Full Length Research Paper

ABSTRACT
In Japan, many young women desire to be slim, contributing to an increase in the number of women with low gestational weight gain. This study aimed to clarify the association between low gestational weight gain and low birth weight infant, desire of pregnant women to be slim, self-efficacy, or quality of life (QOL). Subjects were Japanese women in their ≥24th week of pregnancy who visited four primary hospitals in Japan for prenatal checkups. We conducted a self-administered questionnaire survey of these women and later collected information on childbirth from medical records. Analysis of pre-pregnancy weight showed that 43 (16%) of 268 pregnant women were underweight. Gestational weight gain was insufficient in 172 (64%) women based on the IOM recommendation or in 35 (13%) women based on the guideline used in Japan. More than 50% of the women had a desire to be slim, and 16% were actually on a diet during the first trimester. Self-efficacy had no correlation to low gestational weight gain, whereas gestational weight gain of <10 kg was correlated with low birth weight infant (p <0.025) and poor physical QOL among the women (p<0.019). Research shows that Japanese pregnant women are likely to desire to be too slim, in addition to being a risk factor for infants with low birth weight. Low gestational weight gain is associated with poor physical QOL, but not self-efficacy in pregnant women. It is important for health providers to establish positive prenatal care that does not reinforce weight consciousness among Japanese pregnant women.
Key words: Maternal underweight, gestational weight gain, quality of life, low birth weight infant, desire to be slender.
INTRODUCTION
In Japan, the number of pregnant women who are underweight is on the rise, along with an increasing desire in young women to be thin. In a study conducted by Tsukamoto et al. (2007), approximately 10% of pregnant women had a body mass index (BMI) of <18.5.
In addition, the Ministry of Health, labour and Welfare (2013) estimated that 20 to 25% of Japanese women in their 20s are underweight. From the global perspective, such decline in BMI among Japanese young women is a rare event. Maternal underweight is a known risk factor for giving birth to a low birth weight (LBW) infant (Rahman et al., 2015). Japanese groups have also reported similar findings (Takimoto et al., 2006; Tsukamoto et al., 2007).
In Japan, the birth weight of infants began to decrease in the 1980s and the percentage of LBW infants, which was around 5% in the 1980s, increased to 9.6% in 2009 and has remained at similar levels since (Ministry of Health, Labour and Welfare, 2013). In contrast, no decline in birth weight has been observed in other developed countries, owing to advances in medical technology and a general increase in women’s body size. According to recent epidemiological studies, LBW caused by maternal malnutrition is associated with a high risk of developing lifestyle diseases such as diabetes (Gluckman et al., 2007). In addition, Yachi et al. (2013b) showed that low BMIs at between 20 to 29 years of age is a predictor of gestational diabetes, suggesting that health of both infants and mothers is at risk.
In 2006, the Ministry of Health, Labour and Welfare recommended an optimum gestational weight gain of 9 to 12 kg for women with BMI <18.5 (underweight) and 7 to 12 kg for those with BMI 18.5 to 24.9 (normal weight). However, in 2009, the Institute of Medicine (IOM) of the National Academies of Sciences, Engineering, and Medicine, recommended total gestational weight gain to be 12.5 to 18 kg in underweight women and 11.5 to 16 kg in those with normal weight. This shows that the Japanese guidelines are set at low levels, but it is unclear whether the difference between the IOM’s and Japanese guidelines was because of ethnic variability in physique.
It is not easy to maintain a balance between sufficient nutritional intake and optimum weight gain. It is also difficult to objectively evaluate health-related behavior of young women because of their diverse pre-pregnancy lifestyles and individual variability in weight consciousness. As a result, standardized prenatal education is offered to pregnant women. However, it may be possible to elucidate the proper direction of care if we can understand health-related behavior among Japanese women and psychosocial issues causing underweight. Therefore, in this study we aimed to reveal the association between low gestational weight gain and LBW infant, desire among pregnant women to be slim, self-efficacy, health-related behavior, and quality of life (QOL).
