Full Length Research Paper

ABSTRACT
Childbirth is perhaps, the most painful experience encountered by most women and just like other forms of pain, the experience of labour pain is unique to individual women, so it is only the woman in labour who can describe the extent of pain she is going through. This study assessed the perceptions, attitude, intention to use, also predict factors that influence intention to use epidural analgesia among pregnant women attending antenatal clinic. The study adopted a cross-sectional design and was conducted among 200 randomly selected pregnant women attending Ante-natal Clinic of Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria. Data were obtained using a structured questionnaire and were analyzed descriptively and inferentially. Statistical significance was determined at p < 0.05. The study revealed that majority (85%) of the respondents had good perception of epidural analgesia but majority (86%) displayed negative attitude toward epidural analgesia. More than half (56%) of the respondents got their information on epidural analgesia from nurses and midwives and 72.5% expressed their intention to use epidural analgesia (EA). Furthermore, there was significant relationship between ethnicity and attitude towards epidural analgesia (p= 0.001). Factors predicting intention to use EA include religion (B=0.99, p=0.016), perception of EA (B=-2.47, p=0.001), appropriate pain control (B=1.75, p=0.02), fear of pain procedure (B=-0.2, p=0.01). The study concluded that pregnant women in this setting have a desire to use EA for child birth. Factors that predict the use include perception, religion, and desire for pain control. Efforts should be intensity to improve on the negative attitude of the respondents as this will ensure prompt intervention which may result in positive birth outcome.
Key words: Perception, attitude, epidural, analgesia, pregnant women.
INTRODUCTION
Motherhood comes with many prices for every woman, and one of such is the pain of childbirth. Childbirth is one of the most amazing and unforgettable experience in a woman's life and the number or time of birth.
Notwithstanding, each labour pain’s experience is unique to individual women and calls for a celebration (Whitburn et al., 2017). However, childbirth is perhaps, the most painful experience encountered by most women and it is only the woman in labour who can describe or know the extent of pain she is going through. The anticipated experience of labour pain is one of the thoughts that occupy the mind of a pregnant woman as her due date approaches. The fear and anxiety generated by the feelings about childbirth often prevent most women from enjoying this experience.
Labour is the series of events that take place in the uterus and the vagina to expel the products of conception out of the womb through the vagina into the outer world (Garg and Vanitha, 2019). Although the body of a woman is physiologically designed to go through labour, the process is often accompanied with some degree of stress, discomfort and pain as the system responds to changes that prepare a woman for childbirth. The pain of labour is not known to be beneficial to the process of labour (Onyekwulu et al., 2017) and the maternal physiological responses to labour pain may affect maternal and foetal wellbeing and progress of labour (International Association for the Study of Pain IASP, 2011). To have positive health outcomes for both mother and child despite the pain associated with childbirth, various pharmacological and non-pharmacological methods have been developed to alleviate the labour pains (Ekweani and Avidime, 2016; Ampofo and Caine, 2015; Barakzai et al., 2010).
The quest for pain relief in labour has been in existence in most societies for a long time and various measures such as the use of herbs, drinking wine, use of pressure, heat, water and sun were historically used to relieve childbirth pain (Ampofo and Caine, 2015). Pain relief management during labour has undergone various advancement since 1847, when Simpson found that chloroform could help relieve labour pain (Shidhaye et al., 2012). According to Onyekwulu et al. (2017), non-pharmacological methods of labour analgesia include breathing exercise, hypnosis, transcutaneous electrical nerve stimulation (TENS), low back massage, acupuncture and supportive care while pharmacological methods include parenteral opioids, inhalational agents, and epidural analgesia.
Epidural analgesia is seen as the gold standard technique of relieving labour pain satisfactorily and is the most effective method for restoration of normal uterine activity (James et al., 2012; Cambic and Wong, 2010). Anaesthetic agents placed in the epidural space at the L4-5, L3-4 or L2-3 interspace blocks not only spinal nerve roots in the space but also sympathetic nerve fibres that travel with them. Therefore, these blocks provide pain relief for both labour and birth (Robert et al., 2012). Antonakou and Papoutsis (2016) affirmed that epidural analgesia provides complete labour pain (90-95%) if administered timely and does not impede the progress of the first stage of labour.
Similarly, Okojie and Isah (2014) noted that epidural analgesia carries the advantage of an 'awake' mother who can participate in the delivery process, and foetal effects are minimal. The technique can also be extended for operative deliveries in the event of such occurrence. Its analgesic effect helps in the management of medical conditions coexisting with pregnancy such as preeclampsia by preventing further increases in the blood pressure as well as in the prevention of vaginal and cervical tears that may result from increased straining by the woman because of excessive pain resulting in life-threatening haemorrhages (Sun et al., 2019).
