Full Length Research Paper

ABSTRACT
The aim of this study was to determine the prevalence of paternal depression and the relevant factors associated with paternal depression, mainly focusing on occupational stress. The present study was focused on paternal depression during their partners’ pregnancy as the first part of longitudinal studies. The participants were fathers whose partners were in the third trimester of their pregnancies. Items from the Edinburgh Postnatal Depression Scale in Japanese (EPDS-J, cutoff point ≥13), sociodemographic details, major background factors, the marital relationship, occupational stress, and satisfaction were included in the questionnaire for the survey on postnatal depression. Responses were obtained from 494 participants through Macromill, which is a marketing research company with monitors throughout Japan. IBM SPSS® Statistics version 24.0 and EZR was used for statistical analysis, and P<0.05 was considered statistically significant. In this study, regarding the prevalence of paternal depression in Japan, 155 out of 494 fathers (31.3 and 95% CI 27.3 - 35.7%) were found to have depressive symptoms. The EPDS score can relate to paternal depressive symptoms during their partners’ pregnancy: No marriage, not living together with a partner (and child), and family bereavement. Regarding specific job stress, the items for which the odds ratio was significant were “heavy responsibility,” “it is not a suitable job for me,” “anxiety of being fired/going bankrupt,” and “distressing relationships at workplace.” As marital relationships, this study identified that the factor referring to EPDS with a significant odds ratio was “not often talk with my wife (partner).”
Key words: Paternal depression, prevalence, relevant factors, pregnancy.
INTRODUCTION
Leonard (1981) reported that there is a possibility that some mothers experience postpartum depression, unlike transient maternity blues. According to Yamashita et al. (2000), perinatal depression refers to development during pregnancy and within one month after birth, but it is clinically referred to as postpartum depression several months after delivery. Since postpartum depression can lead to suicide, it has become one of the critically important issues in the perinatal care field (Japan association of Obstetricians and Gynecologists, 2017). Although it was believed that postpartum depression could only be experienced in mothers, Rees and Lutkins (1971) reported that around 13% of fathers in the US who lived with their partners experienced postpartum depression in the two months after birth. In a study in Portugal, Areias et al. (1996) reported that 4.8% of fathers experienced postpartum depression three months after delivery by their partners, and 28.6% had experienced depression at the time of one year after birth. Bielawska-Batorowicz and Kossakowska-Petrycka (2006) reported that 27.5% of fathers in Poland had depression who had a partner with postpartum depression between three and six months after delivery. Paulson and Bazemore (2010) reported that the incidence of postpartum depression was 10.4% in fathers from pregnancy to one year after birth. They also found that the prevalence of postpartum depression can be up to 26% between the 3 and 6 months period of postpartum. A qualitative study also reported that fathers suffer from paternal depression (Hammarlund et al., 2015). These findings suggest the possibility that fathers experience depressive symptoms during their partners’ pregnancy to one year postpartum as well as mothers. According to several reports, mothers with postpartum depression have a tendency for child neglect or insecure attachment with their children due to their difficulty in focusing on parenting (Kerstis et al., 2016; Gutierrez-Galve et al., 2014; Stein et al., 2014). Additionally, Neal Davis et al. (2011) believe that inactive parenting behavior and corporal punishment of children increases if the fathers experience postpartum depression. It is not only mothers but also fathers who experience postpartum depression who can have a negative impact on parenting behaviors (Nishigori et al., 2019). Until recently, there has been little interest in fathers’ experiences of postpartum depression in Japan; therefore previous published studies have not provided sufficient findings (Takehara and Suto, 2012). Recently, the Ministry of Health, Labour and Welfare (MHLW) has encouraged fathers to take childcare leave as part of the coping for the declining birthrate (Ikumen project; MHLW, 2020).
After childbirth, the father should also provide care for the baby in Japan. According to a survey in the Tohoku area that used the Edinburgh Postpartum Depression Inventory (EPDS), Nishigori et al. (2019) reported that 11.2% of fathers had postpartum depression at one month and 12.0% at six months after their partner’s delivery in the Tohoku area. Higai et al. (2008) evaluated the mental status of fathers by the EPDS and the Center for Epidemiologic Studies Depression Scale (CES-D) at one month after delivery in nine facilities near the Kanto area, and they determined that 13.8 (in EPDS) and 18.6% (in CES-D) of fathers had experienced depressive symptoms. Nishimura and Ohashi (2010) surveyed in the Kansai area and reported that 14% of the fathers were depressed one month after birth and 13.6% of fathers had a depressive mood at four months after birth by their partners in a survey within the same prefecture (Nishimura et al., 2015). Also, there was a survey that 16.3% of fathers in Tokyo were judged to be depressed six months after the birth of their children, and it had risen to 19.3% one year after birth (Iwafuji and Muto, 2007).
