ABSTRACT
For many women, labour and childbirth is a time of excitement and anticipation alongside uncertainty, anxiety, fear and pain. The memories and experiences of childbirth remain with the woman throughout her life. Clearly, the support and care they receive during this period is critical. The study aims to assess quality of nursing care offered during intrapartum and postpartum periods, patient satisfaction with care and to find the relationship between maternal satisfaction and some variables example, maternal age, education, duration of labor and reproductive history. A descriptive study was carried out from 22 April, 2013 through 15 February, 2014. A purposive sample of (200) postpartum women, delivered at the maternity teaching hospital. A questionnaire was comprised of two parts: socio-demographic characteristics and History of pregnancy and Women's views of birth Labor Satisfaction Questionnaire (WQBLS4). Data were collected through interview and analyzed through the application of descriptive and inferential statistical approaches by statisitical package for social sciences (SPSS) (17.0) program. ANOVA (F) test was used in the statistical assessment and the figure of p<0.05 was considered as the statistically significant. The study findings, indicate that women were satisfied regarding their expectations of the childbirth process, length and holding their baby, support from husband and their relative, in addition they were strongly satisfied with items related to professional support, environment and general satisfaction. The study concludes that the main factors identified as influencing satisfaction and dissatisfaction were, caregivers and client interaction, the characteristics of the setting, the involvement of clients in the caring process, the nurses’ perception of client characteristics, the outcome of labour for both mother and baby.
Key words: Satisfaction, nursing care, labour.
Pregnancy and birth are physiologic processes, unique to each woman, that usually proceed normally. Most women have normal conception, fetal growth, labor, and birth and require minimal or no intervention in the process. Women and their families hold different views about childbearing based on their knowledge, experiences, belief systems, culture, and social and family backgrounds (American Academy of Family Physicians, 2013). Childbirth is described as a multifaceted experience. Factors contributing to each women's experience or her sense of security and perceived control are; personal support, midwifery care, possible previous experience of deliveries and level of labor pain, intrapartum analgesia, information given and involvement in decision-making. Unplanned medical interventions during childbirth, example, oxytocin augmentation, emergency caesarean and operative vaginal deliveries, intrapartum complications and need of neonatal intensive care are related to maternal dissatisfaction (Dzomeku, 2001).
One indicator of health care quality, is patient satisfaction which is the ultimate consumer satisfaction or client satisfaction. Several studies have considered patient satisfaction to be a predictor of patient's treatment compliance, their ongoing use of health care services, recommendation of health care services to others, and providing a valuable feedback to evaluate health programs (Bradley et al., 1983). Patient satisfaction with nursing care is a patient's opinion about the sufficiency or acceptability of the nursing care they received (Chunuan, 2002). Patient satisfaction with nursing care is an important outcome of health care services, and achieving a high level of satisfaction is one of the goals of healthcare organizations (Bear and Bowers, 1998). Linder-Pelz (1982) mentioned that the patient satisfaction is crucial for maintaining and monitoring the quality of nursing care. In order to improve health care services, patient satisfaction with care should be surveyed (Fakhoury,1998).
Research has demonstrated that a positive childbirth experience helps a woman develop a positive attitude towards motherhood, which facilitates the transition into the maternal role. The positive experience can also establish rich and successful family relations, encourage self esteem, improve self-confidence and ensure positive development of the woman (Chwinui, 2010).
Labour is a time of women's unique sensitivity to environmental factors. Events and the interactions occurring during labour have powerful psychological effects, therefore a positive childbirth experience is desirable for the benefit of both the parturient woman and her child (Andrzejewski and Lagua, 1997). Studies have also confirmed that the intrapartum and postpartum nurse has often been the deciding factor of whether the woman has a positive or negative experience during childbirth (Chunuan, 2002).
In maternal-child nursing practice, patient satisfaction has been widely recognized as one of the critical indicators of the quality and the efficiency of the health care systems (Johansson et al., 2002).
The study was conducted using a destructive quantitative design to assess the quality of nursing care offered during intrapartum and postpartum periods using patients' satisfaction as an indicator. This study was approved by the ethical committee of school of Nursing, University of Sulaimani.
Setting of the study
The study was conducted at the Maternity Teaching Hospital located in Suleimani, Kurdistan region, which is the main maternity hospital that serve as the teaching hospital for the school of medicine, school of nursing, school of health sciences, school of public health and school of pharmacy. Before embarking on any steps in the study, official letter was issued from the school of nursing to the director of the hospital. The letter explained the aim of the study, clarified its procedures, and sought permissions to conduct it in this setting.
Sample of the study
A non – probability purposive sample of 200 women who had given birth in maternity teaching hospital, were selected for the present study. Inclusion criteria included: Primips and multigravida, normal vaginal delivery of term infant without maternal or infant complications, fetuses were in vertex presentation, with no known complications. Those receiving Oxytocin were also included while Exclusion criteria included Women with known complications, including preterm labor, multiple pregnancy, with antipartum hemorrhage, severe anemia, breech presentation, operative vaginal delivery (forceps and vacuum) and elective and emergency c-sections.
Instrument
Two questionnaires were used in this study: Demographic characteristics and history of pregnancy and Women's views of birth Labor Satisfaction Questionnaire (WQBLS4). The questionnaires consists of the following parts:
First questionnaire: Datasheet: The instrument consists of questions, the first (4) items concerning the respondents’ general characteristics (age, educational level, employment and residency) the next (4) items gather information about pregnancy, including No. of Para, abortion, dead fetus and the remaining items pertain to information regarding labor and delivery (duration of labor and oxytocin augmentation). Additional questions addressing satisfaction of hospital services include. Would you return to this hospital for another delivery and would you recommend this hospital to your family or friends for delivery? Second questionnaire: Women's views of birth labor satisfaction questionnaire (WQBLS4): consist of 8 dimensions. The first, professional support consists 5 items, the second subscale measures a woman's expectation which includes 4 items, home assessment 3 items, holding the baby 3 items, support of a husband which includes 3 items, pain in labor 3 items, pain after delivery 3 items, continuity have 2 items, environmental 2 items, control includes 2 items and general satisfaction 2 items.
The rating score for the instrument was 3 for always, 2 for some time, and 1 for never, with Cut-off-point =2. The satisfaction of the quality of nursing care was rated as follows:
Unsatisfied = less than the cut-off-point (<2)
Satisfied = equal or more than cut-off-point (>2)
Statistical analysis: The data were analyzed using SPSS version 17.0 software program.