Although the concept of epidural anaesthesia is widely accepted as a gold standard in the management of labour pain, it is founded on an imperative concept of “patient right” (Okojie and Isah, 2014). Hence, its use is largely dependent on acceptance by the clients; based on their knowledge of its value. The use of epidural anaesthesia among pregnant women for relief of labour pain varies from one culture to another and despite the numerous advantages of epidural analgesia, studies have revealed that the technique is not popular especially in developing countries like Nigeria (Fawaz and Malas, 2018; Shareena et al., 2015; Onyekwulu et al., 2017; Okojie and Isah, 2014). Obuna and Umeora (2014) in a study among Igbo women in Southeast Nigeria reported that ignorance of existing pain relief by women and cultural prejudice accounts for inadequate demand for pain relief during labour. Among some Ghanaian cultural groups, women who are unable to endure labour pain are labelled as emotionally weak (Aziato et al., 2017). It is, therefore humiliating if others know one cannot bear labour pain (Aziato et al., 2016; Ampofo and Caine, 2015). Consequently, utilization of epidural analgesia within these areas is limited. The limited use of epidural analgesia among women during labour could be related to many factors such as inadequate service provision, lack of public awareness about its benefits, parturient ignorance, cultural issues, socioeconomic issues, obstetric factors and attitude (Barakzai et al., 2010; Mugambe et al., 2007; Mohamed et al., 2013).
Unlimited access to health information via various technology and social media has improved the awareness of pregnant women on pharmacological options available to them in managing labour pain, however, there are still misconceptions regarding epidural analgesia and their attitude towards using epidural analgesia is not well identified (Mohamed et al., 2013).
It is a known fact that pain relief in labour is an important aspect of obstetric care, both pharmacological and non-pharmacological approaches are necessary to relieve labour pain effectively (Rachmawati, 2012) and efforts to evaluate perceptions and attitudes of pregnant women towards it become important to determine aspects of it that require improvement. There is wide disparity in utilisation of labour analgesia between developed and developing countries. While analgesia for labour is widely utilized in high-income countries, the case is entirely different in Africa where socio-cultural, economic, spiritual issues revolving round awareness, acceptability and availability of epidural analgesia for labour dominate the scene as well as issues of the choice of methods and complications (Kuti et al., 2008).
There is dearth of literature on factors that determine the intention to use epidural analgesia among pregnant women during labour in Southwestern Nigeria and understanding the unique influence of factors such as knowledge, perceptions, and attitudes of pregnant women within specific socio-cultural context on pregnant women’s intention to use epidural analgesia to relieve labour pain is therefore necessary. Hence, the need for this study.
METHODOLOGY
A cross-sectional research design was adopted to assess factor associated with intention to use epidural analgesia among pregnant women attending antenatal clinic in Ife Hospital Unit of Obafemi Awolowo University Teaching Hospitals Complex (O.A.U.T.H.C), Ile-Ife, Osun State.
The sample size was determined using the Cochrane formula (n=z2p (1-p)/e2) (Singh and Masuku, 2014). Proportion of Epidural Analgesia (EA) use in previous studies includes 11.1% (Olateju et al., 2017), 19.5% (Oladokun et al., 2008), and 9.1% (Barakzai et al., 2010). Using p=13.2%, z=1.96 and e=0.05, the sample size was calculated as n=176.4 and with 10% non-response rate the sample size was calculated to be 194 but was finally increased to 200 to give room for a more robust analysis. Simple random sampling technique through balloting was adopted to recruit consenting pregnant women consecutively during antenatal clinic sessions until the required sample size was reached. The researcher visited the clinic two days per week and average of twenty-five pregnant women were randomly selected at each visit using balloting system. Data were collected with the aid of a semi-structured questionnaire comprising four sections. It was adapted from The Beliefs about Epidural Analgesia Questionnaire (BEAQ) which assesses specific beliefs about epidural analgesia that might influence the decision to choose EA. Section A of the instrument comprised eight socio-demographic variables of the respondents. Section B is a twenty items question in a 5-point Likert scale to measure the respondents’ attitudes towards epidural analgesia. For positively worded variable, the responses were scored as follows: Strongly Agree -5, Agree -4, Undecided -3, Disagree -2 and Strongly Disagree -1. Negatively worded variables were scored in reverse order. The composite score for each respondent was computed. The highest obtainable score was 95, while the least was 19. Respondents with scores from 70 and above were rated as having positive attitude about epidural analgesia for labour while those who score below were rated as having negative attitude. Section C consists of fourteen items on 2-points Likert scale (Agree and Disagree) that assessed the respondents’ perceptions towards epidural analgesia. Each correct answer was allocated a score of 2 while each incorrect answer was allocated a score of 1 for positive statement and vice versa for negative statement. The maximum score was 28 while the minimum was 0. Scores were rated as good perception (15-28) and poor perception (0-14). Section D consists of 10 variables which were used to assess factors that influence the respondent’s acceptance or refusal of epidural analgesia.