These results suggest a risk of postpartum depression of about 10 to 20% in Japanese fathers during the period from one month to one year after the birth of their partners. Some reports include mental health status, child health, marital status, partner’s depression, economic status, and job description as the risk factors for postpartum depression in fathers (Nishigori et al., 2019; Nishimura et al., 2015; Iwafuji and Muto, 2007). Generally, occupational stress is cited as a reason that the number of suicides for men fathers after the onset of depression is higher than for women in Japan (Annual changes in Suicides in 2019; MHLW). To date, a study has shown that job description, working environment, and satisfaction with wages are associated with paternal depression (Higai et al., 2008), and the average working hours per day is also associated with postpartum depression for fathers (Watanabe and Asaka, 2016). It seems possible that these results are due to overlapping work stress and parenting as a specific depressive mood for men. In Japan, however, there is no nationwide survey on the risk of depression in fathers with their partners’ pregnancy to one year after delivery, and it is not clear what specific period will increase the risk for paternal depression. This will be part of a more extensive longitudinal study investigating paternal depressive symptoms from pregnancy to one year after childbirth, and we also examine if the onset of paternal depressive symptoms might be much earlier than after childbirth. Few studies have examined the relevance between paternal depression and occupational stress, which are common causes of depression in fathers and sources of troubled communication with their partners.
The aim of this study was to determine the prevalence of paternal depression and the risk factors associated with paternal depression, mainly focusing on occupational stress. The present study focused on fathers during their partners’ pregnancy as the first part of a longitudinal study.
MATERIALS AND METHODS
Study design
This was the first part of a longitudinal study. In this paper, the prevalence of depression in fathers during their partners’ pregnancies and the relevant factors was examined, mainly focusing on fathers’ occupational stress.
Measurement for paternal depression
Items from the Edinburgh Postnatal Depression Scale in Japanese (EPDS-J) were included in the questionnaire for the survey on postnatal depression. Each answer is given a score of 0 to 3. The maximum score is 30. Previous studies in fathers reported that the EPDS could be used to predict postpartum depression in fathers. The use of the cutoff point varies from 8 to 13 points, depending on the research. The cutoff score of EPDS from different studies was 8 (Nishigori et al., 2019; Nishimura et al., 2015), 10 (Da Costa et al., 2019), 11 (Dudley et al., 2001), 12 (Clavenna et al., 2017); and 13 (Pio de Almeida et al., 2011; Ballard et al., 1994; Lane et al., 1997). This study did not use other measures of depression to determine a cutoff for EPDS-J. Nevertheless, the number of completed suicides were 2.3 times more common in men than in women, although men are less depressed than women because depression increases the risk of suicide in Japan (Annual changes in suicides in 2019; MHLW), suggesting that depressive symptoms tend to be stronger in men than in women. Therefore, this study adopted the highest cutoff point of 13 or more from previous studies.
The risk factors associated with perinatal depression for fathers
Sociodemographic details and major background factors from previous studies for postpartum depression in fathers include: (1) number of children, (2) unexpected pregnancy, (3) the father’s (partner’s) mental health history, (4) family bereavements as life events, (5) child’s health status, and (6) economic status(Nishigori et al., 2019; Nishimura et al., 2015; Iwafuji and Muto, 2007). Since there are various ways of asking questions for each study, the above items for our questions was used in this study.
Several questions in the above studies used the Survey on the Current Status of Working Styles and Attitudes as a reference (National Institute for Labour Policy) that includes questions about the marital relationship (6 items), occupational stress, and satisfaction (11 items) (MHLW, 2015). This is allowed without permission for use in research purposes. The questions for the marital relationship consist of the following items: “building trust in a mutual relationship,” “mutual understanding,” “having enough time with the marital partner,” “having a lot of conversations with the marital partner,” “respect for several hobbies and activity,” “work hard at parenting and housework.” All were examined using a four-point Likert scale, ranging from “not feeling at all” to “always feeling strong.” The questions for occupational stress and satisfaction consist of the following items: “heavy responsibility,” “having no one talking with me at the workplace,” “working long hours,” “not fit for the job,” “difficulty responding to informatization, and technological innovation,” “anxiety of the company’s future,” “anxiety of being fired/going bankrupt,” “excessive emphasis on work performance,” “heavy workload,” “uncomfortable working environment,” and “distressing relationships at workplace.” All were examined using a four-point Likert scale, ranging from “not feeling at all” to “always feeling strong.”
Sample size
The number of births in Japan is currently 864,000 (Vital Statistics in 2019; MHLW) per year. Therefore, it is necessary to have at least 384 cases based on calculating the accuracy of 5% and the confidence rate of 95% of the number of births per year.
Subjects, procedures, and the exclusion criteria
The participants were fathers whose partners were in the third trimester of their pregnancies. Responses were obtained from 494 participants. All data were collected from a web-based nationwide survey through Macromill, a marketing research company with monitors throughout Japan (July 28 to August 3, 2019). They recruited only men whose partners’ pregnancy which was registered as Macromill monitor. The questionnaire was prepared by asking the Macromill monitor to explain the following: it is voluntary and not obligatory to answer the questionnaire; it is anonymous; it explains the possible burdens in this survey (it takes around 15 minutes to answer the questions), and it asks the Macromill monitor to respond to the web questionnaire in the case of approval of the purpose of this study. It also explained that the monitor was given points that can be used for online shopping by answering the questionnaire.
