Full Length Research Paper

ABSTRACT
As postpartum depression has become a major problem, it is necessary to identify mothers who need intensive support to cope with this disorder. Therefore, by summarizing literature from the past five years, this study aimed to clarify the current progress of research on the usefulness of oxytocin as a biomarker for postpartum depression; it also aimed to discuss the prospects for future research based on these findings. Literature published from 2016 to 2020 that examined the relationship among postpartum psychological state, postpartum depression, and oxytocin using the Medical Journal Web and PubMed for local and international literature were reviewed respectively. The search was conducted using the following keywords: “oxytocin,” “postpartum,” “depression,” “anxiety,” “mentality,” “sensation” and “psychology.” Furthermore, research articles (original papers and research reports) were the main focus of the search. Seven articles were extracted from the search. All of them reported an association between oxytocin and maternal psychological state. However, the views among them differed, and studies on the usefulness of oxytocin as a biomarker of postpartum depression were limited. Although various methods have been utilized to measure oxytocin, this study highlights the need for more consistent research methods, accounting for individual differences and factors that may influence oxytocin levels, to ensure accurate oxytocin measurement. This will enable the development of preventative interventions in addressing postpartum depression.
Key words: Oxytocin, biomarker, mother, postpartum depression.
INTRODUCTION
Postpartum depression produces undesirable outcomes, such as psychological distress for the mother and abuse of the child. Tokumitsu reported that the incidence of postpartum depression was 15.1% within one month, 11.6% between one and three months, 11.5% between three and six months, and 11.5% between six and 12 months after childbirth, illustrating that the incidence of postpartum depression in Japan is high (Tokumitsu et al., 2020). In Japan, studies on screening for postpartum depression and identifying risk factors for its development as well as preventive interventions have been conducted (Yubune, 2020). Many previous studies have used the Edinburgh Postnatal Depression Scale (EPDS), developed by Cox et al. (1987) and translated into Japanese by Okano (1996) as a screening tool for postpartum depression. The usefulness of the EPDS in screening for postpartum depression has been suggested by numerous researchers (Mishina et al., 2010; Sugishita and Kamibeppu, 2013). In this context, the Japanese Society of Perinatal Mental Health recommended that the Japanese version of the EPDS be administered in the first month after childbirth (Japanese Society of Perinatal Mental Health, 2017). Since then, EPDS screening has been conducted in many birth centers in Japan.
However, reports indicate that, every two years, 92 women were still committing suicide within the first year postpartum (National Center for Child Health and Development, 2018). In addition, it has been reported that mothers in need of support are extracted even if their score is below eight, which is considered as belonging to the “normal group” in the EPDS (Okawa et al., 2020). However, problems such as variability in judgment among interviewers and a shortage of manpower still exist.
In this context, recent studies have attempted to evaluate psychological stress using various biomarkers. Two main biological systems respond to psychological stress: The endocrine pathway, which transmits hormones from the hypothalamus to the anterior pituitary gland to the adrenal cortex, and the autonomic pathway, which transmits hormones from the hypothalamus to the sympathetic nervous system to the adrenal medulla. Among them, cortisol, a hormone derived from the adrenal cortex whose secretion increases when subjected to excessive stress, has been validated as an endocrine stress marker based on several research reports (Rector et al., 2019; Van den Heuvel et al., 2019; Luiza et al., 2015; Heinze et al., 2016; De Sio et al., 2018). Furthermore, the adrenal cortex has been used to measure stress caused by psychosocial and physical health factors in older adults (Rector et al., 2019) as well as posttraumatic stress (Van den Heuvel et al., 2019), work stress (De Sio et al., 2018), long-term mental problems (Heinze et al., 2016), and isolated environments (Luiza et al., 2015; Meng et al., 2020) in perinatal mothers. The usefulness of many other indices, such as chromogranin A (CgA), immunoglobulin A (IgA), cortisol, and amylase has also been reported (Obayashi, 2013; Cozma et al., 2017; Chojnowska et al., 2021). Furthermore, research using saliva and urine samples has been actively conducted as a simple, non-invasive measure of identifying mental stress. Thus far, various studies have been conducted to measure biomarkers that react to stress to detect the state of stress. However, this study propose that it is important to detect the condition before it becomes stressful (high risk) and to respond to it at an early stage; therefore, taking a preventative approach to managing postpartum depression is necessary.
This study focused on oxytocin as a biomarker for the extraction of such a state. Oxytocin has been studied in recent years because it is related to the formation of attachment, trust, and interpersonal relationships between mother and child. Oxytocin is a peptide hormone that was discovered in the early 1900s as a substance that stimulates uterine contractions and milk secretion in peripheral organs. Kosfeld et al. (2005) also reported that oxytocin increases trust in people. Previous reports on the effects of oxytocin include decreased fear (Kirsch et al., 2005), increased reading (understanding) of others' minds (Domes et al., 2007), increased trust (Theodoridou et al., 2009), and good conversational responses in marital strife conversations (Ditzen et al., 2007). In addition, reports on parent-child relationships include increased attachment protection (Buchheim et al., 2009). These reports indicate that oxytocin is important for the trust and love formed between people or for the biological basis of human activities (economic, political, social and family) (Higashida, 2013). Furthermore, oxytocin has been the subject of numerous studies regarding its association with mother-child attachment formation (Lara et al., 2017), parenting stress, and postpartum depression (Lara et al., 2017; Jobst et al., 2016; Cox et al., 2015). This study examined whether oxytocin can be used as a biomarker or screening tool to identify mothers at high risk for postpartum depression. To do this, what has been learned so far and what remains to be studied was clarified.
