ABSTRACT
Late booking for antenatal care is a frequent occurrence among pregnant women in Nigeria unlike in most developed countries. The objective of the study was to determine the maternal, socio-cultural, religious, and institutional/systemic factors that determine late booking for antenatal care among pregnant women in Enugu, Nigeria. Descriptive, cross-sectional questionnaire based method was employed in the study. A proportionate stratified sampling technique was used to select 282 pregnant women from three selected hospitals for the study. A validated structured questionnaire constructed by the researchers was used for collection of data. Findings were analysed using both descriptive and inferential statistics. Respondents revealed that maternal factors such as health status in present pregnancy [205(70.7%)], ignorance of proper gestational age to register for antenatal [125(43.1%)] and experience from previous pregnancies [101(34.8%)] determine timing of booking among pregnant women. Socio-cultural factors such as husband’s decision [100(34.5%)] and preference for mother in-law/friends/other women’s advice during the early weeks of pregnancy [88(26.9%)] determine timing of booking. Religious factor which mostly determine late booking in the study was preference for prayer and faith healing [157(54.1%)]. Institutional/systemic factors such as long waiting time in hospitals [142(49.0%)] and very frequent antenatal care schedule [129(44.5%)] determine late booking for antenatal care among pregnant women. Health status in present pregnancy, husband’s decision, long waiting time at the clinic and frequent number of ante-natal visits are the major determinants of late booking in Enugu. There is need for transitioning from traditional approach of ANC to Focused Antenatal Care (FANC) model recommended by WHO.
Key words: Determinants, Enugu, late ante natal booking.
Each year, approximately one third of a million women worldwide die due to pregnancy related conditions; 99% of these deaths occur in developing countries of Africa and Asia and approximately three quarter of them are
considered avoidable (WHO, 2014). Preventing problems for mothers and babies depends on an operational continuum of care with accessible high quality care before and during pregnancy, childbirth and the postnatal period, and this also depends on the support available to help pregnant women reach services particularly when complications occur (Lancetto et al., 2010).
An important element of this continuum of care worthy to mention is effective antenatal care. Antenatal care (ANC) can be defined as the care provided by skilled health-care professionals to pregnant women and adolescent girls in order to ensure the best health conditions for both mother and baby during pregnancy (WHO, 2016). The components of ANC according to WHO include: Risk identification, prevention and management of pregnancy-related or concurrent diseases and health education and health promotion. Overtime, this form of care for pregnant women has become an important pillar in reducing maternal mortality rate (Onoh et al., 2013). The goal of antenatal care package is to prepare for birth and parenthood as well as prevent, detect, alleviate or manage the three types of health problems during pregnancy that affect mothers and babies: Complication of pregnancy itself, pre-existing condition that worsen during pregnancy and effects of unhealthy lifestyle (Lancetto et al., 2010). Good antenatal links the woman and her family with formal health system, increases the chance of utilizing a skilled attendant and contributes to good health through the life cycle (Onoh et al., 2013). Inadequate care during this time breaks a critical link in the continuum of care and affects both women and babies (Lancetto et al., 2010).
The first antenatal visit (booking) is a very important component of antenatal care as service providers use the occasion to collect basic medical information that will form the basis of care for the client. Wang et al. (2011) however noted that many women especially in Sub-Saharan Africa tend to wait to start antenatal care until the second or third trimester. Findings of Uganda Demographic and Health Survey (2011) showed that though over 90% pregnant women attended antenatal care at least once, only 48% made four or more antenatal care visits during their entire pregnancy; only 21% of the women made their first antenatal care visit before the fourth month of pregnancy and only 52% of women delivered under the care of skilled birth attendant; the maternal mortality ratio was 438 per 100,000 live birth.
The antenatal policy in Nigeria follows the latest WHO approach to promote safe motherhood. It is worthy to note that despite WHOs’ recommendation and antenatal care policy in Nigeria, studies have shown that late booking has become a persistent pathology in the country similar to what is being reported for other developing countries of the world (Ufenne and Utoo, 2013). Ndidi and Oseremen (2010) in their study revealed that vast majority of Nigerian women who utilize modern antenatal care book late which is in sharp contrast with findings in most developed countries. The prevalence of late booking as reported by researchers were as high as 86% in south west and 79% in Niger delta area of Nigeria (Okunlola et al., 2008; Adekanle and Isawumi, 2008).
