Full Length Research Paper

ABSTRACT
The study aim to determine the factors that make women deliver at home after attending antenatal care, to determine the awareness of women on risks associated with home delivery, to determine the type of birth attendants’ available during home delivery, and to explore the opinions of women on various strategies to prevent home delivery. A non- experimental cross-sectional design was used, with a target population of 960 people and systematic random sampling technique was employed to select the sample of 132 subjects out of the target population. Participation was voluntary and the principle of informed consent was ensured. Questionnaire was used as an instrument for data collection but only 121 were retrieved and analyzed, using SPSS Version 23. The findings of the study revealed that, women deliver at home due to cost of hospital services, male attendant during delivery, distance of the health facility from their home, poor attitude of health care provider and fear of surgical procedure. Also, according to the findings, the strategies of preventing home delivery includes provision of free maternal and child services, good health care provider attitude, health education on danger associated with home delivery, and adequate man power. In conclusion, majority of respondents were aware on factors that make them deliver at home. Recommendations were made that, health services should be subsidized and made available to women of child bearing ages and health education as well as improvement of community awareness on the importance of institutional delivery should be planned and implemented.
Key words: Determinants, home-delivery, antenatal care.
INTRODUCTION
Globally, maternal health is a major health challenge and despite the government’s measures to ensure institutional delivery assisted by skilled attendants; home delivery remains high and is estimated at over 80% of all pregnant women, which is bound to be un-hygienic, unsupervised and usually late when intervention is required (WHO, 2016). The unacceptably high levels of maternal mortality are common subject in global health and development discussions. Although some countries have made remarkable progress, half of the maternal deaths in the world still take place in Sub-Saharan Africa where little or no progress has been made (Sychareun, 2013).
In most developing countries, majority of women in the reproductive age deliver at home by unskilled personnel but with regional variations (George, 2014).In every year, 3.3 million babies are stillborn and maternal deaths have also continued unabated. More than half a million women die of pregnancy related complications, with 99% of these deaths occurring in developing regions particularly Africa and Asia (WHO, 2014). The implication is that, every minute at least a woman dies from pregnancy and childbirth in these regions. Compared to other regions of the world, the lifetime risk of maternal deaths in sub Saharan Africa is 1 in 22 mothers. North Africa has 1 in 210, 1 in 62 for Oceania, 1 in 120 for Asia, and 1in 290 for Latin America and the Caribbean (WHO, 2014).
According to United Nation (UN) and World Bank (World Health Organization and World Bank, 2013) statistics, it is estimated that, 144 women die each day in Nigeria from pregnancy and related complications, making her one of the worst countries for women to deliver babies in the world. Nigeria contributes approximately 10% of the global burden of maternal and child death (National Center for Health Statistics, 2009). According to WHO and UNICEF, Nigeria recorded 58,000 maternal deaths in 2015 and the maternal mortality ratio (MMR) were 576 deaths per 100,000 live births, giving a life time risk of maternal death of 1 in 18. The situation in Northern Nigeria in particular, where maternal mortality is much higher than the national average, is a cause of concern (Nduka and Nduka, 2016).
Nigeria, on home deliveries, show variations among geopolitical zones with the South-East and South-West geopolitical zones reported to have higher percentage of deliveries attended by skilled health providers (82 and 83% respectively) than the North-West and North-East (12 and 20% respectively) of Nigeria (Nduka and Nduka, 2016). This implies that determinants of place of delivery vary from one geographic and social setting to another and their effects together with process of managing them also varies (Karkee, 2015).
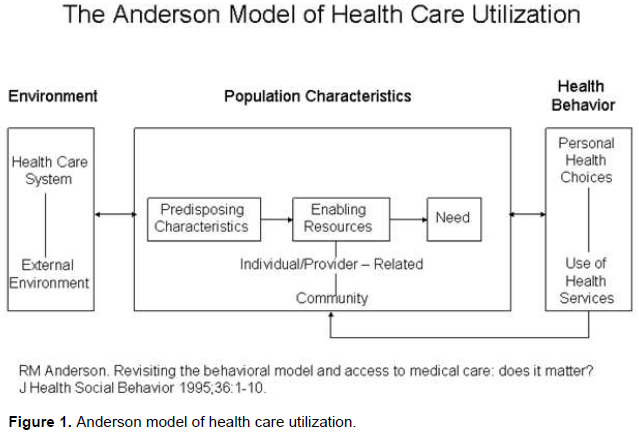
Antenatal care (ANC) attendance provides a unique opportunity to improve the health of women and infants. Utilization of ANC provides opportunities of promoting services that may include weight and blood pressure measurement etc. However, distance to health facilities, inadequate transportation, socio-cultural beliefs and the need for immediate and specialized services have hampered women’s ability to access these services in many less developed countries and northern Nigeria in particular (World Health Organization and World Bank, 2013). Andersen’s model of health care utilization best describes the reason why some Nigerian pregnant women do not utilize health services, especially pertaining institutional delivery. Around the world, there are significant unmet needs for health care, with a better understanding of why people use or do not use these services, health care organizations can seek to improve the quality of human life by bridging the detected gaps to enhance utilization.