To minimize bias, interviews were conducted in an area with adequate confidentiality and privacy and without any involvement of health care provider.
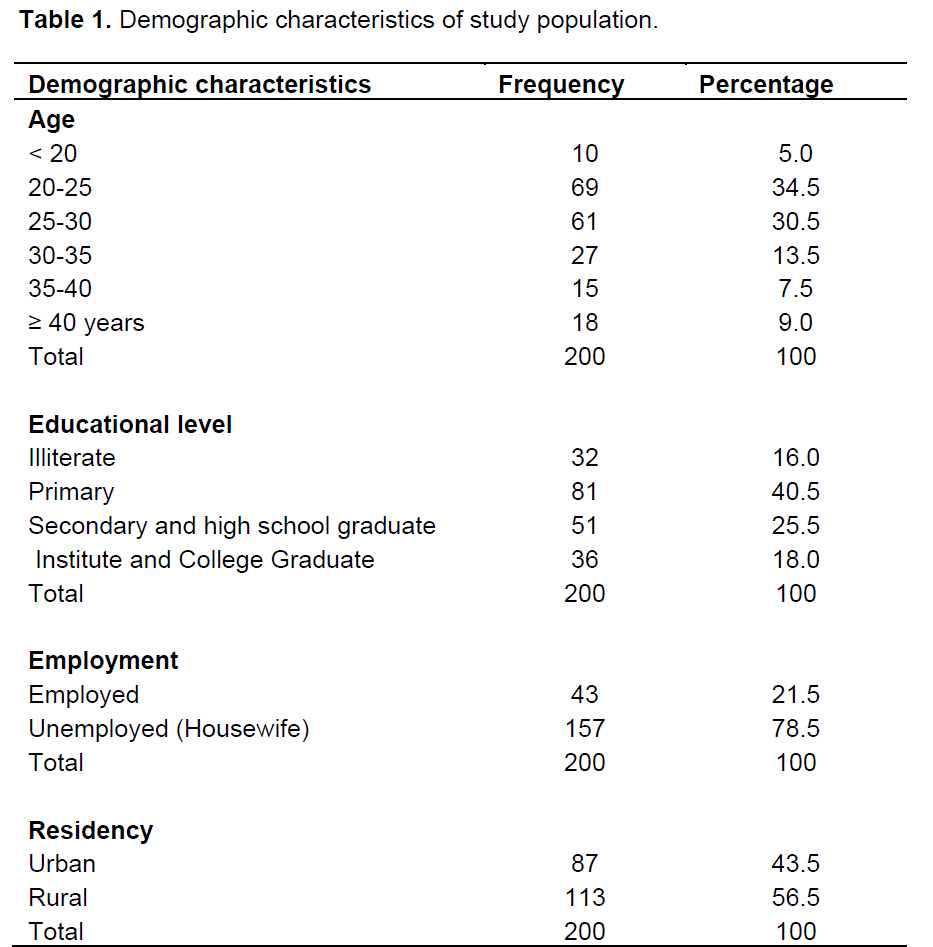
Table 1 shows the following characteristics of the study group, according to demographic data. The study group has age ranged from 17 to 44 years, 35% of women were in the age group of 20 to 25 years. As regards to the educational level, it was found that 40.5% of them had primary school education. The occupational status for the majority, more than