Full Length Research Paper

ABSTRACT
There is a large unmet need for contraception in Ghana, despite many forms of family planning being highly available and a near universal knowledge of contraception among Ghanaian women. This study sought to qualitatively investigate reasons for low-use of contraception in Ghana. Interviews were conducted with 18 women being treated for complications resulting from unsafe abortions to ascertain their views on contraception usage. Thirty healthcare providers, in three hospitals in Kumasi, Ghana were also interviewed. Ten focus groups were held with community members to investigate how contraception is viewed in the larger community. None of the women interviewed were using contraception when they became pregnant. There were three themes for reasons for non-use: Fear of Side Effects, Poor Reception by Health Staff, and Religion. To increase the acceptability of modern contraception, interventions aimed at refuting commonly held misconceptions are sorely needed. Improving the quality of services that women receive when they access services, and ensuring that health workers are well supported to provide the highest quality care possible is highly important.
Key words: Contraception, Ghana.
INTRODUCTION
In low and middle-income countries, including Ghana, approximately 26% of maternal deaths occur among young women aged 15 to 19 (Patton et al., 2009). Many pregnancies in this age group are unplanned and unwanted resulting in high rates of induced abortion, many of which are unsafe (Evens et al., 2014). These unplanned pregnancies, and the resultant unsafe abortions, could be dramatically reduced if women were using highly effective forms of contraception (Singh et al., 2009).
It has been estimated that maternal mortality could be reduced by 25 to 30% if women had access to and used modern methods of contraception (Ahmed et al., 2012). While two-thirds of women of reproductive age in Europe use modern contraception, only 21% of women residing in sub-Saharan Africa were reported using a modern method in 2007 (United Nations (UN), 2013). Despite a consensus that reducing the unmet need for contracep-tion is imperative for countries to meet their development goals, the uptake of modern contraceptives has only slightly increased in recent decades (Alkema et al., 2013; Darroch et al., 2013).
In the most recent Ghana Demographic and Health Survey (DHS, 2008), knowledge about contraception is almost universal; 95% of those surveyed knew of at least one form of modern contraception (GSS, 2009). Ever-use is also quite high with 42.3% of women reporting ever using a modern method of contraception. This is a substantial improvement from the 1980s and early 1990s when lack of knowledge about methods of family planning was high in many parts of sub-Saharan Africa (Bongaarts and Bruce, 1995). However, current use, 13.2% for modern methods, is lower than would be ex-pected given the fertility inclinations of women and their male partners. The total fertility rate in Ghana has fallen from 4.5 to 5 births per woman in 1985 to approximately 3 per woman in 2006 (Finlay and Fox, 2013). This decline is higher than what can reasonably be explained by the contraception prevalence rate in the country, suggesting many women rely on abortion to control fertility (Blanc, 2002).
Women’s ability to plan the number and timing of the children they bear can greatly reduce the health risks associated with pregnancy. However, even with the advances in contraceptive options, significant unmet need remains. In Ghana, the unmet need for contraception, defined as being currently sexually active and not wanting to become pregnant, but not using contraception (WHO, 2011), is approximately 33.5% (Govindasamy and Boadi, 2000). Reasons for non-use of contraception are many and include poor quality of available services, limited choice of available methods, fear or experience of side-effects, and cultural or religious opposition (Creanga et al., 2011). Gender-based barriers are also a factor, as is lack of access to services, particularly for young people, the poorer segments of the population, and those who are not married (Stanback and Twum-Baah, 2001). In national-level surveys, fear of side effects is noted as the main reason for not using contraception by many women (Sedgh and Hussain, 2014). Surveys from around the world suggest the fear of side effects is more salient than other barriers, such as cost, preventing women from utilizing contraception (Diamond-Smith et al., 2012). In Ghana, according to the Ghana DHS, fear of side effects as the reason for non-use increased between 2003 and 2008 (Ghana Statistical Service, 2009). However, further analysis is not possible due to the limited nature of the data available. Studies seeking to find individual-level factors associated with contraception using such data as those available in DHS reports note the importance of qualitative work to further investigate associations (Ngome and Odimegwu, 2014).