MATERIALS AND METHODS
Participants and procedure
This study used cross-sectional method. We conducted a self-administered questionnaire survey of pregnant women (first survey) and later collected information about childbirth from their records (second survey). Subjects were 268 Japanese women who were in their ≥24th week of pregnancy and visited one of four primary care hospitals in Japan for health checkups. Pregnant women with multiple fetuses were excluded from the study. In February to March 2013, the purpose and outline of the study were explained to subjects at the outpatient clinic of each hospital, and a questionnaire survey form was handed to those who had consented to participate in the study. After filling in the form, subjects returned the form by dropping it in a box placed in the outpatient clinic or via mail later. Between March and October 2013, childbirth-related information was collected from their medical record.
Questionnaire forms were returned from 300 consenting subjects. After excluding 32 subjects because of insufficient answers, hospital transfer, or medical complications, 268 (89.3%) subjects were enrolled in the study. In addition, 241 (80.3%) subjects were evaluated in an analysis of pregnant women with BMI < 25, for analysis of association between low gestational weight gain and low birth weight gain, desire to be slender, self-efficacy, and QOL, the reason why to be considered the effect of obesity.
Statistical analysis was performed using IBM SPSS Statistics (version 22), with statistical significance set at p<.05. The chi-square independence test was used for contingency tables, and the Mann-Whitney U test or t-test was used to compare two groups. In addition, a logistic regression analysis was performed to extract risk factors for LBW infant. This study was approved by the Medical Ethics Committee of the University of Tsukuba hospital.
Measures
In the survey, subjects provided information on their age, pregnancy week, occupation, education history, history of childbirth, history of marriage, height, and pre-pregnancy weight. Information on minor pregnancy complications, pregnancy week and weight at childbirth, placenta weight, and blood loss at delivery was collected from medical records. The survey contained four questions about desire to be slim, two of which were yes/no questions asking whether subjects were “wanting to lose weight” or “actually dieting” before becoming pregnant. The other two questions asked whether subjects were “wanting to stay slender during pregnancy” and “worrying about postpartum changes in body shape” using a 5-point scale from 1, “not at all” to 5, “very much so”.
In 1997, Bandura A (1997) defined self-efficacy as one's belief in one's own ability to accomplish a task. The General Self-Efficacy Scale was developed based on the self-efficacy theory; this study used the Japanese version of this scale. The scale consists of 16 items, and its reliability and validity have been verified (Sakano et al. 1986). Each item is answered by selecting either “yes (1 point)?” or “no (0 point)?”, and high scores indicate high self-efficacy.
Health-related behavior in subjects was asked using 7 questions on breakfast, nutritional balance, sleep, exercise, weight, drinking, and smoking.
QOL was evaluated using the Health-Related quality of Life scale developed by the World Health Organization (WHOQOL Group, 1994). This scale is a 26-item assessment tool consisting of 4 subscales: Physical health, psychological health, social relationships, and environmental health. The reliability and validity of the Japanese version have been verified (Tazaki et al., 1997). Subjects were asked about their lifestyle in the last two years and answered using a 5-point scale, from 1, “not at all” to 5, “extremely well”.
RESULTS
Participant characteristics
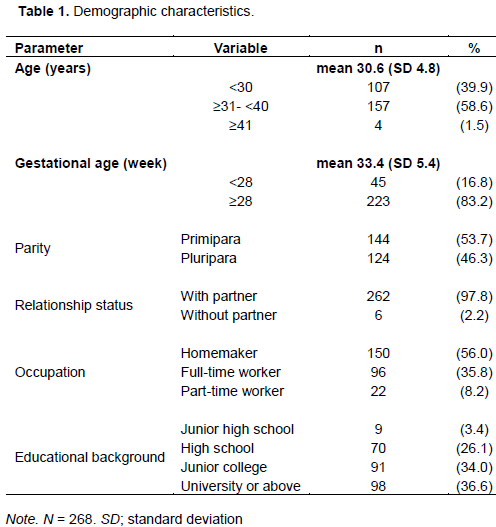
Table 1 shows patient characteristics and childbirth-related information. Mean age (SD; standard deviation) was 30.6 (SD 4.8) years, and mean pregnancy week was 33.4 (SD 5.4). With regard to delivery history and marital status, 144 (53.7%) and 124 (46.3%) women were primipara and multipara, respectively, and 262 (97.8) and 6 (2.2%) were married or single, respectively. Anemia was observed in 116 (45.3%) women, premature delivery in 3, LBW infant in 14 (5.2%), macrosonia in 1, cesarean delivery in 37 (13.8%), and atonic bleeding in 47 (17.5%). Mean gestational duration was 39.1(SD 1.1) weeks.