The researchers in this study through the evaluation of antenatal booking records in selected hospitals found that the prevalence of late booking in South East Nigeria was as high as 75%. The researchers wondered what could be responsible for this late booking of antenatal care and this speculation motivated them to empirically ascertain the determinants of late booking among pregnant women in some selected hospitals in Enugu metropolis. Moreover, this study has not been carried out in South East and the researchers wish to bridge this gap.
The findings from this study will provide information on the factors that determine late booking for antenatal care among pregnant women. The factors identified, especially socio-cultural and organizational/systemic factors will help the policy makers to recognize the need to design new policies and adjust existing ones so as to protect and empower pregnant women as well as improve service delivery in health care setting.
In addition, nurse administrators and managers will be encouraged to enhance nurses’ attitude that may deter women from early booking through supervision, seminars, lectures and workshops. Hospital administrators through the findings of this work will provide needed help and changes that may facilitate early booking e.g prompt attention to pregnant women, and reduction in the cost of antenatal services. Finally, the information gotten will provide a solid basis for proper health education with the aim of reducing the prevalence of late booking among pregnant women and consequent high maternal mortality rate.
Objectives of the study
The aim of this study was to assess the determinants of late booking for antenatal care among pregnant women receiving care in some selected hospitals in South East, Nigeria. The specific objectives were to: Assess the maternal factors that predispose to late booking for antenatal care among pregnant women; identify the socio-cultural factors that are associated with late booking for antenatal care among pregnant women; determine the religious factors that contribute to late booking for antenatal care among pregnant women; assess organizational/systemic factors that determine late booking among pregnant women.
This is a descriptive cross sectional study. The study was carried out in three hospitals in Enugu State. The antenatal clinics of ESUT Teaching Hospital, Enugu, Poly Clinic, Asata and Ntasi Obi Hospital Trans-Ekulu were purposively selected. ESUTTH is a government owned tertiary institution, Poly clinic is a district hospital while Ntasi Obi is a missionary hospital; each located at different areas in Enugu Metropolis. A sample of 310 pregnant women from the three selected hospitals was used for the study. This was drawn from a population of 1061 pregnant women who attend ANC in the selected hospitals using power analysis. Utilizing the sample population for the study (310) and the known population of pregnant women who booked for antenatal in each of the three hospitals (1061) for a six month period, a proportionate stratified sampling method was used to obtain a sample of pregnant women from each hospital. A sample size of 123, 118 and 69 pregnant women constituting 40, 38 and 22%, respectively was obtained from ESUTH, Poly Clinic and Ntasi Obi Hospital, respectively. A researcher developed and pre-tested questionnaire containing 31 questions was used to elicit information from the respondents on their socio-demographic data and factors that determine late booking among pregnant women which include personal, socio-cultural, religious and institutional/systemic factors. Pregnant women who presented for their first ANC visit with a 16 week GA or more were included in the study. Ethical approval was gotten from the research and ethical committee of ESUTH while oral informed consent was gotten from individual respondent before data collection. Data collected was analyzed using descriptive statistics of frequency and percentage. This was done using the statistical tool of IBM statistical package for social sciences (SPSS) version 20.0.
Out of the 310 questionnaire distributed, only 290 were collected and duly filled.