three quarter of them (78.5%) were housewives and more than a half the women (56.5%) were living in rural areas.
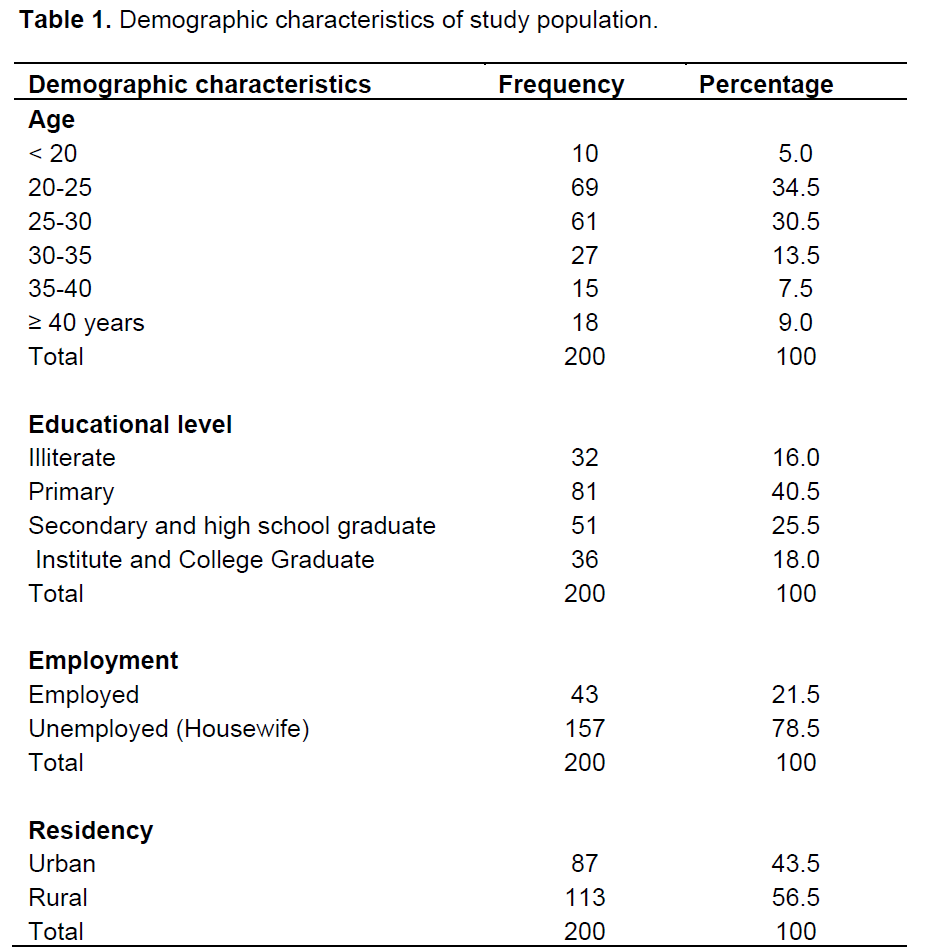
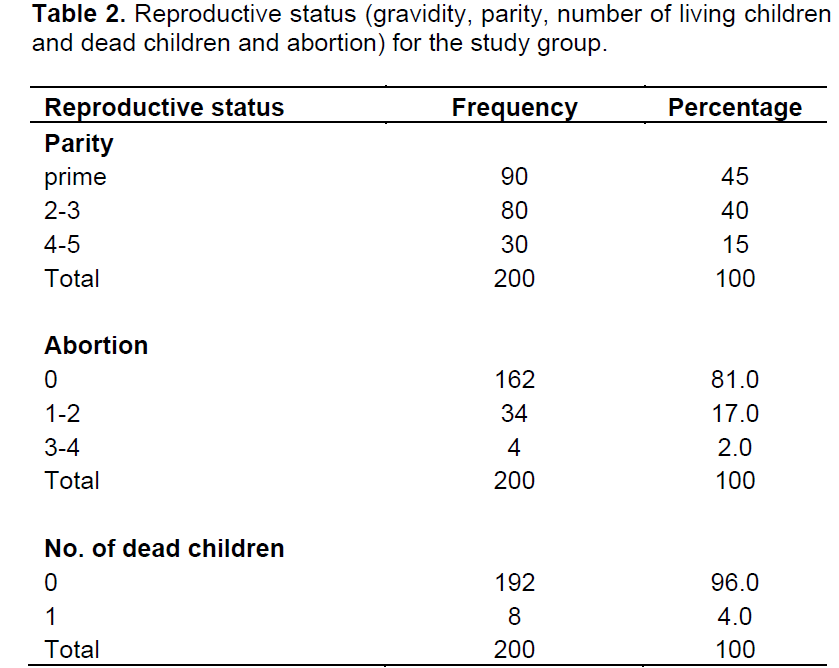
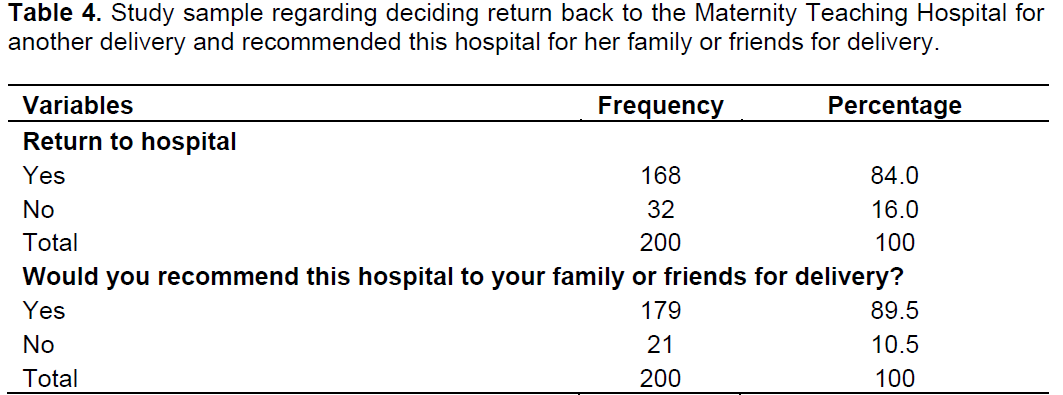
Table 2 shows the reproductive status of the study group. The number of parity range from 0 to 5 Para, most of them (45%) were primipara. The number of abortion range from 0 to 4, and 80% of women hadn’t had previous abortion, also majority (96%) of the women of the study sample haven’t lost any of their