Association between low gestational weight gain and low birth weight infant
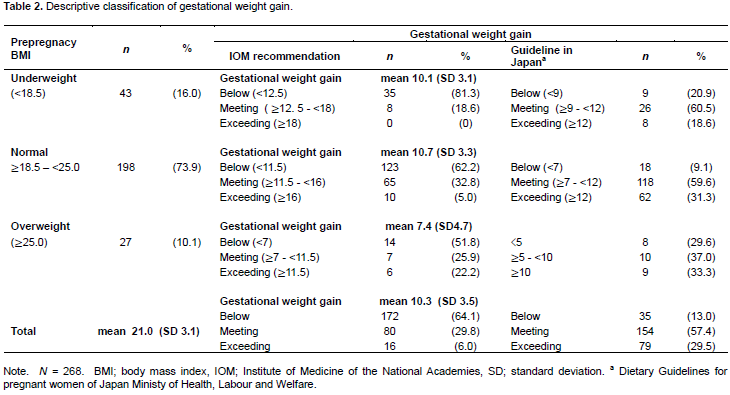
The mean pre-pregnancy BMI of 268 subjects was 21.0 (SD 3.1) and mean gestational weight gain was 10.3 (SD3.5) kg. Subjects were divided into 3 groups based on pre-pregnancy BMI: a total of 43 (16.0%) women with a BMI of <18.5 were considered underweight, 198 (73.9%) with a BMI of ≥18.5 to <25.0 were normal, and 27 (10.1%) with a BMI of ≥25.0 were overweight. Next, gestational weight gain was categorized as insufficient, adequate, or excessive according to IOM recommendations and Japanese guidelines (Table 2). Because the Japanese guidelines do not specify the optimum level of weight gain for pregnant women whose BMI is ≥25.0, we defined <5 kg as insufficient, ≥5 to <10 kg as adequate, and ≥10 kg as excessive. According to the IOM recommendation, 172 (64.1%) pregnant women had insufficient weight gain, but according to the Japanese guideline, this was 35 (13.0%). Mean weight gain was 10.1 (SD3.1) kg in a group of underweight women and 10.7 (SD3.3) kg in a group of normal women, with no significant difference between the groups (p = 0.334).
After excluding overweight woman (BMI of ≥25), the remaining 241 pregnant women were analyzed using logistic regression, with the dependent variable as LBW and independent variables <10 kg and ≥10 kg, to reveal a correlation between LBW infant and low gestational weight gain. After adjusting for pre-pregnancy weight, age, height, history of childbirth, and gestational week, the data showed that a risk of having a LBW infant was 11.1 times when gestational weight gain was <10 kg (p = 0.025; 95% Cl [1.3, 92.8]).
Desire to be slender
Among 241 pregnant women, not including those with BMI ≥25, 130 (53.9%) were “wanting to lose weight” around the time they found out about their pregnancy, while 39 (16.2%) were “actually dieting”. In addition, when asked whether they were concerned about postpartum changes in their body shape, 207 (85.9%) pregnant women answered with “somewhat”, “yes”, or “very much so”. When asked whether they wanted to stay slender during pregnancy, 140 (58.1%) pregnant women answered with “somewhat”, “yes”, or “very much so”, indicating that more than half the women who were not overweight were concerned about their weight and wanted to stay slender during pregnancy.
Health behaviors A total of 195 (72.8%) of the 268 women “had breakfast every morning”, 101 (37.7%) were eating a balanced diet, and 109 (40.7%) slept more than 7 hours. However, 133 (49.6%) pregnant women did not exercise at all, and 48 (17.9%) did not measure their weight regularly. Drinking and smoking were observed in 6 (0.2%) and 10 (0.7%) women, respectively.
