Full Length Research Paper

ABSTRACT
To detect Postpartum depression (PPD) among mothers in early, easy, and accurate way is required. In this study, we aimed to examine whether biomarkers taken during the perinatal period can predict a risk of PPD, in addition to subjective scale scores. A longitudinal survey of 24 mothers was conducted at 6 and 9 months of gestation (T1&T2) and 1 month postpartum (T3). Psychological state was measured by EPDS, GHQ, and CES-D. Sleep quality, which has a profound influence on postpartum psychological state, was measured by PSQI. Values of 10 biomarkers was measured: blood cortisol, adrenaline, noradrenaline, dopamine, IgA, urinary free cortisol, adrenaline, noradrenaline, dopamine, and breast milk IgA. Correlation was analyzed between psychological scale scores and biomarker values at each time point in the survey. The result showed moderately significant correlations between EPDS scores at T3 and urinary dopamine at T3 (r=0.53, p=0.024), and between GHQ scores at T3 and breast milk IgA at T3 (r=-0.61, p=0.020). Some moderately significant correlations between biomarkers in different time points were found, which were seen between blood adrenaline at T2 and urinary adrenaline at T3 (r=0.52, p=0.034), and between urinary cortisol at T2 and urinary noradrenaline at T3 (r=0.55, p=0.023). These findings demonstrated that autonomic nervous system biomarkers and IgA in breast milk reflects mothers’ psychological state, which could be a tool to predict PPD. Furthermore, it was suggested that biomarkers at 9 months of gestation could detect PPD indirectly, by predicting the value of biomarkers at 1 month postpartum.
Key words: Psychological status, stress, biomarkers, postpartum depression.
INTRODUCTION
Postpartum depression among mothers is a serious issue in Japan. Tokumitsu et al. (2020) revealed that 10% of Japanese mothers develop postpartum depression within the first year after childbirth. In addition, maternal postpartum depression has been associated with maternal suicide (Quevedo et al., 2021), which is the leading cause of Japan’s maternal perinatal death (Takeda et al., 2017). Difficulties in mother-infant interactions due to postpartum depression can affect the child’s psychosocial development (Oyetunji and Chandra, 2020). Fathers are more likely to be depressed in households in which mothers are depressed (Takehara et al., 2020). Thus, early detection and treatment of postpartum depression is crucial, as it can not only affect the mothers but also family members. In Japan, postpartum depression screening is recommended for all postpartum mothers during the one-month postpartum checkup (Perinatal Mental Health Consensus Guide, 2017) and is conducted nationwide. The Japanese version of the Edinburgh Postpartum Depression Questionnaire (EPDS), developed by Cox et al. (1992) and translated by Okano et al. (1996), is widely used for screening. Meanwhile, screening using self-report questionnaires may not provide appropriate responses depending on the circumstances of the mothers visiting the clinic (e.g., lack of time and presence of an infant). Additionally, depressive symptoms in Japanese mothers tend to be somatoform (Bashiri and Spielvogel, 1999), and screening for emotional symptoms, such as depressed mood and anxiety, which are assessed in the EPDS, may not be sufficient to accurately screen mothers in need of support. Therefore, a combination use of subjective indicators and objective indicators, such as self-reporting scale and biomarkers, and identifying persons in need of support in a dual structure can enable an effective access to professional support. An objective indicator is the assessment of stress levels using biomarkers. Biomarkers can include various substances from the human body and can be collected from blood, hair, saliva, urine, breast milk, etc. Studies using hair (Mlili et al., 2022; Bowers et al., 2018) and saliva (Cevik and Alan, 2021; Vlenterie et al., 2021) to assess stress levels and mental health in perinatal women have been conducted. In this study, we focused on the use of biomarkers from blood and urine. In Japan, blood and urine tests are required throughout pregnancy health checkups, and all mothers are also subjected to urinalysis at postpartum health checkups, which has the advantage of requiring no additional invasive procedure on the mother. The assessment of stress levels using urinary biomarkers has been reported in the field of occupational health and has been performed by nursing care workers (Toshima, 2018) and night shift workers (Briguglio et al., 2021). Therefore, the applicability of this method to perinatal women must be examined. If biomarkers are useful for assessing mothers' stress levels, they can be used in conjunction with traditional questionnaires to improve screening accuracy. They can also be used to assess the psychological state of mothers who are unable to respond appropriately to questionnaires.
