Full Length Research Paper

ABSTRACT
In patients with HIV infection, wasting has been associated with increased mortality. Even in the era of Highly Active Antiretroviral Therapy (HAART), accelerated disease progression, loss of muscle protein mass, and impairment of strength and functional status are common. However, data on the magnitude of wasting and its risk factors among individuals receiving HAART are scarce in Ethiopia. The aim of this study is to determine the magnitude of wasting and identify associated factors among adults on HAART at anti-retroviral therapy clinics of Hosanna town. Facility based cross-sectional study was conducted from March 20 to April 30, 2014 among 410 adult people on (HAART) at ART health clinics of Hosanna town. Sample clients were selected by simple random sampling technique. Data were collected by face to face, record review using check list and weight scale measurement. Descriptive statistics, Bi-variate and multivariable logistic regression models were done using SPSS version 16 to identify factors associated with wasting. In total, 410 adult people on HAART participated in the study giving a response rate of 97.56%. The overall magnitude of wasting in this study was 37.1%. Food insecurity (AOR= 2.1, 95% CI: 1.28- 3.34), inadequate diversified diet (AOR= 2, 95% CI: 1.18- 3.38), low meal frequency (AOR= 2.2, 95% CI: 1.1- 4.47) and presence of opportunistic infections (AOR= 2.27, 95% CI: 1.47- 3.49) were independent predictors of wasting. Wasting was found to be high (37.1%) among adults on anti-retroviral therapy at ART Clinics of Hossana town. ART intervention should be supported by strategies that can address household food security, nutritional practices and prevention and control of opportunistic infections to improve the health status of people on HAART.
Key words: Anti-retroviral therapy, HIV/AIDs, wasting, weight loss, Hosanna, town clinic.
INTRODUCTION
More than 200 million people in SSA are chronically undernourished, and greater than 33 million are living with HIV infection (WHO, 2008). The HIV epidemic remains one of the main public health challenges, especially in low and middle income countries. In Sub-Saharan Africa (SSA) an estimated 1.9 million people became infected with HIV in 2011. Ethiopia is one of the most seriously affected countries, with a large number of people (approximately 800,000) living with HIV/AIDS and 44,751 AIDS-related deaths in 2011 (WHO, 2011). The EDHS (2011) showed that HIV prevalence in Ethiopia is 1.9% for women and 1.0% for men with an overall prevalence of 1.5%. This remains unchanged from the HIV prevalence reported in 2005 (1.4%) (CSA, 2011).
In Ethiopia, since the advent of the ART program, more than 200,000 people have started treatment in about 500 facilities throughout the country. ART service expansion has been recent and fast from only four facilities in 2003 to 517 in 2009. Parallel with this, the number of people who have accessed ART has also increased substantially from 900 in 2003 to 211,000 in 2009. The impact of the program on the survival and quality of life of patients has also been demonstrated. The drugs used in the country are the 3-Drug Regimen- Tenofovir (TDF) / Zidovudine (AZT) + Lamivudine (3TC) + Efavirenz (EFV) and the 2-Drug Regimen- (Tenofovir (TDF) + Lamivudine(3TC)) (MOH, 2007, 2009).
According to the Center of Disease and Control Definition, CDC, wasting is defined as a rapid rate of Body Weight Loss (BWL) (>5% in 6 months) (Wanke, 2000). In patients with HIV infection wasting has been associated with increased mortality (Kotler et al., 1998), accelerated disease progression (Wheeler et al., 1998), loss of muscle protein mass (Yarasheski et al., 1999) and impairment of functional status (Grinspoon et al., 1999). A weight loss of as little as 5% has been associated with increased morbidity and mortality (Wheeler et al., 1998).