Predisposing characteristics
These categories represent the proclivity to utilize health care services. According to Anderson, an individual is more or less likely to use health services based on demographics, position within the social structure and belief of health services benefit. An individual, who believes health services are useful for treatment, will likely utilize those services for instance age is often presented as a proxy. Older women may be told to deliver in the health facility since older age is a biological risk factor. Older women are also more influential in household decision making than younger women and adolescents in particular, making them to have power of deciding where to deliver. On the other hand, older women may belong to more traditional cohorts and thus be less likely to use modern health facilities than younger women. Young women on the other hand might have enhanced knowledge of modern healthcare services because of their schooling. This will make them place more value on modern health services and use it. Young women may be unmarried and lack social support and this may make them unable and unwilling to use maternal health services.
Enabling characteristics
These include resources found within the family and the community. Family resources comprise economic status and the location of residence. Community resources incorporate access to health care facilities and the availability of people to assist. For instance, income can affect the type of health care provider to be utilized by an individual or family. Income determines the ability of an individual to pay. If the income is low one may decide to use traditional birth attendants, be assisted by family members or even deliver unassisted, instead of going to a health facility just because of lack of funds. On the other hand one may prefer to use health care services with highly skilled personnel no matter how costly it may be if the fund is available.
Need based characteristics
These include the perception of need for services for instance if one perceives labor and delivery as a serious problem, need for advanced care arises, she will look for a skilled health care provider. Also if a mother develops an illness or is diagnosed of any abnormality during pregnancy, it might make her choose to use a skilled healthcare provider based in a functional health facility during delivery. If the mother does not have any problem nor perceive labor as a serious problem, she may not see the need to use a skilled health care provider.
Anderson’s model, in the 1970’s, was later expanded and refined to include the health care system. The health care system includes health policy, resources and organization as well as the changes in these over time. Resources comprise the volume and distribution of both labor and capital including education of health care personnel and available equipment. Organization refers to how a health care system manages its resources which ultimately influences access to and structure of health services. According to this level of revised model, how an organization distributes its resources and whether or not the organization has adequate labor volume will determine if an individual uses their health services. In addition, the updated model includes recognition that consumer satisfaction reflects health care use. The model also includes the notion that there are several health services available, and both the types of service available (that is a hospital, dentist, laboratory or pharmacy) and the purpose of the health care service (that is primary or secondary) will determine the type of service utilized. Thus, according to the revised model, whether or not a specific healthcare service is utilized and the frequency a service is utilized will have different determinants based on characteristics of the population and the health services (Henry and Dahiru, 2010).During the 1980’s and 1990’s, Anderson’s model was again revised to form three components with a linear relationship:
(i) Primary determinants
(ii) Health behaviors
(iii) Health outcomes
Primary determinants
These are noted as the direct cause of health behavior. These determinants include characteristics of the population (Demographics), Health care system (policy, resources and organization), and external environment (political, physical and economic influence on utilization).
Health behavior
The model explains that health behaviors are the direct cause of health outcomes. Health behaviors include; personal health characteristics, use of health services.
Health outcomes
Use of health services determine health outcome, which include the following:
(i) Perceived health status: If a client use health services, she will be able to evaluate herself from past experiences or from knowledge gained through health education given at the health facilities. This will make client use health services promptly to avoid complications. For instance, a mother who attends ANC will be educated on danger signs of pregnancy and this will make her seek help early enough to avoid further complications and death whenever she sees the sign of complication; because she will perceive the complication as a danger to her health and that of her baby.
(ii) Evaluated health status: When one uses health services she will be able to benefit from evaluation of her health status by health care providers and be advised properly on what to do and the best place for her delivery. If any complication is detected, she will be informed earlier to enable her choose the appropriate healthcare provider during delivery.