Validity of the instrument was established through face and content validity techniques. The instrument was validated by experts in the field nursing and obstetrics and gynaecology. A pilot study was conducted among pregnant women at the Urban Comprehensive Health Centre, Eleyele, Ile-Ife to determine the reliability of the instrument. Cronbach’s alpha coefficient obtained for the sections of the instrument was 0.75, 0.80, and 0.95, respectively.
The study was approved by the Ethics and Research Committee of the hospital (ERC/2019/04/06). Informed consent was obtained from the participants and the respondents were informed that their participation is voluntary and that they can withdraw their participation at any point they are unwilling to continue. Respondents were allowed to fill the questionnaires without any interference or cohesion. The questionnaires were thereafter retrieved from them and cross-checked to ascertain the completeness. For patients who could not read and write the researcher or the research assistant administered the questionnaire on them. The balloting procedure was continued until the required sample size was completed. The data collection procedure lasted for four weeks.
Data collected was analysed using the Statistical Package of Social Sciences (SPSS) version 20.0. Descriptive techniques (frequency tables and charts) were conducted to describe the data. In addition, inferential statistics like Pearson’s Chi-square and regression were used to determine associations between variables of interest and factors predicting intention to use EA among the respondents. Statistical significance was set at p<0.05.
FINDINGS
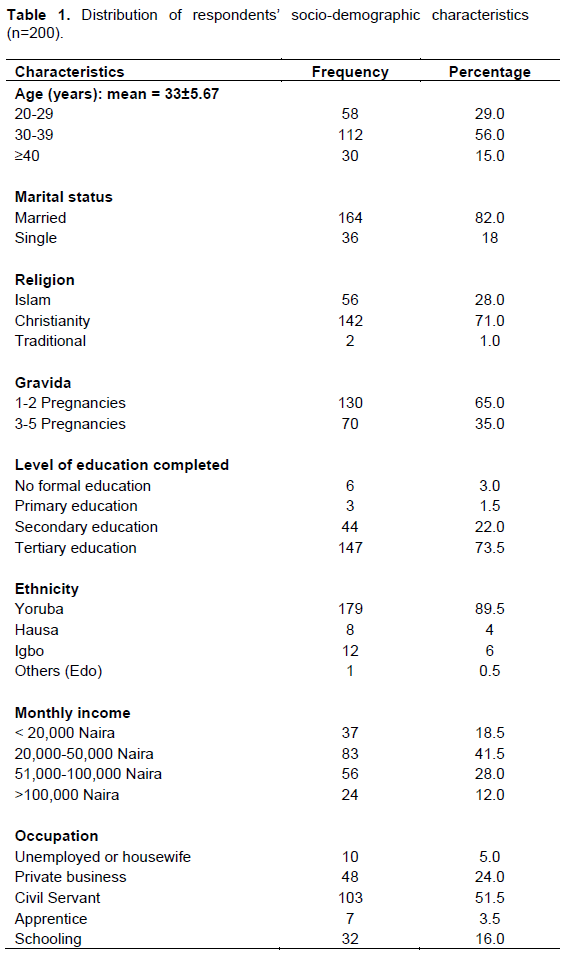
The socio-demographic characteristics of the respondents as presented in Table 1 show that the mean age of the respondents was 39±9 years with the modal age group being 30-39 years, representing 56%. Majority of the respondents were married (82%) and of Christian faith (71%). Moreover, about two-thirds of the respondents had been pregnant twice. In addition, results revealed that 73.5% had tertiary level of education. Most of the respondents were government employees (51.5%) and majority (41.5%) of them earned 20,000-50,000 Naira monthly.
The channels through which the respondents got informed about EA are as shown in Figure 1. The major sources of the respondents’ information were nurses and midwives (56%) and this was followed by doctors (22%).

Perceptions of the respondents towards epidural analgesia
Respondents’ perceptions about epidural analgesia (EA) are shown in Table 2. Epidural analgesia can be used to relief labour pains (87.5%) and that the procedure for administering EA involved inserting needle at the back (84.5%). The perceptions of the respondents vary across the indicators. While majority perceived that EA can affect their baby’s health (53%), affect their own health (56.5%) and cost them more money (78%), majority perceived that the pain of administering EA is worse than that of labour pain (74.5%), increases the risk of operative deliveries (64%) or instrumental deliveries (61%), can cause permanent back ache (68.5%) and that labour pain is a prerequisite for normal labour (62%). Despite these perceptions, majority of the pregnant women expressed intention to use EA during their next delivery (72%), but some agreed that they can recommend it for friends/relatives (74%).
