Full Length Research Paper

ABSTRACT
In rural Zambia, pregnant mothers are referred from rural primary health facilities designed to provide Basic Emergency Obstetric and Newborn Care (BEmONC) to district hospitals where Comprehensive Emergency Obstetric and Newborn Care (CEmONC) can be provided when needed. Maternity waiting homes (MWH) are residential dwellings where mothers can await delivery and may offer a possible early referral source to CEmONC, ultimately serving as an intervention to improve maternal-newborn delivery outcomes. This case series study aimed to advance an understanding of maternal-newborn delivery outcomes for mothers referred from health facilities with and without MWHs to one district referral hospital. A retrospective medical record review of district-level data was performed to compare maternal-newborn delivery outcomes for cases referred from five BEmONC health facilities with and five without MWHs to a CEmONC district referral hospital. Information about MWH use was not recorded in the delivery register, and is unknown. Among all cases (n = 234) referred to a district hospital from facilities with and without MWHs, referrals were more likely to come from facilities with MWHs. Most were referred from facilities more than 12km from the district referral hospital. There were no statistically significant differences in newborn delivery outcomes for cases referred from MWH and non-MWH facilities. More cases with prolonged labor were referred from facilities associated with a MWH than without a MWH (37.3 vs. 23.9%). Access to a MWH may have brought mothers closer to a facility where prolonged labor was recognized and emergency referral was made for obstetric management.
Key words: Newborn health, maternal health, pregnancy complications, delivery outcomes, Zambia.
INTRODUCTION
In the Southern African country of Zambia, there are approximately 14,000 newborn deaths each year (38 babies each day) (WHO, 2018). The newborn mortality rate in rural areas in Zambia is 34 per 1,000 live births (UNICEF, 2017).In Zambia, the main causes of newborn deaths are birth asphyxia, prematurity, and sepsis (United Nations Inter-Agency Group for Child Mortality Estimation [UN IGME], 2018).
Maternal mortality is a major cause of death among women in Zambia where 224 maternal deaths occur per 100,000 live births(UNICEF, 2017; Zambia National Public Health Institute, 2019). In 2017, maternal associated causes were the fourth leading cause of death in Zambian women of childbearing age (Zambia National Public Health Institute, 2019). The primary causes of maternal deaths were obstetric hemorrhage and indirect causes (Zambia National Public Health Institute, 2019).At its current rate, Zambia is not on track to reach Sustainable Development Goal3 of a maternal mortality ratio of less than 70 maternal deaths per 100,000 live births by 2030 (Zambia National Public Health Institute, 2019; United Nations, 2019).
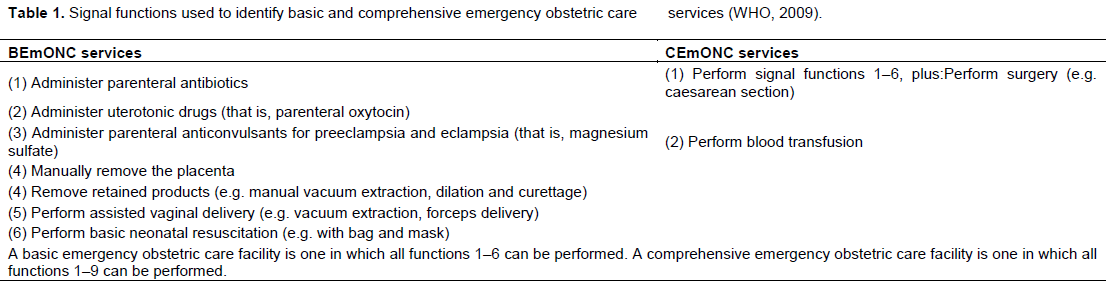
One of the biggest challenges in achieving access to skilled care in countries with large rural populations such as Zambia is connecting mothers with obstetric emergencies to necessary care (Henry et al., 2018). Universal access to Emergency Obstetric and Newborn Care (EmONC) is considered essential to reduce maternal mortality and requires that all pregnant mothers and newborns with complications have rapid access to well-functioning facilities that include a broad range of service delivery types and settings (Otolorin et al., 2015; Campbell et al., 2006). Emergency Obstetric and Newborn Care facilities are divided into those meeting tiered standards of care for providing either Basic Emergency Obstetric or Newborn Care (BEmONC) or Comprehensive Emergency Obstetric and Newborn Care (CEmONC). Signal functions for EmONC are the major interventions for averting maternal and newborn mortalities (Roy et al., 2017) and help differentiate between levels of care provided at a facility. Table 1 provides an overview of signal functions.
In Zambia, pregnant mothers are referred from rural primary health facilities, where BEmONC services are provided, to the district hospital where CEmONC can be provided when a potential complication is recognized by a skilled birth attendant. Mothers are often referred to a CEmONC facility for prolonged labor (1st or 2nd stage), obstructed labor, poor progress, and cephalo pelvic disproportion (CPD). Prolonged labor is defined as labor lasting longer than 24 h after the onset of regular, rhythmical painful contractions accompanied by cervical dilation (WHO, 2008a). Meanwhile, obstructed labor implies that, in spite of strong uterine contractions, the fetus cannot descend through the pelvis because an insurmountable barrier prevents its descent (WHO, 2008a). Cephalopelvic disproportion occurs when there is a misfit between the fetal head and the pelvis, making it difficult or impossible for the fetus to pass safely through the pelvis (WHO, 2008a). In low- and middle-income countries (LMICs), CPD is often due to stunted growth of the maternal pelvic bones from malnutrition, early childbearing, or abnormalities of the shape of the pelvis due to rickets or osteomalacia (WHO, 2008a).