(iii) Consumer satisfaction: Consumer satisfaction is very important for choice of health care provider for instance convenience of using the services, quality of the services provided, availability of the needed service, price or cost of the service, provider characteristics attitude, skills, proficiency etc (Figure 1).
Locally, nearly half of the mothers booked for antenatal care, that ought to have institutional delivery, give birth at home. Nationally, home delivery accounts for majority, while few of the childbirth were attended by the skilled provider in the various health facilities. Therefore, an effort to determine the factors that influence women to deliver at home after attending antenatal care and to reduce the maternal and neonatal mortality rate through delivery in a health facility under skilled personnel, and utilizing antenatal care is the basis of this research. The main objective of this study is to find out the determinants of home delivery following antenatal care in General Hospital Ikara, Ikara Local Government Area, Kaduna State. Therefore, this research aim to answer the following questions: What are the factors that make women deliver at home after attending antenatal care? What are the socioeconomic profiles of women who deliver at home? Who attend to them during home delivery?
METHODOLOGY
A non-experimental cross-sectional design was used to find out the determinants of home delivery following antenatal care. This design was chosen because it is considered appropriate for this study and it involves a single time examination of a cross-section of the research population and allows the researcher to look once at numerous things under investigation.
This study was conducted at the antenatal care unit in General Hospital Ikara, Ikara Local Government Area, Kaduna State. The local government was created in 1976 and located in the northern part of Kaduna state under Zazzau emirate. The hospital is located in Jampalan ward, 1 km from Ikara town where the local government headquarter is located. It was officially commissioned on 20th, May 1983 by his Excellency, the then Governor of Kaduna State, Alhaji Abba Musa Rimi. The hospital serves the inhabitants of Ikara local government, and surrounding local governments like Makarfi, Kubau, and Soba local government of Kaduna state and Tudun -Wada local government of Kano state. The hospital has 56 bed capacities, with an average monthly Patients’ turnover of 2,850. Averagely, about 960 clients attend the facility for antenatal care each month. The hospital has staff strength of about 101, including Nurses, Midwives, Doctors, others health workers and administrative staff. The target population comprised all pregnant women who at least delivered at home and had attended the antenatal clinic at least twice at the General Hospital Ikara during the period of study. A total number of 960 as average monthly clinic attendance from the ANC register were used for this study. The Sample size for this study was calculated using a Daniel sample size formula from Jamila (2015) as stated below:
Where:
n= The required minimum sample
e = Margin of error at 5% (standard value of 0.05). Margin of error refer to the maximum expected difference between the true population parameter and a sample estimate of that parameter.
P= Estimated proportion of home delivery = 9.5% (0.095) (Nduka and Nduka, 2014).
z= Confidence level at 95% (standard value of 1.96). A confidence level refers to percentage of all possible samples that can be expected to include the true population parameter.
Calculation
N= Z2 p (1-p) /e2
n =1.962× 0.095 × (1-0.095) / 0.052
n = 3.8416 × 0.095 × 0.905/ 0.0025
n =3.1464/0.0025
n =132.1. Approximately = 132.
A sample of 132 subjects was selected through systematic random sampling technique from the average monthly clinic attendance of 960. The sampling interval is calculated by dividing the population size by the desired sample size (that is, 960/132 = 7.2 approximately 7).Since the sampling interval is 7, then every 7th term (7,14, 21, and 28 continuously) was selected from the average monthly ANC registered until the required sample size was met.
Inclusion criteria
(i) Pregnant woman who at least deliver once and she is attending ANC at General Hospital Ikara
(ii) Pregnant woman who attended the antenatal clinic at least twice
(iii) Pregnant woman who is willing to participate.
Exclusion criteria
(i) Pregnant woman who came to clinic for booking for the first time
(ii) Pregnant staff of the facility was excluded from the study to avoid bias in favor of their facility.
(iii) Pregnant women who declined to participate in the study.
(iv) Pregnant women who were too sick to participate in the study
A self-administered questionnaire was used to collect data, the questionnaire consisted of five sections that elicited the socio-demographic characteristics of the respondents, and factors that make women to deliver at home after attending antenatal care in the health facility, risk associated with home delivery, birth attendants used during home delivery and strategies for preventing home delivery.
Validity of instrument
The questionnaire was submitted to the researcher expert in the department of maternal and child health and two other experts in the field for content and face validity. The items were scrutinized and modifications were made. All their inputs were used to effect corrections in the final copy of the questionnaire.