Socio demographic data
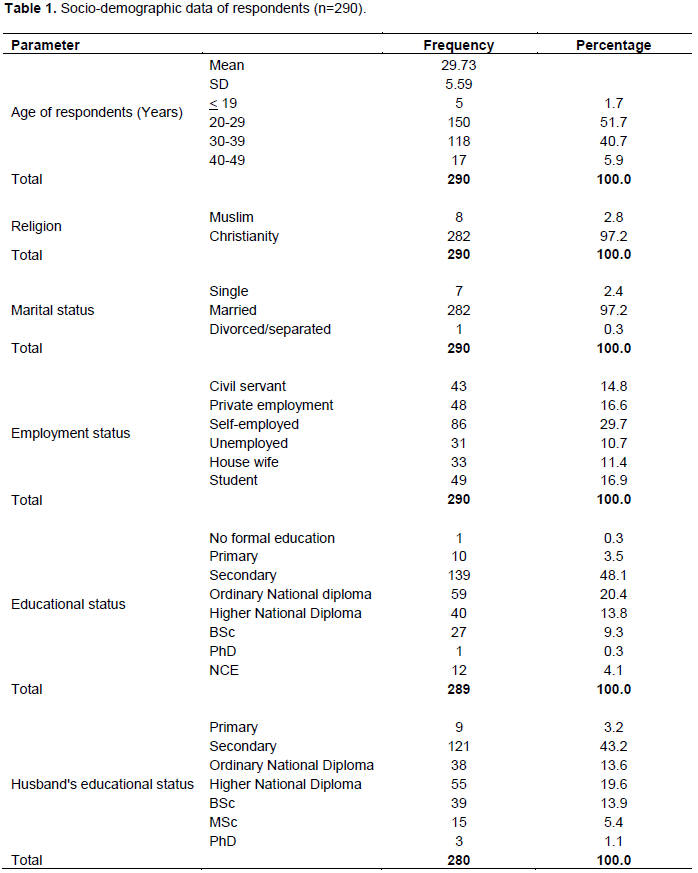
The minimum age of the respondents was 17 years while the maximum age was 47 years; the mean age for all the respondents was 29.73 years with a standard deviation of 5.59 years. Out of the 290 respondents 282(97.2%) were married, while 8(2.7%) are single, 86(29.7%) of the respondents are self-employed while 43(14.8%) are civil servants. Most 157(53.3%) of the respondents husbands were self-employed while 72(25.4) are civil servant, 10(3.5%) of the respondents had primary school education, 139(48.1%) of the respondents had secondary education, while 59(20.4%) had OND. Majority 121(43.2%) of the respondent’s husbands had secondary education, while only 38(13.6%) had OND (Table 1).
Maternal factors
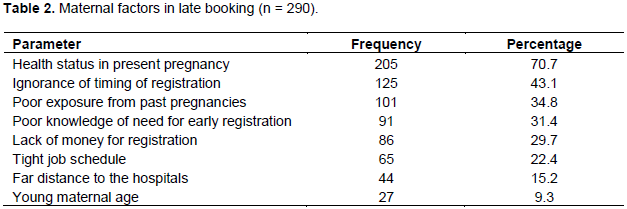
Health status in present pregnancy (70.7%) and ignorance of timing of registration (43.1%) were the major maternal determinants to late booking. Other minor determinants include poor exposure from past pregnancy (34.8%), poor knowledge of need for early registration (31.4%), lack of money for registration (29.7%), and young maternal age (9.3%) (Table 2).
Socio-cultural factors
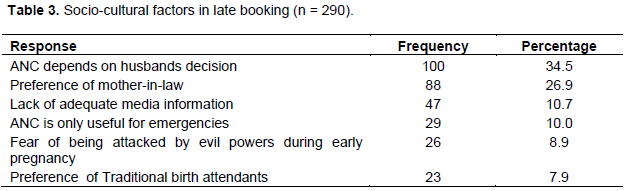
The major socio-cultural factors identified by the respondents were husbands’ decision (34.5%) and preference of mother in laws (26.9%). Others include lack of adequate information (10.7%), preference for TBA (7.9%) (Table 3).
Religious factors
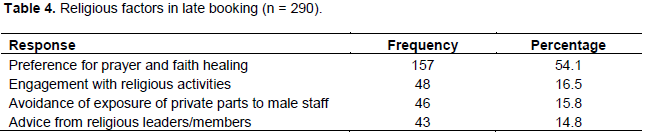
The respondents identified preference for prayer and faith healing (54.1%) as the religious factor in late booking. Other were engagement with religious activities (16.5%), avoidance of exposure of private parts to male staff (15.8%) and advice from religious leaders/members (14.8%) (Table 4).
