Full Length Research Paper

ABSTRACT
Admission of a new born to the Neonatal Intensive Care Unit (NICU) is a stressful and unexpected event to most parents. This quantitative study aimed at identifying factors that contribute to stress in mothers nursing babies in the NICU at the Women and New Born Hospital in Zambia. A cross sectional study was conducted among 280 mothers who were randomly selected over a three-month period. Stress levels were assessed using Parental Stressor Scale: Neonatal Intensive Care Unit (PSS: NICU) questionnaire. Informed consent was obtained from the mothers for the study. Inclusion criteria for the study were mothers of admitted neonates and their neonates who had to remain in the NICU for at least 24 h. Stata software version 13 was used to analyse data Chi square test to determine association between stress and maternal and infant characteristics. Kruskal wallis test was used to determine association between subscales of the PSS: NICU tool and interquartile and median were calculated since the data was not normally distributed. Results revealed that participants were more stressed by alteration of the parental role and the appearance and behaviour of their neonate. All participants rated admission of the neonate as being stressful. Maternal characteristics that were associated with stress included education level and duration of stay in Kruskal-Wallis test showed a statistical difference between the stress subscales with alteration of parental role being the most stressful subscale. Mothers have different stress levels with most of them experiencing moderate and extreme stress; appropriate counselling targeted towards specific stressors identified is required. The limitation of this study is that it did not monitor levels of stress at different times of admission Future research should monitor how maternal stress changes throughout the neonate’s NICU stay. This information can be used to design effective support programme to help mothers adopt coping strategies during their infant’s hospitalization.
Key words: Maternal stressors, neonatal intensive care, Stressor Parental Stressor Scale: Neonatal Intensive Care Unit (PSS: NICU).
INTRODUCTION
The Neonatal Intensive Care Unit (NICU) is a particularly challenging environment for new mothers as several natural processes are disrupted (Williams et al., 2018). NICU is completely different from that anticipated when they discovered they were pregnant and began planning for the eventual birth (Williams et al. 2018). According to Turner et al. (2015), the experience of being a parent of a neonate in the NICU is stressful and the effects of the NICU experience may continue beyond the acute admission.
Busse et al. (2013) indicated that parental stress emanating from the NICU experience influences parenting behaviour as well as producing long term emotional problems and health alteration. Wigert et al. (2013) emphasised that the NICU experience is a complex one in which strong emotions are evoked from families who must depend on professionals who were strangers prior to the infant’s admission. Medical professionals care for the infant in the NICU while the majority of families often have a limited role to play. Entrusting the lives of their babies in medical personnel who are tasked to take care of more than one infant could be one of the reasons that may contribute to the stress experienced by the mothers. In the family circle, the birth of a child requires some adjustments in family life and routines. Therefore, a neonate with a condition that requires neonatal intensive care is more challenging. When an infant is admitted to the NICU, the parents are confronted with the critical care environment and all its associated demands (Obeidat et al., 2009).
The NICU environment is full of staff, machines, and ill infants. As a result, this technological environment creates an intimidating atmosphere, with mothers reporting feeling overwhelmed (Johnson, 2008).
Parents who are unfamiliar with the NICU environment and how to care for the infant become distraught, worried, and anxious. The lack of emotional support and physical preparation for NICU admission combined with overwhelming concern on the safety and comfort of their babies increase the stress levels in mothers. The purpose of this particular investigation is to explore the perceptions of mothers of infants admitted to a level III NICU in Lusaka, Zambia elucidating stressful features of the NICU environment.
METHODOLOGY
Study design
A cross sectional, quantitative study design which involved mothers and their neonates admitted to the Women and New born hospital of the University Teaching Hospital (UTH) in Lusaka district, Zambia was conducted. The inclusion criteria required women who had spent at least 24 h and more in the NICU at UTH. The time spent in other health facilities was not considered as inclusion criteria. The mothers whose neonates were born with congenital abnormalities that were severe to survive extra uterine environment were excluded from the study. A systematic sampling technique involving drawing a list of all mothers who met the inclusion criteria each, and present in the NICU on the day of data collection was used. Every second woman was selected and invited to participate in the study. Those who consented to participation were then interviewed. Approximately five women were interviewed by each data collector on each day until the desired sample size of 280 women was reached. Consent was also obtained from the mother to access information on their admitted infant from the hospital file.
