Full Length Research Paper

ABSTRACT
In Tanzania, the estimated delivery date (EDD) is mainly determined by the last menstrual period (LMP), presumably leading to inaccurate estimates with a falsely high proportion of post-term and preterm deliveries. The study aimed to compare EDD determination by LMP and ultrasound in pregnant Tanzanian women and examine how the dating method affects the proportions born preterm, at term, and post-term and assess how maternal characteristics relate to wrongly EDD determination by LMP. 1123 women attending antenatal care in Moshi, Tanzania were included. Gestational age (GA) at birth was calculated according to LMP and ultrasound separately. The distribution of preterm (GA<259 days), term (GA 259-294 days), and post-term (GA >294 days) births was examined separately for LMP and ultrasound. According to LMP, 17.0% of deliveries were preterm and 17.6% post-term. According to ultrasound, 7.7% of deliveries were preterm and 3.4% post-term. Unplanned pregnancy was associated with an increased odds ratio of 3.06 (95% CI: 1.91-4.91) for preterm delivery when LMP was used for EDD determination instead of ultrasound. Parity 3+ was associated with an increased odds ratio of 2.12 (95%CI: 1.16-3.89) for post-term delivery when EDD was assessed by LMP. LMP based EDD increased the preterm birth rate two times and the post-term birth rate five times compared to ultrasound-based EDD.
Key words: Gestational age, pregnancy length, last menstrual period (LMP), dating methods, preterm, post term, Africa.
INTRODUCTION
Optimal obstetric care that assures women access to quality antenatal care and relevant actions if needed is essential for maternal and child health (WHO, 2017). Ultrasound has proven to be extremely useful in antenatal care as it helps identify high-risk pregnancies (Whitworth et al., 2015). The World Health Organization (2016) therefore recommends that pregnant women have one ultrasound examination before 24 weeks of gestation to determine viability, estimated date of delivery (EDD), detect fetal anomalies, and multiple pregnancies. Yet, despite these recommendations, the vast majority of women in resource-constrained areas like Tanzania go through pregnancy without the benefit of an ultrasound examination.
Determination of EDD is an essential component in the management of pregnancies (Whitworth et al., 2015). However, in settings where ultrasound scanning is not available, health providers must rely on the last menstrual period (LMP) when assessing EDD. LMP has its limitations since dating may be difficult because of imperfect recall, irregular menstrual cycles, bleeding in early pregnancy, and lactation amenorrhea
It is increasingly acknowledged that ultrasound-based EDD may help improve diagnosis and treatment of preterm birth and help reduce the associated perinatal mortality (Marchant et al., 2012). Studies have shown that post-term pregnancy is one of the leading indications for labor induction (Whitworth et al., 2015; Dogl et al., 2018). Therefore, accurate pregnancy dating is crucial for the diagnosis and management of post-term pregnancy. In settings where ultrasound is not offered as part of antenatal care, women are at increased risk of iatrogenic premature births, fetal distress, and uterus rupture due to labor induction (World Health Organization, 2011). The risk of uterus rupture is a problem that needs particular considerations in a sub-Saharan African context, where inductions frequently are performed on women with uncertain gestational age (GA) and by laypeople using different types of herbal mixtures (Kamatenesi-Mugisha and Oryem-Origa, 2007). The use of uterotonics during labor is one of the most frequent causes of uterine rupture in sub-Saharan Africa, as reported by Fofie and Baffoe (2010), who in a Ghanaian study found herbal mixtures used for labor induction were the course of 59% of uterus ruptures.
When discussing the potential benefits of ultrasound in sub-Saharan Africa, economic constraints and lack of human resources have to be considered. In low-income countries like Tanzania, antenatal ultrasound is only available to a few privileged women who have easy access to referral-level hospitals. Further, an extreme shortage of staff trained to perform ultrasound scanning hampers women’s access to early scanning. The lack of access to early scanning contributes significantly to the global burden of maternal and perinatal morbidity and mortality. Therefore, training more nurses/midwives to perform ultrasound scanning must be considered to increase women’s access to early scanning, identify high-risk pregnancies, and improve pregnancy outcomes.
This study compares EDD determination by LMP and ultrasound offered by nurse-midwives/doctors in pregnant Tanzanian women. It examines how the dating method affects the proportions born preterm, at term, and post- term and how maternal characteristics relate to wrongly EDD determination by LMP.