Reliability of instrument
The questionnaire was used for pilot study in a smaller but similar population to test for Clarity and reliability. Five copies of the questionnaire were administered to 5 pregnant women attending ANC in another facility which was similar to the sample studied. Split half method was used and Pearson’s Product moment correlation statistics was applied and a correlation coefficient of 0.89 was obtained which was considered appropriate for use in the study.
Ethical consideration
Permission was obtained from the hospital management after explaining the purpose of the study to them and a summary of the research proposal was submitted to the ethical committee of Kaduna State Hospital Management Board and approval was given for the data collection. Respondents’ consent was also obtained and the need for the study explained to them to gain their co-operation, confidentiality and anonymity of information were guaranteed and respondents were not forced to participate in the study and they were permitted to withdraw at any stage of the study.
Methods of data collection
Questionnaires were distributed by the researcher together with research assistant to the participants who met the inclusion criteria and they were allowed to fill it. It was interpreted and filled for to non-literate participants who did not have formal education, which was then collected back. Confidentiality was guaranteed by storing data in a place where only the researcher can access. Participation by the participants was voluntary and details of the objectives of the study were explained to the participants. Data collection lasted for five days.
Data analysis
The data obtained from the study were coded and analyzed using Statistical Package for Social Sciences (SPSS) version 23. Data were checked before being subjected to analysis. The data were computed using descriptive statistical tools of frequencies, percentages and mean.
DATA PRESENTATION
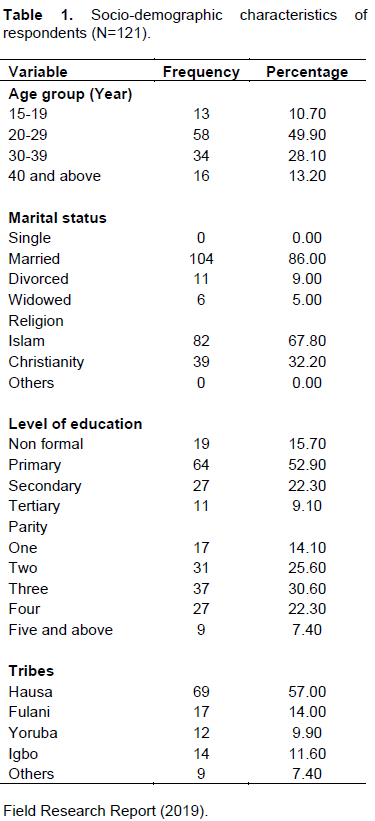
Table 1 shows the demographic characteristics of the respondents. Out of the 121 respondents that returned their questionnaires, 13(10.7%) of them were 15-19years, 58 (49.9%) were 20-29years, 34 (28.1%) were 30-39years, while 16 (13.2%) of them were 40years and above. Their marital status showed that 0 (0.0%) of the respondents were single, 104 (86.0%) were married, 11(9.0%) were divorced, while 6(5.0%) of them were widowed. For religion, they were majorly Muslims 82 (67.8%), while 39(32.2) were Christians. The respondents’ level of education showed that 19 (15.7%) had no formal education, 64 (52.9%) had primary education, 27 (22.3%) had secondary education, while 11(9.1%) of them had tertiary education. The parity of the respondents showed that 17(14.1%) had delivered once, 31 (25.6%) had delivered twice, 37(30.6%) of them thrice, 27 (22.3%) four times, while 9 (7.4%) had delivered five times and above. Their tribes showed that, 69 (57.0%) of the respondents were Hausa, 17 (14.0%) were Fulani, 12 (9.9%) Yoruba, 14 (11.6%) Igbo, while the remaining 9 (7.4%) of them were other tribes. Table 2 shows the responses of respondents on the criteria for social economic factors that make women to deliver at home.
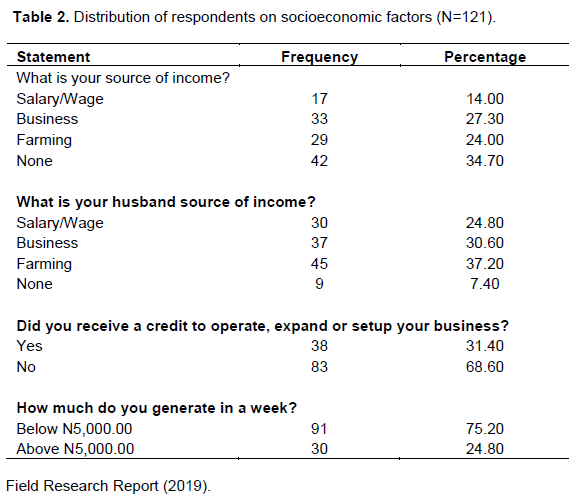
In the questionnaire the women were asked the sources of their income. Seventeen respondents (14.0%) said Salary/Wage; 33 respondents (27.3%), Business; 29 (24.0%), Farming; while 42 (34.7%) had none. From Table 2, 42 indicates that those with none are high, with 34.7%; showing that majority do not have a source of income. Asking them of their husband sources of income, the women responded in this manner: Salary/Wage, 30 respondents (24.8%); Business, 37 (30.6%); Farming, 45 (37.2%); while none had a total number of 9 respondents (7.4%). From the table, the source of these women’s husband income is farming.