There have been several reports of literature reviews on the association between oxytocin and postpartum maternal psychological status or postpartum depression. In a review of oxytocin as a biomarker of postpartum depression, Mah (2016) conducted a literature review on the association between postpartum depression, parenting behaviors, and oxytocin and found that previous findings on the association between oxytocin, maternal mood, and postpartum depression were inconsistent. Other researchers also discussed the need for more research on this topic. In addition, Moura et al. (2016) reviewed six studies on the association between perinatal oxytocin and postpartum depression, as oxytocin is a substance that has attracted attention as a diagnostic and treatment tool for postpartum depression, four of which (Skrundz et al., 2011; Apter-Levy et al., 2013; Stuebe et al., 2013; Cox et al., 2015) showed an association between oxytocin and postpartum depression. Contrastingly, studies by Zelkowitz et al. (2014) and Garfield et al. (2019) reported that no association was found. Similarly, Mah (2016) reported inconsistent findings on the association between oxytocin and postpartum depression and further stated that there is room for improvement in sample size, methods utilized to measure postpartum depression, and methods of analysis. Thus, findings on the association between oxytocin and postpartum depression are contradictory. Future studies should include research methods in order to clarify the progress of the research (Moura et al., 2016), as many relevant studies have been reported since Mah (2016) ’s and Moura et al. (2016)’s reviews. To clarify the progress of the research, studies that have examined the relationship between oxytocin and postpartum depression was included. Literature examining the relationship between maternal psychological status or postpartum depression was also included to investigate the progress of research thus far and the prospects for future research, including methodological prospects. This study will provide an important reference for further research on the potential use of oxytocin as a biomarker for postpartum depression.
METHODS
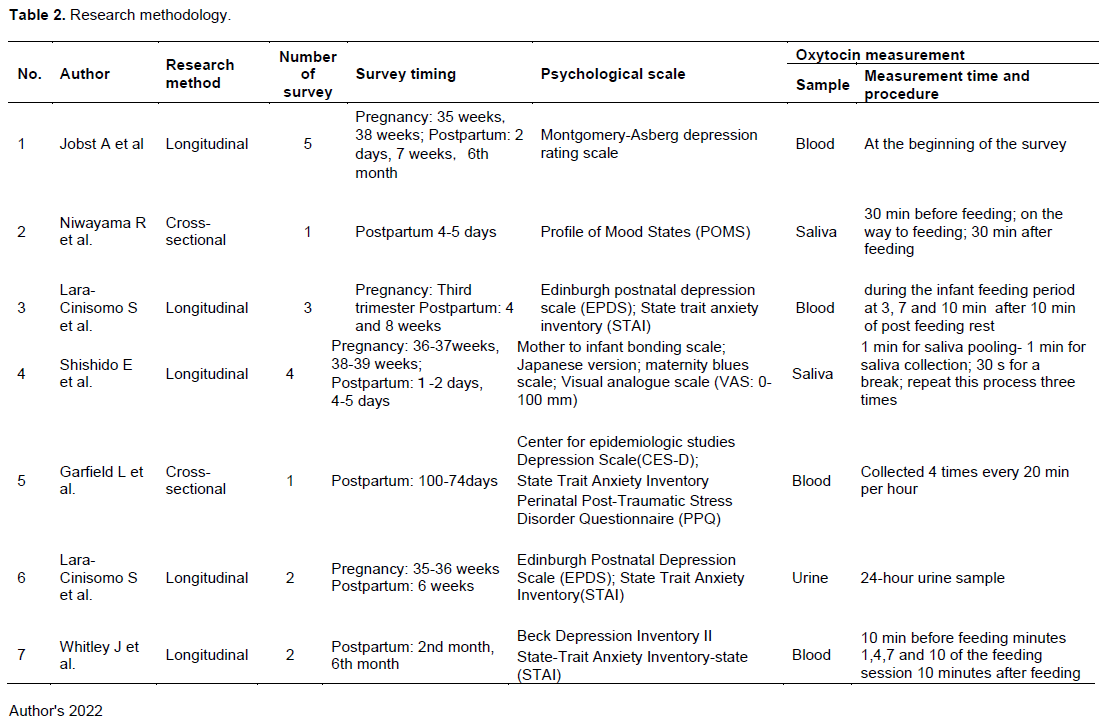
The literature published within five years, from 2016 to 2020, that examined the relationship between postpartum psychological state, postpartum depression, and oxytocin was reviewed using the Medical Journal Web for local literature and PubMed for international literature. We searched the literature using the following keywords: “oxytocin,” “postpartum,” “depression,” “anxiety,” “mentality,” and “psychology,” focusing on research articles (original papers and research reports). A summary of the research methodology for each study is shown in Table 2.
Research design
The studies were quantitative studies using scales. Of the seven studies, two were cross-sectional studies and five were longitudinal studies.