The use of maternity waiting homes (MWHs) may offer an opportunity for early problem identification and referral from BEmONC to CEmONC facilities in rural Zambia, ultimately serving as an intervention to improve maternal-newborn delivery outcomes. Maternity waiting homes provide a setting where mothers can be accommodated during the final weeks of their pregnancy near a facility able to provide BEmONC (WHO, 1996). In LMICs, MWHs can help overcome distance and transportation barriers that prevent mothers from receiving timely skilled obstetric care (Lori et al., 2016). By addressing distance to a health facility and transportation barriers, MWHs could increase the use of skilled birth attendants, thereby reducing newborn morbidity and mortality in rural, low resource areas of Zambia (Lori et al., 2016).
This case series was conducted at Lundazi District Hospital, one of the CEmONC health facilities included in a collaborative research endeavor (parent study) from 2015-2018 to determine the impact of MWHs on health facility delivery among mothers living at least 10km from health facilities in rural Zambia. Using formative research, a team of researchers developed a MWH intervention model with three components: infrastructure, management, and linkage to services (Kaiser et al., 2018). The larger study evaluated the impact of MWHs by employing a controlled before-and-after, quasi-experimental design and using mixed methods to examine outcomes (Scott et al., 2018). The parent study was conducted by the Maternity Homes Alliance, a partnership between the Government of Zambia, Boston University, and Right to Care Zambia (formerly the Zambian Center for Applied Health Research and Development), Africare, and the University of Michigan, funded by Merck Sharp and Dohme for Mothers, the Bill and Melinda Gates Foundation, and The ELMA Foundation (Scott et al., 2018). The Maternity Homes Alliance hypothesized that MWHs can remove the distance barrier and increase access to facility-based delivery (Scott et al., 2018).
This study aimed to advance an understanding of maternal-newborn delivery outcomes for mothers referred from health facilities with and without MWHs to the district referral hospital. The case series study used medical record data from delivery registers located in one district referral hospital to examine a sample of all mothers with complications who were referred from ten lower-level BEmONC facilities and arrived at the higher-level CEmONC district referral hospital. Of these cases, the characteristics of those referred from facilities with and without MWHs were examined. Newborn delivery outcomes included low birth weight [LBW < 2500 grams]; condition of baby [alive or dead]; low Appearance, Pulse, Grimace, Activity, and Respiration [APGAR] score; and breastfeeding within one hour. Maternal delivery outcomes included assisted delivery [forceps, vacuum], prolonged/obstructed labor, and eclampsia. Research for the case series study was conducted through a retrospective hospital-based record review guided by the questions: (1) “Do newborns born to mothers referred from facilities with MWHs have better delivery outcomes than cases referred from non-MWH health facilities?” and (2) “Do mothers referred from facilities with MWHs have better delivery outcomes than cases referred from non-MWH health facilities?” The research hypotheses are: (1) Newborns born to mothers referred from facilities with MWHs will have better delivery outcomes than mothers referred from non-MWH health facilities; and (2) Mothers referred from facilities with MWHs will have better delivery outcomes than mothers referred from non-MWH health facilities.
MATERIALS AND METHODS
A retrospective record review of district-level data recorded by healthcare providers for the Zambian Ministry of Health was performed to compare maternal-newborn delivery outcomes for cases referred from five BEmONC health facilities with and five without MWHs to one rural Zambian CEmONC district referral hospital for delivery. Data from the delivery register (date/time of admission, demographics [name, address, age], delivery outcomes, birth outcomes) were recorded by the attending nurse or midwife on the labor ward. The delivery register, an institutionally based document that does not leave the labor ward, is a permanent record that provides information on delivery process and outcome as well as laboratory tests. Prior to beginning the study, Institutional Review Board approval was obtained from the University of Michigan (HUM00127176) and Zambian Ethics Reviews Converge IRB (2017-May-067), and the National Health Research Authority in Zambia was informed. Verbal permission for data collection was obtained from the Hospital Administrator and District Health Officer directly responsible for oversight of the facility in Zambia.
Setting and sample
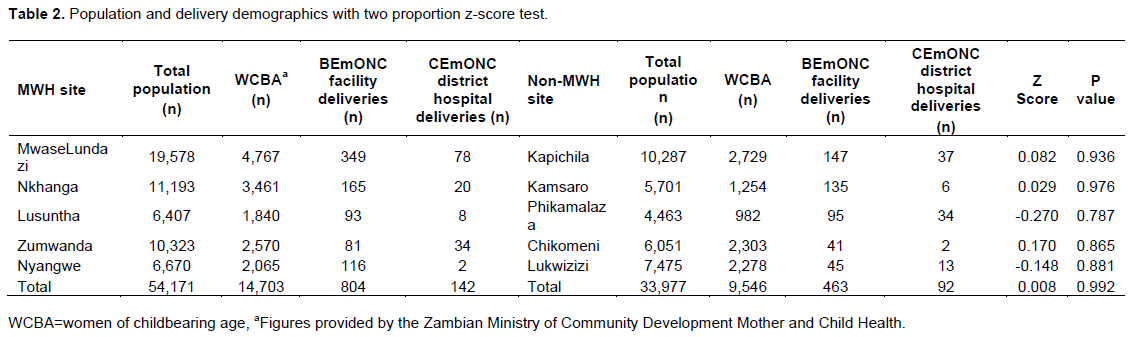
Lundazi District Hospital is a centrally located referral hospital in the Eastern Province where mothers with obstetric complications from all corners of the district deliver (Moyo, et al., 2018). The total population of Lundazi District is 323,870 (Central Statistics Office, 2015). In Zambia, the fertility rate is 4.98 births per woman (World Bank, 2019). In Eastern Province, the fertility rate is 5.8 births per woman (DHS Program, 2014). Table 2 shows the population (Central Statistics Office, 2015) and delivery characteristics of cases referred for delivery to the district hospital from the ten facilities included in the study.