Additionally, mothers experiencing postpartum depression should undergo a screening method that can predict postpartum mental health on the basis of maternal status during pregnancy, given the suggested association with depressive symptoms during pregnancy (Iliadis et al., 2015; Koutra et al., 2014). Once the link between biomarkers in samples collected during pregnancy and postpartum mental health is clarified, the risk of postpartum depression during pregnancy using these methods can be assessed easily and accurately, thereby facilitating prevention and early intervention for mothers’ postpartum depression.
Thus, this study aims to examine whether the psychological status (possibility of postpartum depression) in the postpartum stage can be predicted from the psychological state during early pregnancy and to clarify from the results of the examination of the correlation between a questionnaire and biomarker measurement values whether the use of biomarkers as an objective measurement of psychological state is useful.
METHODOLOGY
This was a longitudinal study from gestational to postpartum period using a self-reported, anonymized questionnaire.
Participants and recruitment
Pregnant women in their sixth month of pregnancy who had antenatal checkups at an ObGyn outpatient clinic in a general hospital in Japan were asked to participate in a study. A total of 24 pregnant women agreed to participate in the study and consented to the survey. However, five of them transferred to another hospital, and data at one month postpartum could not be collected.
Survey locations
The study was conducted at three time points: at 6 months of gestation (T1), 9 months of gestation (T2), and 1 month postpartum (T3). The survey was conducted in the hospital at the time of antenatal health checkups at T1 and T2, as well as the postpartum checkup at T3. The researchers arrived at the hospital on the day of each participant’s checkup, having confirmed the date in advance. Participants were asked to answer a paper questionnaire, which included self-report scales at each time point.
Measurements
Sociodemographic characteristics
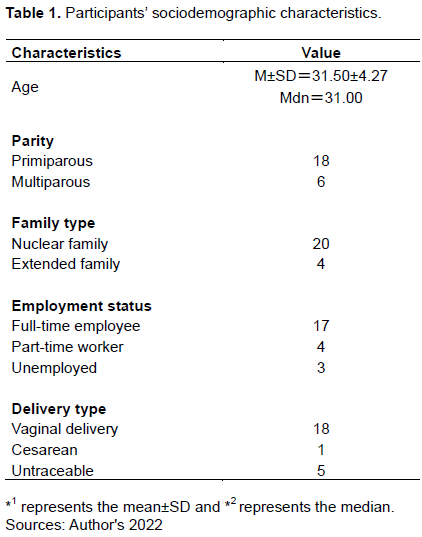
Participant mothers' age, parity, family type (nuclear/extended family), employment status (full-time employee, part-time worker, unemployed), medical history, pregnancy complications, delivery type (vaginal/cesarean), prematurity, and birth weight were obtained. Characteristics were obtained at T1 through face-to-face interviews with the researcher, except for delivery information, which was obtained at T3.
Biomarkers
Nine biomarkers were measured using residues from blood and urinalysis specimens performed during antenatal checkups at T1 and T2. The nine test items were blood cortisol, adrenaline, noradrenaline, dopamine, immunoglobulin A (IgA), urine free cortisol, adrenaline, noradrenaline, and dopamine. At one month postpartum (T3), four parameters were measured using urine samples from the postpartum health checkup: free cortisol, adrenaline, noradrenaline, and dopamine. Furthermore, IgA in breast milk, which was submitted as a research sample with the participant's cooperation, was also measured.
Psychological state
The following psychological scales (1) to (3) were used to measure the psychological state of the participants at the respective points in the pregnancy and postpartum periods.