Qualitative examination of the perceived and real barriers women face will provide a deeper understanding of reasons women face will provide a deeper understanding of reasons for non-use or low uptake of contraceptive options.Qualitative methods allow for understanding complex processes, such as those surrounding the decision to use or not use contraception (Williamson et al., 2009). The purpose of this study was to elucidate reasons for contraception non-use among women in one urban area of Ghana.
METHODOLOGY
Research design
This qualitative study was based in a social network paradigm; the idea that individuals are embedded in social networks which influence their behaviour. The French sociologist Emile Durkheim argued that human societies are similar to biological systems in that they are made up of interrelated elements and that individuals make decisions based not on their own intentions but rather on the social norms which are created by the social environments in which they are embedded (Durkheim, 1951). This paradigm argues that individuals respond to and form their own social networks; these networks in turn influence the behaviour of the individuals that make up the networks.
This study sought to understand the social and personal reasons why young women at risk of unwanted pregnancy were not willing to use contraception. Using a qualitative design, women being treated for post-abortion complications at three hospitals in the Ashanti region of Ghana, the most populous region of the country, as well as the region with the highest maternal mortality ratio, were interviewed. Healthcare providers, including nurses, midwives, and physicians who provide post-abortion and family planning care were also interviewed. Community-based focus groups were held with older women as well as men, separately. The aim of this study was to explore, describe, and contextualize how women are being treated for post-abortion complications and conceptualize the use or non-use of contraception.
Ethical approval was received by the University of Michigan Institutional Review Board (HUM00087225) and the KomfoAnokye Teaching Hospital/Kwame Nkrumah University of Science and Technology Committee on Human Research Publication and Ethics.
Participants
A convenience sample of 18 women who were being treated for post-abortion complications from a self-induced abortion were recruited from the three study hospitals during the study period (September 2013 to March 2014). Women meeting the inclusion criteria of receiving treatment for complications arising from a self-induced abortion were offered participation in the study by the nurse/midwife on duty. If the woman was interested, the research assistant was contacted by the nurse/midwife on duty and came to the hospital to interview the participant. All women were informed of the research objectives and were assured of confidentiality and anonymity. No identifying information was collected. All of the participants were informed of the voluntary nature of the research and were interviewed only after their treatment was completed and before they were discharged. They were informed that non-participation would not impact their care in any way.
Healthcare providers who treat women for post-abortion complications were also recruited as part of the research by the research assistant, who is herself a midwife. When the research was explained to the healthcare staff, as to facilitate the recruitment of women, as described earlier, the healthcare providers were invited to participate. Those who were interested in sharing their
opinions were taken through a consent process and interviewed.
A total of 30 healthcare providers at the three study hospitals participated in semi-structured interviews. Majority (n=28) of the healthcare providers were nurses or midwives. Two were physicians.
Additionally, focus groups discussions (n=8) were held in the community to further contextualize how members of the community conceptualize contraception usage. These focus groups were held with women (n=6) and men (n=2) separately and had between 6 and 10 participants each. These focus groups were held in three (3) market areas surrounding each of the hospitals. The research team (the research assistant and the PI) approached community members in their places of work in the markets to invite participation. Participants were recruited individually, and if they were interested in taking part in the groups, they were taken to a private location away from their business. Individuals were approached until a sufficient number had agreed to participate.
Data collection instruments and procedure
The data were collected by means of individual interviews and focus group discussions. The individual interviews took place in a private room near the ward where the women were being treated. Only the participant and the research assistant were in the room. The focus groups were held in market areas where participants were generally engaged in their daily work. The interview and focus group discussion guides were guided by the literature and the study aims. Open ended questions and probes were used to encourage the participants to speak freely.