Study sites were chosen based on their inclusion in the larger parent study. Researchers and implementing partners in the parent study worked with the Zambian Ministry of Health to identify five intervention sites (Scott et al., 2018). Sites were eligible for inclusion in the parent study if the BEmONC health facility was located ≤2 hours driving time to a CEmONC capable referral facility, performed a minimum of 150 deliveries per year and met at least one of two sets of conditions below (Scott et al., 2018):
Eligibility condition set 1:
i) Facility is able to provide at least five of seven BEmONC signal functions based on 2015 data.
Eligibility condition set 2:
i) Facility has at least one skilled birth attendant on staff.
ii) Facility routinely provides active management of third stage of labour.
iii). Facility has had no stock-outs of oxytocin in the last 12 months.
iv). Facility has had no stock-outs of magnesium sulfate in the last 12 months.
Five comparison sites were matched to intervention sites on annual delivery volume and distance to the referral hospital (Kaiser et al., 2018). Sites with an existing infrastructure that functioned as an MWH were not considered as an option for comparison sites (Scottet al., 2018). Mothers of childbearing age made up 27.1% of the total population.
The case series comparing maternal-newborn delivery outcomes was performed in rural Zambia at Lundazi District Hospital. The maternity ward delivery registers for five full calendar months from September 1, 2017 through January 31, 2018 were reviewed. The beginning timeframe was used due to publication of a new delivery register by the MOH. The ending date was chosen due to constraints by the primary investigator to meet scholastic program responsibilities in her home department. Inclusion criteria included all cases aged 15 years and above (n = 234) who were referred and arrived at the district hospital with a complication from the ten catchment areas. In Zambia, married, pregnant, or parent-children are considered “emancipated minors” if aged 15 years and older. From the sample, 60.7% of cases (n = 142) were referred from five rural facilities with a MWH and 39.3% of cases (n = 92) were referred from five rural non-MWH facilities. It is important to note that information about whether a case actually used a MWH was not recorded in the delivery register.
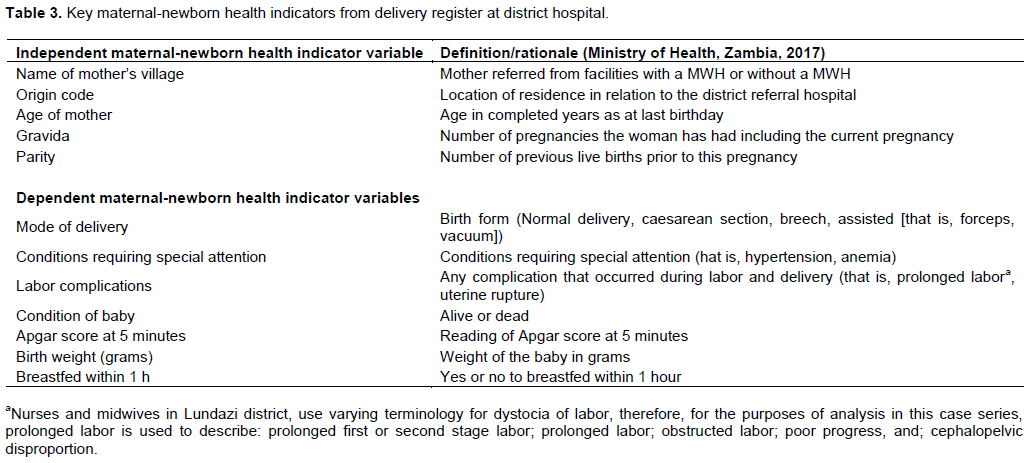
Data collection
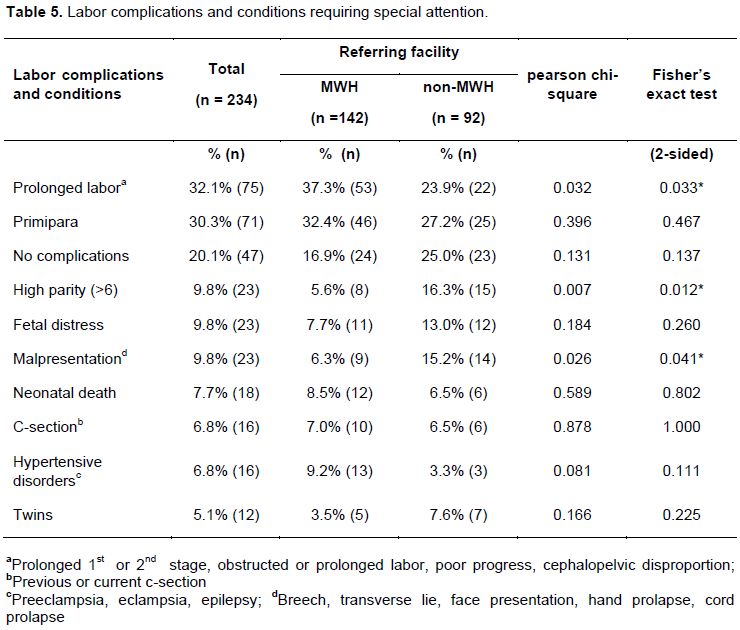
After identifying all cases referred from MWH and non-MWH facilities documented in the Zambian Ministry of Health (MOH) delivery register in the maternity ward at Lundazi District Hospital, data were extracted by two local research assistants (RA) trained by the principal investigator. Both had previous experience performing chart reviews. One RA read directly from the delivery register while the other transcribed the data. The principal investigator double-checked each variable and entered data into an Excel spreadsheet. The key maternal-newborn health indicators used in this analysis are listed in Table 3. Data for conditions requiring special attention and labor complications were sorted into four sub-categories: prolonged labor(prolonged 1st or 2nd stage, obstructed or prolonged labor, poor progress, CPD), caesarian section (C-section) (previous or current C-section), hypertensive disorders (preeclampsia, eclampsia, epilepsy), and malpresentation (breech, transverse lie, face presentation, hand prolapse, cord prolapse).