Edinburg postpartum depression scale (EPDS): The EPDS is a widely used scale in the screening of mothers for postpartum depression during the postpartum period, originally developed by Cox et al. (1992). The Japanese version was verified for reliability and validity by Okano et al. (1996). It consists of a 10-item, 4-case method (0 to 3) that includes reversed items, and the total score ranges from 0 to 30. Postnatal depression (screening positive) is suspected when the score is ≥9. Cronbach’s alpha of the Japanese version was 0.78, sensitivity was 75%, and specificity was 93%.
The general health questionnaire (GHQ): Developed by Goldberg (1979), GHQ is used to understand, evaluate, and detect neurological symptoms. The original version has 60 items, and short-versions with 30, 28, and 12 items have been developed, with verified reliability and validity. A 30-item version of the GHQ (GHQ-30) was used in the current study, and the Japanese version was translated by Nakagawa and Daibou (1985). A score of 0 to 1 was assigned for each item; the total score ranges from 0 to 30, with a score of ≥7 being a positive screening. A cutoff score of ≥7 indicated proper sensitivity (92%) and specificity (85%).
The center For epidemiologic studies depression scale (CES-D): The CES-D was developed to discover depression in the general public for people aged ≥15 years. Originally developed by Radloff (1977), the Japanese version of the CES-D was translated by Shima et al. (1985) with sufficient reliability and validity. It consists of 20 items, 4-case (0 to 3) methods, and total score ranges 0-60. A cut-off score of ≥16 is considered a positive screening.
Sleep quality: Pittsburgh sleep quality index (PSQI) was used to measure the sleep quality at each time point. PSQI was developed by Buysse et al. (1989), which measures sleep habits and quality over the past month. The reliability and validity of the Japanese version was verified by Doi et al. (2000). Respondents were asked to indicate the time they went to bed, time they fell asleep, time they woke up, and their sleep duration, and to select the applicable option using a 4-point scale ranging from 0 to 3. The degree of sleep disturbance is scored by adding the scores of the seven factors obtained from the responses to all of the 18 items. The total score was used for the analysis, ranging from 0 to 21. A cut-off score for the Japanese version is set at ≥6, which is the same as the original version. Cronbach’s alpha was 0.77.
Data analysis
Descriptive statistics were conducted on the basic attributes and scores of each scale. The correlation between psychological scale scores and biomarker values at each time point of the survey was examined using Pearson's correlation coefficient. The relationship between the values of each biomarker during T1&T2 and the psychological scale scores at T3 was also examined using Pearson's correlation coefficient. SPSS 27.0 for Windows was used for the statistical analysis, with a 5% probability of significance and a two-tailed test.
Ethical considerations
This study was conducted with the approval of the Medical Ethics Committee of the University of Tsukuba, Faculty of Medicine and Health Sciences (Approval No.: 1820).
RESULTS
Background factors
The mean age (±SD) of the participants was 31.50 (±4.27) years, 18 were primiparous, and six were multiparous. Twenty of the families consisted of nuclear families and four were in extended families, either living with their biological parents or parents-in-law. The most common occupation was clerical, accounting for six of the respondents, followed by nurses. No pregnancy complications were observed in all subjects and one subject had a history of depression. Eighteen women had a vaginal delivery, one had a cesarean delivery, and five were untraceable (all primiparous), including transfers to other hospitals. Of the 19 patients who could be followed up to T3, 18 had full-term delivery except one at 36 weeks gestation, and all 19 had normal birth weights of 2500 g or more (Table 1).