Data collection
The data were collected using PSS: NICU (Miles et al., 1993) interview schedule with five subscales for including; sights and sounds, Infant appearance and behaviour, alteration in the parental role and staff behaviour, and communication and general stress. The responses to the PSS: NICU were scored on a 5-point Likert scale ranging from 1 point for “not at all stressful”, 2 points for “mild stress”, 3 points for “fairly moderate stress”, and 4 points for “very stressful” and 5 points for “extreme / severe stress”. Higher scores indicated more stress. A maternal and infant information sheet was also used to collect the data on maternal and infant characteristics. The data collection tools were tested for reliability and validity using the Cronbach alpha since it had never been used in Zambia. The result showed a Cronbach alpha of 0.96 which meant the tool was reliable and highly valid to measure stressors in NICU among the mothers.
Ethical considerations
Ethical approval to conduct the study was granted by the University of Zambia Biomedical Research Ethics Committee (UNZABREC) and the Ministry of Health National Health Research Authority (NHRA). Permission to conduct the study was also obtained from the Medical Superintendent at the Women and New born hospital and Lusaka provincial health office. The purpose of the study and issues of confidentiality and anonymity were explained to the respondents and upheld throughout the study. Informed consent was thereafter obtained from all participants.
Data analysis
Data from the interview schedule were analysed using the Stata software version 13. For descriptive statistics, Mean, median and interquartile range for continuous variables and frequencies for categorical variables were calculated. Normality test was done using Shapiro wilk test, since variables were not normally distributed median, interquartile range was used for descriptive statistics and Kruskal Wallis test was used to test for significant among the stress subscale. Chi square was used to test for association between the independent and dependent variables.
RESULTS
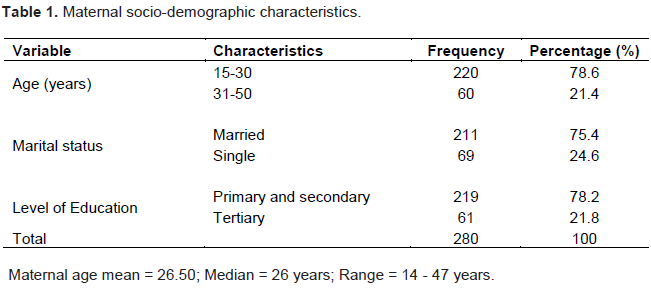
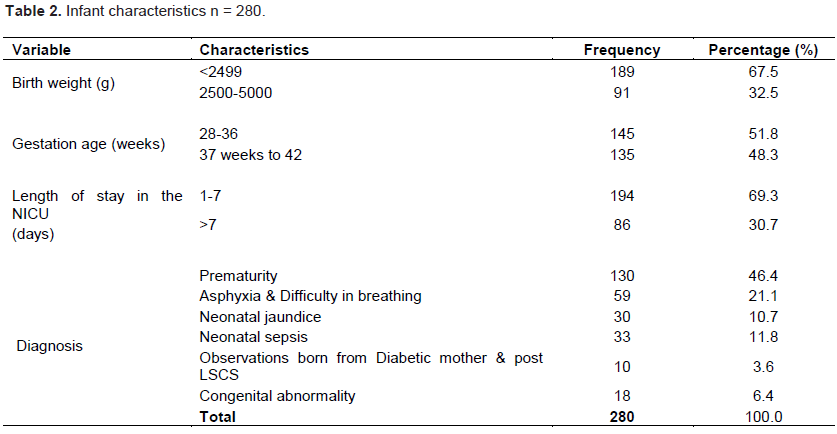
The sample of mothers (N=180) were interviewed using a PSS: NICU tool, a 46 item scale that measures stressors in the NICU environment. In addition, the mothers completed a demographic tool on maternal and infant characteristics for the stressors identified in the review of literature. Data was coded and chi-square were used to determine relationships related to stress and demographics (Table 1). The majority of the respondents were between 15 and 30 years old (78.6%). The median age was 26 years. The majority (75.4%) were married and 24.6% were single. Most of the respondents were in a relationship with their present partner for less than 5 years (70%) and 96.1% of those partners were the biological fathers of the babies they were nursing in NICU. Majority of the respondents (78.2%) attained primary or secondary school education and 21.8% attained tertiary education (Table 2). There were 280 babies included in the study on the basis that the mother was selected to participate. For some mothers (7.2%) who had multiple delivery, only the first twin was included. The baby’s characteristics were recorded from the medical record with consent from the mothers. According to Table 2, most of the babies (67.5%) weighed between 1 and 2.4 kg at birth. The mean birth weight was 2.07 and range was 0.70 to 3.80 kg while the mode was 1.20 kg. About half of them (51.8%) were born prematurely between 28 and 36 weeks gestation age. Only 30% of the babies had spent more than seven days in the NICU at the time of data collection. The mean was 7 days and the range was one to 90 days of admission in the NICU.