The accessibility of Highly Active Anti-Retroviral Therapy (HAART) has extended the lives of many people with HIV/AIDS and greatly reduced morbidity and death due to AIDS and related complications (World Bank, 2007). But, morbidity and mortality related to HIV infection in resource limited setting remains unacceptably high, despite major advances in HIV therapy and increased international funding (WHO, 2007). During HAART era, HIV infection has become a chronic, manageable disease and HIV-associated weight loss and wasting were among the most frequently occurring AIDS – defining conditions during the pre-HAART era. The expectation was that viral control and the immunological recovery with ART and prophylaxis for OI would eliminate nutritional concerns in HIV-infected people. However, weight loss and wasting remain significant problems for adults and children, even in the era of HAART. However, evidences gap exist that show the prevalence of wasting and associated factors among adults on exits in Ethiopia. Moreover, no previous studies have been conducted particularly in the study area. Therefore, this revealed the magnitude of wasting and associated factors among adults on antiretroviral therapy (ART) in ART clinics of Hosanna town, Hadiya zone, Southern Ethiopia.
MATERIALS AND METHODS
Study design and study setting
A facility based cross sectional study was conducted from March 20 to April 30, 2014. The study area is Hossana town, which is 230 km from Addis Ababa, the capital of Ethiopia. There are only two ART units in the town; Nigist Elenie Memorial Referral Hospital and Hosanna Health Center. A total of 3773 clients were on pre ART and ART care programs at these two care units. The source population was all adults aged 18 and older who are enrolled in HAART in the two health facilities. The study included adults on ART antiretroviral therapy willing to participate in the study and who followed ART for 6 months or longer. Individuals who were seriously ill and unable to participate in interview process were excluded. Moreover, pregnant women were also excluded from the study since weight gain during pregnancy may introduce measurement bias.
Sample size determination and sampling procedure
The required sample size was determined using single population proportion formula:
Considering the following assumptions: p=50% (proportion of wasted people on HAART) (EPHTI, 2006), Zα/2 is the value of the standard normal distribution corresponding to a significant level of alpha (α) of 0.05, which is 1.96 and desired degree of precision (d) of 5%, the computed sample size was 384 and by adding 10% non-response rate, the total sample size computed was 422. Lists of eligible ART clients were identified from ART data base before the data collection. There were 801 ART clients at the Hospital and 142 ART clients at the health Center. According to the total number of ART clients in each clinic, proportionate numbers of sample clients (358 from the Hospital and 64 from the health center) were assigned to each clinic. Study participants were selected by simple random sampling technique using random number computer generation method.
Data source and procedure
Four ART adherence counselors as data collectors and one health officer as supervisor were recruited. Data were collected using face to face interview, record review and weight measurements. Data on socio-demographic, economic, nutritional counseling and nutritional support, and lifestyle factors were collected using pre-tested structured questionnaire. Data on adherence in the last month were collected using pre-tested structured questionnaire. However, side effect of ART, duration of ART, opportunistic infections (OIs), weight records and CD4 cell count in the past 6 months and AIDS’ clinical stage were collected from record using check list.
Measurements
Wasting is defined as a rapid rate of Body Weight Loss (BWL) (>5% in 6 months) (Adriana et al., 2005). Wasting (% of weight loss) was calculated as an average weight of the six months minus current weight divided by the average weight and multiplied by hundred. Participants’ current weight was taken using a standard beam balance. Individual dietary diversity Score (IDDS) and meal frequency measured as a record of the 24 h recall of all food groups eaten by the respondents were taken and classified into the 12 food groups using the FAO/Nutrition and Consumer Protection Division recommended questionnaire (FAO, 2007); daily eating occasions over the 24-h period were asked and recorded (Seifu, 2007). Food insecurity was assessed by using a short version of the household food insecurity access scale (HFIAS) developed by the Food and Nutrition Technical Assistance (FANTA) project, which was adapted to individual level context (Coates et al., 2007).
For economic status, wealth analysis initially was performed. First, reliability test was performed using the economic variables included in measuring the wealth of the households. The variables which were used to compute the alpha value were entered into the principal component analysis to obtain wealth status.