Scores of each scale
EPDS
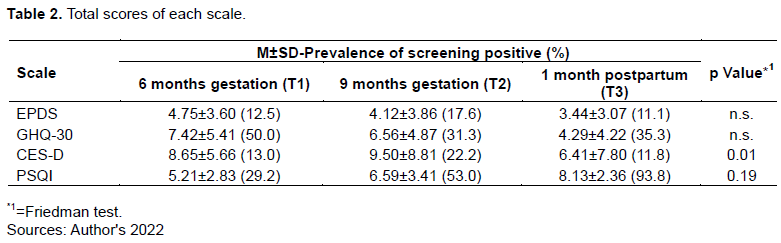
At each time point, excluding missing data, 12.5% of the participants (3 of 24) were suspected to have depression (scores ≥9) at T1, 17.6% (3 of 17) at T2, and 11.1% (2 of 18) at T3. T1 had the highest mean score (±SD) among all time points, which was 4.75(±3.60).
The Friedman test results did not show significant differences in scores between the three time points (Table 2).
GHQ-30
The percentage of participants with a score ≥7 points at each time point was 12/24=50.0% at T1, 5/16=31.3% at T2, and 6/17=35.3% at T3. Friedman test results showed no significant differences in scores between the three time points (Table 2).
CES-D
The percentage of participants with a score of ≥16 at each time point was 3/23=13.0% at T1, 4/18=22.2% at T2, and 2/17=11.8% at T3. The mean score (±SD) at T2 was 9.50±8.81 which was the highest of the three. The Friedman test revealed a significant difference (p=0.01). Additionally, the Bonferroni method was used to adjust the probability of significance for significant differences between each score, and a significant difference was found between T1 and T3 (adjusted p=0.02) (Table 2).
PSQI
The percentage of participants who scored ≥6 points at each time point was 7/24=29.2% at T1, 9/17 (53.0%) at T2, and 15/16 (93.8%) at T3. Regarding significant differences between each score, a significant difference was observed between the scores at T1 and T3 by the Bonfferoni method (adjusted p=0.02) (Table 2).
Association between biomarkers and psychological scales
Analysis of correlations between each scale score at T3 and biomarkers at each of the three time points showed significant correlations in the following items (Table 3).
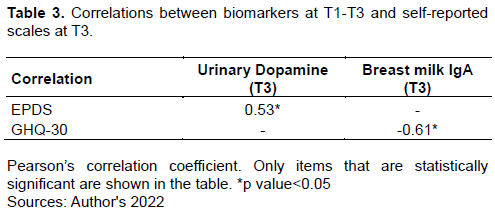
First, a moderately significant correlation was shown for EPDS scores at T3 with urinary dopamine at T3 (r=0.53, p=0.02). None of the biomarkers in the gestational period correlated with EPDS scores at T3. Second, a moderately significant negative correlation with breast milk IgA was also shown at T3 for the GHQ-30 score (r=-0.61, p=0.02). No correlation was found for any of the items in the gestational period. No statistically significant correlation with any biomarker at any of the three time points was detected for the CES-D and PSQI scores at T3.
Association between biomarker values at T1 and T2 and biomarker values at T3
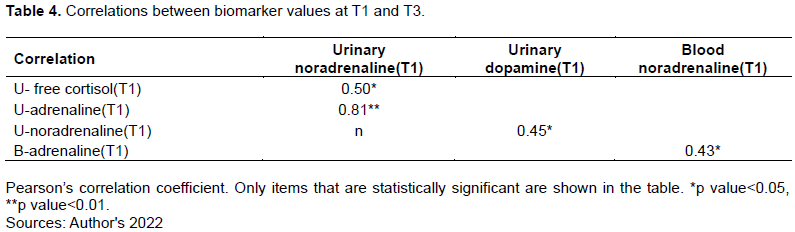
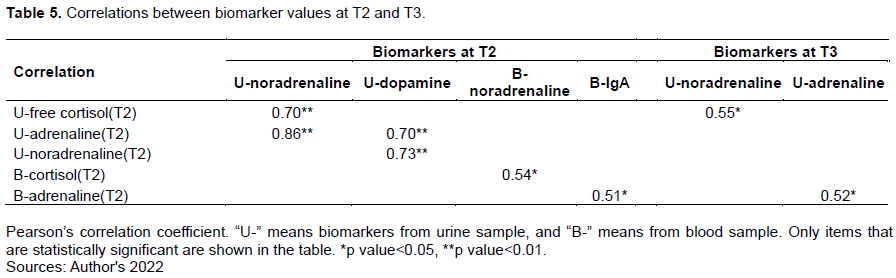
Among the biomarker items at two time points during gestation (T1&T2), the results of an analysis of the items that correlated with the values at T3 showed a moderately significant correlation between urinary free cortisol at T2 and urinary noradrenaline at T3, shown in Table 5 (r=0.55, p=0.02). Additionally, there was a moderately significant correlation between blood adrenaline at T2 and urinary adrenaline at T3 (r=0.52, p=0.03). Regarding the items at T1, none of them showed statistically significant correlation with the values of each item at T3 (Table 4).