Data analysis
The interviews and focus groups were recorded in the local language, Twi, in which they were conducted, and then transcribed in English by a research assistant fluent in the local language. These transcripts were reviewed by another member of the study team also fluent in both English and Twi, while listening to the recordings to ensure fidelity of the translation. Qualitative data were reviewed in Microsoft Word (Microsoft Corp., Redmond, WA). Descriptive statistical and qualitative analyses were performed. The quantitative data were analysed using Microsoft Excel. The qualitative data were analysed using inductive thematic analysis (Joffe and Yardley, 2003). The researchers undertook line-by-line coding of the transcripts, after initial high level reading of all the transcripts. As this research was inductive in nature, codes were derived from the transcripts, rather than deductively from the formative stage of the research. Recurrent issues in the texts were brought together to form these initial codes. From the initial coding, a large number of codes emerged. These codes were then reviewed together to decide which were speaking to similar topics and how they were related to one another. From this large number of initial codes, reappearing and similar codes were identified and consolidated. These higher-level codes organized the initial codes into clusters. These codes were then raised to the level of categories and the categories were grouped together with similar categories into themes. Quotes that were particularly illustrative of these themes were selected.
Rigor
The research team is made of US and Ghanaian researchers familiar with unsafe abortion and family planning in Ghana. Pilot testing was utilized to ensure any problems with the interview guide were identified, and procedures were updated to reflect this process. Including three hospitals, of various sizes, was deemed important to ensure as broad a sample as possible and to include people who choose to seek services at different facilities. Further, using different forms of data collection, namely, both individual interviews as well as focus groups, and sampling different people (women seeking services, health care providers and community members) allowed for triangulation of the findings. In order to elucidate honesty in the participants, it was stressed at the beginning of each session that participation was completely voluntary in order to include only those participants who wanted to take part. Further, for the hospital-based interviews, women were informed of the independent nature of the research assistant; she was not part of their care team, nor did she work at any of the facilities which were a part of the study.
RESULTS
Demographics
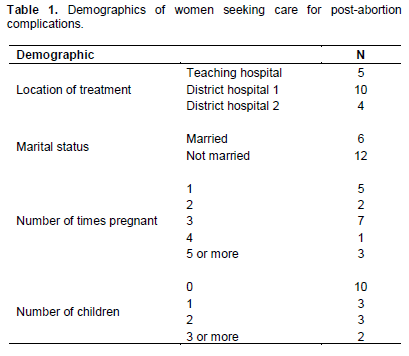
There were 18 women being treated for complications arising from self-induced abortions included in this study. They ranged in age from 13 to 39. Most were not married (6 of 18) and most had been pregnant at least once before the index pregnancy (for only 5 of the participants this was the first pregnancy). (Table 1). There were a total of 17 healthcare providers interviewed in the three hospitals.
None of the women included in this study were using contraception at the time of conception. All participants reported they knew about various contraceptive methods and most had service delivery points in their communities. The explanation women provided for not using contraception was multiple and complicated. Categories emerging from the data were grouped into three themes: Side Effects, Reception by Health Staff, and Religion. All three of these themes fit into the overarching paradigm of social network theory as many of the sources of information are not from individual experiences, but rather from what the participants have heard from others. For example, those who note a fear of side effects are often reporting what they have heard friends or family member report. Likewise, the reception by health staff is sometimes the woman herself who has had a negative experience seeking care, but more often she remembered what she has heard from others. Finally, with the theme of religion, for many individuals religion plays a large part of their social network. Customs and culture can be dictated by religion and the participants are reporting the dictates of their religion which is fundamentally social in nature.
Side effects
Participants in this study were aware and afraid of contraceptive side effects. Some of these side effects are documented as occurring, and some can be classified as misconceptions: fear of health effects which have not been linked to contraception. Women had heard from their friends of losing weight due to being on contraception,or gaining weight, or having a period all the time, or not having a period at all. One woman, a 20 year-old being treated for post-abortion complications said, “I know of a woman who was using some (family planning), but complained about persistent weight loss. She was using the implant, so she went back to the hospital to have it removed for her.” This young woman decided to use contraception from now on; “I even chose condom after the family planning education” (PAC Client-Teaching Hospital, 20 year-old). However, condom usage is a notoriously unreliable form of contraception and is dependent on consistent usage. Effective condom use is also dependent on the woman being able to insist her partner use the condom, which in this setting may be unrealistic due to social norms.
