Full Length Research Paper

ABSTRACT
Intimate partner violence (IPV) is a key public health and social concern among couples in countries globally. A systematic review was conducted to find out information concerning literature on the perpetration of IPV among couples infected with human immunodeficiency virus (HIV). The main objective of this study was to search for evidence of IPV among couples infected with HIV. Specifically, literature related to the types of violence perpetrated by intimate partners who were infected with HIV and literature on their experiences were reviewed. The search engines used in the review included PubMed, CINAHL, PsycINFO, and Google Scholar which focused on the perpetration of violence among HIV infected concordant or discordant couples. Four main categories of violence were identified in the scoping review, namely psychological abuse, physical abuse, sexual victimization or abuse as well as financial and other forms of abuse. Sixty-one (61) literature related to the topic were identified. Fifty-eight (58) articles were left after duplicates were removed. Title and abstract screening brought the number to 9 for full article screening. Nine (9) full-text studies were assessed out of the 58 and only 4 were included as they contained data on all the three categories of IPV: Physical IPV, sexual IPV, and psychological IPV experienced as a result of being HIV positive. Other IPV identified included financial deprivation, prevention of the partner from meeting colleagues, and verbal abuse such as shouting and scornful looks. The results of the systematic review showed limited studies on the perpetration of IPV among HIV infected couples. It is recommended that further studies be done on exploring experiences of couples who perpetrate IPV among HIV seroconcordant or serodiscordant infected couples.
Key words: Perpetrator, intimate partner violence, HIV, disclosure, factors.
INTRODUCTION
Intimate partner violence (IPV) is a public and social concern worldwide and comes in the forms of physical, emotional and sexual abuse.These forms of abuse are found in populations globally (Hembling and Andrinopoulos, 2014; Were et al., 2011). In sub-Saharan Africa, studies have reported high lifetime experience of IPV (Ajayi et al., 2019; Hembling and Andrinopoulos, 2014; Ogum et al., 2018; Adjah and Agbemafle, 2016; Tenkorang and Owusu, 2018). For example, astudy in South Africa revealed 32% of young males perpetrating forms of abuse against their partners as reported (Were et al., 2011). Another study that was conducted in Kenya showed some prevalence of physical abuse (26%) against female partners, 74% of which wasperpetrated by intimate couples (Hembling and Andrinopoulos, 2014).In their view, several plausible mechanisms could drive the relationship between IPV and engagement in HIV care such as fear of new or continued IPV lead couples to avoid disclosure of their status to partners, which in turn has a significant impact on treatment adherence.
Scarcity of literature on best ways of preventing and minimising IPV and abuse among people living with HIV (PLWHIV) in some countries in the African sub-Saharan regionis a concern (Sarnquist et al., 2014). Therefore, the need to review studies on IPV among HIV infectedseroconcordant or serodiscordantpartners to establish knowledge gaps and identify where primary research is essential. Hence, this studyexploredthe pieces of evidence of perpetration of IPV among HIV infectedseroconcordant or serodiscordantpartners.
METHODS
Purpose of the review
The review methodology was undertaken following the approach of Hilary Arksey and O’Malley (2005). Systematic reviews are important in showing evidence of literature around an area or topic that an individual shows interest in and this helps to concentrate and focus the research question and in doing so shows some findings already in the area which helps in identifying knowledge gaps ( (Hilary and O'Malley, 2005). PICO which means population, intervention, comparison and outcome is a framework used to determine the criteria for eligibility in conducting primary research (Table 1) for more information.

Search strategy
Search engines such as PubMed, CINAHL, PsycINFO and Google Scholar were employed as a means of searching for the information. These search engines were chosen as a result of recommendationsthrough discussions among the authors and that of a librarian, University of KwaZulu-Natal. The search was done from 7th January to 3rd May 2019 using the following keywords: “partner violence” “intimate partner” “violence perpetration” “HIV”. Boolean terms such as AND/OR were employed as a way of separating keywords. To get current literature about intimate partner violence in LMICs, the date of publication of included studies was limited to studies done from 2007 to 2018. The reason for limiting this study to between 2007 and 2018 was due to lack of resources.Search language was also limited to English due to lack of expertise to translate studies published in other languages. Study design restriction was however removed.