Association between low gestational weight gain and desire to be slender, self-efficacy, and QOL
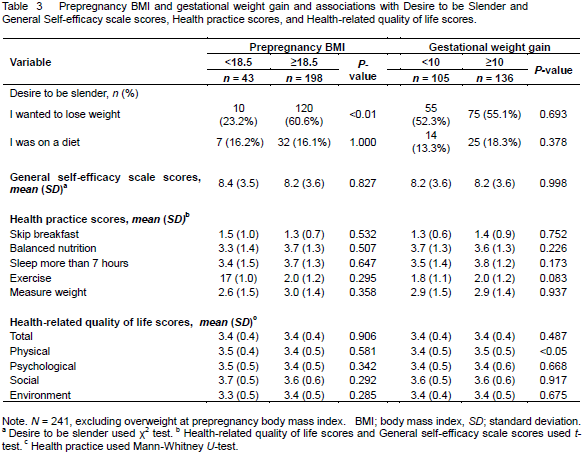
After excluding women with a BMI of ≥25, we compared desire to be slender, general self-efficacy scale scores, and health-related quality of life scores among 241 pregnant women based on pre-pregnancy BMI (<18.5 or ≥18.5) and gestational weight gain (<10 kg or ≥10 kg) (Table 3). Regardless of pre-pregnancy BMI or gestational weight gain, some women were actually dieting during the first trimester, with no significant difference between groups. In addition, no significant correlation was observed between general self-efficacy scale scores and pre-pregnancy BMI or gestational weight gain. Physical QOL was rated low in pregnant women with gestational weight gain of <10 kg (p =0.019; 95% CI [-0.30, -0.02]. t (239) = -2.3).
DISCUSSION
Before becoming pregnant, 16% of the women were underweight. Taking into consideration the global trends in overweight, the pre-pregnancy mean BMI of 21.0 is extremely low (Hill et al., 2015). Although 64% of the women had insufficient weight gain according to the IOM recommendation, the calculation using the Japanese guideline yielded 13%. Gestational weight gain of <10 kg was correlated with LBW infant as well as low physical QOL. In the present study, pregnant women had a mostly healthy lifestyle, but more than half of the women had a desire to be slim, and 16% were actually dieting during the first trimester. We analyzed these findings in terms of psychological characteristics among Japanese women and challenges among care providers.
In many women desire to be slim is tied to the desire to remain beautiful and is influenced greatly by media reports on diet plans and fashion (Uragami et al., 2015). However, similar media reports are likely to be found overseas. Therefore, we asked why Japanese women have a desire to control weight gain by restricting nutritional intake and thus affecting the growth of fetus for their fetus. Yates et al. (2004) reported that Japanese young women have low levels of satisfaction with their appearance despite being underweight. Such self-cognition among Japanese women is similar to the situation in eating disorders. (Bruch and Czyzewski (1988) defined an eating disorder as a pathological state of self-esteem in people who worry about how they look to others. Does this imply that Japanese women as a race have low self-esteem? No correlation was observed between self-efficacy and underweight in this study, suggesting that in Japan a cultural preference for women who are receptive and cooperative may be more strongly involved in the perception of beauty. The relatively high self-efficacy observed in this study may indicate that because self-cognition is established normally through comparisons with others, self-efficacy is not reduced among Japanese even when living in a society with other Japanese as the overwhelming majority.
Desire to be slim may reflect an attempt to boost one’s self-esteem to compensate for unwelcome self-assertiveness. In addition to individual desire to be slim, prenatal education provided by healthcare provider may contribute to low gestational weight gain. Because of highly publicized risks associated with obesity in pregnancy, a weekly weight gain of ≤500 g was established as an easily attainable health index, and health professionals stress the importance of not exceeding this limit to pregnant women during prenatal checkups without conveying the risks associated with insufficient weight gain. This study showed that gestational weight gain of <10 kg is a risk factor for LBW infant, suggesting that 7 kg, which is the minimal weight gain recommended for pregnant women with normal weight, is insufficient for fetal growth. Conversely, other studies have found that the gestational weight gains recommended by the IOM were effective in Chinese women, who are another Asian cohort (Wong et al. 2000).
Healthcare providers should explain the scientific evidence of the risks associated with fetal development or postpartum health problems and educate on proper eating habits. Yachi et al. (2013a) reported that the recommended extra 450-kcal energy intake during the third trimester is not followed in Japan. Healthcare providers should not make pregnant women unnecessarily anxious using the standard weight gain value of <500 g per week just because it is difficult to change individuals’ value about their appearance. It is desirable that the healthcare providers recommend exercise, in addition to diet, as a preventive measure against excessive weight gain. More than half of the pregnant women in the present study did not exercise during pregnancy. In addition, prenatal education should be given using positive terms such “as intake of nutrients essential for the healthy development of the fetus” or “the improvement of physical strength needed for easy and safe delivery”, instead of using negative terms such as “the prevention of weight gain” or “dietary restriction”, which may reinforce the desire to be slim.