Statistical analysis
Descriptive statistics were computed for all maternal-newborn variables by performing crosstabulation. Predictor variables for the maternal-newborn dyad included referral from a referral facility with or without a MWH, distance of facility from district referral hospital, age of mother, gravida, and parity. Newborn outcome variables included condition of baby, Apgar score, birth weight, and breastfeeding within one hour. For Apgar score, per the local definition, a dummy variable was created by coding, as the reference group, all cases with an Apgar score less than or equal to 6 as low Apgar score. An Apgar score at 5 min of 7 to 10 is considered normal (Costa et al., 2016; Pediatrics et al., 2006), while a 5-min Apgar score of < 7 generally indicates a risk of poor birth outcome (Cnattingius et al., 2017; Tiemeier and McCormick, 2019). For low birth weight, a dummy variable was created by coding all cases with a birth weight less than 2500 grams as LBW, in accordance with the WHO (2014) definition. Maternal outcome variables included mode of delivery, labor complications, and conditions requiring special attention.
A Pearson chi-square test of independence was performed for relevant variables to examine whether there was a difference in referral from a facility with a MWH compared to those referred from a facility without a MWH. In addition, certain numerical variables, such as age, gravid (number of pregnancies), parity (number of live births), and village community, were categorized to determine their associations when comparing referrals from a facility with a MWH to referrals from a facility without a MWH. In cases where the sample size was too small to use a chi-squared test, a Fisher’s exact test was performed. Frequencies were established to examine documented labor complications and conditions requiring special attention. Pairwise referral-facility comparisons were conducted as were grouped (MWH vs. non-MWH) comparisons.
The hypotheses were tested with independent and pairwise referral-facility comparison t-tests. Given that multiple significance tests were performed, Bonferroni corrections were performed. Logistic regression with a dichotomized MWH variable (non-MWH = 0, MWH = 1) was performed. Adjusted logistic regression was performed controlling for categorized variables such as age, gravida (number of pregnancies), parity (number of live births), and village referral facility that could interact with the maternal-newborn delivery outcomes. P-values < 0.05 were considered statistically significant. Statistical analysis was performed using SPSS version 25.
RESULTS
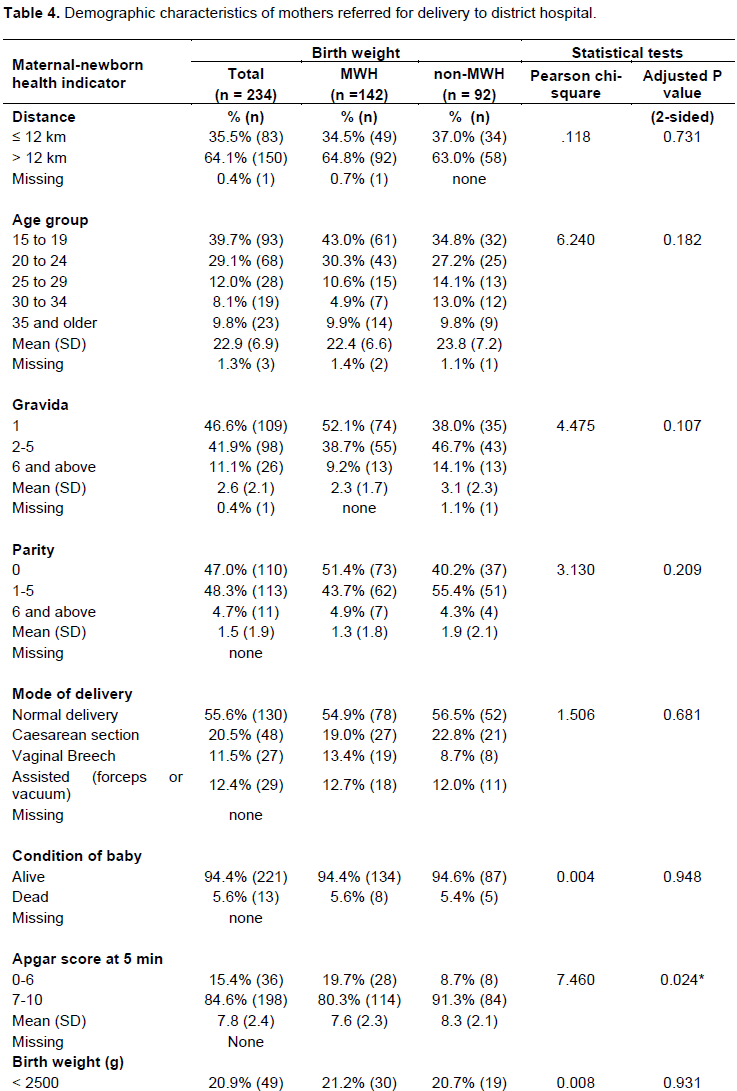
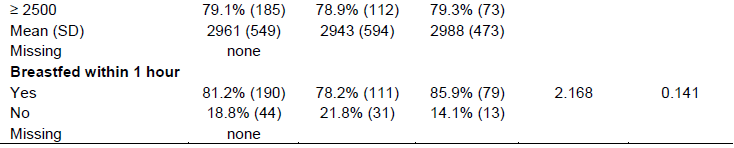
Among all cases from facilities with and without MWHs, referrals were more likely to come from facilities with MWHs (n=142 (60.7%) MWH vs. n=92 (39.3%) non-MWH, P < 0.001). The majority of cases (64.1%) were referred from facilities more than 12km from the district referral hospital. A two population proportions z-score test, performed to compare the populations of paired MWH and non-MWH referral facilities, showed they were similar and well matched (Table 2). Twenty-one percent (n=49) of newborns weighed less than 2500 g. The mean age of mothers was 22.9 years with mean gravida of 2.6 and parity of 1.5. Most cases had a normal spontaneous vaginal delivery (55.6%) while 20.5% had a C-section with the remainder having an assisted (12.4%) or vaginal breech delivery (11.5%) (Table 4). Select demographic and delivery outcome data are shown in Table 4. Apart from low Apgar score, there were no other statistically significant differences in distance, age, gravida, or parity between mothers referred from MWH and non-MWH facilities.
Newborn delivery outcomes