Peer-reviewed studies were included as well as grey literature which was specific to the topic to address the research questions were chosen and included in the study.
Study selection
The selection of the studyhappened in three stages. The screening of the titles was done by one screener using the eligibility criteria as a guide. The screening of the abstracts and full articles were done by two independent screeners. Any disagreements in the two screeners’ responses were resolved through discussions until a consensus was reached. Disagreements in screeners’ responses were resolved when full article screening was being done by the involvement of a third screener.
Criteria for eligibility
Criteria for Inclusion
The following criteria were used in the included studies:
1. Studies that were published in the English language
2. Published literature between January 2007 and August 2018
3. Reportsof articles that were onperpetration of IPV among HIV infected partners
4. Reports of studies on IPV
5. Studies on all reviews including systematic reviews, meta-analysis, scoping reviews, peer-reviewed journal articles, and rapid reviews
6. Study designs about all types of studies likequantitative studies, qualitative studies, cohort studies,pilot studies,randomized control trial studies, cross-sectional studies, and quasi-experimental study designs.
Criteria for exclusion
The criteria for inclusion for this study included:
1. Interventions not including any form of IPV
2. Studies that are not related to HIV infected partners and IPV and those relating to reducing the prevalence of IPV and HIV infections.
3. Articles that have reports not relating to HIV/AIDS and IPV
4. Studies not in the English language
5. Published studies before January 2007 and after August 2018
6. Published studies not relating toHIV infected adults who are in heterosexual relations.
Data extraction
Studies that were selected were thoroughly screened, read and data were extracted based on their study setting, aim/objective, bibliographic details, targeted population and study design; intervention, relevant outcomes of interest and significant outcomes were extracted. The geographical location (rural or urban), as well as the country of the study, were also relevant outcomes of interest that were also extracted.According to the World Bank Group report(2018), dataonlevels of income from countries were also obtained.
Ethical consideration
There was no need for ethical clearance as this was a literature that was reviewed.
RESULTS
The literature search identified 61 unique records as shown in Figure 1. Three (3) of the articles wereduplicates out of the 61 leaving a total of58 articles. The authors assessed 9 full-text articles for eligibility after the title and abstract assessment of the 58 articles. Out of the 9 articles, 4 were included for analysis. The studies that were included were as shown in Table 1. Out of the 9 studies,the 4 articles includeddata on all the three forms of IPV: Physical IPV, sexual IPV, and psychological IPV experienced as a result of being HIV positive. Other IPV identified included financial deprivation, prevention of the partner from meeting colleagues, and verbal abuse such as shouting and scornful looks. Of the four articles, two were conducted in India, one in South Africa and one inSouth-East Ethiopia. All the articles were within the lower-middle-income countries bracket. Most of the articles concentrated on the views of couples that had experienced violence in their relationships and were HIV positive or living with HIV. The tool for the mixed method Appraisal (MMAT) version 11 (Pace et al., 2012)was employed to assess the quality of studies that were included. The authors appraised all relevant articles in the study concerning the quality and methodology by employing the checklists for the MMAT for the outcomes of the appraisal. The incentive for the decisions taken was kept for auditing. The authors had the selected studies appraised by a second reviewer independently. A flowchart summarizing the selection process is as shown in Figure 1.