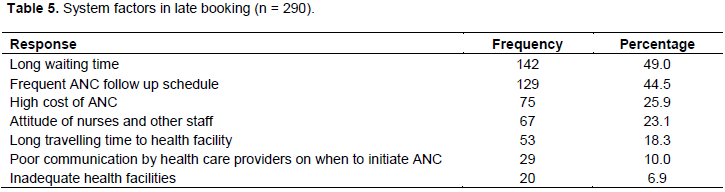
System factors
Long waiting time (49%), frequent ANC follow up schedule (44.5%), attitude of nurses and other staff (23.1%), high cost of ANC (25.9%), poor communication by HCP on when to initiate ANC (24.8%) are some of the identified institutional factors that determine late booking (Table 5).
Health status in index pregnancy, exposure and knowledge from previous pregnancy, ignorance of the appropriate gestational age to register were very outstanding as maternal factors that determine late booking among the study group. This show that most women book late because of the belief that there are no advantages in booking for antenatal care in the first 4 months of the pregnancy. This may also be due to the fact that antenatal care is viewed primarily as curative among the study population rather than preventive. In this environment, it has been noticed that people visit the hospitals only when they are sick, and that is why wellness clinics do not thrive in this area. This can definitely not be different for pregnant women whose conditions are not seen as sick’ but as a natural phenomenon, therefore, there should not be cause for alarm especially if the woman is healthy during this period. Ignorance of time for booking may indicate poor information from health care workers since majority are multigravidas who have attended antenatal in their previous pregnancies. Favorable outcome from previous pregnancy was identified by respondents as a determinant to late booking for ANC. It is pertinent to note that from the demographic history, majority of study respondents were multigravidas and mostly had uncomplicated pregnancy and labour. This further reveals the effect of misconception and ignorance that since they are not first timers and have not had problem in any of their previous pregnancy, they need not book early for antenatal care. This further reveals that parity and outcome of previous pregnancy are also maternal factors that influence pregnant women to book late for antenatal and are in keeping with the findings of the studies by Nwagha et al. (2008) and Kisuule et al. (2013), which revealed that parity, ignorance, absence of any problem in current pregnancy are factors that may influence pregnant women’s’ decision to book late for antenatal care.
Findings from the study revealed that a socio-cultural factor such as husband’s decision plays a vital role in exposing pregnant women to late booking for antenatal care. This may be because in the African culture decisions in the family are male dominant and women are always silent when it comes to deciding on matters that relates to their health due to the cultural inclination of our society and subordinate roles of women. This may also be attributed to the fact that most men in this study are not university graduates. It is believed that the more exposed an individual is the more informed decision they make with regards to their health and that of their family members of which their wives are included. Pregnant women also indicated they booked late due to not receiving enough information from the media. One may reason that this is so because women are too busy these days to seek for information which in turn points to the role reversal as seen in our society today; women are no longer provided for, rather they provide and carry the load of the family and therefore, have no time for their health. In addition, it is usually taken for granted that women are aware of when to book for ante natal care, so it is not usually discussed in media rather topics like complications of pregnancy are given more emphasis. The finding also revealed preference for mother-in-law/older women’s advice with reference to booking time.as one of the factors. This might also be due to the outcome of a complex interplay of gendered cultural hierarchies that locate pregnancy related decision making in remote authorities such as older female relatives like mother-in-laws, older female relatives etc. This might be because these women are seen as new members of the family that are not aware of the family tradition therefore, any decision concerning childbirth should be left for older women in the family who understands the tradition and belief of the family. This also showcase the African culture of subordination of younger women’s interest with all emphasis on whatever older females whom they believe had gone through the process of pregnancy and childbirth feel about the situation at hand. This is line with the study by Kotecha et al. (2012).
Furthermore, it was shown that fear of being noticed and attacked by evil powers, preference for Traditional Birth Attendants in early weeks of pregnancy were other factors responsible for late booking. This may be so because of the disruptive role of socio-cultural perspective in the use of public health facilities services such as antenatal and perceived threats which are often given socio-cultural interpretation increasing women’s anxieties and driving them to seek multiple sources of care. In line with this study, several studies have found a consistent relationship between socio-cultural factors and late booking for antenatal. Study by Dako-Gveke et al. (2013) noted that perceived threats interpreted as socio-cultural increased women’s anxiety driving them to seek multiple sources of care from herbalists, traditional birth attendants and spiritualist disrupting the continued use of skilled care providers with resultant increase in prevalence of late booking among pregnant women.