Selection criteria for participants
Two of the seven studies did not specify the inclusion or exclusion criteria and included mothers with a history of depression or anxiety. The remaining five included healthy pregnant women and postpartum mothers and excluded subjects with serious physical diseases, fetal malformations, in vitro fertilization, chronic or autoimmune diseases, acute heart diseases and schizophrenia, bipolar disorder or drug abuse, epilepsy, obstetric complications, gestational hypertension, alcoholism, infectious diseases (HIV; Human Immunodeficiency Virus, HBV; Hepatitis B Virus, and HCV; Hepatitis C Virus positive), and smokers. Although most studies selected subjects based on medical history charts, Shishido et al. (2019) used the PBI, STAI and CES-D to determine who had depression and anxiety; those without depression or anxiety were included in the study.
Survey period
Both cross-sectional studies surveyed only the postpartum period. Four of the five longitudinal studies surveyed the period from pregnancy to postpartum, and one surveyed only the postpartum period. Four of the five longitudinal studies were conducted during pregnancy and puerperium and one study was conducted during puerperium only. Pregnancy was limited to the second trimester and almost all studies were conducted after 35 weeks. In one cross-sectional study, the survey period in the postpartum period was relatively early (up to three months postpartum), and in the other, the survey period was up to six months postpartum, including the early postpartum period.
Measures
The psychological state of the mothers after childbirth was measured in five out of the seven studies. Two of them used the EPDS, and the others used the MADRS, CES-D and Beck Depression Inventory II. Four of the five studies that measured depressive symptoms also measured anxiety symptoms (four studies) and trauma (one study), with anxiety symptoms measured by the STAI and trauma by the PPQ. In addition, the MBS and POMS were used to measure mothers' psychological state, the MIBS-J to measure attachment formation, and the VAS to measure fatigue.
To measure oxytocin levels, seven samples were taken. Four of the seven samples were blood, two were saliva, and one was urine. In six of the seven studies, samples were collected by repeated measurements (or 24-hour urine collection). The following is a summary of the time and method of measurement and analysis for each sample.
Blood-based measurements
Of the four studies that measured oxytocin in blood, the three studies that performed repeated measurements considered the timing of breastfeeding and inserted an indwelling intravascular catheter. Furthermore, oxytocin was measured four times: three minutes after the start of breastfeeding; seven minutes after, 10 min after; and 10 min after breastfeeding ended (Lara et al., 2017). In Whitley et al.’s study (2020), it was measured 10 min before lactation started; 1, 4, 7 and 10 min after lactation started; and 10 minutes after the end of lactation (Whitley et al., 2020). The AUC was used to show the oxytocin level. Another study, by Garfield et al. (2014), did not mention the timing of breastfeeding and collected samples four times (blood samples 1 to 4) every 20 min for one hour to obtain continuous samples. Blood samples were collected under the following conditions: When blood samples 1 and 2 were collected, the mothers were isolated from their infants, and samples were collected in an environment that excluded objects that might affect oxytocin levels (e.g., pictures of loved ones, baby toys/dolls, or pregnancy/baby-related magazines). Blood samples 3 and 4 were collected near the infants, and after confirming that there was no significant difference in the variability of the four data by an analysis of variance, the median value was calculated for the oxytocin data after adjusting the oxytocin level using 1000 pg/mL as the cutoff criterion.
Measurement by saliva
Niwayama et al. (2017) collected saliva samples three times: 30 min before breastfeeding started, during breastfeeding, and 30 min after breastfeeding ended; they examined the relationship between each timing and psychological measures. Shishido et al. (2019) also established a protocol for each saliva sample collection (one minute saliva collection, one minute saliva collection, and 30 second’s rest. This was repeated three times). Oxytocin levels at each time point were correlated with psychological measures for each survey at four sites from gestation to postpartum.
Measurement by urine
Of the seven studies, that conducted by Lara et al. (2019) was the only one to measure oxytocin using a 24-hour urine sample. The obtained oxytocin values were corrected for creatinine.
RESULTS
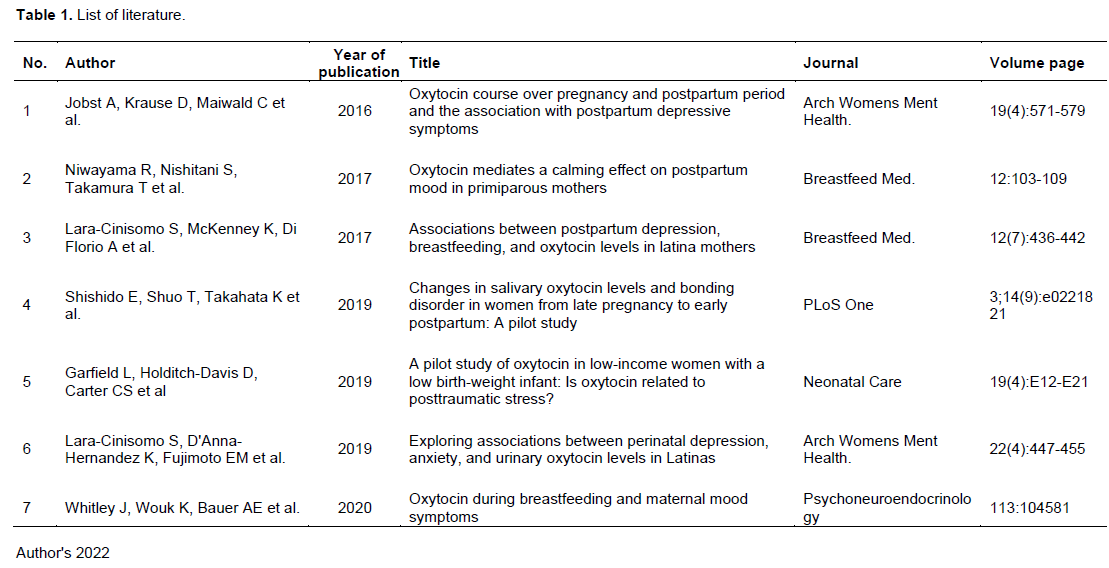
The results of the literature search are summarized in Table 1. The results showed that there were no Japanese references that fit the purpose of this study. International literature was also searched. Regarding the search terms, “oxytocin,” “postpartum,” and “depression” retrieved 77 results; “oxytocin,” “postpartum,” and “anxiety” retrieved 42 results; “oxytocin,” “postpartum,” and “mentality” returned 43 results; “oxytocin,” “postpartum,” and “psychology” retrieved 106 results; and “oxytocin,” “postpartum,” and “sensation” retrieved 12 results. Among them, excluding duplicate references, seven articles that fit the purpose of this study were selected for review. The year of publication was as follows: one in 2016, two in 2017, three in 2019, and one in 2020.