In conclusion, research shows that Japanese pregnant women are likely to desire to be too slim, in addition to being a risk factor for infants with low birth weight. Low gestational weight gain is associated with poor physical QOL, but not self-efficacy in Japanese pregnant women. It is important for health providers to establish positive prenatal care that does not reinforce weight consciousness among Japanese pregnant women. Further research is needed to determine in study area.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
This study was supported by a Grant-in-Aid for Challenging Exploratory Research for FY2011–2013 from the Japan Society for the Promotion of Science (No. 23660057). We thank the pregnant women in the present study for their participation.
REFERENCES
|
Bandura A (1997). Self-efficacy: the exercise of control. New York: Freeman WH. |
|
|
Bruch H, Czyzewski D (1988). Conversations with anorexics. New York: Basic Books. |
|
|
Gluckman PD, Seng CY, Fukuoka H, Beedle AS, Hanson MA (2007). Low birthweight and subsequent obesity in Japan. Lancet 369(9567):1081-1082. |
|
|
Hill B, Mcphie S, Skouteris H (2015). The Role of Parity in Gestational Weight Gain and Postpartum Weight Retention. Women's Health Issues 26(1):123-129. |
|
|
Ministry of Health, Labour and Welfare (2013). National Health and Nutrition Survey. (In Japanese.) |
|
|
Ministry of Health, Labour and Welfare (2006). Dietary Guidelines for Pregnant and Lactating Women. (In Japanese.) Available at: |
|
|
Rahman MM, Abe SK, Kanda M, Narita S, Rahman MS, Bilano V, Ota E, Gilmour S, Shibuya K (2015). Maternal body mass index and risk of birth and maternal health outcomes in low- and middle-income countries: a systematic review and meta-analysis. Obes. Rev. 16(9):758-770. |
|
|
Sakano Y, Tohjyo M (1986). The General self-efficacy scale (GSES): Scale development and validation. Jpn Assoc. Behav. Cogn. Ther 12(1):73-82. (In Japanese). |
|
|
Takimoto H, Sugiyama T, Fukuoka H, Kato N, Yoshiike N (2006). Maternal weight gain ranges for optimal fetal growth in Japanese women. Int. J. Gynecol. Obstet. 92(3):272-278. |
|
|
Tazaki M, Nakane M (1997). WHO Quality of Life 26, Tokyo: Kanekoshobo. (In Japanese.) |
|
|
Tsukamoto H, Fukuoka H, Koyasu M, Nagai Y, Takimoto H (2007).Risk factors for small for gestational age. Pediatr. Int. 49(6):985-990. |
|
|
Uragami R, Kojima Y, Sawamiya Y (2015). Relation between media use and thin-ideal internalization: University undergraduates. Jpn. J. Educ. Psychol. 63:309-322. (In Japanese.) |
|
|
WHOQOL Group (World Health Organization Quality-of-Life) (1994). Development of the WHOQOL: Rationale and Current Status. Int. J. Mental Health 23:24-56. |
|
|
Wong W, Tang N, Lau T, Wong T (2000). A new recommendation for maternal weight gain in Chinese women. J. Am. Diet. Assoc. 100(7):791-796. |
|
|
Yachi Y, Sone H (2013a). Interm analysis of dietary intake and pregnancy course in Japanese pregnant women. Jpn. Soc. Nutr. Diet. 71(5):242-252. (In Japanese). |
|
|
Yachi Y, Tanaka Y, Nishibata I, Sugawara A, Kodama S, Saito K, Sone H (2013b). Low BMI at age 20 years predicts gestational diabetes independent of BMI in early pregnancy in Japan: Tanaka Women's Clinic Study. Diabet. Med. 30(1):70-73. |
|
|
Yates A, Edman J, Aruguete M (2004). Ethnic differences in BMI and body/self-dissatisfaction among Whites, Asian subgroups, Pacific Islanders, and African-Americans. J. Adolesc. Health 34:300-307. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