child.. As regards to parity, more than one half of the women (54.8%) were primipara. Table 3 to 5 shows that the majority (84%) of the study group accepted to return back to the maternity teaching hospital for next delivery and also majority (89.5%) of them recommended this hospital to their family or friends for delivery.
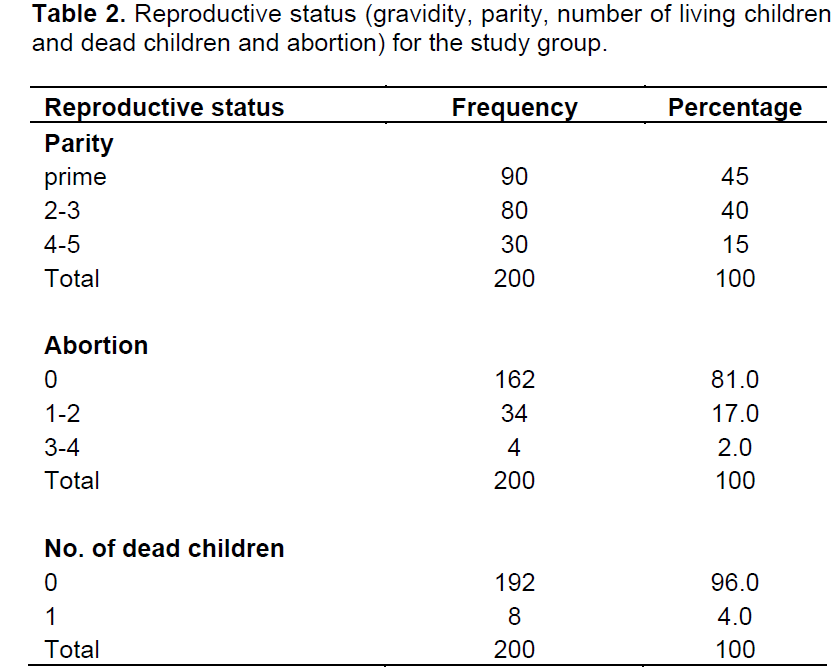
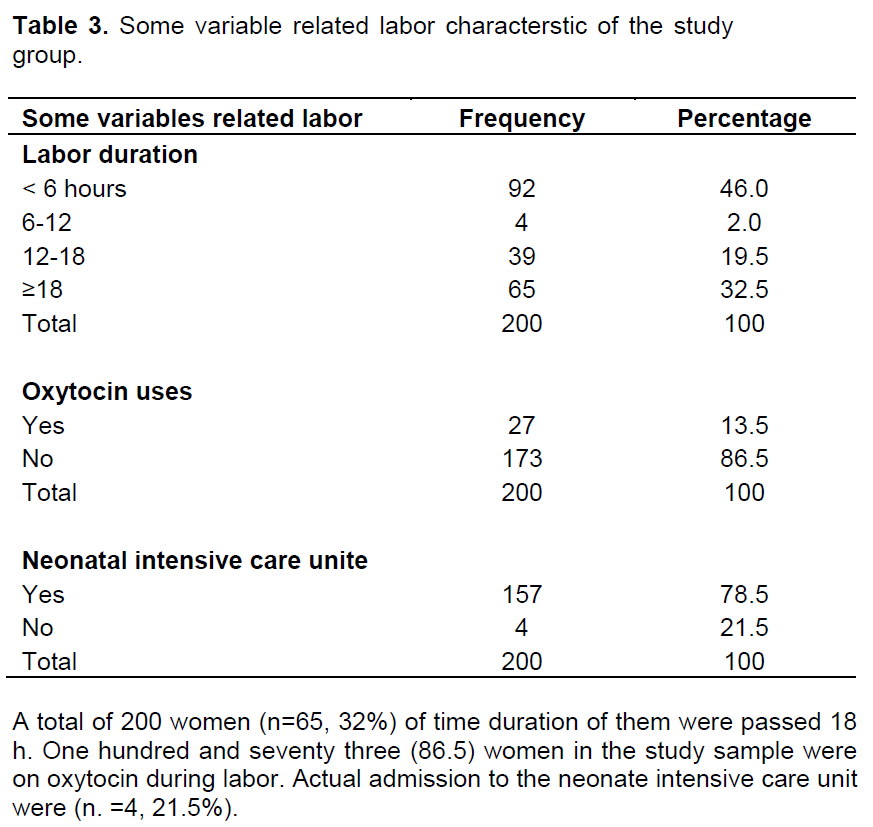
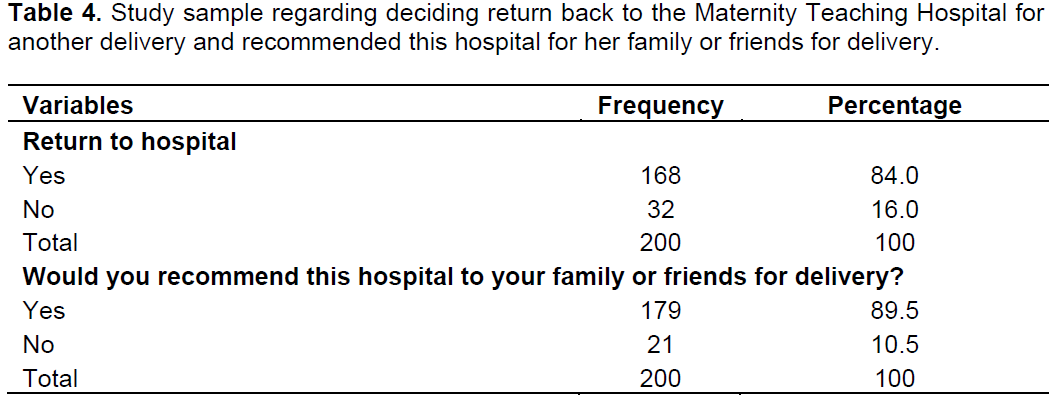
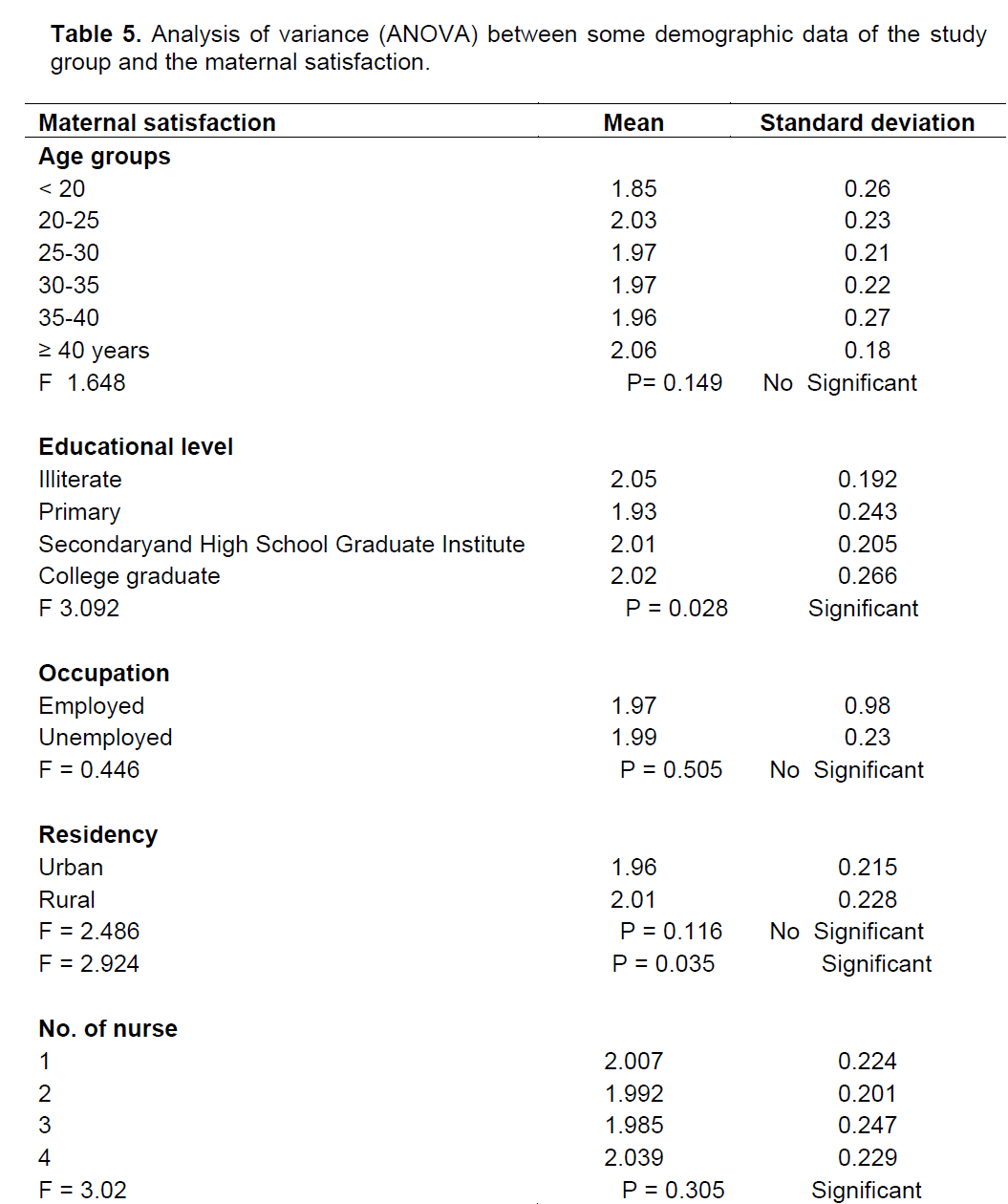
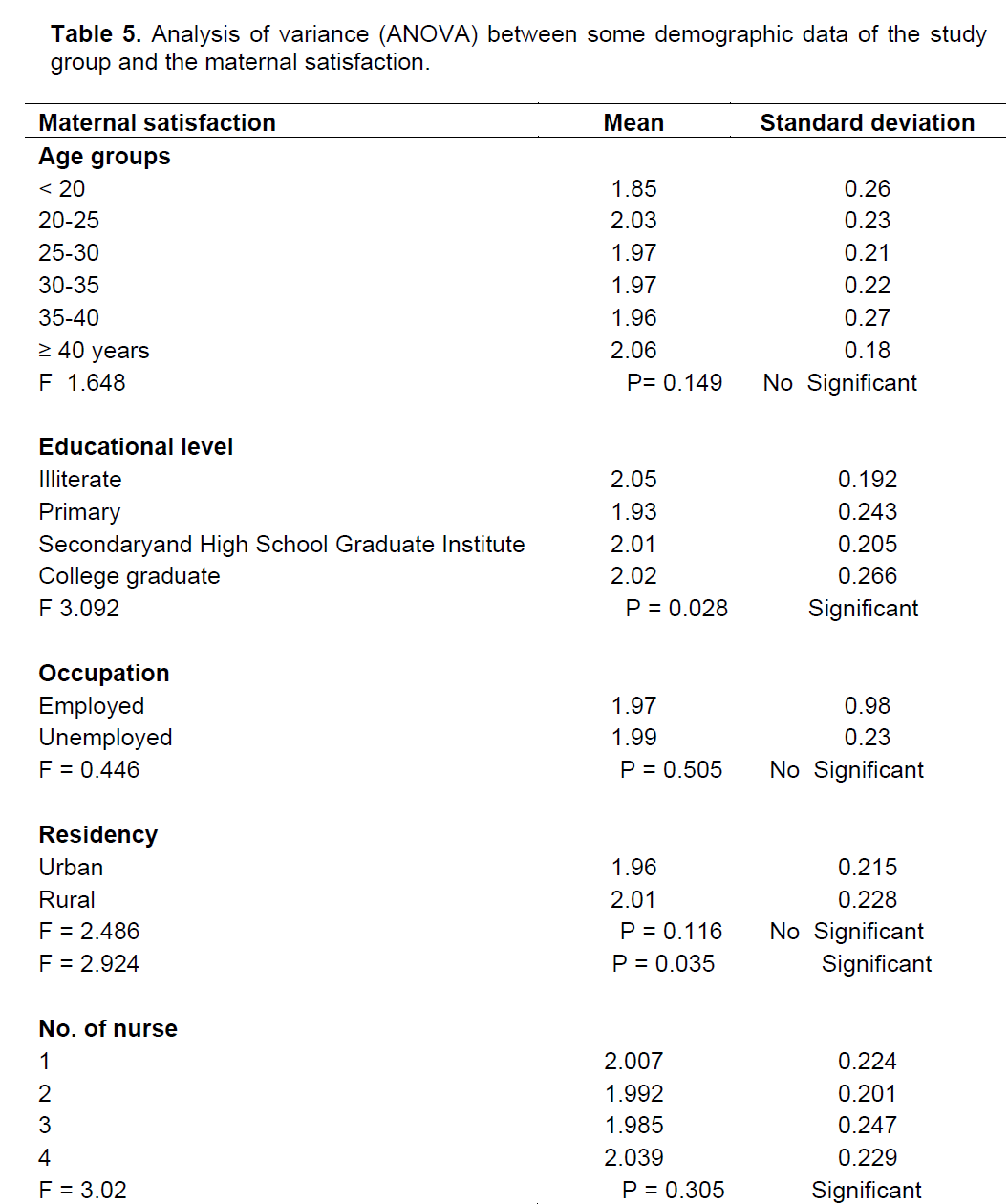