METHODOLOGY
Study design, setting, and population
The data for this prospective cohort study were collected as a part of the PAVE study of intimate partner violence (Sigalla et al., 2017). Data were collected at Pasua and Majengo health centers in Moshi Municipality, Kilimanjaro Region, Tanzania, between March 2014 and May 2015. Pregnant women were recruited when attending antenatal care at the two primary level health facilities. Pregnant women up to 24 weeks of gestation, following the World Health Organization recommendations of the timing of early ultrasound were included (World Health Organization, 2016; Sigalla et al., 2017). All participants who met the inclusion criteria were informed of the nature of the study and signed informed consent to participate in the study (Sigalla et al., 2017).
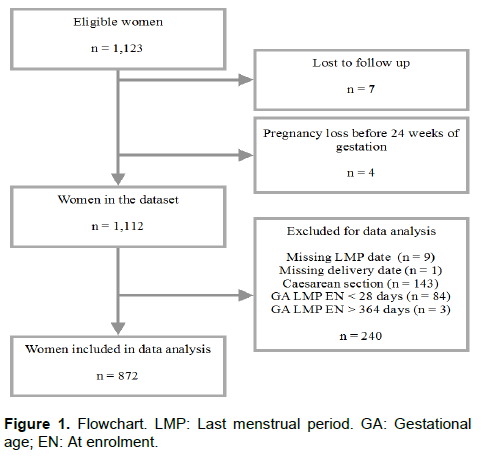
Women who planned to deliver outside of Moshi Municipality and women with multiple pregnancies were excluded from the cohort. For data analysis, women with GA <28 days at enrolment and women with GA >364 days at enrolment were excluded. Women who had a cesarean section and women whose data on LMP or delivery date were missing were also excluded.
Data collection
The women were interviewed at inclusion, where information about socio-demographic characteristics and health-related issues, including LMP, contraceptive use, and pregnancy planning, were collected. Regarding pregnancy planning, the women were asked: “At the time you became pregnant, did you want to become pregnant, did you want to wait until later, did you want no (more) children, or, did you not mind either way?” Only the women answering that they wanted to become pregnant were defined as having a “planned pregnancy”. Within 48 h after delivery, data were collected on the delivery date, delivery mode, and birth weight.
At the date of enrolment, a transabdominal ultrasound scan was performed to determine EDD. Ultrasound measurements of crown-rump length (CRL) were used for GA 5.5-12+6 weeks and head circumference (HC) for GA 13.0 - 23+6 weeks (Hadlock et al., 1992, 1982). All ultrasound scans were performed by three trained nurse-midwives and one general practitioner. They were trained by a Tanzanian obstetrician with expertise in ultrasound scanning and a Danish gynecologist/obstetrician (VR). It has previously been shown that it is possible to teach local health care workers with no prior exposure to ultrasound, to perform proper obstetric ultrasound scans in low-income settings (Greenwold et al., 2014; Nathan et al., 2017). Quality control of the first 288 scanning pictures was performed by a Danish expert in fetal medicine (LS) and VR and the remaining 1100 pictures by VR, to ensure the reliability of ultrasound.
All ultrasound scans were performed either with B-K Medical 2101 and 8665 Convex Array Probe (Majengo HC) or Voluson i BT11 with AB2-7-RS Convex Probe (Pasua HC).
The EDD determined by ultrasound was used as a reference. Women who gave birth preterm according to LMP while at term according to ultrasound were classified as “false” preterm, and women who gave birth post-term according to LMP while at term according to ultrasound were classified as “false” post-term.
Statistics
The EDD was calculated by LMP by adding 280 days to the LMP date. Measures from ultrasound were translated into a GA in days at the day of the examination. EDD was calculated by subtracting GA from 280 and adding the result to the examination date. GA at delivery was calculated by adding the number of days between the ultrasound examination and the delivery to the initial GA. LMP based GA at delivery was the number of days between the LMP date and the delivery date.