Maternal stress
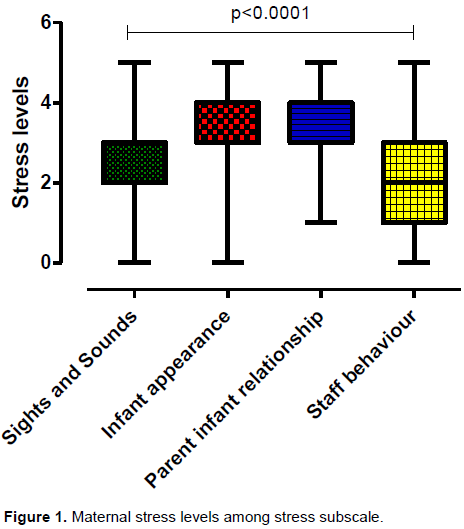
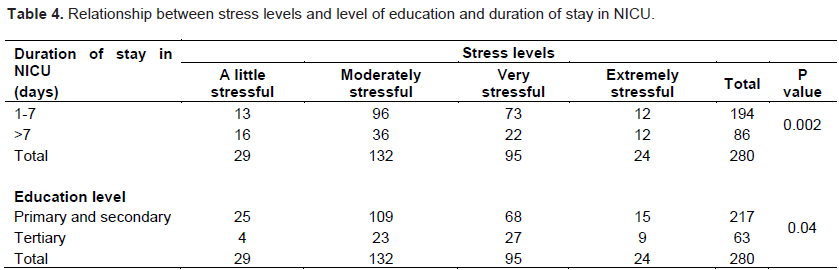
Figure 1 shows a statistical difference in the stress subscale (P value 0.001) with infant appearance and behaviour and parent infant behaviour having the high stress levels. Stress experienced on each subscale was quantified using Likert scale of one to five with five being extremely stressed and Metric 1 scoring method. The results in Table 3 indicate that mothers experienced stress from having their infants cared for in the NICU. The median score for general stress of having an infant admitted in NICU was 4.50 with the total being five. The median scores for the subscales sights and sounds, infant appearance and behaviour alteration in the parental role and staff behaviour and communication were (2.00), (3.00), (4.00) and (2.00) respectively. The highest levels of stress experienced were in the subscales of parental infant relationship and regarding the infant’s physical appearance and behaviour. Table 4 shows a statistically significant relationship between stress experienced by the mothers and duration of stay in the NICU (P value = 0.002) and educational level (P- Value = 0.04).

DISCUSSION
Having a new born infant hospitalised in the NICU is an unexpected and stressful event for a family (Busse et al., 2013). The purpose of the study was to determine the stress levels among mothers of babies admitted in NICU and to identify demographic parameters that influence their stress levels. This current study found that duration of stay in NICU (P value 0.002) and educational level of the mother were associated with stress levels experienced by the mother (P value 0.04).
Chourasia et al. (2013) reported increased stress levels in older mothers, while Woodward et al. (2014) and Carter et al. (2007) reported stress in unmarried, low-income and less-educated mothers, as well as in younger, married mothers with high levels of education. These studies suggest that parental stress levels in the NICU may be influenced by several demographic factors and clinical variables related to both the mother and the infant.