Regarding the exclusion criteria, foreigners living in Japan were excluded because of the possibilities of an insufficient understanding of the questions based on linguistic competences. The present study was the first part of longitudinal studies. While the questionnaires were completely anonymous, the respondents to the first questionnaire (the survey during the partners’ pregnancy) were numbered in the order that they could be linked to the results of the subsequent surveys.
Analysis methods
After descriptive statistics were calculated, the factors associated with postpartum depression were identified using multivariate analysis. The odds ratio [adjusted odds ratio (AOR) and 95% confidence interval (CI)] was calculated by using binomial logistic regression for associated factors of each EPDS cutoff point, and the Kruskal-Wallis test were used to compare EPDS scores on the items associated with depression. Spearman’s correlation coefficient was calculated between the median working hours per day and the EPDS score for fathers. IBM SPSS® Statistics version 24.0 and EZR (Kanda, 2013) was used for statistical analysis, and P<.05 was considered statistically significant.
Ethical considerations
The significance, purposes, and methods of this study were explicated to all target subjects through the Macromill web page. Additionally, it explained that refusing to participate would not affect the participants in any way. The questionnaires were answered anonymously, and the researchers could not identify any subjects so that the privacy of the responders was protected. The ethics committee approved this study of Kagawa Prefectural University of Health Sciences (approval number 274).
RESULTS
A total of 494 men whose partners were in the third trimester of pregnancy responded, including 236 (47.8%) with an expected first child and 258 (52.2%) with an expected second child. The number of participants whose partners were in the eighth month period of their pregnancy (28 to 31 weeks) was 128 (25.9%), ninth month (32 to 35 weeks) was 189 (38.3%), and tenth month (36 to 40 weeks) was 177 (35.8%).
Basic attributes and the odds ratio of EPDS of fathers
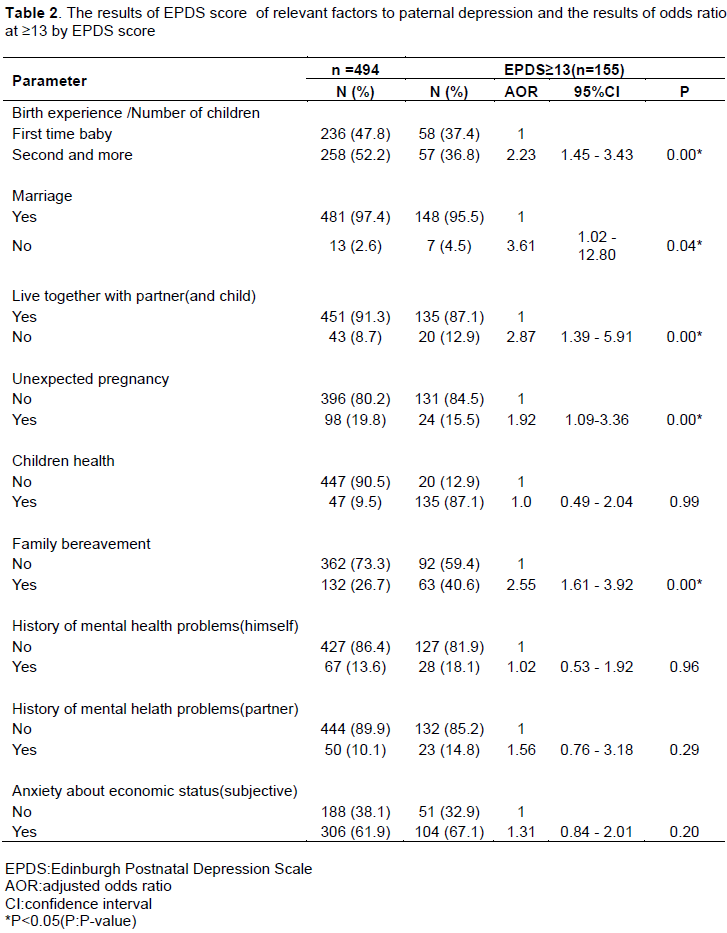
Basic attributes (area, age of fathers, family structure, and personal income), the relevant factors to paternal depression (birth experience/number of children, marriage, live together with partner and child, an unexpected pregnancy, children ’health, family bereavement, history of mental health problems (himself and partner), anxiety about economic status), the results of descriptive statistics, the median of EPDS, the Kruskal-Wallis test, and the binomial logistic analysis of EPDS scores ≥13 are shown in Tables 1 and 2.