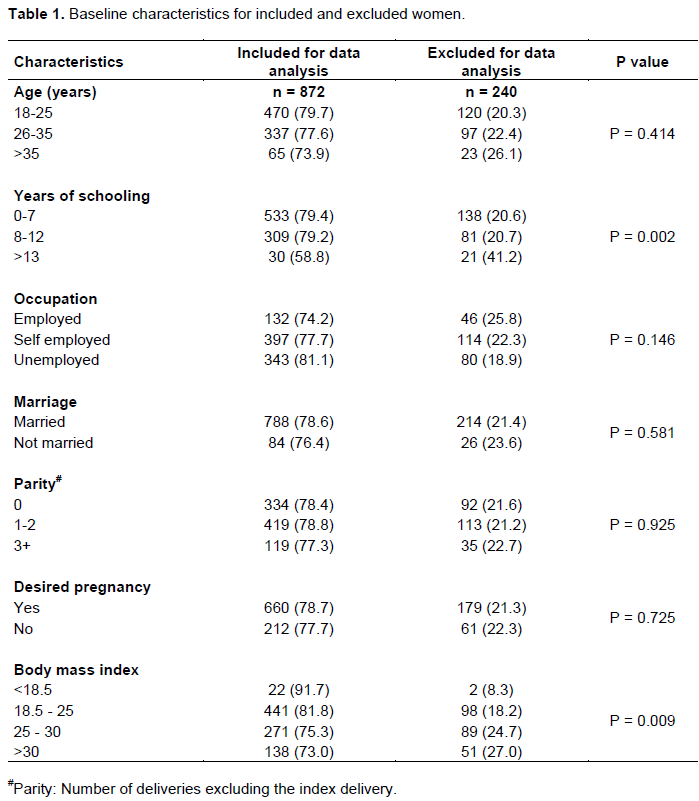
Baseline characteristics were presented for all eligible women attending antenatal health care; both women included and excluded from data analysis. Chi-square test was used to calculate p-values in Table 1, except for Body Mass Index where Fischer’s exact test was used.
The distribution of infants born preterm (GA <259 days), at term (GA 259-294 days), and post-term (GA >294 days) was examined for both pregnancy dating methods (World Health Organization, (2017). Mean birth weight was calculated for each group and subgroup , to indicate the agreement of the classification. To estimate agreement between the pregnancy dating methods, the kappa-value was calculated (McHugh, 2012; The American College of Obstetricians and Gynecologists, 2014).
Logistic regressions were used to explore risk factors for the disagreement between the two methods for the women classified as giving birth preterm according to LMP, but at term according to ultrasound, and for the women classified as giving birth post-term according to LMP, but at term according to ultrasound. Crude odds ratios (OR) with 95% confidence intervals were estimated to determine the associations between different characteristics and the disagreements. Based on literature and our clinical experience, we adjusted for pre-specified potential confounding variables including age (18-25, 26-35, and >35 years), women’s education (0-7, 8-12, and >12 years), parity (0, 1-2, and 3+), planned pregnancy (yes or no), and Body Mass Index (BMI) (<18.5, 18.5-25, 25-30, and >30 kg/m2).
Statistical analysis was conducted using STATA/IC 15.0 for Mac (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC). P-values < 0.05 wereas considered the appropriate level of significance.
RESULTS
During the study period, 1,123 pregnant women attended antenatal care at the two primary level health facilities and were eligible for inclusion and 8723 women were eligible for data analysis (Figure 1).
Baseline characteristics
No significant difference between the included and excluded women was found in age, occupation, marital status, parity and planned pregnancy (Table 1). However, iIncluded and excluded women differed in terms of education and Body Mass Index (BMI). More women with >13 years of schooling were excluded, and more women with higher BMI were excluded. Both differences can be explained by our exclusion of all cesarean section deliveries. More women with >13 years of schooling had a cesarean section and more women with higher BMI had a cesarean section.