However, other studies report no association between heightened levels of stress and maternal demographics, such as age, marital status, education or employment status (Dudek-Shriber, 2004; Meyer et al., 1995; Frank et al., 2005). The difference in these studies could the study settings in which these studies were conducted and differences in their cultural beliefs. Different cultures attach different values in most of these demographics that were being studied. In the Zambian setting where most mothers reported that they were not given any information on prognosis of their admitted infant, high stress levels among those with high education level could be due to the fact that these mothers could read literature related to condition of their baby.
The extent of prematurity and illness severity of the infant have been shown to be predictors of increased levels of maternal stress, with the extent of prematurity said to be associated with either more or less complications (Vwalika et al., 2017). It is therefore assumed that babies born with a lower gestation age have less chances of survival. This could be the reason for increased stress levels in mothers in relation to the infant appearance. Those mothers with healthy premature infants could be assured of high likelihood of survival and reduced complications, and therefore, reduced stress. Most respondents were generally stressed with having an infant admitted in NICU (stress median score 4.00). The situations mothers described as very stressful in this research were the infant appearance (median score 3.00) and behaviour and parent infant relationship (Table 3).
The results of this study are in agreement with Browne and Talmi (2005); Nugent et al. (2007) and Gale et al. (2003), who revealed that the most common stressor of families with infants admitted is physical appearance of the infant. The current study has revealed that most of the babies admitted in the NICU were premature (46%). Literature shows that babies born prematurely do not have a physical appearance like one who is born at term and they do behave differently as they usually have apnoeic spells which could worry mothers who may not understand. Their appearance has been said to contribute to the stress experienced by their mothers. This finding concurs with findings of previous studies that also demonstrated that the primary sources of stress identified by NICU mothers are related to their infant’s behaviour, appearance and their parental role, whereas the perception of the NICU environment appears to affect mothers to a lesser degree (Busse et al., 2013; Chourasia et al., 2013; Dudek-Shriber, 2004).
De Rouck and Leys (2009) reported that the feeling of disruption of the parental role contributes greatly to the amount of stress experienced by parents of infants in NICU. More other previous studies are consistent in their findings and assert that change in parental roles is an important aspect behind parental stress in NICU settings (Musabirema et al., 2015; Carter et al., 2007; Dudek-Shriber, 2004; Lau and Morse, 2007; Preyde and Ardal, 2003; Shaw et al., 2006). Interaction between parents and their infants is regarded as a crucial activity that has a significant impact on the parental care of a child, and therefore, it directly relates to parental roles in NICU settings. Shaw et al. (2006) explore the influence of psychological distress amongst parents of infants in a NICU and report a strong correlation between severe acute stress disorder and parental role alteration. Another source of stress for mothers documented by Phillips and Tooley (2005) is the distress they often feel when they do not see, touch, or are not in close proximity of their babies. Therefore, understanding possible factors associated with parental stress is a fundamental principle for providing quality care that responds to the parents’ needs in such a way that it reduces stress and anxiety in a NICU.
This study has revealed that most of the respondents experienced a lot of stress (median score 4.00) arising from having their baby admitted to NICU. Assel et al. (2002) concluded that parental stress, even at low levels, has been shown to disturb the relationships of parents with their healthy infants. This finding is consistent with what other researchers documented on stress being one of the most common barriers to effective parenting and yet one of the most important predictors of the developmental outcome of the infant (Umasankar and Sathiadas, 2016; Hall et al., 2015; Hildingsson and Thomas, 2014; Shaw et al., 2006). In addition, the distress that these parents experience has been noted to influence their parenting behaviour (Lefkowitz et al., 2010) and can affect the long-term relationship with their children and their ability to take care of them.
The findings of this study are not consistent with the findings of Stacey et al. (2015) and Harvey (2010) who reported that when parents are not provided with communication and information about the needs, care, and physical appearance of their infants, their stress levels increase tremendously. Results of this study revealed that most mothers did not get any information on the prognosis of their child but this construct was not significant in increasing their stress. Which is also consistent with findings of Charchuk and Simpson (2005), who found that the parents of an infant admitted to the NICU face challenges including access to information, disclosure about the diagnosis, and treatment and prognosis of their newborn.