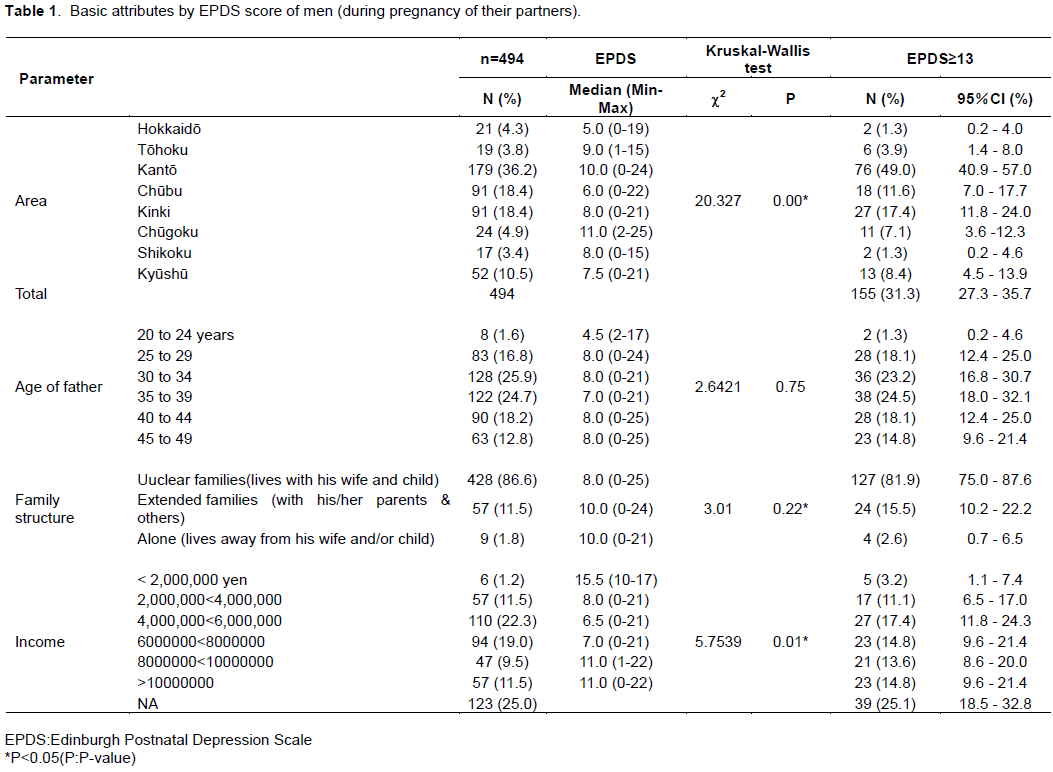
The prevalence of paternal depression identified EPDS scores ≥13: 155 out of 494 fathers (31.37%, 95% CI 27.3 - 35.7%) were found to have depressive symptoms. The Kruskal-Wallis test was conducted to examine the differences in the EPDS values for each area (P<0.05). The median of EPDS for the Chugoku area (Yamaguchi, Hiroshima, Shimane, Tottori, and Okayama prefecture) was the highest at 11.0, followed by the Kanto area (Tokyo, Saitama, Chiba, Kanagawa and Ibaragi, Tochigi, and Gunma prefecture) at 10.0. There was a significant difference in the EPDS score by paternal income in the Kruskal-Wallis test (P<.05). The median EPDS of less than 2,000,000 yen was highest at 15.5. Nonetheless, the median EPDS of more than 8 million yen was high at 11.0.
According to the binomial logistic regression analysis, EPDS scores ≥13 were significantly associated with the birth experience/number of children ≥2 (AOR 2.23, 95% CI 1.45-3.43), no marriage (AOR 3.61, 95% CI 1.02-12.80), not live together with a partner (and child) (AOR 2.87, 95% CI 1.39-5.91), unexpected pregnancy (AOR 1.92, 95% CI 1.09-3.36), and family bereavement (AOR 2.55, 95% CI 1.61-3.92) (Table 2).
The results of paternal depression and job description and occupational stress
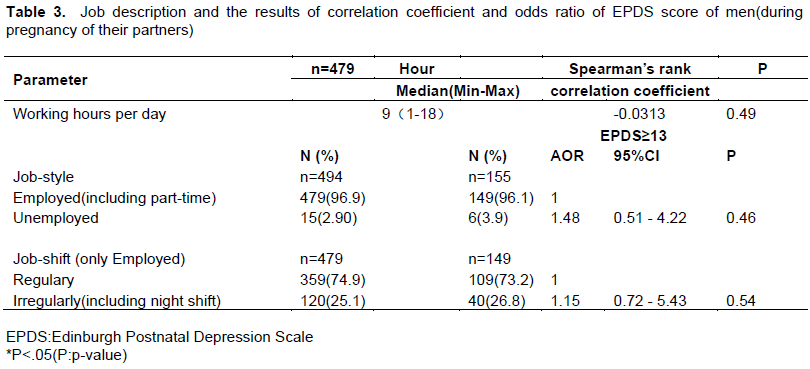
The median working hours per day was not associated with EPDS for fathers (Spearman’s correlation coefficient -0.0313, P>.05) (Table 3).