DISCUSSION
The current study aimed (1) to analyze biomarkers that could predict the status of depression at 1-month postpartum and (2) to elucidate the association between the 10 biomarkers measured at three time points (6 months of gestation (T1), 9 months of gestation (T2), and 1-month postpartum (T3)) and the psychological scales using blood, urine, and breast milk specimens from 24 mothers. Discussion will be made whether biomarkers can be a useful objective measure of psychological status on the basis of the examination results of the relationship between the questionnaire and biomarker values, and whether the psychological status during pregnancy can predict the possibility of postpartum depression.
Participant characteristics
With the average age of primiparous Japanese mothers in 2017 - 2019 being 30.7 years (Ministry of Health, Labor and Welfare, 2021), the participants of this study can be considered a population that tends to be generally similar to the childbearing age of Japanese women. Moreover, compared to the percentage of primiparous women with the number of births in Japan (approximately 45.9%), many of the participants in this study were primiparous (Ministry of Health, Labor and Welfare, 2021). All five subjects who were not located after T2 were primiparous, but even taking this into account, this is a population in which primiparous mothers are approximately twice as common as multiparous mothers. Therefore, the effects of the differences in parity characteristics should be considered.
Predictability of psychological status at 1 month postpartum in terms of biomarker values during pregnancy and the postpartum period
This study found a significant correlation between T3 EPDS scores and T3 urinary dopamine, as well as T3 GHQ-30 scores and T3 breast milk IgA. Thus, as the likelihood of postpartum depression increased, urinary dopamine levels increased, whereas breast milk IgA decreased. This finding suggests that biomarkers can be used as objective assessment tools for psychological status during the postpartum period.
Previous studies have also reported the possibility of measuring physical and psychological stress in organisms using urine catecholamines (Steckl and Ray, 2018; Zipursky et al., 2017; Sakuma and Nagasaka, 1996). Urine dopamine is a type of urinary catecholamine, and the current study supports these findings. The results for IgA in breast milk also support those of previous studies (Juncker et al., 2022; Ziomkiewicz et al., 2021; Groër et al., 2005), which revealed that IgA in breast milk decreased under high stress conditions. When using breast milk samples for assessment, new donated breast milk from the mothers must be obtained and used. However, given that some mothers stop breastfeeding after childbirth because they are on medication or because they wish to stop breastfeeding, obtaining breast milk samples uniformly from all mothers is difficult. Furthermore, mothers face time constraints in collecting specimens, and space is also required to collect samples, which is also a facility issue. Meanwhile, there are always remnant samples of urine and blood, so there is no problem with sample collection. However, due to the cost and time required to perform biochemical tests in the laboratory, results may not be available while the mother is visiting the hospital for her one-month checkup, making it impossible to identify and respond to the problem at an early stage. To obtain immediate results and immediately identify mothers who need to be addressed, it is desirable to be able to realize simple evaluations using test strips, as is the case with urine protein and urine glucose.