After record review, the hypothesis “Newborns born to mothers referred from facilities with MWHs will have better delivery outcomes (LBW, condition of baby, low Apgar score, breastfeeding within one hour) than mothers referred from non-MWH health facilities” was not supported. Eighteen newborn deaths were reported (7.7%). Fetal distress was noted for 23 cases (9.8%). Cases with LBW were no more likely to be referred from MWH compared to non-MWH facilities (X2 = 0.008, P = 0.931) (Table 4). Regarding condition of baby (alive or dead), there was no statistically significant difference for cases referred from MWH compared to non-MWH (X2 =0.004, P = 0.948). Cases from MWH and non-MWH had similar rates of breastfeeding within one hour of birth that were not statistically different (X2 = 2.168, P = 0.141) (Table 4).
The majority (84.6%) of all newborns in both groups had Apgar scores of 7 or above. When compared to cases referred from facilities without a MWH, those referred from facilities with a MWH were more likely to have newborns with an Apgar score from 0-6 (X2 = 7.460, P = 0.024) (Table 4). However, a regression model demonstrated no significant difference among groups referred from MWH and non-MWH facilities for Apgar score when controlling for variables that could interact with the maternal-newborn delivery outcomes, including subcategories within distance, age, gravid (number of pregnancies), and parity (number of live births).
Maternal delivery outcomes
No maternal deaths were recorded in the case series. Seventy-five cases with either labor complications or those requiring special attention had prolonged labor (Prolonged 1st or 2nd stage, obstructed labor, poor progress, CPD) (32.1%), while 71 were primiparas (first birth) (30.3%). The second hypothesis was “Cases referred from facilities with MWHs will have better delivery outcomes (assisted delivery, prolonged/obstructed labor, eclampsia) than cases referred from non-MWH health facilities; this was only partially supported. Cases referred from facilities with MWHs had similar modes of delivery compared to cases referred from non-MWH health facilities (X2 = 1.506, P= 0.681) (Table 5). Frequency distributions for labor complications and conditions requiring special attention are presented in Table 5. Cases with prolonged labor were more often referred from facilities associated with MWHs (X2 = 0.032, P = 0.033) (Table 5). Among all mothers presenting with complications at one district hospital, cases with high parity (6 or more live births) were more likely to come from non-MWH facilities than facilities with MWHs (X2 =.007, P = 0.012). Similarly, cases experiencing malpresentation as a labor complication were more likely to come from a non-MWH facility than a facility with a MWH (X2 =0.026, P = 0.041) (Table 5). Pairwise referral facility and grouped (five MWH vs. five non-MWH) comparisons did not show any significant differences among groups in the sample.
DISCUSSION
Among all cases referred to one district hospital from facilities with and without MWHs, we found that referrals were more likely to come from facilities with MWHs (60.9% vs. 39.3%, P <0.001). More cases of mothers with prolonged labor were referred from facilities associated with a MWH than without a MWH (37.3% [n = 53] vs. 23.9% [n = 22], P = 0.033). The discovery that 21% of newborns were classified as LBW is discussed in a separate commentary. Because information about MWH use per se was not recorded in the delivery register, and is therefore unknown, this study could not directly test differences in maternal-newborn outcomes among cases that used a MWH and those that did not. However, findings demonstrate the potential positive influence of referral from facilities associated with MWHs, especially for those with prolonged labor as a complication.