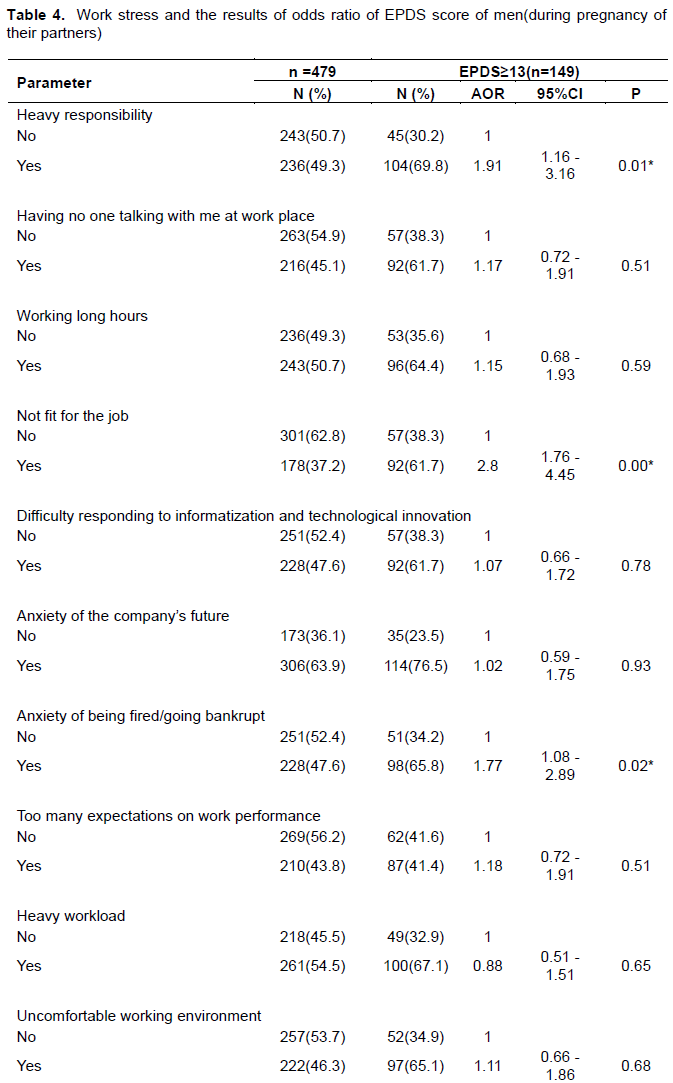
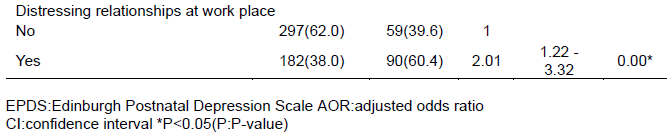
The several items of occupational stress were significantly associated with EPDS scores ≥13: heavy responsibility (AOR 1.91; 95% CI 1.16-3.16), not fit for the job (AOR 2.80; 95% CI 1.76-4.45), the anxiety of being fired/going bankrupt (AOR 1.77, 95% CI 1.08-2.89), and distressing relationships at workplace (AOR 2.01, 95% CI 1.22-3.32) (Table 4).
The Relationship with partner
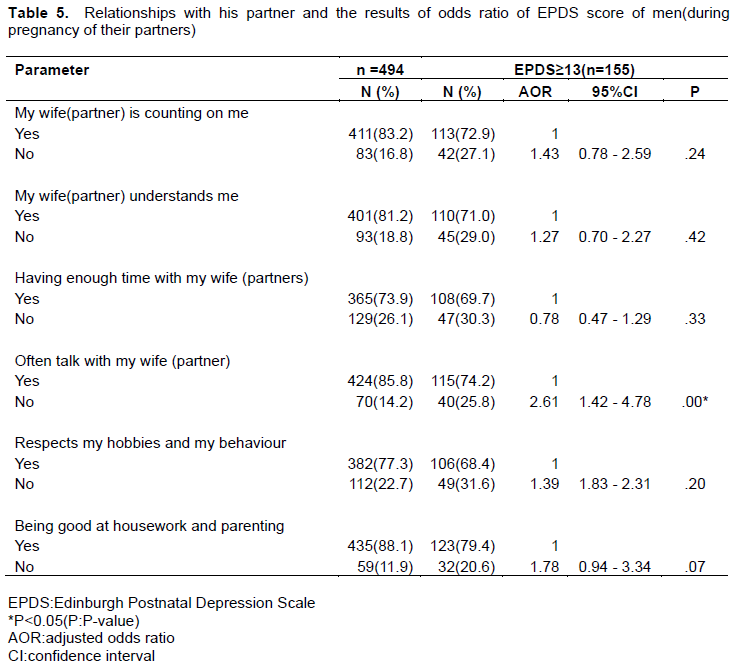
Only one of the variables concerning the relationships with partners was significantly associated with EPDS scores ≥13: not often talk with my wife (partner) (AOR 2.61, 95% CI 1.42-4.78) (Table 5).