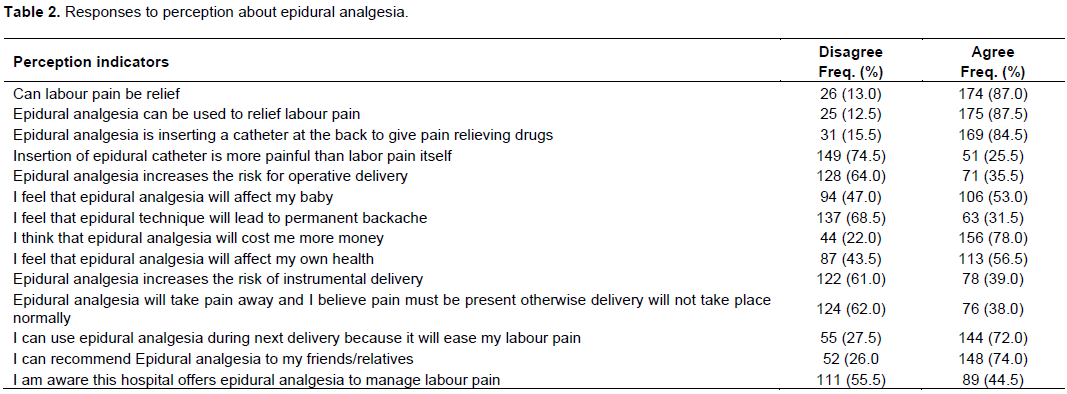
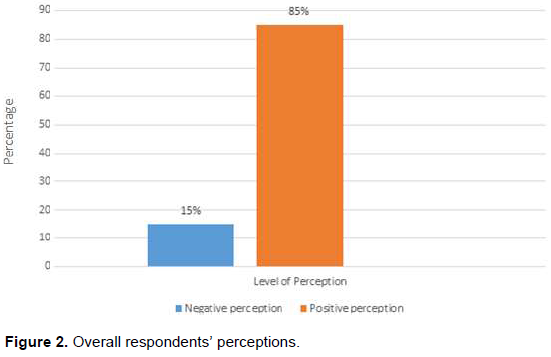
Figure 2 shows that on the aggregate, more than four-fifth (85%) of the respondents showed positive perception about epidural analgesia.
Respondents’ attitudes towards epidural analgesia
Table 3 presents the attitude of the respondents to EA. These include desire to fully enjoy childbirth process (65%), fear of pain associated with insertion of EA (53.5%), desire to have a more relaxed childbirth (58.5%) and belief in ability to give birth without anaesthesia (63.5%). Conversely, majority disagreed that they desired pain-free childbirth (62%), and that frequent use of EA shows that it does not have adverse effects (56%). However, less than half of the respondents (42%) were at the quandary about being unable to bear-down during labour with EA. A summary of the respondents’ attitude is as shown in Figure 3. Majority of the respondents (86%) showed negative attitude to epidural analgesia.
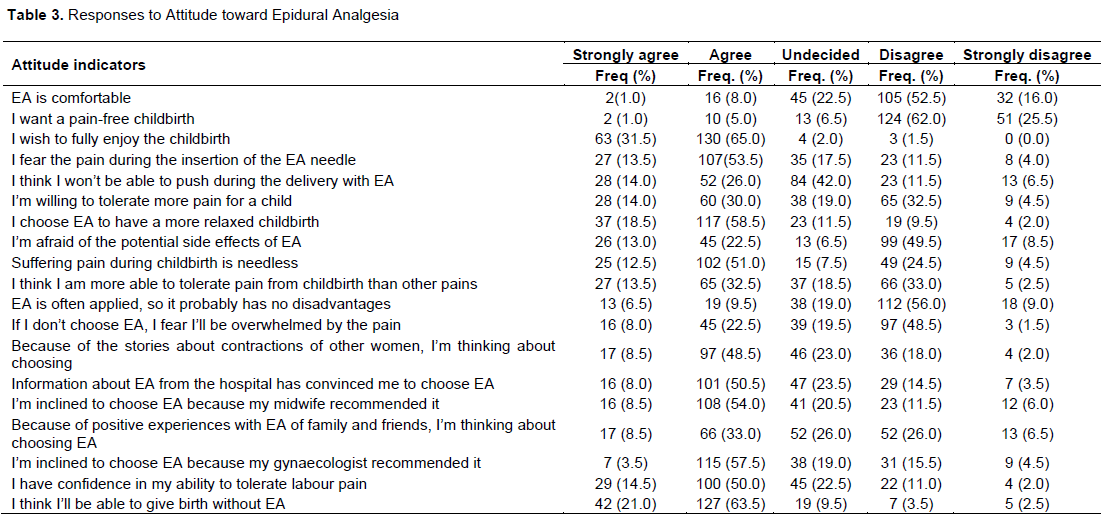
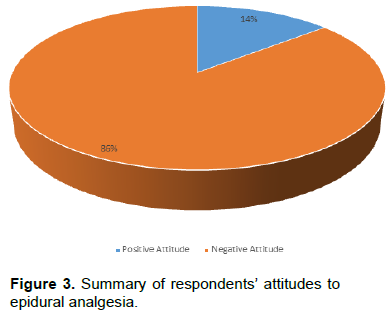
Figure 4 depicts the respondents-identified factors influencing their use of EA. Majority of the respondents (90%) identified desire for pain control as a factor influencing acceptability of Epidural Analgesia, 83.5% identified encouragement by a nurse/midwife concern over possible risk to baby (75.5%), relief of pain and stress (74.5%) and desire for natural childbirth (67%) are some of the factors which will influence the acceptance of EA by the respondents.