This study revealed the religious factor that has an obvious influence on pregnant women making them to book late for antenatal care was preference for prayer and faith healing. One need not wonder why it is so since there are proliferations of churches and prayer ministries in our societies today. Most Christians attend spiritual/ prayer houses that offer prayers and care during pregnancy as most Christian organizations have spiritual/ prayer houses that offer care to women especially their members that are pregnant. Another, possible explanation could be linked to the belief and fact that pregnancy is surrounded by a lot of uncertainties. Pregnant women always seek shelter from evil by running to these prayer ministries especially during the early months of their pregnancy forgetting or neglecting antenatal care. The study also reveals that advice from religious leaders/ members, engagement with religious activities were some of the religious factors that determine late booking for antenatal. Obviously, due to the trust which people normally have on their religious leaders/ members they tend to heed to their advice even when it is detrimental to their health? They will rather choose to get deeply involved with the religious activities of ministries. This might be the case with this proportion of the study population who booked late due to the advice and engagement in religious activities. This finding implies that mass media should intensify their effort in health education so as to help these religious leaders to understand that while these pregnant women come to them for prayers, they should also advise them to seek orthodox care. A study by Dairo and Owoyokun (2010) on religious factors that affect early booking supports these findings as it revealed that most Christians especially protestants attend spiritual houses for prayer at the expense of antenatal care.
The outcome of the result showed that out of the institutional/systemic factors listed, long waiting time and frequent antenatal care follow-up schedule were most significant factors. In other words, most pregnant women book late for antenatal because they do not want to waste their time or come for antenatal visit frequently. They choose to wait until second or third trimester before booking for antenatal so as to reduce the number of antenatal visits and also reduce the time they will have to wait before being attended to. This finding supports the need for the health institutions to adopt the Focus Antenatal Care approach as was recommended by the WHO in 2002. Under this approach, the WHO recommended only four antenatal visits for normal pregnancy and booking which should occur by 16 weeks gestation. Also implicated under organizational/systemic factors for late booking among pregnant women were attitude of the nurses and other staff and poor communication by healthcare providers on when to initiate antenatal care. This indicates the need for more comprehensive health education on the importance and timing of antenatal care and also the need for attitudinal change among nurses and other health care workers. Owing to the state of Nigeria today, it is obvious from this study that late booking for antenatal care is partly due to harsh economic condition as some of the pregnant women indicated that they booked late due to high cost of antenatal services. In Enugu State, antenatal care services is free in state government hospitals only for civil servants with evidence of tax payment and majority of the respondents and their spouses are not civil servants so they have to pay for the services. The outcomes of this study are in consonance with the findings of a survey by Zegeye et al. (2013) on prevalence and determinants of late antenatal care visit among pregnant women attending antenatal care in Debre, Berhan Health institutions, Central Ethiopia. Their result revealed that poverty, frequent antenatal schedule, long traveling time, long waiting time and inadequate health facilities are factors affecting the timing of antenatal care initiation.
Majority of the respondents booked for antenatal at 5 months gestational age and are multigravidas. Personal/ maternal factors especially health status in present pregnancy, ignorance of the appropriate time (gestational age) to register, exposure (enough knowledge from previous pregnancies) predispose pregnant women to late booking for antenatal care. Husband’s decision and preference for mother-in-law/friends/other women’s advice during the early weeks of pregnancy are the socio-cultural factors that are mostly responsible for late booking for antenatal. Preference for prayer and faith healings the religious factor that mostly is responsible for late booking among pregnant women. Finally, long waiting time and frequent antenatal care follow-up schedule as institutional/systemic factors are responsible for late booking
Based on the findings from this study, the researchers made the following recommendations; Health education on the timing and importance of attending antenatal care early should be done in communities where women and other people that influence the pregnant women’s decision to attend care live so that they get this information even before they conceive. This can be done through the media, places of worship, schools and community gatherings; Community based health education programs are needed to correct the misconception about antenatal care; The campaign for male involvement in issues of reproductive health such as antenatal care should be sustained so that they will get to know why it is important that their wives should book early for antenatal care; promoting education, public health enlightenment, reduction in poverty and modification of certain cultural practices could be helpful in mitigating hindrances resulting from these factors, thereby contributing towards the improvement in maternal and child health; there is need for transitioning from traditional approach of ANC to Focused Antenatal Care (FANC) model recommended by WHO because some of the pregnant women booked late because of frequent antenatal care follow-up schedule; Efforts should be made to promote maternal education so as to empower women to take care of themselves during pregnancy.