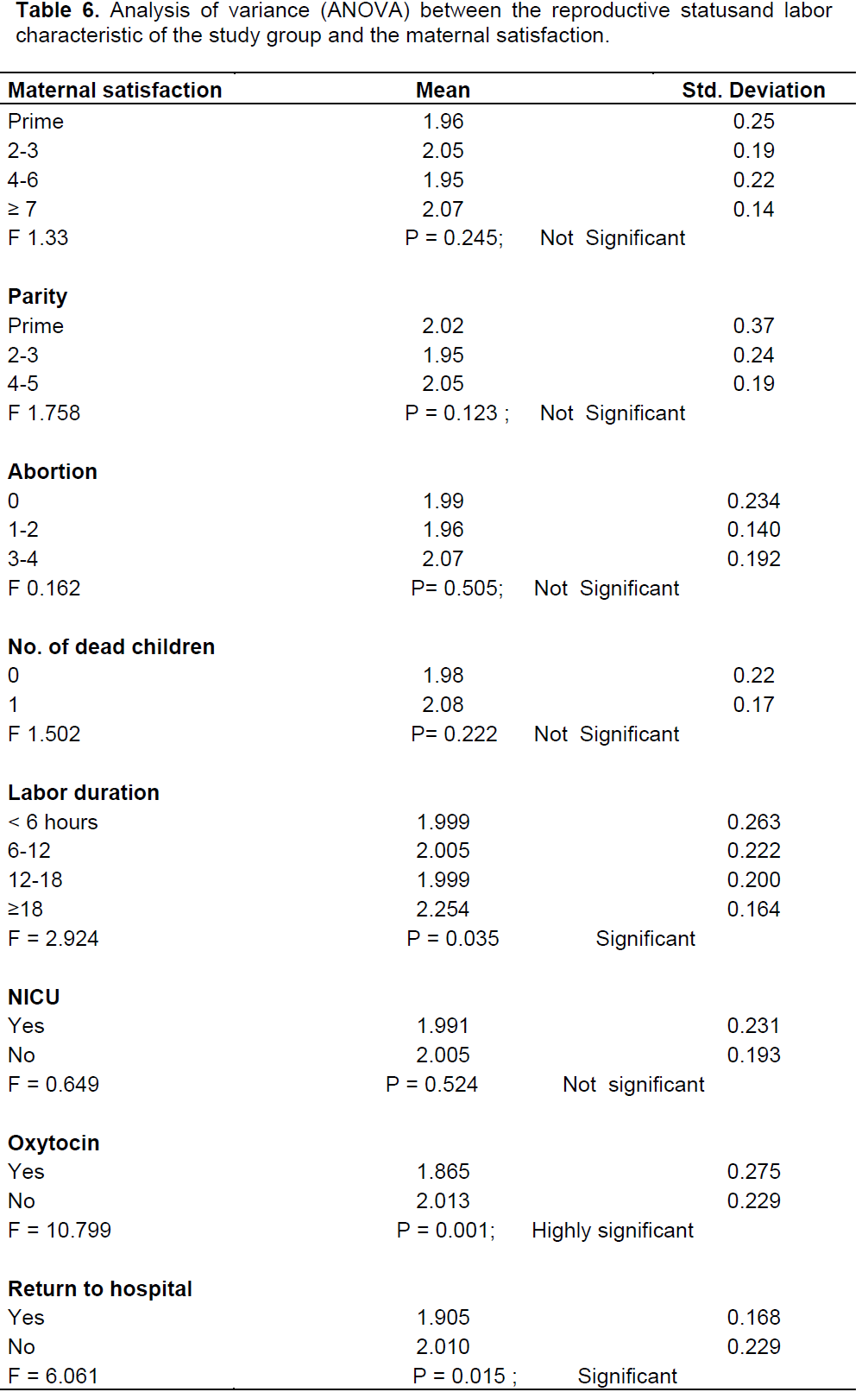
Table 6 indicates significant relationship between maternal satisfaction and some variables like educational level and number of nurses and maternal satisfaction regarding the quality of nursing care during her labor and delivery. Patient satisfaction with childbirth experience was not associated with parity, the experience of pregnancy and antenatal attendance were significant relationship with labor duration, returning back to hospital and highly significant relationship with giving Oxytocin was found.