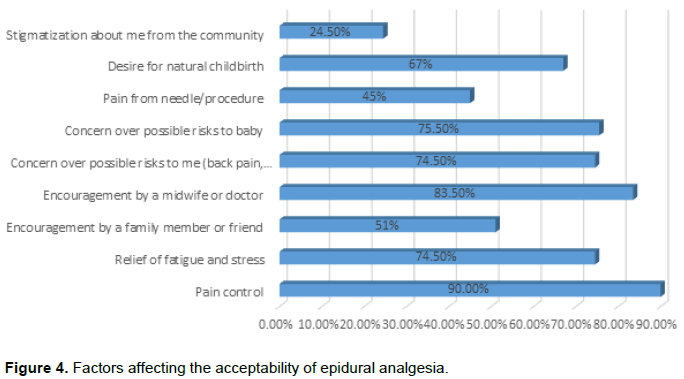
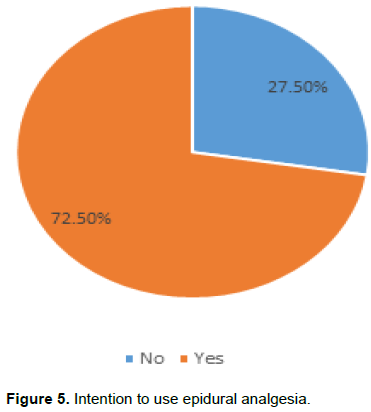
Figure 5 shows that majority of the participants 145 (72.5%) of the respondents showed their intention to use epidural analgesia.
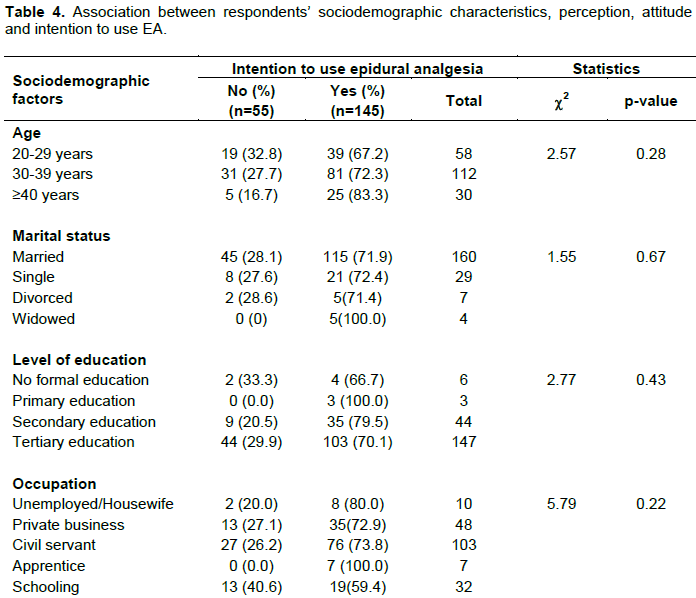
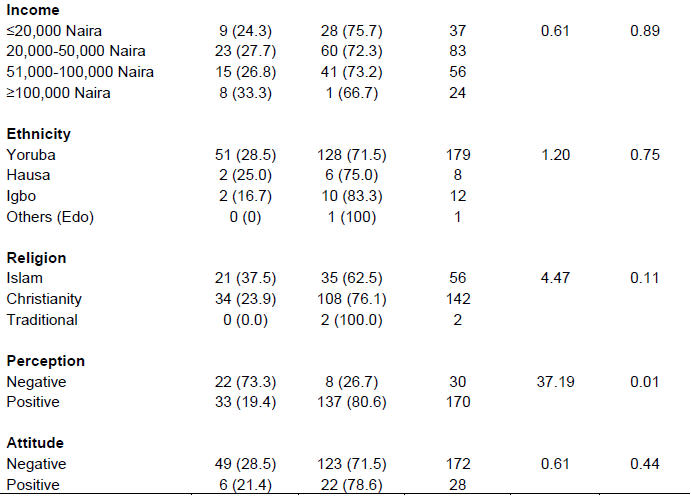
Table 4 describes the association between the independent variables (socio-demographic, attitude and perception) and intention to use EA. Among all the variables, only ethnic group of the respondents is significantly associated with their attitude. Respondents who were of Yoruba and Igbo descents were significantly more likely to show negative attitudes compared with those who were Hausa or other groups (c2=15.509, p=0.001).