Gestational age dispersion and classification of preterm, term and post-term delivery
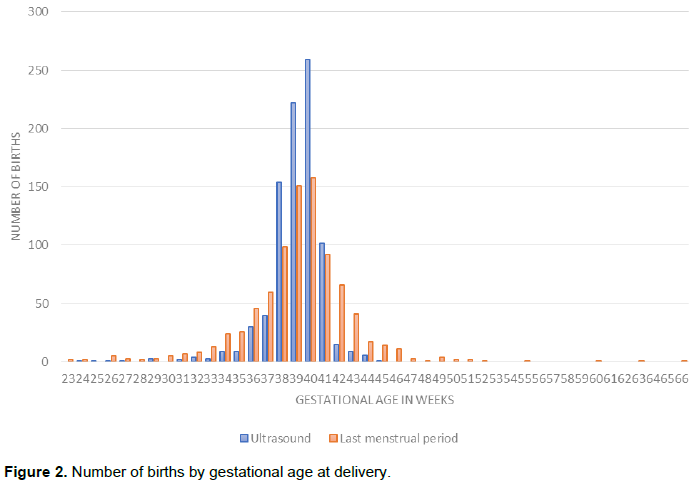
Figure 2 shows the distribution of GA at delivery according to LMP and ultrasound. As seen, the dispersion of GA was wider for LMP than for ultrasound. According to LMP, 109 women gave birth between 33+0 and 36+6. In the same interval, 51 women gave birth according to ultrasound. At GA from week 43+0 to 46+6, 83 women gave birth according to LMP compared to 16 according to ultrasound. The agreement between ultrasound and LMP stratified by children born preterm, at term, and post-term are summarized in Table 2. A notable difference in the percentage born preterm, at term, and post-term according to the two methods is seen and is further illustrated by a kappa-value of 0.209, which indicates a minimal level of agreement. In comparison with ultrasound, LMP classified more women women preterm (17.06.9% vs 7.7%) and post-term (17.68% vs 3.4%). For 32.78% of the women, there was no agreement in preterm, term and post-term classification between the two methods. Mean birth weight was used as an indicator of the agreement of the classification. Children born preterm according to both methods had the lowest mean birth weight (2307 g), whereas children born post-term according to both methods had the highest mean birth weight (3275 g). Children born preterm according to LMP had a 440 g higher mean birth weight than children born preterm according to ultrasound. Children born at term according to LMP had similar birth weight to those born at term according to ultrasound (3157 g vs 3179 8g), and the same was pictured for post-term births (3223 1g vs 3195 g).
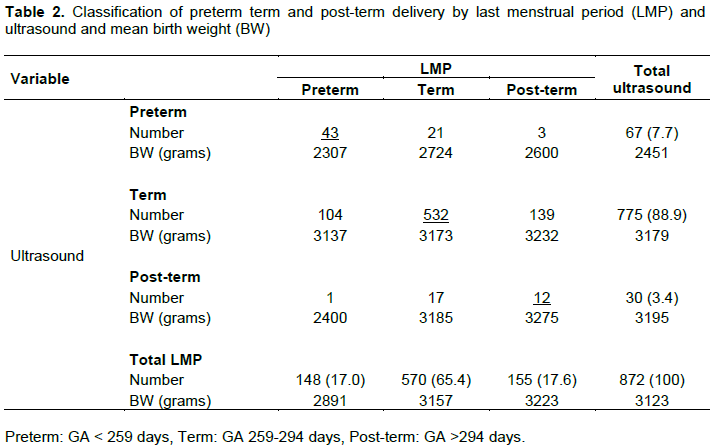
A group of 104 (11.9%) women were classified preterm by LMP, while at term by ultrasound, and thereby falsely diagnosed as preterm delivery according to LMP (Table 2). Another group of 140 (16%) women were classified post-term by LMP, while at term by ultrasound, and thereby falsely diagnosed as having post-term birth according to LMP. Table 3 shows baseline characteristics and/or for these two groups of women, compared to the 532 women classified at term by both methods. The distribution of women in each BMI category was similar for the groups classified as false preterm, false post-term and term by both methods.