A young man who was part of a focus group, when asked about family planning, answered, “I have heard a couple of them say that if you go in for it (family planning), you might not be able to give birth again and some also say that it will give you certain infections and illness. So the alternative is that they will sit down and not try it at all.” When asked if he and his wife use family planning, he said, “As for me, I will not even use family planning methods. Once she gets pregnant, she must give birth” (Male FGD, Kumasi).
A 28 year-old being treated for post-abortion complications says about family planning, “I have heard that it helps you to space out your children in terms of child birth, I have heard a couple of women who said that if you use family planning methods, you will be prone to illness.” She had a history of using condoms, which she purchased at a drug store, before she became pregnant this time, although she was not using them at the time she became pregnant with the index pregnancy. When asked why she did not use other methods that were available at a clinic, she said, “I know you can go to the hospital and have it (family planning) done. I was afraid of side effects such as illness; that is why I avoided the hospital” (PAC Client, Teaching Hospital, age 28). After her treatment for the complications, she was educated about family planning methods and chose the implant. She was asked if she is expecting any side effects and she replied, “Please, I just want to know if really the family planning methods will not make me sick.”
An older woman who participated in a community focus group said, “As the side effects that are associated with the use of family planning methods even me who is seated here, I am very much afraid of its side effects by listening to what people say. A sister of mine came to tell me that, she has taken the injection and for about three months now, she has had her menses and on top of it, she in continually bloating and growing bigger every time. So I think your family planning medications or methods are not good. So please find something and do about it” (FGD-Women, Kumasi).
A 20 year-old being treated for post-abortion complications said, “My sister said she was growing big when she was using the method. Others say it gives you a lot of side effects. Hearing all these things about family planning, I am even afraid” (PAC Client, District Hospital 1, age 20).
A 28 year-old being treated for post-abortion complication reported, “I have heard of it (family planning) but I have also heard that if you do it, it comes to stay inside your heart. A lady told me she went for the injection and after that she lost a considerable amount of weight” (PAC-Client, District Hospital 1, age 28).
A 32 year-old being treated for post abortion complications said, “It was a friend talking about it (family planning). She said she did family planning to protect herself from getting pregnant. I can say it helped because ever since she did, she has not become pregnant yet. For me, I am afraid. Because I have heard other people say that if they do it, they get a lot of side effects like hypertension and the others” (PAC client, District Hospital 1, age 32).
One woman, a 27 year-old, who chose to use the IUD following this experience said, “What I can say is that if you are able to use family planning it will be better for you but the education on the use of family planning has not gone far so there are still a large percentage of who, doubt the efficacy of some of these methods. Some of the women are of the notion that when it is time for you to give birth, if you were on a family planning method, it becomes very difficult for you to conceive; hence, their reluctance in the use of family planning methods. Some are also afraid to use it. Some of them are also misinformed by people who have previously used some of the methods. So with all these, most women are not even encouraged to go seek family planning methods” (PAC client, Teaching Hospital, age 27).
The participants in this study were very much aware of family planning methods and where to access them, but they were reluctant to adopt these methods mainly due to stories they heard from friends and family members who had used contraception. While many of the side effects reported as part of this study are not evidence-based, the fear of them is enough to prevent women from adopting modern methods of contraception. Some of the side effect reported, such as menstrual changes, are experienced by a large number of individuals and may be bothersome enough for women to stop using the method.
Reception by health staff
Participants expressed concern about the reception they would receive from healthcare workers when accessing contraception. When asked if people in her community use family planning, one woman said, “Yes, just a few. They are usually people who are married. But for the young girls, they are afraid that when they visit the clinic, they will be shouted upon.”