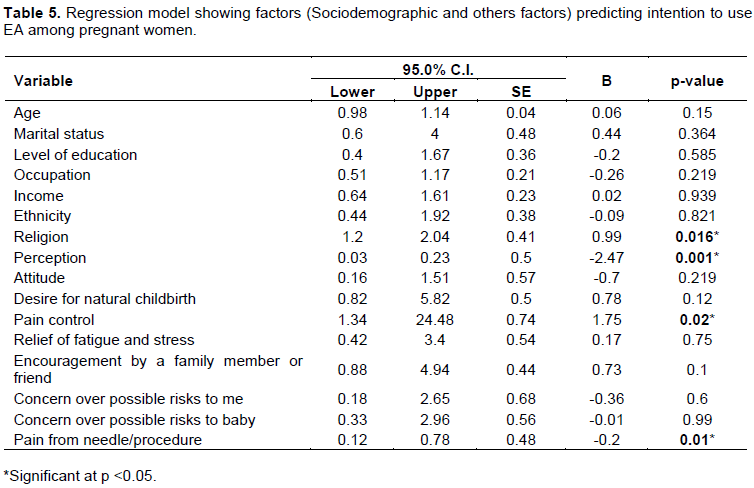
A regression model was performed to identify factors that predicts respondent to use EA. Regression analysis showed that religion (B =0.99, p= 0.016), perception (B =-2.47, p= 0.001), pain control (B =1.75, p= 0.02), and pain from needle/procedure (B =-0.2, p= 0.01) are the predictors of intention to use analgesia among participants (Table 5).
This study assessed the perceptions, attitudes and acceptability of epidural analgesia among pregnant women and also predicts factors that influence intention to use epidural analgesia among pregnant women attending antenatal clinic.
DISCUSSION
This study assessed perception, attitude and identified factors predicting the intention to use EA among women attending antenatal clinic in a Nigerian teaching hospital. One of the interesting findings from this study is the desire to use EA by a large number of the respondents. More than two-thirds (72%) of the respondents expressed a desire to use epidural analgesia during the next delivery, while 74% would recommend EA to their friends and relatives. Previous studies by Iliyasu et al. (2012; Onyekwulu et al., (2017) reported that a similar proportion proportion of respondents expressed a desire to use EA. The level of education of the respondents, majority of whom were graduates might play some positive roles in this regard.
Factors predicting the intention to use EA by the respondents include religion, perception of EA, and desire for pain control positively predicts the desire to use EA while pain from needle/procedure negatively predict the intention to use analgesia among participants. On the aggregate, majority of the respondents in this study reported positive perceptions of EA. This could be due to high literacy level among the respondents. Furthermore, since the study was conducted in a tertiary hospital setting, most of the patients are usually well-exposed to modern health technologies. This was however contrary to the findings by previous scholars (Okeke et al., 2005; Barakzai et al., 2010) who opined that there is a common belief among Africans usually backed by religious views that labour pain is a course placed on womanhood which must be experienced by all women could be the major reason for these findings.
The present study revealed that desire to control pain was the major reason why the respondents will accept EA. Van denBussche et al. (2006) predicted that those who catastrophize about pain would be eager to avoid pain and thus would decide to use EA. They reported positive relationship between pain catastrophizing and intention to use EA. Encouragement by a health worker was also indicated as factor that could make them to choose EA.
Similar view was reported by Harkins et al. (2010). Further analysis revealed that ethnicity and age of the respondents have significant association with the attitude of the respondents. Respondents who were of Yoruba and Igbo descents were significantly more likely to show negative attitudes compared with those who were Hausa or other tribe. In a previous study by Hakins et al. (2010) and Iliyasu et al. (2012), ethnicity was one of the factors associated with use of EA. Similarly, Iliyasu et al. (2012) reported that other socio-demographic variables such education, religion, gravidity, and parity were not statistically significant with use of EA. These variables were not significant in this study.
Although, women in the current study largely reported positive perception regarding EA, their attitude toward the intervention was largely negative (86%). Majority disagreed that they desired pain-free childbirth (62%), and that frequent use of EA shows that it does not have adverse effects (56%). Moreover, most of the respondents (42%) were at quandary about being unable to bear-down during labour with EA. There is lack of clarity on the intention of the respondents as varying proportions of women reported different levels of agreement, disagreement or uncertainty about using EA in their future labour were almost the same. This uncertain attitude affected the women’s decision toward using EA. Previous researches provided similar results (Minhas et al., 2005; Naithani et al., 2011; Raynes-Greenow et al., 2007; Oladokun et al., 2008). Although positive perception is expected to yield positive attitude, this was not the case in this study as majority of the participants had negative attitude toward the use of EA during labour. This could be attributed to prevailing sociocultural opinions regarding EA and the common belief that women must experience labour pain as part of labour process among the study participants in the study setting; a view which was not examined by this study.