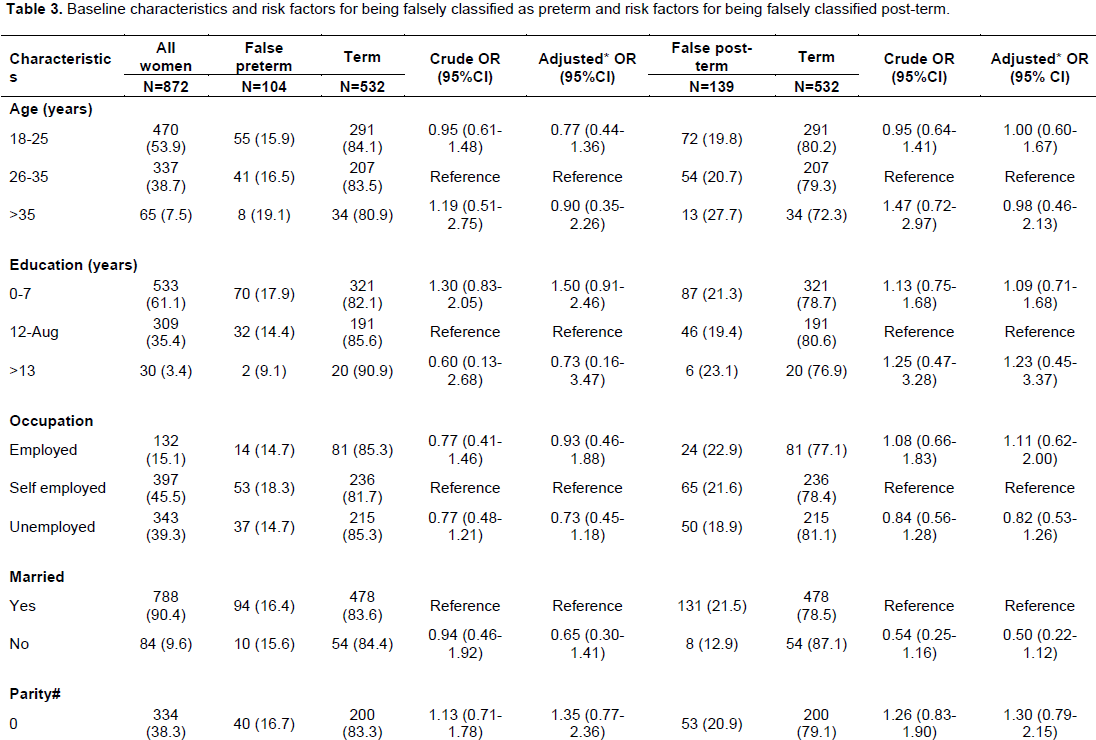
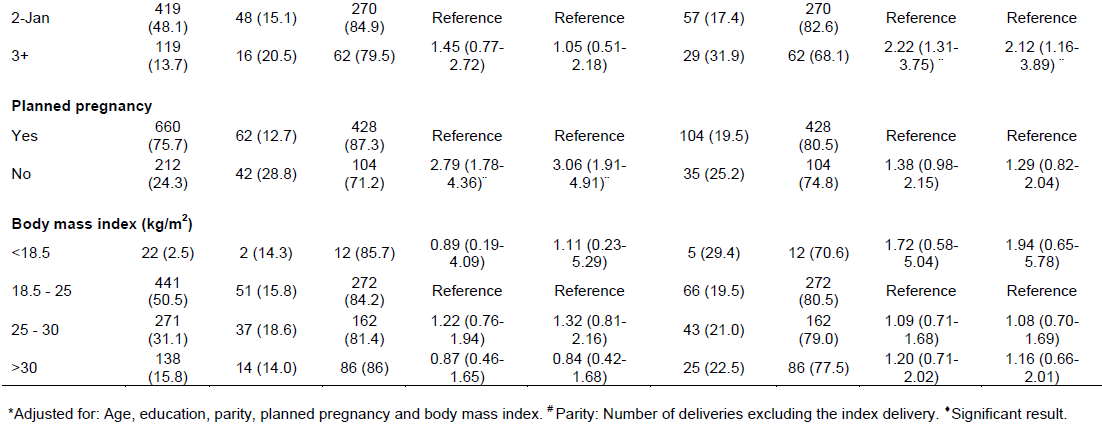
Risk factors for being falsely classified as having a preterm or post-term delivery
In all, 104 women were classified as preterm by LMP while at term by ultrasound (falsely preterm). Among these women, 40% (42/104) reported that their pregnancy was unplanned. The corresponding figure among women giving birth at term was 20% (104/532). Women who were unplanned pregnant were almost three times more likely to be classified as falsely preterm than women who were planned pregnant (crude OR = 2.79; 95%CI: 1.78-4.36 and adjusted OR = 3.06; 95% CI: 1.91-4.91). Among women classified as falsely post-term (n=139), it was found that 21% (29/139) of the women had previously delivered three times or more whereas the same applied for 12% (62/532) of the women who were classified as being at term. Women of parity 3+ were more than two times more likely to be classified as falsely post-term in comparison with women who had delivered 1-2 times (crude OR =2.22; 95%CI:1.31-3.75 and adjusted OR = 2.12; 95%CI:1.16-3.89).
DISCUSSION
LMP based EDD determination leads to 17.0 and 17.6% of deliveries classified as preterm and post-term, respectively. The corresponding figures for ultrasound were 7.7 and 3.4%. LMP determined EDD was associated with three times increased risk of a “false” diagnosed of preterm birth among unplanned pregnant women and two times increased risk of a “false” diagnosed of post-term birth among women with parity 3+.