Statistical data analysis
First data were edited, coded and entered into Epi data 3.1; data cleaning such as editing; recoding and checking for missing values were made after exporting to SPSS window version 16.0. The data analysis ranges from the basic description to the identification of potential factors of wasting. The basic descriptive summaries of patients’ characteristics and outcome of interest were computed using simple frequencies, cross tabulation, measure of central tendencies and measure of dispersions. Bi-variate analysis model was used to show the relation between wasting and various associated factors. Finally, all potential variables that result (P < 0.25) with the outcome variable were entered into multivariable logistic regression model to identify independent predictor of wasting. P-value < 0.05 was considered as statistically significant and odds ratio at 95% confidence interval is used to examine the precision and strength of association.
Data quality control
The questionnaire was adapted from previous literatures and modified into the study context. It was prepared first in English and translated into Amharic, and then retranslated back to English by an expert who is fluent in both languages to maintain consistency. Training was given for data collectors and supervisor on the objectives and methods of data collection. Pre testing of the questionnaire was made on 5% of sample clients from the nearby Woreda Health Centre a two week prior to the actual survey. Based on the feedback obtained from the pre-test, questions which need clarification were revised. Daily, the data were strictly revised for completeness, consistency, accuracy and clarity by the supervisors and principal investigator. In addition, the data were thoroughly cleaned and carefully entered into computer using Epi data version 3.1 and double entry verification. Weight of participants was taken using standard beam balance and the scale was checked at zero before and after each measurement.
Ethical statement
Ethical approval was sought from ethical review committee of Jimma University, College of Public Health and Medical Sciences and then submitted to Hadiya Zone Health Bureau, Nigist Elienie Mohammed Hospital, Hosanna Health Centre administrators and other concerned bodies to obtain their co-operation. Verbal consent was taken from each participant after the purpose of the study was explained. They were told to withdraw at any time from responding to questions. Participants were informed that all the data obtained from them will be kept confidential and any personal identifiers were not noted.
RESULTS
Socio- economic characteristics
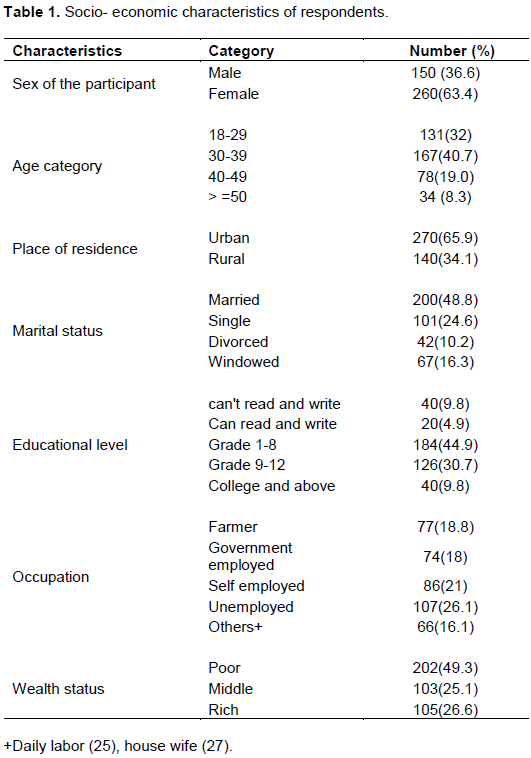
In total, 410 adults from HAART participated in the study giving a response rate of 97.56%.Out of 410 participants, female accounts for 260 (63.4%). The mean age of respondents was 34.67 (SD: 9.33), and 167 (40.7%) of them were in the age range of (30-39).