In this study, nurses and midwives constitute the source of information to the majority of the pregnant women who were aware of epidural analgesia. This was followed by those who got informed through doctors. Ekweani and Avidime (2016) noted that the majority of the clients who knew about pain relief in labour acquired their knowledge through healthcare workers (56.1%). The finding is slightly different from that of Onyekwulu et al. (2017) in which doctors (44.7%) followed by nurses (30.9%) were major sources of information about EA. Ezeonu et al. (2017) equally reported doctors (79.30%), nurses (55.20%), and internet (41.40%) as the main source of information in a study at Eastern Nigeria.
Nurses being central to the provision of maternal care, play major roles in informing parturient about what to expect during labour; hence, these findings. As with previous studies, only a few respondents gained knowledge from media, friends/relatives and other sources.
This observation is similar to previous studies by Onyekwulu et al. (2017) and Mugambe et al., 2007). However, literature has also shown that friends, relatives information leaflets and internet could also be a major source of information (Mung’ayi et al., 2008; Barakzai et al., 2010; Ezeonu et al., 2017). On the contrary, Iliyasu et al. (2012) reported that friends, books, health worker and the internet were the sources of information on EA among respondents in a study conducted in Northern Nigeria.
Implication of the study
Nurses remain pivotal to health educating the clients on the choice of various treatment modalities available to make labour pleasurable. Hence, they have more roles to play in changing the attitudes of the pregnant women to adopting EA in the presence of prevalent negative attitude among the study population. Despite the prevalent negative attitude to EA, the fact still remains that childbirth is a major life event, and women have the right to choose between experiencing natural birth process for the culturally inclined or 'painless childbirth' for the modern woman. This can only be assured when nurses advocate for women to be involved in the decision-making process regarding all aspects of childbirth, including options for pain management. Strategies for such reforms should include a need assessment among stakeholders; provision of information, education and communication for parturient while dispelling rumours; and provision of a wide range of choices of methods of obstetric analgesia in this and similar settings.
CONCLUSION
This study concluded women in this setting have a great desire to use EA for child birth. Factors including perception, religion, and desire for pain control can predict women who will use EA. Efforts should be intensity to improve on the positive perceptions of the respondents and this will ultimately result in prompt presentation and intervention with positive birth outcomes.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Ampofo EA, Caine V (2015). A narrative inquiry into women's perception and experience of labour pain: A study in the western region of ghana. International Journal of Africa Nursing Sciences, 3:86-93. |
|
|
Antonakou A, Papoutsis D (2016). The effect of epidural analgesia on the delivery outcome of induced labour: a retrospective case series. Obstetrics and gynaecology international, vol. 2016, 5 pages, |
|
|
Aziato L, Ohene LA, Dedey F, Clegg-lamptey JN (2016). I was in real pain surgical nurses' personal pain experiences in Ghana. International Journal of Caring Sciences 9(1):90-98. |
|
|
Aziato L, Acheampong AK, Umoar KL (2017). Labour pain experiences and perceptions: a qualitative study among post-partum women in Ghana. BMC Pregnancy and Childbirth, 17(1):73. doi: HYPERLINK |
|
|
Barakzai A, Haider G, Yousef F, Haider A, Muhammad N (2010). Awareness of women regarding analgesia during labor. Journal of Ayub Medical College of Abbottabad 22(1):73-75. |
|
|
Cambic CR, Wong CA (2010). Labour Analgesia and Obstetric outcome. British Journal of Anaesthesia 105((S1)):i50-i60. |
|
|
Ekweani JC, Avidime S (2016). The awareness and desirability of pain relief in labour among pregnant women in Zaria. Port Harcourt Medical Journal 10(3):115. |
|
|
Ezeonu PO, Anozie OB, Onu FA, Esike CU, Mamah JE, Lawani LU, Anozie RO (2017). Perceptions and practice of epidural analgesia among women attending antenatal clinic in FETHA. International Journal of Women's Health 9:905-911. |
|
|
Fawaz M, Malas S (2018). Lebanese women'sawareness and attitude towardepidural anesthesia during labor. Datain Brief 19:530-534. |
|
|
Garg N, Vanitha VG (2019). A Randomized Controlled Trial of Intravenous Paracetamol and Intravenous Tramadol for Labour Analgesia. Obstetrics and Gynecology Research 2:003-013. |
|
|