Strengths and limitations
Ultrasound was used as the reference since it provides the best EDD (17-21). However, ultrasound is limited as it translates measures into a specific GA, without taking into account gender and maternal age, which both are known to affect the measures (22). According to ultrasound, we found 3.4% women delivered post-term. This is comparable to the rate of 3.4% found by Savitz et al. (2002) and 2.7% found by Taipale and Hiilesmaa (2001). These results indicate that our ultrasound estimates are reliable.
Information were lacking about induced deliveries and were thus not able to exclude these deliveries from the analysis. This may be considered a limitation. Bukola et al. (2012) examined medical labor inductions in seven African countries and found a rate of 4.4%. It was assumed that the rate of medical inductions in our cohort was similar. Another limitation is that information on the women’s use of herbal concoctions for labor induction is lacking. Hence, the use of herbs is widespread in Tanzania and other African countries, and their uterus contractive effect is well described (Kamatenesi-Mugisha and Oryem-Origa, 2007; Fofie and Baffoe, 2010; Nikolajsen et al., 2011). Most likely, some of the women in our cohort used herbal concoctions for labor induction, and it would have been relevant to study its association with preterm birth. Unknown rates of labor induction, either medically or with herbs, could have affected our results. Further, the women were not ask about co-morbidities. This may also be considered a limitation since a number of maternal illnesses, conditions and medical treatments are associated with spontaneous preterm birth (Goldenberg et al., 2008).
Interpretation
LMP determined EDD was associated with 17% deliveries being diagnosed as preterm. Our findings are considerably higher when compared with other studies. Savitz et al. (2002) and Taipale and Hiilesmaa (2001) found the proportion of preterm births 12 and 4.6%, respectively, when EDD was based on LMP. Taipale and Hiilesmaa (2001) excluded women with uncertain LMP, which presumably increase the accuracy of LMP, and explain the lower preterm birthrate according to LMP, which is comparable to their preterm birthrate at 4.4% according to ultrasound. Similarly, we found 17.6% of the deliveries being diagnosed as post-term by LMP, which is also comparatively higher than what has been reported by Savitz et al. (2002) and Taipale and Hiilesmaa (2001) who found the post-term birthrate to be 12.1 and 10.2% according to LMP. The fact that larger proportions of deliveries in the present cohort are diagnosed preterm and post-term indicates that Tanzanian women have less accurate LMP leading to higher proportions of pregnancies classified as preterm and post-term. Further, the studies by Savitz et al. (2002) and Taipale and Hiilesmaa (2001) were conducted in high-income countries where access to prenatal care is greater than in Tanzania. Finally, Taipale and Hiilesmaa (2001) only included spontaneous labors in their study population, thereby presumably underestimating the post-term birthrate, since a part of the post-term women assumingly underwent induction of labor on the indication post-term pregnancy. In our cohort, the women were informed about the ultrasound based EDD. It is likely to have the consequence that some of the index pregnancies were induced timely, medically or with herbs, leading to lower rates of post-term pregnancies. It is also conceivable that fewer women would seek preterm labor induction knowing the ultrasound based EDD, leading to lower rates of preterm births.
LMP based EDD is inaccurate for many reasons. The method assumes a regular cycle of 28 days with ovulation at the 14th day. Despite regularity, a light bleeding can occur in early pregnancy and can be misinterpreted as menstruation. Further, amenorrhea and recent use of hormonal contraceptives can also lead to difficulties in assigning a correct LMP. The aforementioned reasons are naturally and cannot be avoided, but the method additionally relies on correct recall. It is reasonable to think that African women live a more traditional life, where family planning and recording of LMP are not as common as in high-income countries.