In answer to the question, why do women not go to the clinic, “They are sometimes afraid of reaction from the healthcare providers” (FGD, Men, Kumasi).
One woman who was part of a community-based focus group mentioned, “My niece died about a week ago. She was pregnant, her boyfriend gave her some drug to take and after taking it, she died in the room of the boy. But according to what I heard, they said if you are a student and you go to the clinic to seek for family planning services, you are turned away because they consider you as a child” (FGD, Women, Kumasi).
One woman who was included as part of a focus group knew this about family planning: “For me I know that there are drugs you can take or apply that can protect you against unwanted pregnancies.” Although she had heard of side effects from friends as well as media sources, she did not believe them and still wanted to be using a method. When asked why she did not go to the facility in her community to accept a method of family planning, she reported, “The truth is that I am afraid of the nurses and healthcare attendants there” (FGD, Women, Kumasi).
Religion
Although not mentioned as frequently as other reasons not to use family planning, religion was noted by some of the participants. Male members of the community, as well as healthcare providers, reported religion as a reason why couples and women did not use family planning methods, although none of the women interviewed following post-abortion care mentioned religion as a barrier to contraceptive use. Male participants in the focus groups mentioned they would not allow their wives to use family planning because of their religion. One woman stated, “With us the Christians and Muslims, there are sections that say that family planning is not good. Based on that, we have some of the husbands not agreeing to it” (FGD, Women, Kumasi).
Another woman in a focus group said, “There are some churches that kick against the use of family planning” (FGD, Women, Kumasi). Another woman in a different focus group said, “There are some churches that do not approve of the use of family planning by their members. It has been tagged there as a sin. I for instance go to Pentecost Church, where the elders of the church has kicked vehemently against family planning” (FGD, Women, Kumasi).
One midwife answered a question about why more women do not accept family planning methods, “Some of them are because of the religious beliefs, it might be because of their religion” (Midwife, Teaching Hospital). Another nurse said, “Some are as a result of poor education and also sometimes religious beliefs and practices play a major role.”
DISCUSSION
International family planning efforts continue to make gains in improving women’s access to and knowledge of contraception methods in recent decades. Far more women in many low income countries know of multiple methods and are aware of where in their communities they can go to access these services. However, many women are still choosing not to use methods of highly effective contraception, and levels of use in West Africa are low (Cleland et al., 2011). None of the women inclu-ded in this study who were seeking care for complications arising from self-induced abortions were using contraception at the time the index pregnancy occurred. All of the pregnancies were unwanted and some of the women went to extreme measures to terminate the pregnancy. On the surface, it seems counterintuitive that women who did not want to become pregnant were not being proactive in preventing these pregnancies from occurring, especially since they were knowledgeable about contraception and had physical access to it. It appears that women are less fearful of abortion than they are of contraception, as has been reported elsewhere (Biney, 2011).
Worries about side effects were, by far, the most common reason women cited for not using contraception. Some of these fears, such as menstrual irregularities from the injection and the IUD, are factually-based. Others, such as an IUD migrating from the uterus to be lodged in the heart, are not. These sorts of fears of the IUD have been noted in other low-income settings (Rustagi et al., 2010) and can be hard to counteract. Most contraceptives do, in fact, have side effects, how-ever, the perception women have of the side effects they can expect are often informed by inaccurate information from friends and trusted family members and lead to disproportionate fear of contraception (Campbell et al., 2006). Although fear of the side effects of contraception is not a new phenomenon, and it has been mentioned as a barrier for women accepting modern contraception in many previous studies, family planning programs in many settings have not addressed these fears (Hindin et al., 2014). Previous work has shown that personal expe-riences and stories from social networks are more salient than medical opinions in shaping women’s perceptions of the safety of contraceptive devices including the IUD (Rustagi et al., 2010). Similar to the findings presented here, in their qualitative study in Accra, Ghana, Hindin et al. (2014) found fear of side effects, especially menstrual changes and future infertility were main reasons for non-use of contraception especially for young women.