Harkins J, Carvalho B, Evers A, Mehta S, Riley ET (2010). Survey of the factors associated with a woman's choice to have an epidural for labour analgesia. Anaesthesiology research and practice 2010. |
|
|
Iliyasu Z, Galadanci HS, Abubakar IS, Isah H, Aliyu MH (2012). Desire for Obstetric analgesia among women in Northern Nigeria. Tropical Journal of Obstetrics and Gynaecology 29(2):53-55. |
|
|
International Association for the Study of Pain (IASP). (2011). Working together for pain relief. |
|
|
James JN, Prakash KS, Ponniah M (2012). Awareness and attitudes towards labour pain and labour pain relief of urban women attending a private antenatal clinic in Chennai, India. Indian Journal of Anaesthesia 56:195-198. |
|
|
Kuti O, Faponle AF, Adeyemi AB, Owolabi AT (2008). Pain Relief in labour: A randomized controlled trial comparing pentazocine with Tramadol. Nepal Journal of Obstetrics and Gynaecology 3(1):14-18. |
|
|
Minhas M, Kamal R, Afshan G, Raheel H (2005). Knowledge, Attitude and Practice of Parturients Regarding Epidural Analgesia for Labour in a University Hospital in Karachi. Journal of Pakistan Medical Association 55:63-66. |
|
|
Mohamed HF, Alqahtani A, Almobaya N, Aldosary M, Alnajay H (2013). Women's awareness and attitude toward epidural analgesia. Journal of Biology, Agriculture and Healthcare 3(6):46-52. |
|
|
Mugambe J, Nel M, Hiemstra L, Steinberg WJ (2007). Knowledge of and attitude toward pain relief during labor of women attending the antenatal clinic of Cecilia Makiwance Hospital, South Africa. South Africa Family Practice 49(4):16-16d. |
|
|
Naithani U, Bharwal P, Chauhan SS, Kumar D, Gupta S (2011). Knowledge, attitude and acceptance of antenatal women toward labour analgesia and caesarean section in a medical college hospital in India. Journal of Obstetric Anaesthesia and Critical Care 1(1):13. |
|
|
Obuna J, Umeora OU (2014). Perception of labor pain and utilization of obstetric analgesia by Igbo women of Southeast Nigeria. Journal of Obstetric Anaesthesia and Critical Care 4(1):18-22. |
|
|
Okeke CI, Merah NA, Cole SU, Osibogun A (2005). Knowledge and perception of obstetric analgesia among prospective parturients at Lagos University Teaching Hospital. Nigerian Postgraduate Medical Journal 12(4):258-261. |
|
|
Okojie NQ, Isah EC (2014). Perception of epidural analgesia for labour among pregnant women in a nigerian tertiary hospital setting. Journal of the West African College of Surgeons 4(4):142-161. |
|
|
Oladokun A, Eyelade O, Morhason-Bello I, Fadare O, Akinyemi J, Adedokun B (2008). Awareness and desirability of labour epidural analgesia: A survey of Nigerian women. International Journal of Obstetric Anesthesia 18(1):38-42. |
|
|
Olateju S, Adetoye A, Ijarotimi T, Olowookere S (2017). Effect of video demonstration on choice of epidural labour analgesia in a Nigerian tertiary hospital. Cochrane South Africa, South African Medical Research 10(1):26. |
|
|
Onyekwulu FA, Ugwu IC, Aniwada EC, Okeke TC (2017). Awareness and Perception of Epidural Labour Analgesia Amongst Parturient in South Eastern Nigeria. Clinical Medicine Research 6(3):116-120. |
|
|
Rachmawati I (2012). Maternal reflection on labour pain management and influencing factors. British Journal of Midwifery 20(4):263-270. |
|
|
Raynes-Greenow CH, Roberts CL, McCaffery K, Clarke J (2007). Knowledge and decision-making for labour analgesia of Australian primiparous women. Midwifery 23(2):139-145. |
|
|
Robert D, Vincent JR, David H (2012). Epidural analgesia during labour. |
|
|
Shareena T, Mahmood SF, Padmanabha S (2015). A survey on knowledge and attitude towards labour analgesia among pregnant women attending antenatal clinic. Journal of Evolution of Medical and Dental Sciences 4(104):16909-16911. |
|
|
Shidhaye RV, Galande M, Bangal VB (2012). Awareness and attitude of Indian pregnant women towards labour analgesia. Journal Anaesthesia, Pain and Intensive Care 16(2):131-136. |
|
|
Singh AS, Masuku MB (2014). Sampling Techniques & Determination of Sample Size in Applied Statistics Research: An Overview. International Journal of Economics, Commerce and Management 2(11):1-22, |
|
|
Sun J, Yan X, Yuan A (2019). Effect of epidural analgesia in trial of labor after cesarean on maternal and neonatal outcomes in China: a multicenter, prospective cohort study. BMC Pregnancy Childbirth 19:498. |
|
|
Van den Bussche E, Crombez G, Eccleston C, Sullivan MJL (2006). Why women prefer epidural analgesia during childbirth: The role of beliefs about epidural analgesia and pain catastrophizing. European Journal of Pain11(3):275-282. |
|
|
Whitburn LY, Jones LE, Davey MA, Small R (2017). The meaning of labour pain: how the social environment and other contextual factors shape women's experiences. BMC Pregnancy and Childbirth 17(1):157. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