Majority of the respondents 270 (65.9%) live in urban areas. Two hundred forty eight (60.5%) of them are headed by maled, and 110 (26.8%) of them live with a family size of greater than or equal to five. Among the participants, 200 (48.8%) were married and 67 (16.3%) were windowed. Regarding educational status, 40 (9.8%) completed college and above. Concerning their occupation, 107 (26.1%) of the respondents were unemployed. Majority of the respondents 193 (58.5%) were Hadiya by ethnicity, and 196 (59.4%) were Protestants. About sixty percent of the respondents disclosed their HIV status. Majority of the participants 282(69%) took drinking water from pipe water. Regarding wealth status, 202 (49.3%) had poor economic status. Regarding life style situation, 3.2% did physical exercise and 10(3%) drank alcohol during the study period (Table 1).
Health care related factors
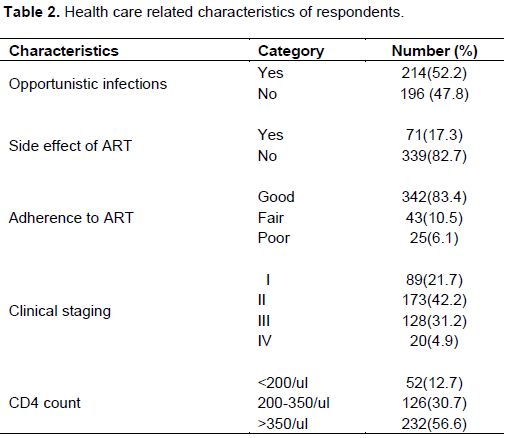
Of the total, 214(52.2%) were diagnosed with opportunistic infections (OIS) during the past six months before the survey. Out of the 214 OIS, 22.40% were diagnosed with tuberculosis, 49.60% were diagnosed with oral candidiasis and 28% were diagnosed with diarrhea during the past six months before the survey. Seventy one (17.3%) respondents had side effect of ART during the past two weeks before the survey. Nearly 5% of the participants 20(4.9 %) were at stage four and one hundred twenty eight (31.2%) were at stage three, during six months before the survey (Table 2). About 6% of individuals had poor adherence to ART. Out of 410 respondents, 52 (12.7%) had CD4count < 200 cells/μl (Table 2).
Dietary and food Security characteristics of respondents
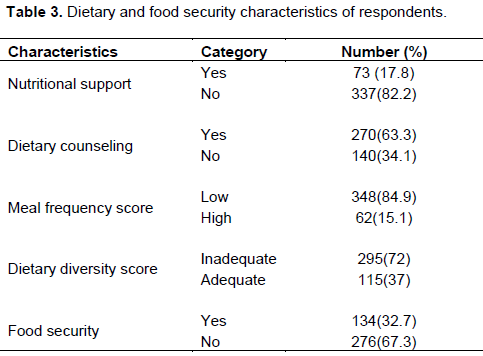
Majority of respondents, 271(82.1%) did not get nutritional support and 209(63.3%) of them were counseled about dietary feeding (Table 3). Larger proportion of the respondents (72%) had inadequate diversified food and (84.9%) had low meal frequency score within the 24 h dietary recall period. Larger proportions of the respondents (67.3%) were identified as food insecure (Table 3).
Prevalence of wasting among people on HAART
Overall, the prevalence of wasting (BWL >5%) in this study was 37.1% (Figure 1) and females were most affected (18.79%).