A longitudinal study was conducted at five time points: 35 weeks and 38 weeks of gestation, and 2, 7 and 6 months postpartum in 100 healthy women aged 24 to 42 years with a normal pregnancy and postpartum course (Jobst et al., 2016). Plasma levels of oxytocin were measured by the enzyme-linked immunosorbent assay (ELISA) in blood samples. Maternal psychological status was assessed using the Montgomery-Asberg Depression Rating Scale (MADRS) with a cutoff score of ≥10, with participants divided into the following groups based on their scores: “depressed” and “non-depressed.” The survey was conducted in the morning, with blood samples collected at the beginning of the survey, followed by completion of the questionnaire immediately thereafter. Blood samples were stored (at 4°C) immediately after collection. Thirty min after collection they were centrifuged at 1600 xg for 15 min and stored at -80°C until analysis. The analysis showed that oxytocin levels in the “non-depressed group” continued to increase from 35 weeks of gestation to six weeks postpartum, while oxytocin levels in the “depressed group” increased at 38 weeks gestation, decreased on the second postpartum day, and increased until six months postpartum.
To investigate the effects of oxytocin levels on maternal mood, changes in oxytocin secretion associated with breastfeeding and the associated changes in maternal mood were studied. Twenty-four lactating mothers were surveyed four to five days postpartum (Niwayama et al., 2016). Oxytocin was measured from saliva samples using an enzyme immunoassay 30 min before (baseline), during (lactation), and 30 min after completing (post-lactation) breastfeeding. The mothers’ psychological state was also assessed using the Profile of Mood States (POMS) scale. It was found that oxytocin levels increased 30 min before (baseline), during (lactation), and 30 min after completion of (post-lactation) breastfeeding. Tension-anxiety, fatigue, and confusion scores on the POMS scale were higher at 30 min after the completion of breastfeeding (post-lactation) than at 30 min before (baseline). Furthermore, these scores significantly decreased 30 min after breastfeeding compared to 30 min before (baseline). In contrast, there was a significant increase in the liveliness score.
To examine the association between neuroendocrine responses to breastfeeding and postpartum depression, a longitudinal study of 28 perinatal women was conducted at three time points: Late pregnancy, four weeks postpartum, and eight weeks postpartum (Lara-Cinisomo et al., 2017). In the second trimester, the EPDS and the State Trait Anxiety Inventory (STAI) were administered; in the fourth snd eighth week postpartum, the EPDS and STAI were administered and the lactation status was evaluated. In addition to the EPDS, STAI, and lactation status, at eight weeks postpartum, oxytocin (blood sample; blood was collected 3, 7 and 10 min after the start of lactation and 10 min after the end of lactation after inserting an indwelling intravascular catheter) was also measured. Oxytocin levels were calculated as the area under the blood concentration-time curve (AUC), which is expressed as blood concentration × time and is a comprehensive index that includes factors such as maximum blood concentration (Cmax) and half-life (t1/2) and can be used as an index that captures fluctuations in oxytocin concentration. The results showed that depressive symptoms and anxiety tendencies during pregnancy were associated with early breastfeeding cessation (cessation before eight weeks postpartum), and an association between oxytocin levels, early breastfeeding cessation, and depressive symptoms at eight weeks postpartum was found.
The purpose of this study was to determine the changes in salivary oxytocin levels in first time mothers from late pregnancy to early postpartum, the factors associated with these changes, and the attachment formation relationship between mothers and children (Shishido et al., 2019). Participants without depression or anxiety were selected based on the Parental Bonding Instrument (PBI), the STAI, and the Center for Epidemiologic Studies Depression Rating Scale (CES-D). The participants were asked to complete the Mother-to-Infant Bonding Scale Japanese version (MIBS-J), the Maternity Blues Scale (MBS), and the Visual Analogue Scale (VAS: 0-100 mm), which measures postpartum fatigue at four time points: 36-37 weeks of gestation, 38-39 weeks of gestation, 1-2 days postpartum, and 4 to 5 days postpartum. The results showed that salivary oxytocin levels increased significantly from late pregnancy (gestational weeks 36-39) to one day postpartum, and then decreased until five days postpartum. There were significant negative correlations between the MBS and salivary oxytocin levels as well as between postpartum fatigue (VAS) and salivary oxytocin levels at one and five days postpartum.