Analysis of the key findings (evidence established)
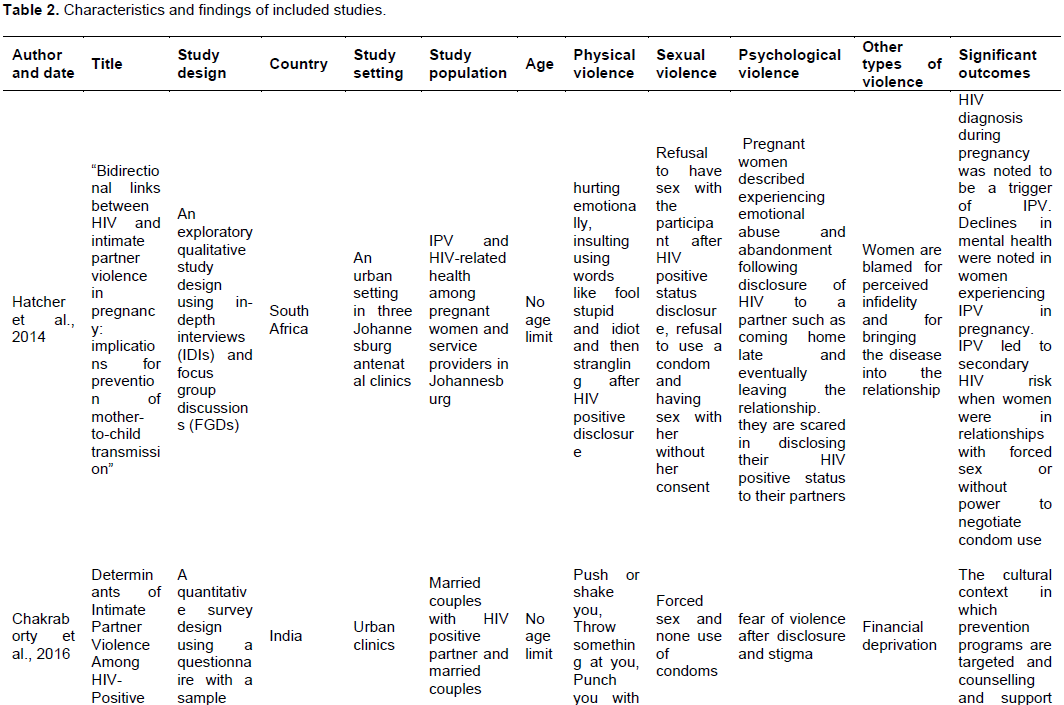
Four main categories of violence were identified in thescoping review. These were physical violence, sexual violence, psychological violence and othertypes of violence. Under each of these headings were significant outcomes as shown in Table 2.
Physical violence
The four included studies identified several forms of physical violence among couples. The physical violence found by Hatcher et al. (2014) included hurting emotionally, insulting words like a fool, stupid and idiot and then strangling after HIV
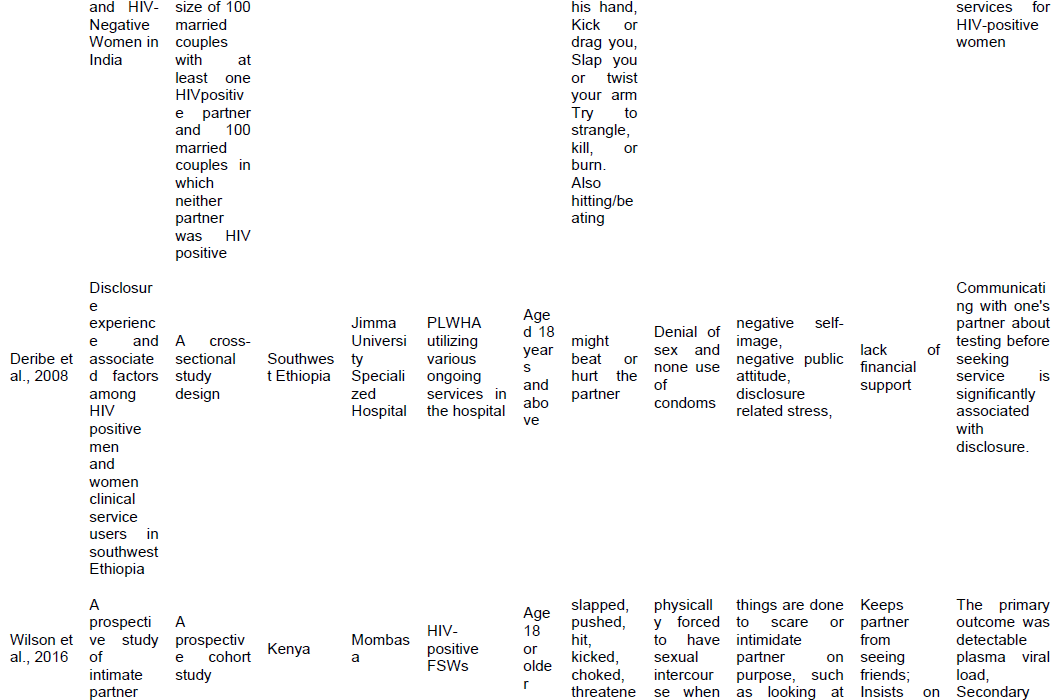
positive disclosure by the partners. Pushing or shaking of the partners, throwing something at them, punching them with the hands, kicking or dragging them, slapping them or twisting their arms and trying to strangle, kill, or burn them were some of the physical violence perpetrated as identified by Chakraborty et al. (2016) in their study. They also found hitting or beating as physical violence in their findings. Again, Deribe et al. (2008) found no physical violence. However, they found a failure to disclose seropositive status because of fear of violence like yelling and rejection.Wilson et al. (2016)in their study found slapping, pushing, hitting, kicking, choking, threatening or the use of a weapon to hit partners as some of the physical violence that was perpetrated among couples after seropositive status disclosure.