Relevance of psychological status during pregnancy and the postpartum period
In the current study, the biomarkers collected during pregnancy did not suggest direct predictors of psychological status during the postpartum period. However, a moderate correlation was found between some of the urinary and blood biomarkers (urinary cortisol and blood adrenaline) at T2 and some of the urinary catecholamines (adrenaline and noradrenaline) at T3. This suggests that heightened psychological and physical stress in late pregnancy may also affect the psychological status during the first month postpartum. Given that urinary catecholamines can potentially be useful in predicting stress levels, as shown in the literature, if the association between these biomarkers in late pregnancy and the postpartum period is robust, the measurement of biomarkers in late pregnancy may be used for the risk assessment of postpartum depression during pregnancy.
STUDY LIMITATIONS
Due to the small sample size, it is necessary to carefully select the types of biomarkers and scales to be investigated and increase the sample size for future studies, such as multiple regression analysis based on the correlations obtained in this study.
In addition, since the survey was conducted in a limited area within Japan, there are limitations in generalizing the results of this study.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Bashiri N, Spielvogel AM (1999). Postpartum depression: a cross-cultural perspective. Primary Care Update for OB/GYNS 6(3):82-87. |
|
|
Bowers K, Ding L, Gregory S, Yolton K, Ji H, Meyer J, Ammerman RT, Van Ginkel J, Folger A (2018). Maternal distress and hair cortisol in pregnancy among women with elevated adverse childhood experiences. Psychoneuroendocrinology 95:145-148. |
|
|
Briguglio G, Teodoro M, Italia S, Verduci F, Pollicino M, Coco M, De Vita A, Micali E, Alibrandi A, Lembo G, Costa C, Fenga C (2021). Salivary Biomarkers and Work-Related Stress in Night Shift Workers. International Journal of Environmental Research and Public Health 18(6):3184. |
|
|
Buysse DJ, Reynolds CF, III, Monk TH, Berman SR, Kupfer DJ (1989). The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Research 28:193-213. |
|
|
Cevik A, Alan S (2021). Are pregnancy and postpartum oxytocin level a predictive biomarker for postpartum depression? Journal of Obstetrics and Gynaecology Research 47(12):4280-4288. |
|
|
Cox MJ, Owen MT, Henderson VK, Margand NA (1992). Prediction of infant-father and infant-mother attachment. Developmental Psychology 28:474-483. |
|
|
Doi Y, Minowa M, Uchiyama M, Okawa M, Kim K, Shibui K, Kamei Y (2000). Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects 97(2-3):165-172. |
|
|
Goldberg DP, Hillier VF (1979). A scaled version of the General Health Questionnaire. Psychological Medicine 9(1):139-145. |
|
|
Groër M, Davis M, Casey K, Short B, Smith K, Groër S (2005). Neuroendocrine and immune relationships in postpartum fatigue. MCN the American Journal of Maternal Child Nursing 30(2):133-138. |
|
|
Iliadis SI, Koulouris P, Gingnell M, Sylvén SM, Sundström-Poromaa I, Ekselius L, Papadopoulos FC, Skalkidou A (2015). Personality and risk for postpartum depressive symptoms. Archives of Women's Mental Health 18(3):539-46. |
|
|
Japanese Society of Perinatal Mental Health (2017). Perinatal Mental Health Consensus?Guide (ver. 1) CQ2: How to screen perinatal depression? (in Japanese). |
|
|
Juncker HG, Ruhé EJM, Korosi A, van Goudoever JB, van Gils MJ, van Keulen BJ (2022). Maternal Stress and Human Milk Antibodies During the COVID-19 Pandemic. Frontiers in Nutrition 9:923501. |
|
|