The purpose of this study was to examine the relationship between traumatic stress, depressive symptoms, and oxytocin in eight postpartum mothers (10 to 74 days postpartum) of preterm and low birth weight infants who were considered to have high levels of traumatic stress (Garfield et al., 2019). The mean age of the participants was 22.5 years, and five of them were breastfeeding. The mean birth weight of the infants was 1168.4 g, and the mean number of weeks in utero was 29. The mothers of infants currently on ventilators were excluded from the study. Blood samples were used to determine oxytocin. An indwelling needle was inserted into the subject's forearm, and oxytocin was collected four times (blood samples 1 to 4) every 20 min for 1 h to obtain a continuous sample, considering fluctuations in oxytocin due to stimuli such as needle insertion and visual stimulation of the infant. Blood samples 1 and 2 were collected in isolation from the infant and in an environment that excluded objects that might further affect oxytocin levels (e.g., pictures of loved ones, baby toys and dolls, or pregnancy/baby-related magazines), while blood samples 3 and 4 were collected near the infant. Blood samples were transported on ice, centrifuged (1500 xg, 15 min), and stored at -80°C until analysis. Analysis of variance was used to confirm that the four oxytocin levels obtained were not significantly different, excluding the data of the participant who showed a spike in oxytocin, and the median value was calculated after adjusting the oxytocin level using 1000 pg/mL as a cutoff criterion to examine the relationship with the questionnaire. Maternal psychological state was assessed using the CES-D and STAI, and traumatic stress was assessed using the Perinatal Posttraumatic Stress Disorder Questionnaire (PPQ). The results showed that breastfeeding mothers had lower depressive symptoms and posttraumatic stress symptoms than non-breastfeeding mothers. Women with elevated posttraumatic stress also had higher levels of depressive symptoms and lower levels of oxytocin.
A total of 108 women were included in this study. Depressive symptoms were measured using the EPDS, anxiety was measured using the STAI, and oxytocin was measured by 24-hour urine collection at two time points: late pregnancy (35 to 36 weeks) and six weeks postpartum (Lara-Cinisomo et al., 2019). The results showed that, overall, oxytocin levels decreased significantly from late pregnancy to postpartum, but participants with high EPDS and STAI in late pregnancy did not show significant changes in oxytocin levels from gestation to postpartum. At six weeks postpartum, participants with high scores on the EPDS and STAI continued to show persistently high oxytocin levels during pregnancy. Oxytocin levels in the depressed group were higher than those in the non-depressed group, and oxytocin levels in the high anxiety group were higher than those in the low anxiety group in both late pregnancy and postpartum data. However, there were no significant differences between the two groups.
Hypothesizing that postpartum depression is related to low oxytocin levels during lactation, a longitudinal study of 222 women (aged 18 to 45 years) at two and six months postpartum was conducted (Whitley et al., 2020). Participants were recruited at 34 weeks of gestation and demographic data was also collected. Patients with a history of psychiatric disorders, neonatal intensive care unit stays of more than 12 h, and perinatal deaths were excluded from the study. At two and six months postpartum, depressive and anxiety symptoms were measured using the Beck Depression Inventory II and STAI, respectively. Blood samples for oxytocin were collected 10 min before lactation started; one, four, seven, and 10 min after lactation started; and 10 min after lactation ended. Oxytocin levels measured across the feedings were defined using the AUC. The results showed no significant differences in oxytocin levels during breastfeeding due to depressive or anxiety symptoms; however, at two months postpartum, oxytocin was lower in mothers with depressive symptoms. At six months postpartum, this trend reversed with higher oxytocin levels displayed in mothers with depression.
Overall, the above seven studies reported an association between oxytocin and maternal psychological state. However, Niwayama et al. (2017), Lara et al. (2017), Shishido et al. (2019), and Garfield et al. (2014) mentioned a negative psychological state and low oxytocin levels, and Lara-Cinisomo et al. (2019) reported that a negative psychological state may be associated with high oxytocin levels. Furthermore, Whitley et al. (2020) showed similar results at two months postpartum and found negative psychological states and low oxytocin levels at six months postpartum. In addition, Jobst et al. (2016) found differences between the presence of postpartum depressive symptoms and oxytocin fluctuations from gestation to postpartum and stated that oxytocin fluctuations may predict postpartum depression.
DISCUSSION
Although prior research has shown an association between oxytocin and postpartum depression, the methods utilized and overall findings of these studies have yielded inconsistent results. Thus, the purpose of this study was to discuss the research trends and, based on this, future research issues regarding the usefulness of oxytocin as a biomarker for postpartum depression. To do so, the study examined the survey and analysis methods used in recent studies and discussed the direction of future research based on the findings thus far. The literature review revealed that there are still minimal studies and insufficient views regarding oxytocin as a biomarker for postpartum depression. However, various research methods have been utilized in investigating this relationship, which will be an important reference for future studies. The study’s findings are discussed in relation to prior research as follows.