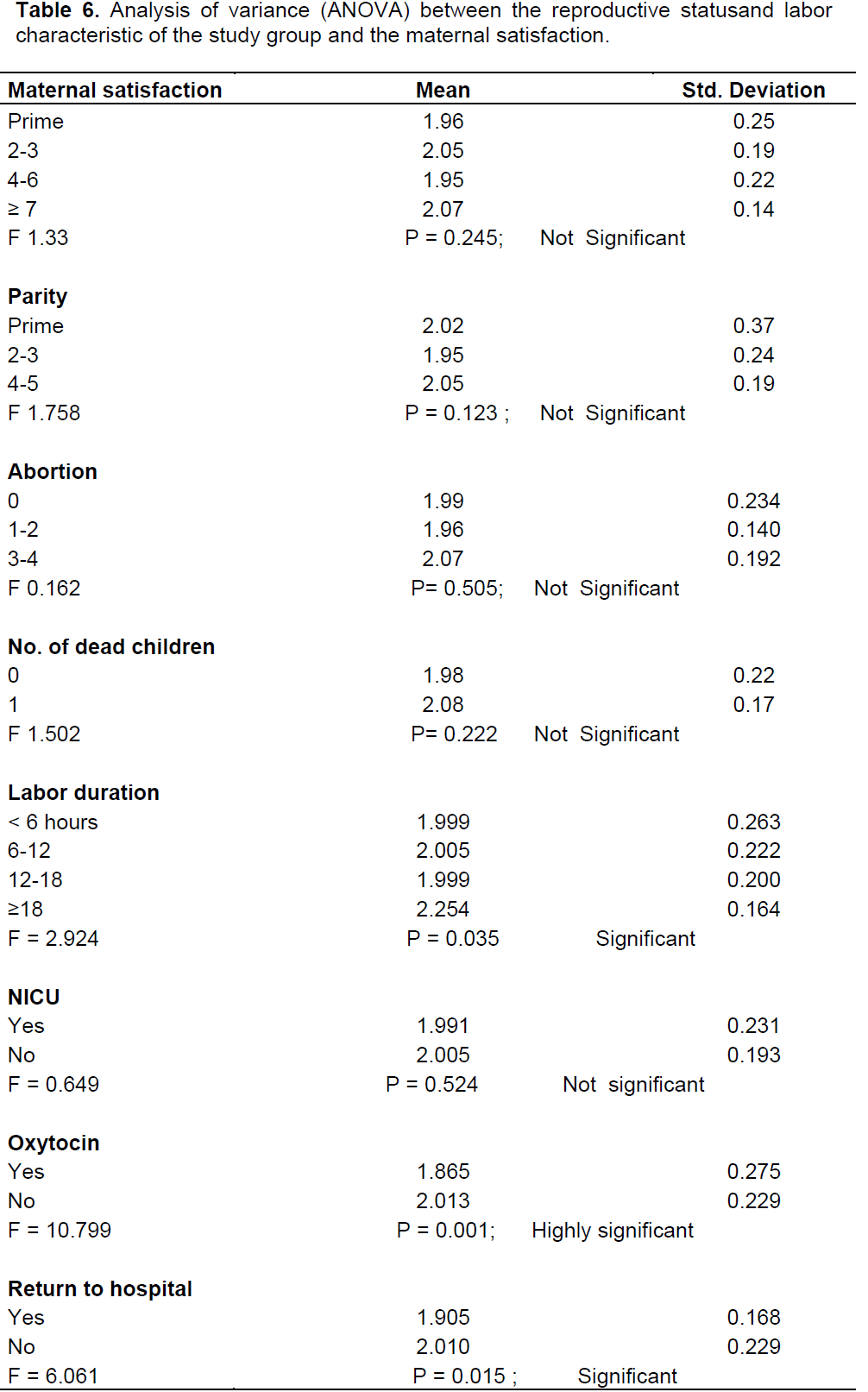
Table 7 shows that there was low mean of scores in most of the items regarding continuity category, including careers, identify themselves, welcomeing them and being present to the client all times during childbirth process, pain in labor and pain after delivery, they are expected to offer them more pain relief than they have during labour because they were on oxytocin for labour acceleration. While they were satisfied regarding their expectations of childbirth process, length, holding their baby, support from husband and their relative, in addition they were strongly satisfied regarding items related to professional support, environment and general satisfaction.
The study group has age ranged from 17 to 44 years, 35% of women were in the age group 20 to 25 years. As regards the educational level, it was found that 40.5% of them had primary school education. With regards to the educational status of the majority, more than three quarter of them (78.5%) were housewives and more than half of the women (56.5%) were living in rural areas As regards the demographic characteristics of the study sample, the results of the present study showed that more than three quarters of the women's age ranged between 20 to 35 years. This is anticipated because it is the normal age of childbearing. Lomoro et al. (2002) who investigated the mothers’ perspectives on the quality of postpartum care found that the mean age of mothers was 28 years (range 20 to 38).