For the question, did you receive a credit to operate, expand or setup your business? Yes had 38 respondents (31.4%), while No had 83 respondents (68.6%).This table also indicates that these women have minimum support from organizations or their local government. The response on question on how much income they generate in a week, those who generate below N,5000.00 had a respondent of 91 (75.2%) while those that can generate above N5,000.00 had a respondent of 30 (24.8%). Those who can generate below N5,000.00 are more, while those that can generate above N5,000.00 are few. This indicates that these women need support from their husbands and the local government to provide them with jobs.
Table 3 shows the responses on factors that make women deliver at home. The result shows that, 73 (60.3%) of the respondents were aware while 48 (39.7%) them were not aware of the factors. The respondents’ reason of home delivery are: 33 (27.3%) prefer to deliver at home because birth attendants live near them, 42 (34.7%) prefer to deliver at home because of low cost of services; 29 (24.0%) of them prefer to deliver at home because the service is safer; while 17 (14%) prefer to deliver at home because the attendants possess spiritual power. The respondents’ reasons of not wanting to deliver in the hospital, shows that 24 (19.8%) of respondents do not want male attendants during delivery, 33 (27.3%) of is because of the distance to facilities from their home, 45 (37.2%) of the respondents is due to poor attitude of health care providers, while 19 (15.7%) of the respondents are afraid of surgical procedures. Effectiveness of home delivery showed that, 32 (26.4%) of the respondents perceive home delivery as very effective, 40 (33.1%) of them perceive it as effective, 24 (19.8%) of them perceive it as fair, while 25 (20.7%) of them perceive it as ineffective.
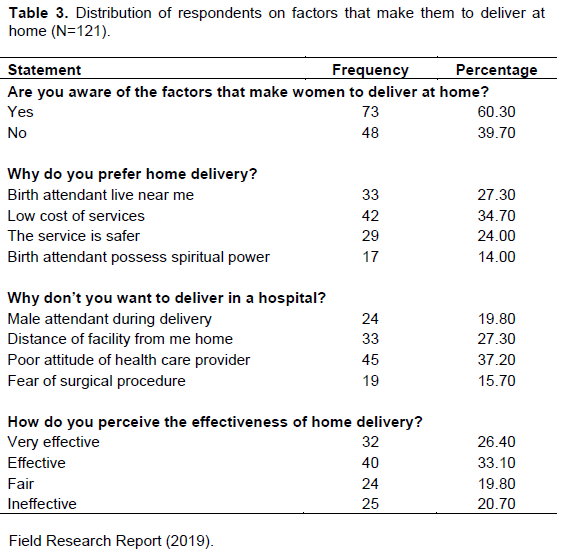
Table 4 shows the responses of respondents on their awareness on risks associated with home delivery. Forty nine (40.5%) of the respondents were aware of the risks associated with home delivery, while 72 (59.5%) of them were unaware. Also, 55 (45.5%) of the respondents had experienced some risks associated with home, while 66 (54.5%) of them were inexperienced. Likewise, 47 (38.8%) of the respondents know that a woman who deliver at home may end up with Heavy bleeding, 35 (28.9%) are aware they may end up with tear; 13 (10.7%) are aware of retained placenta; and 26 (21.5%) of them know that woman who deliver at home may end up with sepsis. Furthermore, 43 (35.5%) of the respondents know that babies delivered at home may end up with Neonatal asphyxia, 27 (22.2%) of them know that babies delivered at home may end up with Neonatal tetanus, 39 (32.2%) of them know that babies delivered at home may end up with Neonatal sepsis, while 12 (9.9%) of them know that babies delivered at home may end up with Neonatal death.