Measures
All seven studies examined the relationship between maternal psychological measures using scales and oxytocin measures using biochemical indicators. Although the scales used differed depending on how the negative psychological state was defined, anxiety symptoms, which have been associated with postpartum depression, were measured by the STAI, which has been incorporated in many studies and has been found to be associated with oxytocin. In addition, the EPDS, MADRS, CES-D and Beck Depression Inventory II were used to measure postpartum depression, however, there was no agreement on the relationship between the scores obtained on the scales and oxytocin. The psychological state reflected in oxytocin should be examined not only for postpartum depression, but also for psychological states related to postpartum depression. This will enable the unique psychological state before postpartum depression to be captured, which can be utilized to detect postpartum depression early.
Survey participants
Five out of the seven studies were conducted on normal postpartum mothers and those with a history of mental illness were excluded. However, Whitley et al. (2020) stated that the limitation of their study was that all the mothers had relatively mild depressive symptoms. Jobst et al. (2016) also stated that the reason for their different results, compared to previous studies, was that the mothers were not in the “diagnosed” postpartum depression group, and that there is a need to further examine mothers who have been diagnosed with postpartum depression. Thus, to obtain more accurate results, it is necessary to consider mothers who experienced a wide range of psychological conditions. For this purpose, including mothers with psychiatric disorders, high anxiety levels, or other backgrounds or factors that are likely to cause instability in their psychological state should be considered, rather than including only normal postpartum mothers as in five of the seven studies reviewed.
Survey institution and oxytocin measurement
The survey period was conducted only in the early postpartum period or from late pregnancy to the early postpartum period. Ogawa (1980) found that oxytocin levels increased as pregnancy progressed and were even higher in the second stage of labor. Goldstein et al. (2005) showed that oxytocin secretion is increased by estrogen, which is elevated toward the expected day of parturition, and that oxytocin receptor expression is increased in the brain. It is well known that oxytocin levels are higher closer to delivery and that they drop quickly as the uterus recovers after delivery. Although oxytocin levels drop during the postpartum period, they rise again during lactation and trigger the suckling reflex. Jobst et al. (2016) investigated the period from late pregnancy to early postpartum, when oxytocin undergoes a period of great fluctuation, and found that the transition of oxytocin from late pregnancy to the early postpartum period was related to maternal depression. In addition, Lara et al. (2017) and Whitley et al. (2020) observed differences in the oxytocin variation due to breastfeeding and showed the transition as the AUC to examine the relationship with maternal psychological state. As shown in these reports, there have been several studies examining the relationship between oxytocin fluctuations and mothers’ psychological state. Garfield et al. (2019) calculated the median after confirming that there was no significant difference between the data obtained from the questionnaire survey and the repeated measurements of four times per hour, regardless of the timing of breastfeeding. Data were collected in this manner owing to the variation of oxytocin and the discrimination of oxytocin spikes. It has been found that regardless of the duration of breastfeeding, oxytocin fluctuates greatly with some stimuli (such as breastfeeding) or influences and that there are large individual differences in these fluctuations (Matsunaga et al., 2020). Furthermore, Garfield et al. (2019), who stated that there are large individual differences in oxytocin levels, adjusted their oxytocin data based on a cutoff of 1000 pg/mL for all oxytocin values above 1000 pg/mL. This suggests that it should be fully considered how appropriate it is to use the calculated oxytocin data. Furthermore, the relationship between oxytocin and psychological state needs to be further investigated using values that consider fluctuations through repeated measurements, rather than simply measuring oxytocin levels once and examining the relationship with psychological states. In addition, the factors that cause individual differences in oxytocin levels and fluctuations should be further examined. However, oxytocin is known to be stimulated and fluctuates not only due to breastfeeding but due to various factors, one example being visual factors, which include objects that may affect oxytocin levels, such as pictures of loved ones, baby toys/dolls, or pregnancy/baby-related magazines. Therefore, Garfield et al. (2019) had to carefully consider how to set up an environment in which the measurement would be conducted, accounting for these factors that may influence oxytocin levels. This suggests that the consideration of additional factors should be accounted for to ensure a more accurate measurement of oxytocin.
Oxytocin as a stress Indicator
All seven studies included in this review reported an association between oxytocin and maternal psychological state. However, although Niwayama et al. (2017), Lara et al. (2017), Shishido et al. (2019), and Garfield et al. (2019) reported negative psychological states and low oxytocin levels, similar to the findings of previous studies, Lara et al. (2019) reported that negative psychological states may be associated with high oxytocin levels. Whitley et al. (2020) also showed a relationship between negative psychological states and low oxytocin levels at six months postpartum. As stated by Higashida (2013), oxytocin is important for trust and love to be formed between people or for the biological basis of human activities (economic, political, social and family). There are also many reports on its association with childcare stress and postpartum depression (Cox et al., 1987; Lara et al., 2017; Jobst et al., 2016); thus, it is quite possible that oxytocin could be an indicator for early detection of postpartum depression. Matsunaga et al. (2020) found that there are individual differences in oxytocin variability with breastfeeding and that mothers with higher oxytocin levels had greater accuracy in perceiving pleasant facial expressions compared to unpleasant facial expressions. This may explain why oxytocin has a blunting effect on the stress felt by mothers. This further suggests that minimizing stress may reduce the likelihood of postpartum depression. Therefore, to utilize oxytocin as a biomarker for postpartum depression, further research should be conducted with careful considerations regarding the research methods utilized when investigating the association between oxytocin and postpartum depression.