Women seemed, for most part, to be willing to accept some form of contraception after being treated for complications arising from self-induced abortions, and many reported they did in fact accept a form of contraception. They required intensive education about the various methods of family planning available to them and were curious to learn more about contraception methods from the interviewer. Somewhat worrying, though, is that many of the women who accepted horm-onal forms of contraception from the treatment facility were not expecting any side effects. For example, one woman chose an IUD, and when asked if she was expecting any side effects, she responded, “No, please, there are no side effects associate with the use of family planning methods” (PAC Client, Teaching Hospital, age 27). IUDs often have side effects, especially menstrual changes, and being ill prepared could lead to dissatisfaction, and potentially discontinuation, if normal side effects were to arise. Many women who state they are not using contraception because of side effects are, in fact, not using contraption because of misinformation (Campbell et al., 2006). These women would benefit from appropriate and comprehensive sexual education, including education about contraception. For some women, the education they had received as part of their post-abortion care was enough to encourage them to adopt highly effective forms of contraception. Fears of future infertility are often a large deterrent to women, especially unmarried women who have not yet had children, using hormonal forms of contraception (Hindin et al., 2014). Especially in settings where a woman’s fertility is a huge part of her worth, anything that will potentially limit her ability to become pregnant when she wants to, will not be risked. In pronatalist cultures, like Ghana, it may be more acceptable to have an unplanned pregnancy than to take on the perceived risk of making yourself infertile by using hormonal contraception (Williamson et al., 2009). There were multiple mentions in the current study of participants knowing someone who, after using contraception, was not able to become pregnant when they so desired. Even if women do not currently desire to become pregnant, maintaining their fertility is hugely important to their future goals and they want to have children once their social situation determines that it is time to do so (Campbell et al., 2006).
Women formed their opinions about the side effects they were expecting often from the accounts of friends and/or family. This underscores the importance of women’s social networks in their interest in and ability to access health services. In a large-scale cross-national study using DHS data, Sedgh and Hussain (2014) found women were significantly more likely to report non-use of contraception due to concerns regarding side effects and health risks in countries having the highest levels of unmet need for contraception. In that study, Ghana had the highest level of unmet need of any country in sub-Saharan Africa at 36.1% of married women. Nearly 20% of these women cited fears of side effects as the reason they were not using contraception even though they were fecund, having sex and wishing to delay their next pregnancy by at least two years. Misconceptions about the danger of using hormonal forms of birth control are often reported to be community-wide (Campbell et al., 2006). In the current study, women and men of all ages reported hearing of side effects from friends and family members, and these were often the reason why women were not using contraception.
The large number of women in this study, who were not using contraception because of a fear of side effects, some real and some perceived, underlines the need for increased education and improved counseling for women on the modes of action of contraception, what side effects are normal and safe, and what to expect when initiating a new method of contraception. Women also need to be aware of available alternatives should side effects become untenable. An important distinction needs to be made during counseling or education sessions between actual side-effects, such as irregular bleeding, and misinformation as these can both be deterrents to use, but are different (Diamond-Smith et al., 2012). A lack of understanding of the mode of action for contraception and what side effects are not harmful is imperative for women to fully understand before they begin any method of contraception. There is some indication that even when young women do receive information about contraception, more often than not, it reinforces rather than eliminates misconception (Wood and Jewkes, 2006). Ensuring women receive correct information is therefore highly important. This study did not assess to what extent providers themselves have misinformation about contraception, but previous work has found this to be another significant barrier to women using contraception (Campbell et al., 2006).
Furthermore, these educational campaigns need to be extended beyond just the women themselves. Given the large impact of a woman’s social network on her decision to use or not use contraception, addressing miscon-ceptions on a societal level is hugely important.