In relation to the educational level, only 16% of the study sample were illiterate while most of them were educated which will help them to be able to identify their health needs and expectations during post partum period. In addition, education is a mean that enables women to gain access of knowledge and to control many events in their life. However, more than three quarters of women were housewives while slightly less than one fifth of them were working. This result insisted the need for complete pregnancy and postpartum health advices for these women because exposure to work outside the home gives women better chances of contact with a more experienced person and to acquire valuable health and social information. In addition, more than half of the women were living in rural areas while the rest were living in urban areas. This reflected women's needs for more health advices and extension of postpartum care services to the community where mothers are receiving care during home visits (Mohamed et al., 2012).
In addition, the present study found that majority (45%) of the women were primipara while the finding of previous study by Lomoro et al. (2002) mentioned that most of the mothers (90%; n = 45) were first para. This reflects women's needs for more support and assistance with baby care and their own personal care. Also, first para women experience certain physical health problems in the postpartum period that may affect their future health condition and the health of their children.
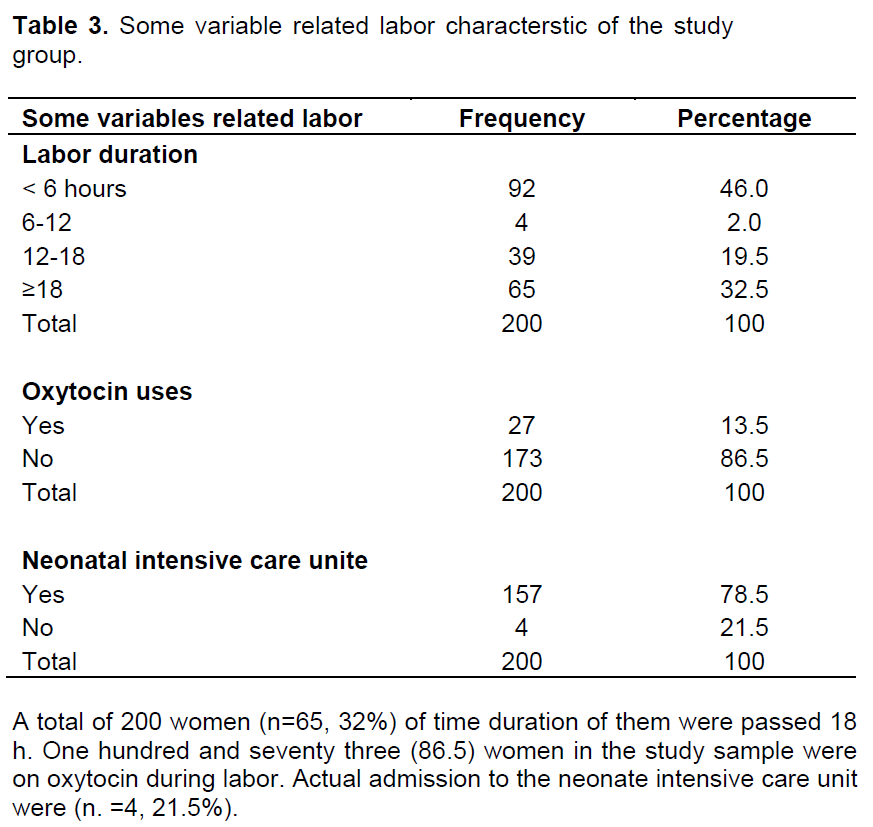
One hundred and seventy three (86.5) women in the study sample were on oxytocin during labor. Actual admission to the neonate intensive care unit were n. =4, 21.5%. In Maternity Teaching Hospital, policy allows mothers after birth tokeep their babies with them in baby friendly ward. While study done by Chunuan (2002) present Twenty-nine of the infants remained with their mothers for an hour after birth, and then were moved to the normal nursery for assessment and bathing. Only 1 infant was moved to the high-risk nursery immediately after birth for suspected complication. Relation between demographic and maternal satisfaction (Lomoro et al., 2002) stated that women with higher education level who had childbirth preparation and expectations for labor, had higher global satisfaction with the childbirth experience. In contrast, Rochanaroon (1998) reported that age and patient satisfaction with the antenatal care experience were positively related and educational level was negatively associated with patient satisfaction with the antenatal and the intrapartum care (Lomoro et al., 2002).
Women who had childbirth preparation and expectations for labour had higher global satisfaction with the childbirth experience (Goodman et al., 2004). Vanasuvanich (1995) found that the residency and career of patient were associated with patient satisfaction with nursing care. However, age, educational level, marital status, family income, type of family, parity, gestational age, and different prenatal care providers were not associated with patient satisfaction with nursing care received during the intrapartum period (Lomoro et al., 2002).
Regarding postpartum women’s satisfaction
These findings indicated that the women were satisfied with their care during labor and delivery. However, in the study opinion reason return to several factors, first, because of the arrival of a healthy baby and giving birth to a healthy baby may balance for any negative experience, second In addition, the timing of assessment, patient satisfaction may affect the subjects answers and third reason hospitalized postpartum women may feel hesitant to criticize the care they received because their health care providers were still involved.
Based on Brown and Lumley (1994) study, two-third of the subjects reported that their intrapartum care was managed in the they want it, while 27% stated that their care was mixed, and 6% of the subjects did not like the care they receive. Banthurng et al. (1992) found that most of the postpartum women (82.4%) were highly satisfied with services provided by nursing students, and 13.8% of the postpartum women were moderately satisfied with services provided by nurses.
Behaviours that reflect positive attitudes towards clients, such as being patient with clients, politeness, not shouting at them and not belittling them, along with a good level of competence, are important for patient satisfaction. These findings agree with that found by Jewkes et al. (1998) in a study on ‘why do nurses abuse patients’. Their respondents reported that ‘nice nurses’ were those who explained procedures and did not shout at or speak rudely to women. Another factor that determined satisfaction with care was the characteristics of the setting, for example the availability of human andmaterial resources.
Findings revealed that client’s sources of dissatisfaction include negative behaviors of caregivers (ineffective communication, neglect and unfriendliness) such as shouting at them; ignoring them, frowning at them, belittling them, and whispering among caregivers that make clients uncomfortable.
Also, other sources of dissatisfaction include characteristics of the hospital setting, which include the non-availability of human and material resources, such as infrastructure, staffing and financial problems. In addition, clients did not understand their hospital bills and this made them dissatisfied with the hospital because they felt they were being exploited. In contrast, in this study, women are not complaining about this issue because all health services in Kurdistan reign are free they are paying nothing.