Sexual violence
All the 4 articles found sexual violence among couples after seropositivestatus disclosure (Chakraborty et al., 2016; Deribe et al., 2008; Hatcher et al., 2014; Wilson et al., 2016). Hatcher et al. (2014)found the refusal to have sex with the partnerafter HIV positive status disclosure, refusal to use a condom and having sex with her without her consent as sexual violence against particularly the women.Forced sex and none use of condoms were those found by Chakraborty et al. (2016)whilst Deribe et al.(2008)found denial of sex and none use of condoms as some of the sexual violence among couples. Wilson et al. (2016)found that participants were physically forced to have sexual intercourse when they did not want to have sex after they had disclosed their seropositive statuses.
Psychological violence
Here again, most participants in the four articles included in the study (Chakraborty et al., 2016; Deribe et al., 2008; Hatcher et al., 2014; Wilson et al., 2016) said they were psychologically abused when they disclosed their seropositive statuses to their partners. Pregnant women described having experienced some emotional abuse and abandonment after they had disclosed to their intimate partnersthat they were HIV positive. Some of these pieces of violence as perpetrated by intimate partners included coming home late and eventually leaving the relationship. Intimate partnerswere also scared of telling their HIV infected statuses to their heterosexualpartners(Hatcher et al., 2014). Fear of violence after disclosure and stigmawerefound by Chakraborty et al. (2016)and negative self-image, negative public attitude, disclosure related stress were those found by Deribe et al.(2008). Wilson et al. (2016)identified in their study that participants did things to scare or intimidate their partners on purpose, such as looking at her/him scornfully, yelling or smashing things.
Financial abuse and other forms of violence
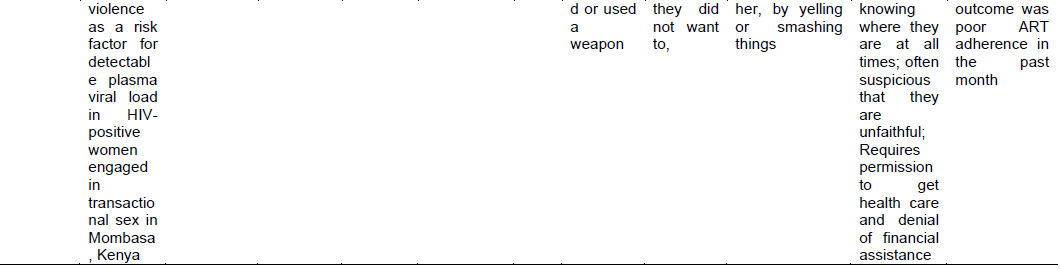
All the articles identified found thatwomen were blamed for supposedunfaithfulness and also accused of bringing the infection into their relationship (Hatcher et al., 2014), financial deprivation (Chakraborty et al., 2016) and lack of financial assistance (Deribe et al., 2008) prevented partners from visiting friends. Some of these acts of violence included insisting on knowing where their partners were always; often suspicious that their partnerswere unfaithful and needed permission to get health care. Denial of financial assistance (Wilson et al., 2016) was one of the violent activities found.