Although women in Ghana have wide access to contra-ception methods in all Ghana Health Service facilities, and all recent indications suggest that knowledge of contraception is high, if healthcare providers are not willing to provide non-judgmental services especially to young women in need of services, women’s access will be hampered. Physical access is not enough to ensure women experience access. Knowledge about where they can access the services will not be sufficient to increase utilization if women are afraid of the treatment they will receive when they attempt to access services. This finding is not unique to Ghana. In their review of qualitative literature investigating limits to modern contra-ceptive use, Williamson et al. (2009) note that young women have limited access to contraceptive services in many settings not because physical inaccessibility, but because of fears of receiving a negative reception from clinic staff. In settings where culture manifests itself through providers’ biases (Campbell et al., 2006), and where social disapproval of pre-marital sex is high (Williamson et al., 2009), intensive work with family planning providers to offer nonjudgmental services, or even having special adolescent days, could increase the ability of Ghanaian women to access contraception. In previous work in Ghana, Stanback and Twum-Baah (2001) found that providers put up many barriers for women wishing to access family planning services, including marriage and minimum-age requirements, which reflected the providers’ own personal attitudes. Ensuring that all policies are medically-based rather than being based on provider bias, and ensuring these policies are put into practice, can help to ensure women receive the care they are entitled to.
This study does have a few limitations which need to be addressed. Firstly, as with most qualitative studies, this study does not comprise a representative sample and this limits the generalizability of the results. We do believe, however, that the results accurately voice the opinions and views of the women in this limited geographical area. Although saturation was reached, the relatively small sample size is also a limitation. Finally, as a cross-sectional study, it is impossible to ascertain whether the women who chose contraception after their counseling as part of their treatment for post-abortion complications continued to use this contraception and were satisfied with their method.
CONCLUSION
There have been important gains in recent decades, especially in terms of improving awareness and accessibility of contraception methods in Ghana. With almost all women knowing many forms of family planning and knowing where they can access them, community education initiatives appear to have worked well. However, to increase the acceptability of modern contraception, multi-faceted, community-wide interven-tions aimed at refuting commonly held misconceptions are sorely needed. Increasing women’s awareness of how contraception works and the different methods available to them will allow them to choose a method best suited to their needs. Improving the quality of services that young women receive when they access services, and ensuring that health workers are well supported to provide the highest quality care possible is highly important. Only through outreach and a concerted effort to improve client relations, can the health system begin to reduce the large amount of unmet need for contraception currently in Ghana.
CONFLICT OF INTEREST
Authors declare that there are no conflicts of interest.
REFERENCES
|
Ahmed S, Li Q, Liu L, Tsui AO (2012) Maternal deaths averted by contraceptive use: an analysis of 172 countries. Lancet 380(9837):111–125. Crossref |
||||
|
Alkema L, Kantorova V, Menozzi C, Biddlecom A (2013) National, regional and global rates and trends in contraceptive prevalence and unmet need for family planning between 1990 and 2015: A systematic and comprehensive analysis. Lancet 381(9878):1642-1652. Crossref |
||||
|
Biney AAE (2011). Exploring contraceptive knowledge and use among women experiencing induced abortion in the Greater Accra region, Ghana. Afr. J. Reprod. Health 15(1):37-46. Pubmed |
||||
|