In this case series, access to a MWH may have brought mothers closer to a BEmONC facility where prolonged labor was recognized and emergency referral to CEmONC at one district hospital was made for obstetric management. Untreated prolonged or obstructed labor is dangerous and a major cause of both maternal and newborn morbidity and mortality (Dolea and AbouZahr, 2003). The situation is even worse for poor, remote, and rural populations where access to health services may be limited due to ongoing gaps in the Zambia health system (Ngoma-Hazemba et al., 2019).Emergency referral is critical to improving maternal and newborn health outcomes for time-sensitive conditions, such as prolonged labor, that underlie many unpredictable problems during pregnancy, delivery, and the postnatal period (Conlon et al., 2019). For the newborn, neglected obstructed labor may cause asphyxia leading to stillbirth, brain damage, or neonatal death (Dolea and AbouZahr, 2003). Maternal complications include intrauterine infections following prolonged rupture of membranes, trauma to the bladder and/or rectum due to pressure from the fetal head or damage during delivery, and ruptured uterus with consequent hemorrhage, shock, or even death (Dolea and AbouZahr, 2003).
To attain Sustainable Development Goal targets, newborns and their mothers need access to quality health care. The finding of few significant differences in maternal-newborn delivery outcomes, and no cases of maternal deaths, for cases referred from MWH and non-MWH facilities could be explained by overall improvements in maternal-newborn health made in Lundazi District over the past five years. The presence of the Saving Mothers, Giving Life (SMGL) program for two years prior to starting the MWH intervention study may confound the results of this case series. In Zambia, SMGL put in place key interventions to improve maternal and newborn health across 16 districts (SMGL, 2018). Working with the Zambian government from 2013-2018, the initiative set out to make high-quality, safe childbirth services available and accessible to mothers and their newborns, focusing on the critical period of labor, delivery, and the first 48 hours postpartum (SMGL, 2018).
In conjunction with stimulus from the SMGL initiative, several explanations are plausible for why the hypotheses were not supported. It is possible the insignificant differences in maternal-newborn delivery outcomes in the sample could reflect that women were not necessarily using a MWH. Another explanation could be that quality care was provided at rural BEmONC facilities in the district. It is encouraging that nurses and midwives may be identifying maternal-newborn health problems early and referring appropriately. Furthermore, despite potential geographic barriers, such as distance and transportation difficulties, our findings suggest that a good system is in place in the district for referring cases to CEmONC when complications arise. Another explanation for insignificant differences in the sample could be that MWHs had not been open for a sufficiently long period of time to influence maternal-newborn outcomes. MWHs were opened from between one month to one year prior to the case series data collection timeframe. Finally, it was difficult to interpret the findings given the ongoing improvements in maternal and newborn delivery outcomes from the SMGL interventions.
Given that this case series is the first of its kind to explore the delivery outcomes of mothers and their newborns referred from health facilities with and without MWHs, no direct comparisons can be made to other studies. However, findings related to labor complications
from mothers in this case series can be assessed in light of findings from other studies investigating maternal- newborn health outcomes. In a retrospective observational study involving MWHs in rural Ethiopia, Braat et al. (2018) examined the impact of a MWH by comparing pregnancy outcomes among MWH users and non-users at hospitals with and without MWHs. They found high-risk mothers who used a MWH had less favorable socio-demographic characteristics, but better birth outcomes than both mothers who gave birth at the same hospital but did not use the MWH and mothers who gave birth at a hospital without a MWH (Braat et al., 2018). The mothers in our study never used a MWH, or at least we do not know whether they did or not. In the cohort study in Ethiopia, MWHs contributed to reducing maternal deaths, stillbirths, and uterine ruptures by providing an important service to mothers living in rural areas who have difficulty accessing facilities providing EmONC MWH (Braat et al., 2018). While in our case series the socio-demographic characteristics were similar across all cases, referral from facilities associated with a MWH likely allowed for early and rapid recognition of prolonged labor at a BEmONC facility. Subsequent timely referral to CEmONC at the district hospital for management of prolonged labor in this case series lends support to the effectiveness of facilities associated with MWHs as a potentially lifesaving intervention to improve maternal-newborn delivery outcomes.
Healthcare organization factors could influence maternal-newborn dyad delivery outcomes. Since no clear guidelines exist, wide variation in classification of labor complications, conditions requiring special attention, and subjective remarks regarding stability of maternal-newborn dyad by nurses and midwives at the district referral hospital may occur. For example, because of potential differences in how nurses and midwives are educated and trained to recognize maternal and newborn complications and the willingness to report more than one complication, midwives may register Apgar scores, fetal distress, or prolonged labor differently. These factors could influence reporting of maternal-newborn health indicators.
In this study, maternal-newborn delivery outcome variables could have been affected by factors such as the implementation of the SMGL program in Lundazi District. In Zambia, the proportion of mothers with childbirth complications delivering in EmONC facilities rose by 23% after one year of SMGL (Serbanescu et al., 2017). In the past three years, SMGL communities saw the maternal mortality ratio decline by 55% and the stillborn and neonatal deaths decline by 44% in target facilities in Zambia, with an accompanying increase of 38% in mothers giving birth in a facility in the target districts (SMGL, 2018). Furthermore, as part of the SMGL program, community health workers were active in all study sites and likely influenced the health-seeking behavior of pregnant mothers.