This study with regard to mothers experiences on the sights and sounds in the NICU, most of them reported low stress levels. These results are contrary to findings of Turan et al. (2008) and Johnson (2016) and who reported that the technological environment of the NICU creates an intimidating atmosphere and mothers report that they often feel overwhelmed and stressed. Parents who are unfamiliar with the NICU environment and how to care for the infant become distraught, worried, and anxious. They often might perceive that their infant is in pain and do not understand the NICU procedures. The hospital environment is unfamiliar and parents are dependent on doctors and nurses to be able to cope with their situation (Wigert et al., 2013). When members of staff are able to answer the parents’ question it has been found that it lessens the parents’ stress because knowledge can easy uncertainty.
CONCLUSION
This study has provided important information for nurses and midwives who are working at the NICU in Zambia. Identifying the stressors in NICU can assist nurses in intervention planning to reduce stress and find ways of supporting stressed mothers. Implementing policies like Family-Centered Care that address stressors concerning their roles and their understanding of their infant would address a significant cause of stress for mothers. Future research should identify strategies and effective coping mechanisms that would assist with preventing or reducing stress for mothers when their infants are admitted to a NICU.
Implications of the study
The result of this study implies that nurses working in the NICU need to give more information to the mothers for them to understand the physical appearance of their babies. The mothers should also be involved more in the care of their babies while they are admitted. The ï¬nding of high general stress suggests that it is important for nurses to determine more precisely what the speciï¬c stressors are so that their intervention protocols can better address each parents’ needs, reduce their stress, and enhance their ability to understand and cope with their infant.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
We would like to acknowledge the financial support provided by the Norwegian agency for Development (NORAD) through the NORHED QZA -0848 QZA-MW-13/00032 Grant to conduct this study.
REFERENCES
|
Assel M, Landry S, Swank P, Steelman L, Miller-Loncar C, Smith K (2002). How do mothers' childrearing histories, stress and parenting affect children's behavioural outcomes? Child: Care, Health and Development 28(5):359-368. |
|
|
Browne J, Talmi A (2005). Family-based intervention to enhance infant-parent relationships in the neonatal intensive care unit. Journal of Pediatric Psychology 30(8):667-677 |
|
|
Busse M, Stromgren K, Thorngate L, Thomas KA (2013). Parents responses to stress in the neonatal intensive care unit. Critical Care Nurse 33(4):52-60. |
|
|
Carter JD, Mulder RT, Darlow BA (2007). Parental stress in the NICU: the influence of personality, psychological, pregnancy and family factors. Personality and Mental Health 1(1):40-50. |
|
|
Charchuk M, Simpson C (2005). Hope, disclosure, and control in the neonatal care unit. Health Communication 17(2):191-203. |
|
|
Chourasia N, Surianarayanan P, Adhisivam B, Vishnu BB (2013). NICU admissions and maternal stress levels. The Indian Journal of Pediatrics 80(5):380-384. |
|
|
De Rouck S, Leys M (2009). Information needs of parents of children admitted to a neonatal intensive care unit: A review of the literature (1990-2008). Patient Education and Counseling 76(2):159-173. |
|
|
Dudek-Shriber L (2004). Parent stress in the neonatal intensive care unit and the influence of parent and infant characteristics. The American Journal of Occupational Therapy 58(5):509-520. |
|
|
Frank LS, Cox S, Allen A, Winter I (2005). Measuring neonatal intensive care unit-related parental stress. Journal of Advanced Nursing 49(6):608-615. |
|
|
Gale G, Franck LS, Kools S, Lynch M (2003). Parents' perceptions of their infant's pain experience in the NICU. International Journal of Nursing Studies 41(1):51-58. |
|
|