In our cohort, 24% of the women reported having an unplanned pregnancy, which was associated with increased risk of preterm birth according to LMP. It is intuitively that women not planning a pregnancy are less aware of their menstruation, and therefore recall LMP less accurately. They are maybe less aware of pregnancy symptoms, and might realize the pregnancy at a late stage, by which recall of LMP is challenging. The association between unplanned pregnancy and increased risk of preterm delivery according to LMP has to our knowledge not been shown before. The contrary has been reported by Savitz et al. (2002) who found that unplanned pregnancies were more likely to be post-term when LMP was used for EDD determination. The association found between parity 3+ and post-term birth when EDD was based on LMP may explain the high rate of post-term birth found in the present study. Tanzanian women gave birth to 5.2 children in average between 2010 and 2015, while Finnish women gave birth to 1.8 and American women gave birth to 1.9 children in average in the same period (Kamatenesi-Mugisha and Oryem-Origa, 2007; Fofie and Baffoe, 2010; United Nations Population Division, 2017). With an average of 5.2 children per Tanzanian women, the time interval between pregnancies can be short. Some women might experience a new pregnancy before the return of their menstrual cycle, the use of LMP will in such situations cause an inaccurate EDD determination. Women with LMP based GA >364 days at enrollment were excluded for data analysis (three women), though some or all of them might experience a new pregnancy before the return of their menstrual cycle. The exclusion of the three women leads to lower rates of post-term births.
Summing up, 12 and 16% of the women in our cohort were diagnosed as “false” preterm and “false” post-term by LMP (Table 2). It is known, that accurate EDD determination may lead to improved diagnosis and treatment of preterm birth and prevent iatrogenic preterm birth due to labor induction on the wrong indication. Regarding iatrogenic preterm births, it should be recognized that induction of labor is widespread in sub-Saharan Africa and Tanzania and that the procedure may comprise a threat to maternal health if performed on the wrong indication (Kamatenesi-Mugisha and Oryem-Origa, 2007; Fofie and Baffoe, 2010). Fofie and Baffoe (2010) examined uterine rupture in Ghana and found 1:124 pregnant women having a uterine rupture, whereof 58.5% was caused by local administered herbs with suspected uterine contractive effects. A Ugandan interview study found that nearly all of the 198 interviewed women used herbs to induce the labor (Kamatenesi-Mugisha and Oryem-Origa, 2007). A recently published 20-point toolkit on induction of labour enlists ultrasound assessment of the fetus as one of the measures for improving outcomes of induced labour in low-resource settings (Ngene and Moodley, 2020).
Since optimal obstetric management is dependent on EDD, accurate delivery date estimations are necessary for the health of the mother and the child. We believe improved EDD by ultrasound will optimize treatment of preterm births and prevent untimely labor inductions. Keeping in mind that Tanzanian is a resource constraint country where most births occur at home or in peripheral clinics, we suggest that nurse-midwives are trained to perform antenatal scanning to determine EDD and detect diagnosis of problems such as multiple pregnancy and placenta previa. This approach is supported by evidence that nurse-midwives with basic ultrasound training have proven to achieve high levels of accuracy in gestational age assessment (Rijken et al., 2009) as well as preforming early antenatal scanning with high levels of accuracy (Chen et al., 2009). We believe this is a viable option to improve antenatal care and address maternal and perinatal morbidity and mortality.
CONCLUSION
In this study, the EDD based on LMP doubled the preterm birthrate compared to ultrasound and estimated post-term birth five times more often than ultrasound. EDD determination by LMP was associated with two times increased odds of preterm delivery among unplanned pregnant women, and three times increased odds of post-term delivery among women with parity 3+. Early ultrasound examination of pregnant women in Tanzania would significantly increase the accuracy of delivery date estimations, and thereby improve treatment of preterm births and prevent untimely induced labors.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors thank the women who participated in this study. They thank the research assistants in Moshi for conducting the interviews. This research was conducted under the auspices of the interdisciplinary research project PAVE (The Impact of Violence on Reproductive Health in Tanzania and Vietnam) which is funded by DANIDA (the Danish International Development Agency; project number 12-006KU).