DISCUSSION
The purpose of this study was to clarify the prevalence of depressive symptoms for men with their partners’ pregnancy and the relevant factors using EPDS-J.
The Prevalence of paternal depression during their partners’ pregnancy
In this study, regarding the prevalence of paternal depression in Japan, 155 out of 494 fathers (31.3 and 95% CI 27.3 - 35.7%) were found to have depressive symptoms (EPDS≥13). In Japan, men can experience a high rate of exacerbation in mental health problems during their partner’s pregnancy. Regarding paternal depressive symptoms, the prevalence of 31.3% obtained in the present study was higher than that of Paulson and Bazemore’s report (2010) in the third trimester, which was about 10%. A meta-analysis of the prevalence of depression in women in the third trimester of pregnancy reported 16.3% in Japan (Tokumitsu et al., 2020), but men could be more likely to be depressed such situations.
The factors associated with paternal depressive mode
There were significant differences in the comparison of the median of EPDS for each region of Japan. The highest EPDS score was in the Chugoku area. This study identified the distinct regional differences that the paternal depressive tendency has in Japan. Regarding economic status, there has been no study that compared details of income and the EPDS scores in Japan. Comparing the EPDS score by individual income, the median of EPDS scores were significantly higher at less than 2 million yen and more than 8 million yen. For fathers, the increasing EPDS may be related not only to economic anxiety but also to contributing higher incomes as depressive factors.
Additionally, the EPDS score can relate to paternal depressive symptoms during their partners’ pregnancy: no marriage (AOR 3.61, 95% CI 1.02-12.80), not living together with a partner (and child) (AOR 2.87, 95% CI 1.39-5.91), unexpected pregnancy (AOR 1.92, 95% CI 1.09-3.36) and family bereavement (AOR 2.55, 95% CI 1.61-3.92). It was found that the factors relating to the instability of life may lead to depression in the father. Previous studies were also identified as associated factors with paternal depressive symptoms (Nishigori et al., 2019; Nishimura et al., 2015; Iwafuji and Muto, 2007).
In Japan, the prevalence of postpartum depression in primiparas is higher than in multiparas in mothers (Tokumitsu et al., 2020). The reason may be that the mother’s mental health condition deteriorates due to facing the challenge of parenting; raising children for the first time. In this study, fathers had an odds ratio of 2.23 (95% CI 1.45 -3.43) for two or more children. In the case of fathers, anxiety due to first-time parenting may not be a factor associated with an increase in the EPDS. In other words, there is a possibility that mothers and fathers may have completely different roles for parenting and relationships with their children. Also, the rate of fathers taking childcare leave is limited in Japan because there is a gap between companies in the benefits of welfare and leave compensation. It is fathers who primarily earn most of the household income, so that the increased economic burden of having more children may affect their mental health and well-being.
While it was not associated with paternal depressive symptoms, Watanabe and Asaka (2016) suggested that working hours per day is associated with postpartum depression. Higai et al. (2008) pointed out that job description, working environment, and satisfaction about wages are related to paternal depression, but it was not compared to EPDS regarding occupational stress in Japan. In this study, there was a relationship between occupational stress and EPDS scores. Regarding specific job stress, the items for which the odds ratio was significant were “heavy responsibility” (AOR 1.91, 95% CI 1.16-3.16), “not fit for the job” (AOR 2.80, 95% CI 1.76-4.45), “anxiety of being fired/going bankrupt” (AOR 1.77, 95% CI 1.08-2.89), and “distressing relationships at the workplace” (AOR 2.01, 95% CI 1.22-3.32). In a situation where there can be the expectation of a new baby, the following factors can lead to a deterioration of the father’s mental health: heavy responsibilities on the job, the possibilities of economic anxiety despite being a significant source of the household income, and difficulty with human relationships in the workplace. Relationships with partners may also affect the mental health of fathers during childrearing. This study identified that the factor referring to EPDS with a significant AOR was “not often talk with my wife (partner)” (AOR 2.61, 95% CI 1.42-4.78). Good communication with partners may be related to a father’s mental well-being. Effective communication skills could be working on tolerating stress and successfully addressing psychosocial issues (Hargie, 2006). It is essential to conduct intervention studies to explore whether better communication with their partners and in the workplace helps them to maintain their psychological health.
Belsky (1984) identified that one of the factors of parenting behavior is the influence of the parents’ own experience of being raised in childhood, and these experiences can influence the formation of one’s personality. Additionally, it was pointed out that one’s personality can be interrelated with the marital relationship, employment status, and social support (Belsky, 1984). In this study, the relationship between marital relationship, employment status, and the EPDS score were examined. One of the major factors of depression in this study among men whose partners were pregnant could relate to their communication skills with their partners and the workplace. This may lead to increased depressive symptoms that overlapped occupational stress during childcare when relationships with partners are poor, depending on the personality characteristics of the men. Good relationships with their partners might also reduce the risk of paternal depression. To prevent a postpartum crisis, it is necessary to build a good relationship with a partner by having conversations between the husband and wife from the beginning of and during the pregnancy.