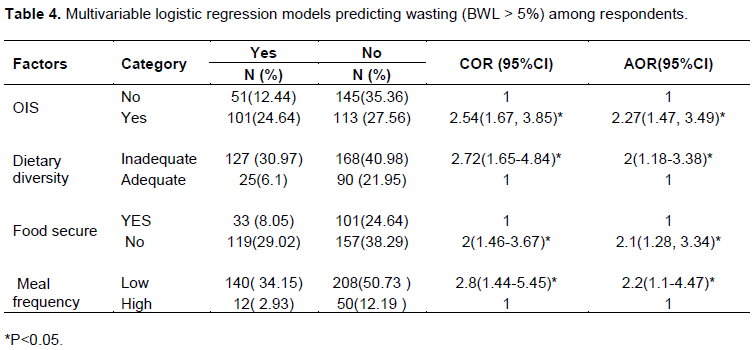
Factors associated with wasting among people on HAART
Variables with p-value <0.25 in the bivariate analysis were entered to multivariable regression model by backward likely hood ratio. Interaction effect and multi linearity were assessed; both were not found. In addition, variables did not meet the assumption of X2-tests were excluded before multivariable model. In the multivariate analysis, food insecurity (AOR= 2.1, 95% CI: 1.28- 3.34), inadequate diversified diet (AOR= 2, 95% CI: 1.18- 3.38), low meal frequency (AOR= 2.2, 95% CI: 1.1 to 4.47), and presence of opportunistic infections (AOR= 2.27, 95% CI: 1.47- 3.49) were independent predictors of wasting (Table 4). Participants who were diagnosed with OIS during the past six weeks were more than two times likely to be wasted than not infected with OIS (AOR= 2.27, 95% CI: 1.47 to 3.49) (Table 4).
DISCUSSION
The overall prevalence of wasting was 37.1%. Earlier studies revealed that the magnitude of weight loss (BWL>5%) in Boston (USA) was 21% (Wanke et al., 2000). This high prevalence of wasting in this study could be due to high prevalence of food insecurity which leads to lack of access to adequate, safe and nutritious food resulting in weight loss (Paluku et al., 2011). The results of this study identified food insecurity, inadequate dietary diversified diet, presence of opportunistic infections and low meal frequency as predictors of wasting (BWL > 5%) at p<0.05 among adults on ART. Participants who were diagnosed with OIS during the past six weeks were more than two times likely to be wasted than those not infected with OIS (AOR= 2.27, 95% CI: 1.47- 3.49). This result is in line with the study conducted in Boston (Grinspoon et al., 2003, Mangili et al., 2006). In addition, participants who had low meal frequency were more than two times likely to be wasted than who have high meal frequency (AOR= 2.2, 95% CI: 1.1-4.47). This result is in agreement with the study conducted at Boston (Grinspoon et al., 2003, Mangili et al., 2006). Respondents who were food insecure were more than two times likely wasted than those who were food secure (AOR= 2.1, 95% CI: 1.28- 3.34). This result is supported by a study done in Malawi.
This finding is in agreement with a study conducted at Miami–Dade County and resource limited setting (Paluku et al., 2011; Adriana et al., 2005). Participants who were taking inadequate diversified were two times more likely to be wasted than who have adequate diversified food (AOR= 2, 95% CI: 1.18- 3.38).This result is supported with a study conducted in Zambia (Kelly et al., 1999).
The present study has the following limitations. The first is recall bias may limit subjects to remember components of their nutritional intake and respondents may not tell the real information about their food security status due to the need for aid. The second is, cause -effect association cannot be determined since the study design is cross sectional.