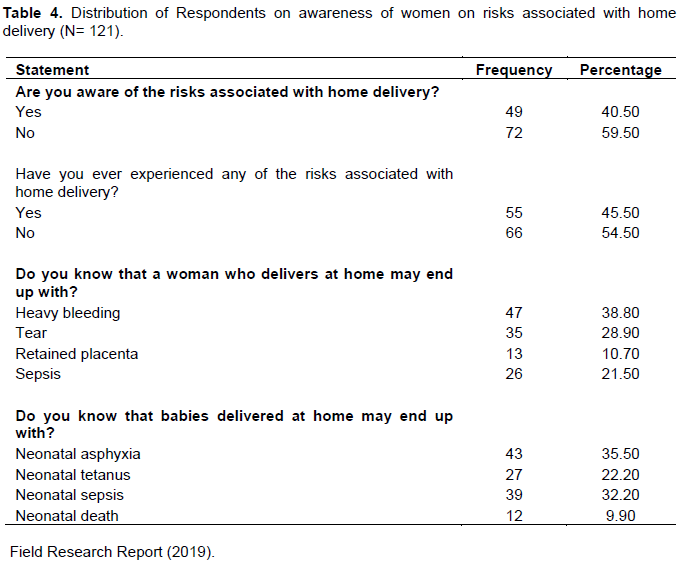
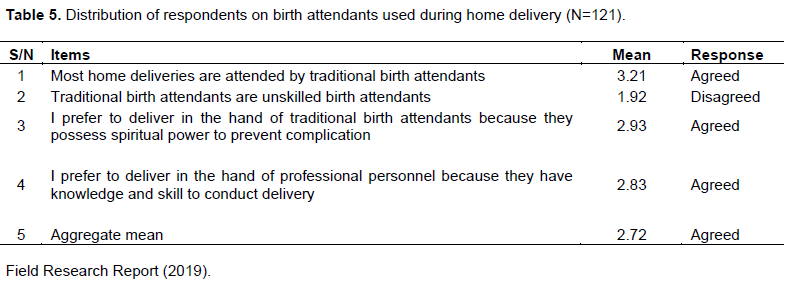
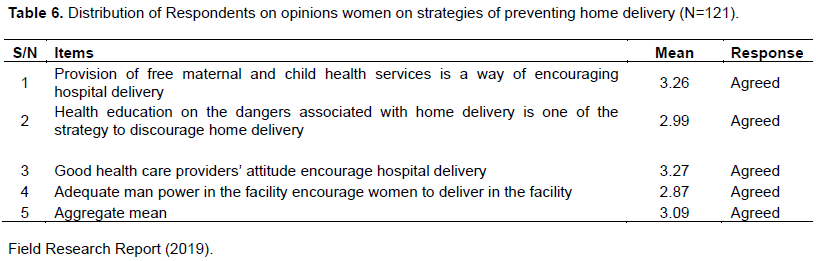
Table 5 shows the responses of respondents on birth attendants used during home delivery, and the respondents agreed with statement in items of 1, 3 and 4 but disagreed with the statement of item 2. Table 6 shows the responses of respondents on their opinions on strategies of preventing home delivery, and the respondents agreed with the statement in items 1, 2, 3 and 4.
DISCUSSION
Socio economic factors that make women to deliver at home
The findings on the sources of income for women shows that a majority, 34.7%, do not have a source of income; 27.3% are engaged in small scale business with little source of income; 24.0% are farmers; and 14.5% of these women work to receive salary/wages. Their responses on their husband sources of income show that, 37.2% of the men engage in farm activities, 30.6% engage in business, 24.8% earn salary/wages, while 7.4% do not have a source of income. For those who received credit that support operation to expand or setup a business to generate income, 68.6% did not receive while 31.4% did. Those who generate below N5,000.00 are high, while those that generate above N5,000.00 are few; indicating that these women needs support from their husbands and the local government to empower them with jobs. This finding is consistent with that of Yaya (Izugbara and Duru, 2009) on socioeconomic factors associated with choice of delivery place among mothers which found that 60.2% deliver at home due to low socioeconomic status, while 39.8% deliver in the hospital.
Factors that make women to deliver at home
The results shows that, majority of the respondents (60.3%) were aware of the factors that make them deliver at home, while the remaining (39.7%) are unaware. Also majority of the respondents (34.7%) prefer to deliver at home because of low cost of services compared to hospital services, 27.3% prefer to deliver at home since birth attendants live near them, 24.0% of them prefer home delivery because the service is safer, while the remaining 14% prefer to deliver at home because the home attendants possess spiritual power. Also, majority of respondents (37.2%) do not want to deliver in a hospital because of poor attitude of health care provider, 27.3% of them do not want to deliver in a hospital because of the distance to facilities from their home, and 19.8% of them do not want to deliver in a hospital because of male attendants during delivery, while the remaining 15.7% do not want to deliver in a hospital because of fear of surgical procedure.