Blanc AK, Grey S (2002) Greater than expected fertility decline in Ghana: Untangling a puzzle. J. Biosoc. Sci. 34:475–495. Crossref |
||||
|
Bongarts J, Bruce J (1995). The causes of unmet need for contraception and the social content of services. Stud. Fam. Plann. Crossref |
||||
|
Campbell M, Sahin-Hodoglugil NN, Potts M (2006). Barriers to fertility regulation: A review of the literature. Stud. Fam. Plann. 37: 87-98. Crossref |
||||
|
Cleland JG, Ndugwa RP, Zulu EM (2011). Family planning in sub-Saharan Africa: Progress or stagnation? Bull. World Health Organ. 89:137-143. Crossref |
||||
|
Creanga AA, Gillespie D, Karklins S, Tsui AO (2011). Low use of contraception among poor women in Africa: an equity issue. Bull. World Health Organ. 89(4):258-266. Crossref |
||||
|
Darroch JE, Singh S (2013) Trends in contraceptive need and use in developing countries in 2003, 2008, and 2012: an analysis of national surveys. Lancet 381(9879):1756-1762. Crossref |
||||
|
Diamond-Smith N, Campbell M, Madan S (2012). Misinformation and fear of side-effects of family planning. Cult. Health Sex. 14(4):421-233. Crossref |
||||
| Durkheim E (1951) Suicide: A Study in Sociology. Free Press, New York. | ||||
|
Evens E, Otieno-Masaba R, Eichleay M, McCarraher D, Hainsworth G, Lanes C, Onduso P (2014). Post-abortion care services for youth and adult clients in Kenya: A comparison of services, client satisfaction and provider attitudes. J. Biosoc. Sci. 46:1–15 Pubmed |
||||
| Finlay JE, Fox AM (2013). Reproductive health laws and fertility decline in Ghana. Int. J. Gynecol. Obstet. 123(Suppl)1:e24-8. | ||||
| Ghana Statistical Service, GSS (2009). Ghana Demographic and Health Survey Ghana Statistical Service, Ghana Health Service. Accra, Ghana. ICF Macro, Calverton, Maryland, U.S.A. | ||||
| Govindasamy P, Boadi E (2000). A Decade of Unmet Need for Contraception in Ghana: Programmatic and Policy Implications. Macro International Inc. Calverton, Maryland USA National Population Council Secretariat Accra, Ghana. | ||||
|
Hindin MJ, McGough LJ, Adanu RM (2014). Misperceptions, misinformation and myths about modern contraceptive use in Ghana. Fam. Plann. Reprod. Healthc. 40:30-35. Crossref |
||||
| Joffe H, Yardley L (2003). Content and thematic analysis. In Research Methods for Clinical and Health Psychology. Sage Publications. | ||||
|
Ngome E, Odimegmu C (2014). The social context of adolescent women's use of modern contraceptives in Zimbabwe: a multilevel analysis. Reprod. Health 11:64. Crossref |
||||
|
Patton GC, Carolyn C, Susan MS, Russell MV, Dagmar MH, Krishna B, Theo V, Jane F, Colin DM (2009). Global patterns of mortality in young people: a systematic analysis of population health data. Lancet 374(9693):881-892. Crossref |
||||
| Rustagi N, Taneja DK, Kaur R, Ingle GK (2010). Factors affecting contraception among women in a minority community in Delhi: A qualitative study. Health Popul. Perspect. Issues 33(1):10-15. | ||||
|
Sedgh G, Hussain R (2014) Reasons for contraception nonuse among women having unmet need for contraception in developing countries. Stud. Fam. Plann. 45(2):151-169. Crossref |
||||
| Singh S, Darroch JE, Ashford LS, Vlassof M (2009) Adding it up: The costs and benefits of investing in family planning and maternal and newborn health. New York and Washington DC; Guttmacher Institute and United Nations Population Fund. | ||||
|
Stanback J, Twum-Baah KA (2001). Why Do Family Planning Providers Restrict Access to Services? An Examination in Ghana. Int. Fam. Plan. Perspect. 27(1):37-41. Crossref |
||||
| World Health Organization (WHO) (2011). Unsafe abortion: global and regional estimates of incidence of unsafe abortion and associated mortality in 2008. WHO, Geneva. | ||||
| United Nations Department of Economic and Social Affairs Population Division. Population Facts No. 2013/9 Geneva, 2013. | ||||
|
Williamson LM, Parkes A, Wight D, Petticre M, Hart GJ (2009) Limits to modern contraceptive use among young women in developing countries: A systematic review of qualitative research. Reprod. Health 6(3):1-12. Crossref |
||||
|
Wood K, Jewkes R (2006). Blood blockages and scolding nurses: Barriers to adolescent contraceptive use in South Africa. Reprod. Health Matters 14(27):109-118. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