CONCLUSION
In this study, 31% of fathers experienced depressive symptoms during their partner’s pregnancy. The occupational stress and relationships with their partners can be factors predicting paternal depression. Today, in Japan, the average age of women at first childbirth is over 30, and the average age of their partners has also increased over the years. Postpartum depression for women has been indicated as relevant to suicide, and it should be emphasized. However, because suicides are more common among Japanese men, the risk of suicide from depression in men with partners during pregnancy should be considered. It was also found that the magnitude of occupational stress was related to depression in fathers. In Japan, as the age of parents who have children is rapidly increasing, there is a possibility of starting childrearing in their thirties and forties, and when the workload increases, this will force men to provide care for their children. It can be assumed that the age at which depression occurs coincides with the age of the parents who are raising children. It necessitates mental health support from health professionals for fathers whose partners are pregnant and the mothers.
LIMITATION
This report covers only the third trimester of pregnancy, and it does not include data on paternal depression throughout the whole pregnancy of their partners. While the EPDS was used as the scale used to measure the incidence of paternal depression in men during the pregnancy of their partners, the determination of the cutoff point for the EPDS remains ambiguous. Therefore, the EPDS and other indicators should be combined with this measurement for fathers in future research.
The prevalence rate found in this study was higher than previous studies in Japan (Nishigori et al., 2019; Nishimura et al., 2015), though, mostly when taking into account that a stringent cutoff score on the EPDS (≥13) was used. Although the EPDS has been validated for the use of fathers (Matthey et al., 2001), this scale was not developed for fathers, and the EPDS may have some ambiguous items and has a limited ability to detect anxiety and depressive symptoms in fathers. Additionally, it might not be representative of fathers in Japan because there was a biased that all participants were registered as Macromill (the marketing research company) monitors.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
This work was supported by JSPS KAKENHI Grant Number 18K10399.
REFERENCES
|
Areias ME, Kumar R, Barros H, Figueiredo E (1996).Correlates of postnatal depression in mothers and fathers. The British Journal of Psychiatry 169(1):36-41. |
|
|
Ballard CG, Davis R, Cullen PC, Mohan RN, Dean C (1994). Prevalence of postnatal psychiatric morbidity in mothers and fathers. The British Journal of Psychiatry 164(6):782-788. |
|
|
Belsky J (1984). The Determinants of Parenting: A Process Model. Child Development 55(1):83-96. |
|
|
Bielawska-Batorowicz E, Kossakowska-Petrycka K (2006).Depressive mood in men after the birth of their offspring in relation to a partner's depression, social support, fathers' personality and prenatal expectations. Journal of Reproductive and Infant Psychology 24(1):21-29. |
|
|
Clavenna A,Seletti E,Cartabio M,Didoni A,Fortinguerra F,Sciascia T,Brivio L,Malnis D, Bonati M (2017).Postnatal depression screening in a pediatric primary care setting in Italy. BMC Psycheatry 17(42). |
|
|
Gutierrez-Galve L, Stein A, Hanington L, Heron J, Ramchandani P (2014). Paternal depression in the postnatal period and child development: mediators and moderators. Pediatrics 135(2):e339-e347. |
|
|
Davis RN, Davis MM, Freed GL, Clark SJ (2011). Fathers' depression related to positive and negative parenting behaviors with 1-year-old children. Pediatrics 127(4):612-618. |
|
|
Da Costa D, Daniele C, Abrahamowicz M, Dasgupta K, Sewitch M, Lowensteyn I, Zelkowits P( 2019).A prospective study of postnatal depressive symptoms and associated risk factors in first-time fathers. Journal of Affective Disorders249:371-377. |
|
|
Dudley M.,Roy K.,Kelk N.,Bernard D(2001).Psychological correlaties of depression in fathers and mothers in the first postnatal year. Journal of Reproductive and Infant Psychology 19(3):187-202. |
|
|
Hammarlund K, Andersson E, Tenenbaum H, Sundler AJ (2015). We are also interested in how fathers feel: a qualitative exploration of child health center nurses' recognition of postnatal depression in fathers. BMC Pregnancy Childbirth 15:290. |
|
|
Hargie O (2006). The handbook of communication skills 3rd edition. Routledge. |
|
|