LIMITATIONS
As a case series using data from the delivery register at one district referral hospital in rural Zambia, the study has several limitations. Results may not be generalizable to other districts in Zambia, nor to the broader population. The biggest limitation is that we do not know if women actually stayed at a MWH. And thus, we can only assume the influence. The study was also limited by the variables in the delivery registers; moreover, the data were retrospective and any assumptions about maternal-newborn outcomes are inferred. The data collected in the delivery register represents only a snapshot of the time around birth, and are not updated by staff to reflect complications that occurred after delivery. It was not possible to explore other aspects of antenatal care or socio-demographic information that could be associated with maternal-newborn delivery outcomes such as intrauterine infections, maternal smoking or alcohol use, poor fetal growth, mother’s weight, etc. Exclusion of this information could bias the observed results. Furthermore, only data for those referred to the one district hospital from BEmONC study sites were available. We have no data from referrals from study facilities to other hospitals.
Regarding newborn delivery outcomes, while there were slight statistically significant differences in Apgar score among MWH and non-MWH users, they were not present when controlling for distance, age, gravida, and parity. Moreover, there is likely significant inter-observer variability in the 5 minute Apgar score documented in the maternity delivery register. It is important to recognize the limitations of the Apgar score, which includes subjective components, as an expression of the newborn’s physiologic condition at one point in time (Committee on Obstetric Practice American Academy of Pediatricsâ€Committee on Fetus and Newborn, 2015). The Apgar score provides a convenient method for reporting the status of the newborn infant immediately after birth, and quantifies clinical signs of neonatal distress, such as cyanosis or pallor, bradycardia, depressed reflex response to stimulation, hypotonia, and apnea or gasping respirations (Watterberg et al., 2015); however, researchers have found large variations in the distribution of Apgar scores, likely due to national scoring practices, making the Apgar score an unsuitable indicator for benchmarking newborn health across countries (Siddiqui et al., 2017).
No clear guidelines or protocols were in place at the hospital for diagnosing or documenting most maternal-newborn delivery outcomes. The quality of documentation in the delivery register likely varied by the person entering the data. Students training in the district hospital were often the ones entering information into the delivery register. While there were few cases with incomplete documentation, under-reporting of delivery outcomes in the delivery register is a potential limitation. Lack of electricity, understaffing, operating at over-capacity, and competing demands for the attention of nurses and midwives make data entry difficult or under-prioritized and, therefore, may have caused gaps in the register. Every provider was responsible for identifying complications, thus creating potential for not recognizing or recording complications or conditions requiring special attention. Finally, because data about actual use of MWHs by case and referrals that occurred to other CEmONC facilities were unavailable, no inferences about causality or correlation between maternal-newborn delivery outcomes and a woman’s use of MWH could be made.
CONCLUSION
By examining maternal-newborn delivery outcomes for cases referred from five facilities with MWHs and five without MWHs to one district hospital, this study found that, among all referrals across the ten facilities, more came from facilities with a MWH than from those without MWHs. Although there was no significant difference in maternal or newborn outcomes, and lack of pertinent data precluded an assessment of MWH utilization, the use of MWHs likely allowed for early access and rapid recognition of prolonged labor at a BEmONC facility, offering a probable referral source to CEmONC in rural Zambia. Early recognition of prolonged labor at a BEmONC facility with a MWH may have led to crucial referrals to the CEmONC facility for management.
This study is the first case series that we are aware of to focus on the impact of referrals from facilities with MWHs on maternal-newborn delivery outcomes in a low-resource setting. It is innovative, timely, and important because it provides new knowledge on the association of referral from facilities with MWHs and maternal-newborn delivery outcomes. Among all mothers referred to a district hospital from facilities with and without MWHs, we found that referrals were more likely to come from facilities with MWHs. This finding is significant as we enter the post-2015 era of sustainable development with a goal to reduce the inequities of preventable death by reaching all mothers and newborns. We recommend improving access for mothers to a MWH close to a facility where pregnancy complications can be recognized and emergency referral to CEmONC made for obstetric management if necessary. More research is needed to compare the long-term impact of MWHs on newborn delivery outcomes and health in communities. Additional investigation of maternal-newborn outcomes comparing documented MWH use and referral to CEmONC facilities in urban settings is justified to understand the potential wide-ranging impact of MWH use.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors appreciate the sources of funding for the current study: The University of Michigan International Institute, African Studies Center, Department of Afro-American and African Studies and the South African Initiatives Office, University of Michigan School of Nursing New Research Investigator Award, University of Michigan School of Nursing Global Outreach Scholarship, and the Michigan Chapter of the National Association of Pediatric Nurse Practitioners. The parent study program was developed and is being implemented in collaboration with Merck for Mothers, Merck’s 10-year, $500 million initiative to help create a world where no woman dies giving life. The development of the parent study article was additionally supported in part by the Bill and Melinda Gates Foundation (OPP1130334) https://www.gatesfoundation.org/How-We-Work/Quick-Links/Grants-Database/Grants/2015/07/OPP1130334 and The ELMA Foundation (ELMA-15-F0010) http://www.elmaphilanthropies.org/the-elma-foundation/.