Significant findings
Some significant outcomes in this review included detectable plasma virus load, poor antiretroviral therapy (ART) adherence in the past month before the study (Wilson et al., 2016)and discussing about testing with one’s partner before seeking health service which was significantly associated with disclosure (Deribe et al., 2008). Again, the cultural context in which prevention programs were targeted as well ascounselling and support services for HIV-infected females (Chakraborty et al., 2016)were significant outcomes. Finally,the diagnosis for HIV during pregnancy was found to be a trigger of violence. Declines in mental health were noted in women experiencing IPV in pregnancy and IPV led to secondary HIV risk when women were in relationships with forced sex or without power to negotiate condom use(Hatcher et al., 2014).
DISCUSSION
A shown in Table 2, there were four articles (Hatcher et al., 2014; Chakraborty et al., 2014; Deribe et al., 2008; Wilson et al., 2016) that were extracted for the study. Despite much attention to HIV and IPV, international policy consensus on the need to facilitate safer disclosure of HIV status for women who experience or fear violence remains a problem (Kennedy et al., 2015), only four studies evaluating such studies globallywere identified. None of the four articles provided obvious evidence for the perpetration of IPV by men or women after the disclosure of the HIV statuses of their partners as this did not separate the contribution of the safer disclosure components from the broader multiple-component interventions as identified. The evidence for the four studies did not support safer disclosure and prevention of IPV making it quite limited, and so more studies will be required in this area.
Hatcher et al. (2014)conducted their study on bidirectional links between HIV and IPV in pregnancy: Implications for prevention of mother-to-child transmission where they used an exploratory qualitative study design and in-depth interviews (IDIs) as well as focus group discussions (FGDs) in three urban clinics in South Africa. The population was pregnant women and service providers in Johannesburg. The main findings were that there was the perpetration of physical violence, sexual violence, psychological violence as well as other forms of violence such as women being blamed for alleged unfaithfulnessand also being accused of bringing the infection into the family. The most important outcomes were the diagnosis of HIV during pregnancy which probably served as the trigger for IPV; there was also a reduction in mental health which was noticed in women who had experienced IPV during pregnancy and IPV resulted in a secondary risk for HIV infection when female partners had forced sex in their relationships or were without the power to negotiate the use of condoms (Hatcher et al., 2014). The second article was by Chakraborty et al.(2016)who used a quantitative survey design andquestionnaire and a sample size of 100 married partners with at least one of them being HIV positive and 100 married partners who were both not HIV positive. They found that there wasthe perpetration of physical, sexual, psychological as well as financial deprivation. The outcomes as identified in this study were that prevention programs were provided as well as the provision ofcounselling and support services for HIV-positive women(Chakraborty et al., 2016). The third study that was included for this review was that ofDeribe et al. (2008)who conducted their study on “Disclosure experience and associated factors among HIV positive men and women clinical service users in south-west Ethiopia”.
The main categories of violence identified were physical violence, sexual violence, psychological violence as well as lack of financial support. Themain outcomes werethat discussing with one's partner about testing for HIV before seeking health service was significantly associated with disclosing the HIV status (Deribe et al., 2008). The final and fourth study was by Wilson et al. (2016)who conducted their study entitled “A prospective study of IPV as a risk factor for detectable plasma viral load in HIV-positive women engaged in transactional sex in Mombasa, Kenya”. The main findings were significantly similar to Chakraborty et al. (2016), Deribe et al. (2008) and Hatcher et al. (2014)except for findings such as keeping partner from visiting friends; insisting on knowing the whereabouts of their partners always; always suspicious that they are unfaithful; requiring permission to seek health care and denying them financial assistance. The four studies, even though had some important findings on intimate partner violence, there is lack of studies on men perpetrating intimate partner violence following disclosure of the female partners or both. There is, therefore, the need to do a study to determine the views of men perpetrating violenceagainst their female intimate partners following the disclosure of their HIV positive statuses.
CONCLUSION
The findings of these studies suggest that disclosing the HIV status among couples needs to be improved as fear of IPV issignificantly high. Although these findings may serve as the starting point data for HIV status disclosure, more data on HIV status disclosure is important. Experiences of perpetrators of IPV against HIV positive partners were also limited and need to be explored by studies in this area. Finally, disclosure of HIV status to an intimate partner has significant importance in preventing new infections as well as preventing the perpetration of IPV against HIV seropositive couples. It is recommended that prevention of HIV infection should target male perpetrators of IPV against their female seropositive partners to institute positive behavioural changes in intimatepartners.