Higai S, Endo T,Hiejima Y, Shioe K (2008).Postnatal depression and related factors in fathers of one-month-old infants (Seigo 1-kagetsu no kodomo o motsu chichioya no sango utsu to kanren yÅin). Japanese Journal of Maternal Health 49(1):91-97. |
|
|
Iwafuji H, Muto T (2007). Casual relationship between ante-and postnatal depression and marital intimacy:from longitudinal research with new parents(Sanzen sango ni okeru fūfu no yokuutsu-sei to shinmitsu-sei no inga kankei -- dai 1-shi shussan no fūfu o taishŠto shita jūdan kenkyū kara). Japan Journal of Family Psychology 21(2):34-45. |
|
|
Japan association of Obstetricians and Gynecologists (2017). Maternal Mental Health Manual: Sango kea no kireme no nai shien ni mukete. |
|
|
Japan.Ministry of Health, Labour and Welfare (MHLW) (2020). Ikumen project. |
|
|
Japan.Ministry of Health, Labour and Welfare (2019). Vital Statistics in 2019(Reiwa gannen jinkÅ dÅtai tÅkei no nenkan suikei) |
|
|
Japan Ministry of Health, Labour and Welfare (MHLW) (2019).Annual changes in suicides in 2019 (Reiwa gannenchÅ« ni okeru jisatsu no jÅkyÅ). |
|
|
Japan Ministry of Health, Labour and Welfare (MHLW) (2015). Manual for Implementing the Stress Check System under the Industrial Safety and Health Act.( RÅdÅ anzen eisei-hÅ ni motodzuku sutoresu chekku seido jisshi manyuaru) |
|
|
Kanda Y (2013). Investigation of the freely available easy-to-use software 'EZR' for medical statistics. Bone Marrow Transplantation, 48:452-458. |
|
|
Kerstis B, Aarts C, Tillman C, Persson H, Engström G, Edlund B, Öhrvik J, Sylvén S, Skalkidou A (2016). Association between parental depressive symptoms and impaired bonding with the infant. Archives of Women's Mental Health 19(1):87-94. |
|
|
Lane A, Keville R, Morris M, Kinsella A, Turner M, Barry S (1997). Postnatal depression and elation among mothers and their partners: prevalence and predictors. The British Journal of Psychiatry 1771:550-555 |
|
|
Leonard LG (1981). Postpartum depression and mothers of infant twins. The American Journal of Maternal/Child Nursing 10(2):99-109 |
|
|
Matthey S, Barnett B, Kavanagh DJ, Howie P (2001). Validation of the Edinburgh Postnatal Depression Scale for men, and comparison of item endorsement with their partners. Journal of Affective Disorder 64(2-3):175-184. |
|
|
Neal Davis R, Davis MM, Freed GL, Clark SJ (2011). Fathers' depression Related to Positive and Negative Parenting Behaviors with 1-Year-Old Children. Pediatrics 127(4):612-618. |
|
|
Nishigori H, Obara T, Nishigori T, Metoki H, MizunoS, Ishikuro M, Sakurai K, Hamada H, Watanabe Z, Hoshiai T, Arima T, Nakai K, Kuriyama S, Yaegashi N(2019). The prevalence and risk factors for postpartum depression symptoms of fathers at one and 6 months postpartum: an adjunct study of the Japan Environment & Children's Study. The Journal of Maternal-Fetal and Neonatal Medicine 33(16):2797-2804. |
|
|
Nishimura A, Ohashi K (2010). Risk factors of paternal depression in the early postnatal period in Japan. Nursing and Health Sciences 12(2):170-176. |
|
|
Nishimura A, Fujita Y, Katsuta M,Ishihara A, Kazutomo O (2015). Paternal postnatal depression in Japan: an investigation of correlated factors including relationship with a partner. BMC Pregnancy and Childbirth15:128. |
|
|
Paulson JF, Bazemore SD (2010). Perinatal and postpartum depression in fathers and its association with maternal depression: a meta-analysis. The Journal of the American Medical Association 303(19):1961-1969. |
|
|
Pio de Almeida LS, Jansen K, Köhler CA, Pinheiro RT, da Silva RA, Bonini JS (2011). Working and short-term memories are impaired in postpartum depression. Journal of Affective Disorders 136(3):1238-1242. |
|
|
Rees WD, Lutkins, SG (1971). Parental depression before and after childbirth. Journal of the Royal College of General Practitioners 21:26-31. |
|
|
Stein A, Pearson RM, Goodman SH, Rapa E, Rahman A, McCallum M Pariante CM (2014). Effects of perinatal mental disorders on the fetus and child. Lancet 384(9956):1800-1819. |
|
|
Takehara K, Suto M (2012). Paternal Depression (Chichioya no sango utsu).The Journal of Child Health 71(3):343-349. |
|
|
Tokumitsu K, Sugawara N, Maruo K, Suzuki T, Shimoda K, Yasui-Furukori N (2020). Prevalence of perinatal depression among Japanese women: a meta-analysis Ann Gen Psychiatry 19(41). |
|
|
Watanabe M, Asaka Y (2016). Survey of depression in husbands during their wife's pregnancy (Tsuma no ninshin-ki ni okeru otto no yokuutsu no jittai to kanren yÅin) .Japanese Journal of Maternal Health 57(1):174-182. |
|
|
Yamashita H, Yoshida K, Nakano H, Tashiro N (2000). Postnatal depression in Japanese women: Detecting the early onset of postnatal depression by closely monitoring the postpartum mood. Journal of Affective Disorders 58(2):145-154. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