Koutra K, Vassilaki M, Georgiou V, Koutis A, Bitsios P, Chatzi L, Kogevinas M (2014). Antenatal maternal mental health as determinant of postpartum depression in a population based mother-child cohort (Rhea Study) in Crete, Greece. Social Psychiatry and Psychiatric Epidemiology 49(5):711-721. |
|
|
Ministry of Health, Labor and Welfare (2021). Overview of birth statistics 2021 1. Birth trends (in Japanese). |
|
|
Ministry of Health, Labor and Welfare (2021). Overview of monthly vital statistics annual report 2021 2. number of births (in Japanese). |
|
|
Mlili NE, Ahabrach H, Cauli O (2022). Hair Cortisol Concentration as a Biomarker of Symptoms of Depression in the Perinatal Period. CNS and Neurological Disorders Drug Targets, Mar 16. |
|
|
Nakagawa Y, Daibou I (1985). The Japanese Version of the GHQ (in Japanese). Tokyo: Nihon Bunka Kagakusha. |
|
|
Okano S, Murata M, Masuchi S, Tamaki R, Nomura J, Miyaoka H (1996). Reliability and validity of Japanese version of Edinburgh Postpartum Depression Self-assessment Scale (EPDS) (in Japanese). Psychiatry Diagnostics, 7(4):525-533. |
|
|
Oyetunji A, Chandra P (2020). Postpartum stress and infant outcome: A review of current literature. Psychiatry Research 284:112769. |
|
|
Quevedo de Avila L, Scholl CC, de Matos MB, da Silva RA, da Cunha Coelho FM, Pinheiro KAT, Pinheiro RT (2021). Suicide Risk and Mood Disorders in Women in the Postpartum Period: a Longitudinal Study. Psychiatric Quarterly, 92(2):513-522. |
|
|
Radloff LS (1977). The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychological Measurement 1(3):385-401. |
|
|
Sakuma N, Nagasaka N (1996). Changes in urinary excretion of catecholamines and their metabolites in pediatric dental patients. ASDC Journal of Dentistry for Children, 63(2):118-22. |
|
|
Shima S, Kano T, Kitamura T, Asai M (1985). New Depression Self-Rating Scale. Psychiatry 27:717-723. |
|
|
Steckl AJ, Ray P (2018). Stress Biomarkers in Biological Fluids and Their Point-of-Use Detection. ACS Sensors 3(10):2025-2044. |
|
|
Takeda S, Takeda J, Murakami K, Kubo T, Hamada H, Murakami M, Makino S, Itoh H, Ohba T, Naruse K, Tanaka H, Kanayama N, Matsubara S, Sameshima H, Ikeda T (2017). Annual Report of the Perinatology Committee, Japan Society of Obstetrics and Gynecology, 2015: Proposal of urgent measures to reduce maternal deaths. Journal of Obstetrics and Gynaecology Research 43(1):5-7. |
|
|
Takehara K, Suto M, Kato T (2020). Parental psychological distress in the postnatal period in Japan: a population-based analysis of a national cross-sectional survey. Scientific Reports 10:13770. |
|
|
Tokumitsu K, Sugawara N, Maruo K, Suzuki T, Yasui-Furukori N, Shimoda K (2020). Prevalence of perinatal depression among Japanese men: a meta-analysis. Annals of General Psychiatry 19:65. |
|
|
Toshima H (2018). Occupational stress among care workers: evaluation by a novel physiological method (in Japanese). Nihon Koshu Eisei Zasshi 65(6):266-276. |
|
|
Vlenterie R, Geuijen PM, van Gelder MMHJ, Roeleveld N (2021). Questionnaires and salivary cortisol to measure stress and depression in mid-pregnancy. Public Library of Science Online 16(4):e0250459. |
|
|
Ziomkiewicz A, Apanasewicz A, Danel DP, Babiszewska M, Piosek M, Orczyk-Pawi?owicz M (2021). Maternal Distress and Social Support Are Linked to Human Milk Immune Properties. Nutrients 13(6):1857. |
|
|
Zipursky RT, Press MC, Srikanthan P, Gornbein J, McClelland R, Watson K, Horwich TB (2017). Relation of Stress Hormones (Urinary Catecholamines/Cortisol) to Coronary Artery Calcium in Men Versus Women (from the Multi-Ethnic Study of Atherosclerosis [MESA]). American Journal of Cardiology 119(12):1963-1971. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