The findings is consistent with that of Olufunke and Akinlujoye (2012) and Adebayo et al. (2013), who reported that the reasons for home delivery are because the services is cheaper, more culturally acceptable, closer to the homes of clients than hospital services, and the attendants have good attitude and provide more compassionate care than orthodox health workers. Also, majority of the respondents (33.1%) deliver at home because they perceive home delivery as effective, while 26.4% of them perceive home delivery as very effective.
Birth attendants used during home delivery
The result of analysis shows that the respondents agreed that most of the home deliveries are attended by traditional birth attendants. This finding is line with result of Henry and Dahiru (2010) and Peter (2011), which found that 86% of people that attended antenatal care deliver at home by unskilled traditional birth attendant. They also disagree that traditional birth attendants are unskilled birth attendants. This finding contradicts Izugbara and Duru (2009) and Rehban et al. (2011), who state that, there are two main categories of birth attendants used during home delivery, which include skilled birth attendant (professional health care providers) and unskilled birth attendants (traditional birth attendants). The respondents also agreed that, they prefer to deliver in the hand of traditional birth attendants because they possess spiritual power to prevent complication. The finding contradicts Adebayo et al. (2013) and Yaya et al. (2014), who stated that, TBAs cannot recognize and intervene medically, which may lead maternal death during childbirth such as obstructed labor, unsafe abortions, eclampsia, hemorrhage and infection. They also agreed that, they prefer to deliver in the hand of professional personnel because they have knowledge and skill to conduct delivery. This finding is line with World Health Organization and World Bank (2013), that said a skilled birth attendant is a health professional – such as a midwife, doctor, nurse – who has been educated and trained to proficiency in the skills needed to manage normal (uncomplicated) pregnancies, childbirth and immediate post natal period and to identify, manage or refer women and their newborns with complication.
Opinions of women on strategies of preventing home delivery
The result of analysis from Table 6 shows that the statement in item 1, 2, 3, and 4 are the strategies to prevent home delivery. The finding is in agreement with that of Peter (2011), who stated that, provision of free maternal and child health services, health education on dangers associated with home delivery, good attitude of health care provider and adequate man power in the facility are the strategies to prevent home delivery.
The findings of this research will inform healthcare providers why women prefer to deliver their babies at home, why some do not want to deliver in the facilities, and the risks associated with home delivery. This will help the nurse managers to plan services in such a way that it will provide 24 hours service availability for consumers and at a reduced cost too. Nurses or care providers in the communities should intensify their campaign on need to use health facilities. Reproductive health education should be intensified by health workers. It will help nurses / midwives in the communities to avoid those characteristics that scare consumers from the health facilities for instance unavailability, lack of respect for consumers, high cost of services and so on. Nurses who work in communities should try to establish good rapport with their clients and family to build confidence and enhance usage. Health workers should apply more empathy in their relationship with clients and there should be good communication between the provider and consumer. In addition, it will help the nurses in academic field to groom their nursing students with the attitude to respect clients’ decision and to give the utmost care needed.
Four research objectives and two were formulated. The theory which was reviewed for this study was Anderson’s model of healthcare utilization which was used for analyzing the determinants of home delivery. 132 questionnaires as an instrument for data collection were distributed to the study’s sample but only one hundred and twenty one (121) questionnaires were retrieved and valid for analysis, while the remaining eleven questionnaires were missing after the administration. The data were analyzed in frequency, percentage and mean using the SPSS Version 23. The findings of this study showed that among the factors that make women deliver at home include: cost of hospital services, male attendant during delivery, distance from the health facility, poor attitude of health care provider and fear of surgical procedure.
Limitation of the study
The study was limited only to pregnant women attending antenatal care at General Hospital Ikara, Ikara local government area due to financial constraint and limited time. These prevented the researcher from using a larger population. The study investigated determinants of home delivery following antenatal care in General Hospital Ikara, Ikara local Government area, Kaduna State.