The authors have not declared any conflict of interests.
REFERENCES
|
Adekanle DA, Isawumi AI (2008). Late Antenatal Care Booking and Its Predictors among Women in South Western Nigeria. Online Journal of Health and Allied Sciences, 7(1):1-6.
|
|
|
|
Dairo MD, Owoyokun KE (2010). Factors affecting the utilization of antenatal care services in Ibadan, Nigeria. Benin Journal of Postgraduate Medicine, 12(1):3-13.
|
|
|
|
|
Dako-Gyeke P, Aikins M, Aryeetey R, Mccough L, Adongo PB (2013). The influence of socio-cultural interpretations of pregnancy threats on health-seeking behavior among pregnant women in urban Accra, Ghana. BMC Pregnancy and Childbirth, 13(1):211.
Crossref
|
|
|
|
|
Kisuule I, Kaye DK, Najjuka F, Ssematimba SK, Arinda A, Nakitende G, Otim L (2013). Timing and reasons for coming late for the first antenatal care visit by pregnant women at Mulago hospital, Kampala Uganda. BMC Pregnancy and Childbirth, 13(1):121.
Crossref
|
|
|
|
|
Kotecha P, Patel S, Shah S, Katara P, Madan G (2012). Health seeking behavior and utilization of health services by pregnant mothers in Vadodara slums. Healthline, 3(1):30-32.
|
|
|
|
|
Lincetto O, Mothebesoane-Anoh S, Gomez P, Munjanja S (2010). Antenatal Care: Opportunities for Africa's Newborns. New York: World Health Organization.
|
|
|
|
|
Nwagha UI, Ugwu OV, Anyachie US (2008). The influence of parity on the gestational age at booking among pregnant women in Enugu, South East Nigeria. Nigerian Journal of Physiological Sciences, 23(1-2):67-70.
|
|
|
|
|
Ndidi EP, Oseremen IG (2010). Reasons given by Pregnant women for late initiation of antenatal care in the Niger Delta, Nigeria. Ghana Medical Journal, 44(1):47-52.
|
|
|
|
|
Okunlola MA, Ayinde OA, Omigbodun AO, Owonikoko KM (2008). Factors influencing gestational age at antenatal booking at the University College Hospital, Ibadan. Journal of Obstetrics and Gynaecology, 26(3):195-197.
Crossref
|
|
|
|
|
Ufenne DI, Utoo B (2013). Gestational age at booking for antenatal care in a tertiary health facility in north-central, Nigeria. Nigerian Medical Journal of the Nigeria Medical Association, 53(4):236-239.
|
|
|
|
|
Wang W, Alva S, Wang S, Fort A (2011). Levels and Trends in the Use of Maternal Health Services in Developing Countries. DHS Comparative Reports No. 26. Calverton, Maryland, USA: ICF Macro. Available at:
View
|
|
|
|
|
World Health Organization (WHO) (2002). Antenatal Care Randomized Trial. Manual for the implementation of the new model. Geneva: Department of Reproductive Health and Research. Family and Community Health, World Health Organization. Available at: View
|
|
|
|
|
World Health Organization (2014). Maternal mortality fact sheet. Available at:
View
|
|
|
|
|
World Health Organization (WHO) (2016). WHO recommendations on antenatal care for a positive pregnancy experience. World Health Organization. Available at:
View
|
|
|
|
|
Zegeye AM, Bitew BD, Koye DN (2013). Prevalence and determinants of early antenatal care visit among pregnant women attending antenatal care in Debre Berhan Health Institutions, Central Ethiopia. African Journal of Reproductive Health, 17(4):130-136.
|
|