REFERENCES
|
Braat F, Vermeiden T, Getnet G, Schiffer R, van den Akker T,Stekelenburg J (2018). Comparison of pregnancy outcomes between maternity waiting home users and non-users at hospitals with and without a maternity waiting home: retrospective cohort study. International Health 10(1):47-53. |
|
|
Campbell OM, Graham WJ and Lancet Maternal Survival Series steering group (2006). Strategies for reducing maternal mortality: getting on with what works. The Lancet 368(9543):1284-1299. |
|
|
Central Statistics Office (2015). Report on Characteristics of Households and Housing. |
|
|
Cnattingius S, Norman M, Granath F, Petersson G, Stephansson OandFrisell T (2017). Apgar score components at 5 minutes: risks and prediction of neonatal mortality. Paediatric and Perinatal Epidemiology 31(4):328-337. |
|
|
Committee on Obstetric Practice American Academy of Pediatricsâ€Committee on Fetus and Newborn (2015). Committee opinion no. 644: the Apgar score. Obstetrics and Gynecology126:e52-e55. |
|
|
Conlon CM, SerbanescuF, Marum L, Healey J, LaBrecque J, Hobson R, Spigel L(2019). Saving Mothers, Giving Life: it takes a system to save a mother. Global Health: Science and Practice 7(S1):S6-S26. |
|
|
Costa TL, Mota A, Duarte S, Araujo M, Ramos P (2016). Predictive Factors of Apgar Scores below 7 in Newborns: Can We Change the Route of Current Events. Journal of Anesthesia and Clinical Research 7(672):2. |
|
|
DHS Program (2014). Zambia: standard demographic and health survey 2013-2014. |
|
|
Dolea C, AbouZahr C (2003).Global burden of obstructed labour in the year 2000. World Health Organization, pp. 1-17. |
|
|
Henry EG, Thea DM, Hamer DH, DeJong W, Musokotwane K, Chibwe K, Semrau K (2018). The impact of a multi-level maternal health programme on facility delivery and capacity for emergency obstetric care in Zambia. Global Public Health 13(10):1481-1494. |
|
|
Lori JR, Munro-Kramer ML, Mdluli EA, Musonda GK, Boyd CJ (2016).Developing a community driven sustainable model of maternity waiting homes for rural Zambia.Midwifery 41:89-95. |
|
|
Ministry of Health, Zambia (2017).Human resources for Health Planning & Development Strategy Framework. |
|
|
Moyo N, Makasa M, Chola M, Musonda P (2018). Access factors linked to maternal deaths in Lundazi district, Eastern Province of Zambia: a case control study analysing maternal death reviews. BMC Pregnancy and Childbirth 18(1):101. |
|
|
Ngoma-HazembaA, Hamomba L, Silumbwe A, Munakampe MN, Soud F (2019).Community Perspectives of a 3-Delays Model Intervention: A Qualitative Evaluation of Saving Mothers, Giving Life in Zambia. Global Health: Science and Practice 7(Supplement 1):S139-S150. |
|
|
Otolorin E, Gomez P, Currie S, Thapa K, Dao B (2015). Essential basic and emergency obstetric and newborn care: from education and training to service delivery and quality of care. International Journal of Gynecology and Obstetrics 130(S2). |
|
|
Pediatrics TAA, Newborn C, GynecologistsA (2006).The Apgar score.Pediatrics 117:1444-1447. |
|
|
Roy L, Biswas TKandChowdhury ME (2017). Emergency obstetric and newborn care signal functions in public and private facilities in Bangladesh. PloS One 12(11):e0187238. |
|
|
SMGL (2018).Saving Mothers Giving Life. |
|
|
Scott NA, Kaiser JL, VianT, Bonawitz R, Fong RM, Ngoma T... and Rockers PC (2018). Impact of maternity waiting homes on facility delivery among remote households in Zambia: protocol for a quasi experimental, mixed-methods study. BMJ Open 8(8):e022224. |
|
|
Serbanescu F, Goldberg HI, Danel I, Wuhib T, Marum L, Obiero W ... and Conlon CM (2017). Rapid reduction of maternal mortality in Uganda and Zambia through theSaving Mothers, Giving Life initiative: results of year 1 evaluation. BMC Pregnancy and Childbirth 17(1):42. |
|
|
Siddiqui A, Cuttini M, Wood R, Velebil P, Delnord M, Zile I ... and Zeitlin J (2017). Can the Apgar Score be Used for International Comparisons of Newborn Health? Paediatric and Perinatal Epidemiology 31(4):338-345. |
|
|
Tiemeier H, McCormick MC (2019).The Apgar paradox. European Journal of Epidemiology 34(2):103-104. |
|
|
UNICEF (2017).UNICEF Zambia maternal, newborn, and child health. |
|
|
UN IGME (2018). Levels and trends in child mortality. |
|
|
United Nations (2019). Sustainable Development Goal 3: Ensure healthy lives and promote well- being for all at all ages. |
|
|
WHO (1996).Maternity waiting homes: a review of experiences. World Health Organization. |
|
|
WHO (2008a).Managing prolonged and obstructed labour. |
|
|
WHO (2009).Monitoring emergency obstetric care: a handbook. |
|
|
WHO (2014). Global Nutrition Targets 2025: Low birth weight policy brief. |
|
|
WHO (2018). Global Health Observatory: Zambia statistics summary (2002 - present). |
|
|
Watterberg KL, Aucott S, Benitz WE, Cummings JJ,Eichenwald EC, Goldsmith J, Ecker JL (2015).The Apgar score. Pediatrics 136(4):819-822. |
|
|
World Bank (2019).Fertility rate, total (births per woman). |
|
|
Zambia National Public Health Institute (2019). Maternal mortality trends and correlates in Zambia. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


