Journal of Evidence-Based Healthcare 3:207-215. |
|
|
Phaneuf M (2012). Continuité et qualité des soins.In , 23. Coimbra, Portugal. |
|
|
Polit DF, Beck CT (2012). Resource Manual for Nursing Research: Generating and Assessing Evidence for Nursing Practice. 9th ed. Philadelphia: Wolters Kluwer Health/lippincott Williams and Wilkins. |
|
|
Sullivan EJ (2012). Effective Leadership and Management in Nursing. 8th ed. Boston: Pearson. |
|
|
Weiss SA, Tappen RM, Grimley K (2015). Essentials of Nursing Leadership and Management. 6th ed. Philadelphia: F. A. Davis Company. |
|
|
World Health Organization (WHO) (2006). Quality of Care: A Process for Making Strategic Choices in Health Systems. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