COMPETING INTERESTS
The authors hereby declare that they have no financial or personal relationship(s) which may have inappropriately influenced them in writing this article.
ACKNOWLEDGMENTS
This research was partially funded by the CHS PhD Scholarship grant awarded by the College of Health Sciences, University of KwaZulu-Natal, Durban. The assistance of the staff of the College of Health Sciences and the School of Nursing and Public Health, University of KwaZulu-Natal is gratefully acknowledged. The authors also wish to acknowledge the contributions of Tivani P. Mashamba-Thompson and Desmond Kuupiel for their immense contribution to this work.
REFERENCES
|
Ajayi LA, Olanrewaju FO, Olanrewaju A, Nwannebuife O, Amoo EO (2019). Gendered violence and human rights: An evaluation of widowhood rites in Nigeria. Cogent Arts and Humanities 6(1). |
|
|
Arksey H, O'Malley L (2005). Scoping studies: towards a methodological framework. International Journal of Social Research Methodology 8(1):19-32. |
|
|
Chakraborty H, Patted S, Gan A, Islam F, Revankar A (2016). Determinants of Intimate Partner Violence Among HIV-Positive and HIV-Negative Women in India. Journal of Interpersonal Violence, 31(3):515-530. |
|
|
Deribe K, Woldemichael K, Wondafrash M, Haile A, Amberbir A (2008). Disclosure experience and associated factors among HIV positive men and women clinical service users in Southwest Ethiopia. BMC Public Health 8:81. |
|
|
Hatcher WN, Pallitto CC, Mokoatle K, Stöckl H, MacPhail C, García-Moreno C (2014). Bidirectional links between HIV and intimate partner violence in pregnancy: implications for prevention of mother-to-child transmission. Journal of the International AIDS Society 17(1):19233. |
|
|
Hembling J, Andrinopoulos K (2014). Evidence of increased STI/HIV-related risk behavior among male perpetrators of intimate partner violence in Guatemala: results from a national survey. AIDS Care26(11):1411-1418. |
|
|
Kennedy CE, Haberlen S, Amin A, Baggaley R, Narasimhan M (2015). Safer disclosure of HIV serostatus for women living with HIV who experience or fear violence: a systematic review. Journal of the International AIDS Society 18(5). |
|
|
OgumAlangea D, Addo-Lartey AA, Sikweyiya Y, Chirwa ED, Coker-Appiah D, Jewkes R, Adanu RMK (2018). Prevalence and risk factors of intimate partner violence among women in four districts of the central region of Ghana: Baseline findings from a cluster randomised controlled trial. PLoS One 13(7):e0200874. |
|
|
Adjah ESO, Agbemafle I (2016). Determinants of domestic violence against women in Ghana. BMC Public Health 16:368. |
|
|
Pace R, Pluye P, Bartlett G, Macaulay AC, Salsberg J, Jagosh J, Seller R (2012). Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. International Journal of Nursing Studies 49(1):47-53. |
|
|
Sarnquist CC, Moyo P, Stranix-Chibanda L, Chipato T, Kang JL, Maldonado YA (2014).Integrating family planning and prevention of mother to child HIV transmission in Zimbabwe. Contraception, 89(3):209-214. |
|
|
Tenkorang EY, Owusu AY (2018). A life-course understanding of domestic and intimate partner violence in Ghana. Child Abuse Negl 79:384-394. |
|
|
Were E, Curran K, Delany-Moretlwe S, Nakku-Joloba E, Mugo NR, Kiarie J (2011). A prospective study of frequency and correlates of intimate partner violence among African heterosexual HIV serodiscordant couples. AIDS 25(16):2009-2018. |
|
|
Wilson KS, Wanje G, Yuhas K, Simoni JM, Masese L., Vander Stoep A, . . . Scott McClelland R (2016). A Prospective Study of Intimate Partner Violence as a Risk Factor for Detectable Plasma Viral Load in HIV-Positive Women Engaged in Transactional Sex in Mombasa, Kenya. AIDS Behav, 20(9):2065-2077. |
|
|
The World Bank Group Report (2018). Bank TW. Annual Report 2018. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