In conclusion, wasting was found high among adult people on HAART in the study area. The current care and treatment ways of ART did not address the issues of wasting. So, intervention strategies should address the issues of food insecurity, inadequate diversified diet, low meal frequency and presence of opportunistic infections among people on HHART.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adriana C, Yang Z, Shenghan L, Lihua X, Craig P, Sabrina S (2005).HIV-Related Wasting in HIV-Infected Drug Users in the Era of Highly Active Antiretroviral Therapy Clinical Infectious Diseases 41(8):1179-1185. |
|
|
Central Statistical Agency (CSA) (2011). EDHS, Ethiopia, Addis Ababa, CSA, 2011. |
|
|
Coates J, Swindale A, Bilinsky P (2007). Household Food Insecurity Access Scale (HFIAS) for Measurement of Household Food Access: Indicator Guide Version 3. Food and Nutrition Technical Assistance Project Academy for Educational Development, Washington DC. |
|
|
Ethiopia Public Health Training Initiative (EPHTI), Carter Center, Ethiopia Ministry of Health, and the Ethiopia Ministry of Education (2006). Research Methodology |
|
|
Food and Agriculture Organization (FAO) (2007). Nutrition and Consumer Protection Division: Guidelines for Measuring Household and Individual Dietary Diversity. FAO, Rome. |
|
|
Federal Ministry of health (FMO) (2007). National guidelines for comprehensive HIV prevention, care and treatment. Addis Ababa, Ethiopia. |
|
|
Grinspoon S, Corcoran C, Rosenthal D, Stanley T, Parlman K, Costello M, Treat M, Davis S, Burrows B, Basgoz N, Klibanski A (1999). Quantitative assessment of cross-sectional muscle area, functional status and muscle strength in men with the AIDS wasting syndrome. Journal of Clinical Endocrinology and Metabolism 84:201-206. |
|
|
Grinspoon S, Mulligan K (2003). Weight Loss and Wasting in Patients Infected with Human Immunodeficiency Virus. Clinical Infectious Diseases 36(2):S69-S78, |
|
|
International Bank for Reconstruction and Development/the World Bank (2007). HIV/AIDS, Nutrition, and Food Security: What We Can Do, a Synthesis of International Guidance. |
|
|
Kelly P, Musonda R, Kafwembe E, Kaetano L, Keane E, Farthing M (1999). Micronutrient supplementation in the AIDS diarrhoea-wasting syndrome in Zambia: a randomized controlled trial. AIDS. 1999:13(4):495-500. 2811802. |
|
|
Kotler D, Tierney A, Wang J, Pierson R (1998). Magnitude of body-cell mass depletion and the timing of death from wasting in AIDS. American Journal of Clinical Nutrition 50:444-447. |
|
|
Mangili A, Murman D, Zampini M, Wanke C (2006). Nutrition and HIV Infection: Review of Weight Loss and Wasting in the Era of Highly Active Antiretroviral Therapy from the Nutrition for Healthy Living Cohort. Clinical Infectious Diseases 42(6):836-842. |
|
|
MOH/HAPCO (2008). Effectiveness of ART Program in Ethiopia. Addis Ababa: unpublished. |
|
|
Paluku B, Hedwig D, Theresa B, Angella M, Steve C (2011).Impact of household food insecurity on the nutritional status and the response to therapeutic feeding of people living with human immunodeficiency virus. Patient Preference and Adherence 5:619-627 |
|
|
Seifu A (2007). Impact of Food and Nutrition Security on Adherence to Anti-Retroviral Therapy (ART) and Treatment Outcomes among Adult PLWHA in Dire. Dawa Provisional Administration, Dire Dawa. |
|
|
Wanke CA, Silva M, Knox TA, Forrester J, Speigelman D, Gorbach SL (2000). Weight loss and wasting remain common complications in individuals infected with human immunodeficiency virus in the era of highly active antiretroviral therapy. Clinical Infectious Diseases Volume 31(3):803-805. |
|
|
Wheeler DA, Gibert CL, Launer CA, Muurahainen N, Elion RA, Abrams DI, Bartsch GE (1998). Weight loss as a predictor of survival and disease progression in HIV infection. Journal of Acquired Immune Deficiency Syndromes 18:80-85. |
|
|
WHO, UNAIDS and UNICEF (2011). GLOBAL HIV/AIDS Response Epidemic Update and Health Sector Progress towards Universal Access, Progress Report. |
|
|
World Health Organization (WHO) (2008).Joint United Nations Programme on HIV/AIDS (UNAIDS), report on the global AIDS epidemic. Geneva: UNAIDS and the World Health Organization World Health Organization (WHO) (2007). Joint United Nations Programme on HIV/AIDS (UNAIDS), AIDS Epidemic Update. UNAIDS and the World Health Organization, Geneva. |
|
|
Yarasheski K, Zachwieja J, Gischler J, Crowley J, Horgan M, Powderly W (1998). Increased plasma Gln and Leu R(a) and inappropriately low muscle protein synthesis rate in AIDS wasting. American Journal of Physiology 275:E577-E83. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