CONCLUSION AND RECOMMENDATIONS
Home deliveries have important influence on maternal and child health wellbeing in Nigeria. The study has identified factors that make women deliver at home, awareness of women on risks associated with home delivery, birth attendants used during home delivery, and opinions of women on strategies of preventing home delivery. Some of the factors that make women deliver at home include: cost of hospital services, male attendant during delivery, distance from the health facility, poor attitude of health care provider and fear of surgical procedure. However, according to the findings of the study, the strategies to prevent home delivery includes: provision of free maternal and child services, good health care provider attitude, health education on danger associated with home delivery, and adequate man power. Therefore, without available and accessible healthcare that is less costly, all other efforts to reduce maternal mortality will be in vain. It is recommended therefore that:
(i) Since the government alone cannot provide health services and the TBAS are always used by rural women, some training should be given to the TBAS on care during delivery and need for early referral to prevent maternal morbidity and mortality.
(ii) Due to the level of poverty in the country that discourages mothers on the use of health facilities, health services should be subsidized and made available to women of child bearing age, if the MDG’S will be achieved since cost is one of the major deterrents of home delivery.
(iii) There should be improvement of women's socioeconomic position in order to promote the utilization of health services.
(iv) Health policy-makers should make sure that women's inability to pay does not barricade their access to essential maternal health services.
(v) It is true that the government has done much in terms of training of healthcare providers and provision of health facilities; the healthcare providers posted to rural health facilities should be encouraged to stay in their health facilities by being provided with the necessary amenities like security, light, water and some monetary incentives for instance rural allowance to motivate them to stay in rural areas.
(vi) They should also be monitored to avoid abandonment of facilities and their work to unskilled attendants.
(vii) Women should be given incentives in all the states for using government health facilities and skilled providers during (ANC) and delivery to encourage useage.
(viii) Education of the girl child up to secondary school level is very important to empower them on the use of the media and in understanding health messages which will make them increase use.
(ix) Programs on health education and improvement of community awareness about the importance of institutional delivery should be planned and implemented.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adebayo IO, Osakinle EO, Osakinle DC (2013).Quality assessment of the practice of focused antenatal care (FANC) in rural and urban primary health centres in Ekiti State. Open Journal of Obstetrics and Gynecology 3:319-326 |
|
|
George EB (2014). A review of socio-economical determinants of home delivery and its impact on quality of life of maternal and child. Journal of Clinical Nursing 10:15-24. |
|
|
Henry VD, Dahiru T (2010). Utilization of Non-Skilled Birth Attendants in Northern Nigeria: A Rough Terrain to the Health-Related MDGs. African Journal of Reproductive Health 14(2):37 |
|
|
Izugbara CO, Duru C.J (2009). Traditional Medicine.Department Of Political science, University of Calabar, Javaprovince, Austria.Sidney School of Public Health. |
|
|
Karkee A (2015): Determinants of facility delivery after implementation of safer mother programme in Nepal: a prospectivecohort study. BMC Pregnancy and Childbirth 13:193. |
|
|
National Center for Health Statistics: advance report of final mortality statistics (2009). Monthly Vital Statistics Report 40:11. |
|
|
Nduka I, Nduka EC (2016). Determinants of non institutional deliveries in an urban community in Nigeria. Journal of Medical Investing Practice 9:102-7. |
|
|
Olufunke CR, Akinlujoye B (2012). Why do some women still prefer traditional Birth Attendants and home delivery; qualitative study on home delivery care services in west. |
|
|
Peter S (2011). Where There Are (Few) Skilled Birth Attendants. Journal Health Population Nutrient 29:81-91 |
|
|
Rehban MG, Merkatz IR, Hill JG (2011).Caring for our future: a report by the expert panel on the content of prenatal care. A Journal Obstetrics and Gynecology 77(5):782-787. |
|
|
Sychareun G (2013). Quantification of maternal and child morbidity and mortality associated with home delivery in sub Saharan Africa. Acta Tropica 86(2-3):125-139. |
|
|
WHO (2014). Home delivery fact sheet No 115. World Health Organization. Geneva. |
|
|
WHO (2016). Maternal and Child Mortality fact sheet. World Health Organization, Geneva. |
|
|
WHO (2016). Strategies of preventing home delivery. Geneva: WHO; 2016.Second report of WHO Expert Committee. Technical Report Series 830. |
|
|
World Health Organization and World Bank (2013).The Millennium Development Goals Report on home delivery. |
|
|
Yaya AS, Alemu FM, Woldeyohannes SM (2014). institutional delivery service utilization and associated factors among mothers who gave birth in the last 12 months in Sekela district, Norh west of Ethiopia: a community based cross-sectional study. BMC Pregnancy Childbirth. 12:174. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