Hall S, Hynan N, Phillips R, Press J, Kenner C, Ryan DJ (2015). Development of program standards for psychosocial support of parents of infants admitted to a neonatal intensive care unit: A national interdisciplinary consensus model. Newborn and Infant Nursing Reviews 15(1):24-27. |
|
|
Harvey E (2010). The experiences and perceptions of fathers attending the birth and immediate care of their baby. Doctoral dissertation, Aston University. |
|
|
Hildingsson I, Thomas J (2014). Parental stress in mothers and fathers one year after birth. Journal of Reproductive and Infant Psychology 32(1):41-56. |
|
|
Johnson AN (2008). Promoting maternal confidence in the NICU. Journal of Pediatric Health Care 22(4):254-257. |
|
|
Johnson AN (2016). Stress beyond the neonatal intensive care unit (NICU) discharge: Implications to outcome. Pediatrics and Neonatal Nursing - Open Journal 3(1):15-19. doi: 10.17140/PNNOJ-3. |
|
|
Lau R, Morse CA (2007). Stress experiences of parents with premature infants in a special care nursery. Stress and Health: Journal of the International Society for the Investigation of Stress 19(2):69-78. |
|
|
Lefkowitz D, Baxt C, Evans J (2010). Prevalence and correlates of posttraumatic stress and postpartum depression in parents of infants in the neonatal intensive care unit (NICU). Journal of Clinical Psychology in Medical Settings 17(3):230-237 |
|
|
Meyer EC, Garcia CT, Seifer R (1995). Psychological distress in mothers of preterm infants. Journal of Developmental and Behavioral Pediatrics. |
|
|
Miles MS, Funk SG, Carlson J (1993). Parental stressor scale: neonatal intensive care unit. Nursing Research 42(3):148-52. |
|
|
Nugent JK, Keefer CH, Minear S, Johnson L, Blanchard Y (2007). Understanding newborn behavior and early relationships. The Newborn Behavioral Observations (NBO) System Handbook. |
|
|
Obeidat HM, Bond EA, Callister LC (2009). The parental experience of having an infant in the new born intensive care unit. The Journal of Perinatal Education 18(3):23. |
|
|
Musabirema P, Brysiewicz P, Chipps J (2015). Parents perceptions of stress in a neonatal intensive care unit in Rwanda. Curationis 38(2):1-8. |
|
|
Phillips SJ, Tooley GA (2005). Improving child and family outcomes following complicated births requiring admission to neonatal intensive care units. Sexual and Relationship Therapy 20(4):431-442. |
|
|
Preyde M, Ardal F (2003). Effectiveness of a parent "buddy" program for mothers of very preterm infants in a neonatal intensive care unit. Cmaj 168(8):969-973. |
|
|
Shaw R, Deblois T, Ikuta L, Ginzberg K., Fleisher B, Koopman D (2006). Acute stress disorder among parents of infants in the neonatal intensive care nursery. Psychosomatics 47(3):206-212. |
|
|
Stacey S, Osborn M, Salkovskis P (2015). Life is a rollercoaster… What helps parents cope with the Neonatal Intensive Care Unit (NICU)? Journal of Neonatal Nursing 21(4):136-141. |
|
|
Turan T, Basbakkal Z, Ozbek S (2008). Effect of nursing interventions on stressors of parents of premature infants in neonatal intensive care unit. Journal of Clinical Nursing 17(21):2856-2866. |
|
|
Turner M, Chur-Hansen A, Winefield H, Stanners M (2015). The assessment of parental stress and support in the neonatal intensive |
|
|
Umasankar N, Sathiadas M (2016). Maternal stress level when a baby is admitted to the neonatal intensive care unit at Teaching Hospital Jaffna and the influence of maternal and infant characteristics on this level. Sri Lanka Journal of Child Health 45(2). |
|
|
Vwalika B, Marie CD, Mwanahamuntu MK, Cherry L, Kaunda E, Tshuma GG, Somwe W, Ahmed Y, Elizabeth MY, Stringer J, Stringer SA, Benjamin H (2017). Maternal and newborn outcomes at a tertiary care hospital in Lusaka, Zambia 2008-2012. International Journal of Gynecology and Obstetrics 136(2):180-187. |
|
|
Wigert H, Dellenmark MB, Bry K (2013). Strength and weakness of parent - staff communication in the NICU: A survey assessment. BMC Pediatrics 13.1(2013):71. |
|
|
Williams KG (2018). The neonatal intensive care unit: Environmental stressors and supports. International Journal of Environmental Research and Public Health 15(1):60. |
|
|
Woodward LJ, Bora S, Clark CA (2014). Very preterm birth: maternal experiences of the neonatal intensive care environment. Journal of Perinatology 34(7):555. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