CONCLUSION
This study summarizes recent research articles on the usefulness of oxytocin as a biomarker for postpartum depression and reveals the following: (i) oxytocin measurement protocols vary in different studies, and (ii) oxytocin fluctuations during the perinatal period vary greatly among individuals in terms of time, value, and transition with stimulation (breast milk). These findings indicate that further research is needed to determine the appropriate method and timing of oxytocin concentration measurements during the perinatal period. Further studies that consider individual differences in oxytocin concentrations are expected to index oxytocin as a biomarker for postpartum depression and enable preventive interventions for this disorder in mothers.
CONFLICT OF INTERESTS
The authors declare no conflicts of interest with the research or writing of this paper.
ACKNOWLEDGMENTS
This work was supported by JSPS KAKENHI Grant Number JP18K10377.
REFERENCES
|
Apter-Levy Y, Feldman M, Vakart A, Ebstein RP, Feldman R (2013). Impact of maternal depression across the first 6 years of life on the child's mental health, social engagement, and empathy: the moderating role of oxytocin. American Journal of Psychiatry, 170(10):1161-1168. |
|
|
Buchheim A, Heinrichs M, George C, Pokorny D, Koops E, Henningsen P, O'Connor M-F, Gündel H (2009). Oxytocin enhances the experience of attachment security. Psychoneuroendocrinology 34(9):1417-1422. |
|
|
Chojnowska S, Ptaszy?ska-Sarosiek I, K?pka A, Kna? M, Waszkiewicz NJ (2021). Salivary biomarkers of stress, anxiety and depression. Journal of Clinical Medicine 10(3):517. |
|
|
Cox EQ, Stuebe A, Pearson B, Grewen K, Rubinow D, Meltzer-Brody S. (2015). Oxytocin and HPA stress axis reactivity in postpartum women. Psychoneuroendocrinology 55:164-172. |
|
|
Cox JL, Holden JM Sagovsky R. (1987). Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. The British Journal of Psychiatry 150:782-786. |
|
|
Cozma S, Dima-Cozma LC, Ghiciuc CM, Pasquali V, Saponaro A, Patacchioli FR (2017). Salivary cortisol and α-amylase: subclinical indicators of stress as cardiometabolic risk. Brazilian Journal of Medical and Biological Research 50(2):e5577. |
|
|
De Sio S, Letizia C, Petramala L, Saracino V, Cedrone F, Sanguigni P, Buomprisco G, Perri R, Trovato Battagliola E, Mannocci A, La Torre G (2018). Work-related stress and cortisol levels: is there an association? Results of an observational study. European Review for Medical and Pharmacological Sciences 22(24):9012-9017. |
|
|
Ditzen B, Neumann ID, Bodenmann G, von Dawans B, Turner RA, Ehlert U, Heinrichs M (2007). Effects of different kinds of couple interaction on cortisol and heart rate responses to stress in women. Psychoneuroendocrinology 32(5):565-574. |
|
|
Domes G, Heinrichs M, Michel A, Berger C, Herpertz SC (2007). Oxytocin improves "mind-reading" in humans. Biological Psychiatry 61(6):731-733. |
|
|
Garfield, L, Giurgescu C, White-Traut R, Carter C, Holditch-Davis D, McFarlin BL, Seng JS, Schwertz D (2014). 158. Prenatal depressive symptoms, oxytocin and birth-weight in urban African American women. Brain, Behavior, and Immunity 40(Supplement):e46 |
|
|
Garfield L, Holditch-Davis D, Carter CS, McFarlin BL, Seng JS, Giurgescu C, White-Traut R (2019). A pilot study of oxytocin in low-income women with a low birth-weight infant: is oxytocin related to posttraumatic stress? Advances in Neonatal Care 19(4):E12-E21. |
|
|
Goldstein I, Meston Cindy M, Davis S, Traish A (2005). Women's sexual function and dysfunction: Study. Diagnosis and Treatment. CRC Press. ISBN 978-1-84214-263-9. |
|
|
Heinze K, Lin A, Reniers RLEP, Wood SJ (2016). Longer-term increased cortisol levels in young people with mental health problems. Psychiatry Research 236:98-104. |
|
|
Higashida H (2013). Social memory and autism: recovery of autistic disturbance by intranasal or subcutaneous OT administration and single nucleotide polymorphisms of CD38. Drug Delivery System 28(4):310-317. |
|
|
Jobst A, Krause D, Maiwald C, Härtl K, Myint AM, Kästner R, Obermeier M, Padberg F, Brücklmeier B, Weidinger E, Kieper S, Schwarz M, Zill P, Müller N (2016). Oxytocin course over pregnancy and postpartum period and the association with postpartum depressive symptoms. Archives of Women's Mental Health 19(4):571-579. |
|
|
Kirsch P, Esslinger C, Chen Q, Mier D, Lis S, Siddhanti S, Gruppe H, Mattay VS, Gallhofer B, Meyer-Lindenberg A (2005). Oxytocin modulates neural circuitry for social cognition and fear in humans. Journal of Neuroscience 25(49):11489-11493. |
|
|
Kosfeld M, Heinrichs M, Zak PJ, Fischbacher U, Fehr E (2005). Oxytocin increases trust in humans. Nature 435(7042):673-676. |
|
|