This study argued that this could be because 55% of the study sample were multiparous, and did not need help as regards the care of the baby. Patients indicated that they perceived the abuse they received to be aninseparable part of the procedures and methods of working on the midwife unit. Jewkes et al. (1998)
and Martin, 2005) reported from their study that most women expects that they would have problems delivering in the hospital setting again as they could be shouted at, beaten or neglected. These comments were largely based on previous personal experience, or that of friends.
This would reduce the length of interaction with the staff of the hospital, reduce the stay in hospital and consequently the need for intervention, and decrease cost to the woman. The results of this study are consistent with that of Mwaniki et al. (2002) and Field (1982) who reported that the delay in admission to a health facility once mothers are on labour, lack of satisfaction with quality of care given (shortage of drugs and essential supplies, unfriendly staff who were not committed to their work and lack of cleanliness in the health facility) are major demotivating factors in the use of health facilities for maternity services.
The main factors identified as influencing satisfaction and dissatisfaction were, caregivers and client interaction, the characteristics of the setting, the involvement of clients in the caring process, the nurses’ perception of client characteristics, the outcome of labour for both mother and baby, the acceptability of alternative places for delivery, and the respondents’ expectations and perceptions of hospital delivery. Of all these factors, however, caregiver attitude was seen as the strongest factor in determining maternal satisfaction with care. All respondents mentioned that if the interpersonal relationships with their caregivers were good (politeness, kindness, and patience), then they were satisfied with their care even when other factors were not addressed. If a positive caregiver attitude was attained, the client found the hospital safe enough for future use. On the other hand, if the hospital was not found to be safe enough because of negative attitudes such as shouting, ignoring or whispering, this led to plans not to use the hospital in future. However, if
the client did not find a safer alternative to hospital delivery (baby and mother), she then planned to use the hospital again as a last resort by reporting very close to second stage of labour, and eventually recommendeing the hospital to her family and friends.
1. To improve satisfaction with nursing care, accessibility housekeeping, and availability of resources should be in high quality.
2. As a major component of health care services, nurses need to deal with the quality of structure of care to improve quality of nursing care. The nurse also needs toevaluate women’s stress during the intrapartum period because the level of stress predicted patient satisfaction with nursing care.
3. To reduce their stress during the intrapartum period, the nurse has to make the environment conduesive by supporting the women.
4. Further studies should be conducted in other health care settings such as teaching hospitals or private hospitals because health care delivery and the structure of care vary by types of hospital.
5. Staffs of the hospital should have frequent education on communication and interpersonal relationship.
6. Caregivers need to fully understand the expectations that patients have in their care, and provide care that is consistent with those expectations.
7. The community members should be educated on hospital delivery and the need to report to the hospital early in labour.
8. Open-ended questions may also be better than Likert-scale questionnaires in assisting patients to describe their
feelings towards nursing care they received during the intrapartum period.
9. The study may be replicated on a larger sample. A comparative study may be undertaken between a hospital catering to rural population and a hospital catering to urban population. Similar study may be conducted to find the level of satisfaction between Primiparae and multiparae mothers in maternity wards.
The authors have not declared any conflict of interests.
REFERENCES
|
American Academy of Family Physicians (AAFP) (2013). Quality Patient Care in Labor and Delivery: A Call to Action.
View
|
|
|
|
Banthurng W, Thaenpichet S, Pakthop M, Prasopkittikun T (1992). Parturients satisfaction toward nursing services, faculty of nursing, Srinakharinwirot University. Thai. J. Nurs. 41:129-148.
|
|
|
|
Bear M, Bowers C (1998). Using a nursing framework to measure client satisfaction at a nurse-managed clinic. Public Health Nurs. 15(1):50-59.
Crossref
|
|
|
|
Bradley C, Brewin CR, Duncan SL (1983). Perception of Labour: Discrepancies between midwives and patients' ratings. Br. J. Obstet. Gynaecol. 90(12):1176-1179.
Crossref
|
|
|
|
Brown S, Lumley J (1994). Satisfaction with care in labor and birth: A survey of 790 Australian women. Birth 21(1):4-13.
Crossref
|
|
|
|
Chunuan SK (2002). Patient satisfaction with health care services received during intrapartum in one regional hospital in the southern part of Thailand.
|
|
|
|
Chwinui N (2010). Patient satisfaction with intrapartum and postpartum nursing care. Memoire Online.
View
|
|
|
|
Dzomeku MV (2001). Maternal Satisfaction with care during labour: A case study of Mampong-Ashanti district hospital maternity unit in Ghana. Int. J. Nurs. Midwifery 3(3):30-34.
|
|
|
|
Fakhoury WK (1998). Satisfaction with palliative care: What should we be aware of? Int. J. Nurs. Stud. 35(3):171-176.
Crossref
|
|
|
|
Field PA (1982). Client care seeking behaviours and sources of satisfaction with nursing care. Nursing. Nurs Pap. 14(1):15-29.
|
|
|
|
Mohamed HAEA, El Ngger N, Lamadah SM (2012). Women'perspectives regarding the quality of postpartum nursing care In Ain Shams Maternity Hospital–Cairo, Egypt. J. Am. Sci. 8(2):366-377.
|
|
|
|
Jewkes R, Abrahams N, Mvo Z (1998). Why do nurses abuse patients? Reflections from South African Obstetric services. Soc. Sci. Med. 47(11):1781-1795.
Crossref
|
|
|
|
Johansson P., Oléni M., and Fridlund B.(2002): Patient satisfaction with nursing care in the context of health care: a literature study. Scand. J. Caring Sci. 16:337-344.
Crossref
|
|
|
|
Linder-Pelz SU (1982). Toward a theory of patient satisfaction. Soc. Sci. Med. 16(5):577-82.
Crossref
|
|
|
|
Lomoro OA, Ehiri JE, Qian X, Tang SL (2002). Mothers' perspectives on the quality of postpartum care in Central Shanghai, China. Int. J. Qual. Health Care 14(5):393-401.
Crossref
|
|
|
|
Martin M (2005). Women's judgments and attitudes about the quality and quantity of postpartum teaching. Parity 14(13):52.
|
|
|
|
Rochanaroon D (1998). Satisfaction of clients to pregnancy taking care service before and after delivery in Chonburi Hospital. J. Nurs. Assoc. Thailand Eastern Region. 20:26-31.
|
|
|
|
Vanasuvanich C (1995). Satisfaction of pregnant Moslem women during labour in Pattani Hospital. Unpublished research, Pattani, Thailand, 1995.
|