REFERENCES
|
Bukola F, Idi N, M'Mimunya M, Jean-Jose WM, Kidza M, Isilda N, Metin, G (2012). Unmet need for induction of labor in Africa: secondary analysis from the 2004-2005 WHO Global Maternal and Perinatal Health Survey (A cross-sectional survey). BMC public health 12(1):1-10. |
|
|
Chen M, Leung TY, Sahota DS, Fung TY, Chan LW, Law LW, Lau TK (2009). Ultrasound screening for fetal structural abnormalities performed by trained midwives in the second trimester in a low-risk population--an appraisal. Acta Obstet Gynecol Scand 88(6):713-9. |
|
|
Dogl M, Romundstad P, Berntzen LD, Fremgaarden OC, Kirial K, Kjollesdal AM, Heimstad R (2018). Elective induction of labor: A prospective observational study. PLoS One 13(11):e0208098. |
|
|
Fofie C, Baffoe P (2010). A two-year review of uterine rupture in a regional hospital. Ghana medical journal 44(3):98-102. |
|
|
Goldenberg RL, Culhane JF, Iams JD, Romero R (2008). Epidemiology and causes of preterm birth. Lancet 371(9606):75-84. |
|
|
Greenwold N, Wallace S, Prost A, Jauniaux E (2014). Implementing an obstetric ultrasound training program in rural Africa. International Journal of Gynecology & Obstetrics 124(3):274-277. |
|
|
Hadlock FP, Deter RL, Harrist RB, Park SK (1982). Fetal head circumference: relation to menstrual age. AJR American journal of roentgenology 138(4):649-53. |
|
|
Hadlock FP, Shah YP, Kanon DJ, Lindsey JV (1992). Fetal crown-rump length: reevaluation of relation to menstrual age (5-18 weeks) with high-resolution real-time US. Radiology 182(2):501-505. |
|
|
Kamatenesi-Mugisha M, Oryem-Origa H (2007). Medicinal plants used to induce labour during childbirth in western Uganda. Journal of ethnopharmacology 109(1):1-9. |
|
|
Marchant T, Willey B, Katz J, Clarke S, Kariuki S, ter Kuile F, Armstrong Schellenberg J (2012). Neonatal mortality risk associated with preterm birth in East Africa, adjusted by weight for gestational age: individual participant level meta-analysis. PLoS medicine 9(8):e1001292. |
|
|
McHugh ML (2012). Interrater reliability: the kappa statistic. Biochemia medica 22(3):276-282. |
|
|
Nathan RO, Swanson JO, Swanson DL, McClure EM, Bolamba VL, Lokangaka A, Goldenberg RL (2017). Evaluation of Focused Obstetric Ultrasound Examinations by Health Care Personnel in the Democratic Republic of Congo, Guatemala, Kenya, Pakistan, and Zambia. Current problems in diagnostic radiology, 46(3):210-215. |
|
|
Ngene NC, Moodley J (2020). Improving the safety of induction of labor in low-resource settings using a 20-point toolkit. International Journal of Gynecology & Obstetrics 151(2):300-301. |
|
|
Nikolajsen T, Nielsen F, Rasch V, Sorensen PH, Ismail F, Kristiansen U (2011). Uterine contraction induced by Tanzanian plants used to induce abortion. Journal of ethnopharmacology 137(1):921-925. |
|
|
Rijken MJ, Lee SJ, Boel ME, Papageorghiou AT, Visser GH, Dwell SL, McGready R (2009). Obstetric ultrasound scanning by local health workers in a refugee camp on the Thai-Burmese border. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 34(4):395-403. |
|
|
Savitz DA, Terry JW, Dole N, Thorp JM, Siega-Riz AM, Herring AH (2002). Comparison of pregnancy dating by last menstrual period, ultrasound scanning, and their combination. American Journal of Obstetrics and Gynecology 187(6):1660-1666. |
|
|
Sigalla GN, Mushi D, Meyrowitsch DW, Manongi R, Rogathi JJ, Gammeltoft T, Rasch V (2017). Intimate partner violence during pregnancy and its association with preterm birth and low birth weight in Tanzania: A prospective cohort study. PLoS One 12(2):e0172540. |
|
|
Taipale P, Hiilesmaa V (2001). Predicting delivery date by ultrasound and last menstrual period in early gestation. Obstet Gynecol 97(2):189-94. |
|
|
The American College of Obstetricians and Gynecologists (2014). Practice bulletin no. 146: Management of late-term and postterm pregnancies. Obstetrics and gynecology 124(2 Pt 1):390. |
|
|
United Nations Population Division (2017). Total fertility rate (live births per woman): United Nations Statistics Division [updated 2013 Aug 20. |
|
|
Whitworth M, Bricker L, Mullan C (2015). Ultrasound for fetal assessment in early pregnancy. The Cochrane database of systematic reviews (7):Cd007058. |
|
|
World Health Organization (WHO) (2011). WHO recommendations for induction of labour: Geneva: World Health Organization. |
|
|
World Health Organization (WHO) (2017). Preterm Birth: World Health Organization; [updated November 2017. |
|
|
World Health Organization (WHO) (2016). WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. Geneva: World Health Organization. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