Lara-Cinisomo S, D'Anna-Hernandez K, Fujimoto EM, Pedersen CA (2019). Exploring associations between perinatal depression, anxiety, and urinary oxytocin levels in Latinas. Archives of Women's Mental Health 22(4):447-455. |
|
|
Lara-Cinisomo S, McKenney K, Di Florio A, Meltzer-Brody S (2017). Associations between postpartum depression, breastfeeding, and oxytocin levels in Latina mothers. Breastfeeding Medicine 12(7):436-442. |
|
|
Luiza JW, Gallaher MJ, Powers RW. (2015). Urinary cortisol and depression in early pregnancy: role of adiposity and race. BMC Pregnancy and Childbirth 15:30. |
|
|
Mah BL (2016). Oxytocin, postnatal depression, and parenting: A systematic review. Harvard Review of Psychiatry 24(1):1-13. |
|
|
Matsunaga M, Kikusui T, Mogi K, Nagasawa M, Ooyama R, Myowa M (2020). Breastfeeding dynamically changes endogenous oxytocin levels and emotion recognition in mothers. Biology Letters 16(6):20200139. |
|
|
Meng C, Wang W, Hao Z, Hong L (2020). Investigation on the influence of isolated environment on human psychological and physiological health. Science of the Total Environment 716: 136972. |
|
|
Mishina H, Takayama J, Nishiumi M (2010). Screening for postpartum Depression at one month well-child visit. Journal of Children's Health 69(5):703-707. |
|
|
Moura D, Canavarro MC, Figueiredo-Braga M (2016). Oxytocin and depression in the perinatal period-a systematic review. Archives of Women's Mental Health 19(4):561-570. |
|
|
Niwayama R, Nishitani S, Takamura T, Shinohara K , Honda S , Miyamura T , Nakao Y , Oishi K , Araki-Nagahashi M (2017). Oxytocin mediates a calming effect on postpartum mood in primiparous mothers. Breastfeeding Medicine 12:103-109. |
|
|
Obayashi K (2013). Salivary mental stress proteins. Clinica Chimica Acta; International Journal of Clinical Chemistry, 425(425):196-201. |
|
|
Ogawa S (1980). Physiological variation of oxytocin in normal females and males: relation of estrogen, progesterone, testosterone and LH-RH to oxytocin secretion. Nihon Naibunpi Gakkai Zasshi 56(9):1182-1199. |
|
|
Okano T (1996). Reliability and validity of the Japanese version of the Edinburgh postpartum depression self-assessment sheet (EPDS). Archives of Psychiatric Diagnostics and Clinical Evaluation 7(4):525-533. |
|
|
Okawa H, Ishii A, Tanaka T (2020). Efforts to introduce the "Mental Health Checklist" (EPDS) at maternity health checkups. Shizuoka Journal of Maternal Health 9(1):21-23. |
|
|
Rector JL, Tay L, Wiese CW, Friedman EM (2019). Relative sensitivity of cortisol indices to psychosocial and physical health factors. PLOS ONE, 14(4):e0213513. |
|
|
Shishido E, Shuo T, Takahata K, Horiguchi S (2019). Changes in salivary oxytocin levels and bonding disorder in women from late pregnancy to early postpartum: A pilot study. PLOS ONE 14(9):e0221821. |
|
|
Skrundz M, Bolten M, Nast I, Hellhammer DH, Meinlschmidt G (2011). Plasma oxytocin concentration during pregnancy is associated with development of postpartum depression. Neuropsychopharmacology 36(9):1886-1893. |
|
|
Stuebe AM, Grewen K, Meltzer-Brody S (2013). Association between maternal mood and oxytocin response to breastfeeding. Journal of Women's Health 22(4):352-361. |
|
|
Sugishita K, Kamibeppu K (2013). Relationship between prepartum and postpartum depression to use EPDS. Maternal Health 53(4):444-450. |
|
|
Theodoridou A, Rowe AC, Penton-Voak IS, Rogers PJ (2009). Oxytocin and social perception: oxytocin increases perceived facial trustworthiness and attractiveness. Hormones and Behavior 56(1):128-132. |
|
|
Tokumitsu K, Sugawara N, Maruo K, Suzuki T, Shimoda K, Yasui-Furukori N (2020). Prevalence of perinatal depression among Japanese women: a meta-analysis. Annals of General Psychiatry 19: 41. |
|
|
Van den Heuvel LL, Wright S, Suliman S, Stalder T, Kirschbaum C, Seedat S (2019). Cortisol levels in different tissue samples in posttraumatic stress disorder patients versus controls: a systematic review and meta-analysis protocol. Systematic Reviews 8(1):7. |
|
|
Whitley J, Wouk K, Bauer AE, Grewen K, Gottfredson NC, Meltzer-Brody S, Propper C, Mills-Koonce R, Pearson B, Stuebe A (2020). Oxytocin during breastfeeding and maternal mood symptoms. Psychoneuroendocrinology 113:104581. |
|
|
Yubune K (2020). Examination of the screening of depressed state from early pregnancy, metaphase, and advanced stage to one month after giving birth. The Showa University Society 75(4):465-473. |
|
|
Zelkowitz P, Gold I, Feeley N, Hayton B, Carter CS, Tulandi T, Abenhaim HA, Levin P (2014). Psychosocial stress moderates the relationships between oxytocin, perinatal depression, and maternal behavior. Hormones and Behavior 66(2):351-360. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


