Full Length Research Paper

ABSTRACT
The Human Immunodeficiency Virus (HIV) is a neurotropic virus that is associated with cognitive, behavioral and motor deficits known as HIV Associated Neurocognitive Disorder (HAND). This was a prospective study aimed at determining the prevalence of cognitive impairment as well as comparing the performance of the HIV positive patients on a screening test, the International HIV Dementia Scale (IHDS), and subtests drawn from a neuropsychological test battery - WHO/UCLA. The screening test and neuropsychological test battery were administered to HIV positive patients while the HIV negative patients had only the test battery administered to determine the mean score of each test domain. Neurocognitive impairment was defined using the cut-off score of 10 for the International HIV Dementia scale and Z scores greater than 1 SD in at least two domains of the neuropsychological test battery. The mean performance on each domain of the test battery was determined after administration to the HIV negative individuals. Ninety-two HIV positive patients (57 females and 35 males) and ninety-two age, sex and education matched HIV negative subjects (46 females and 46 males) were enrolled into the study. The median age and interquartile range were 33(26-39) and 35(27-46) for the HIV positive and negative participants respectively. The prevalence estimates of cognitive impairment determined by the IHDS and the test battery were 42.4 and 76.1%, respectively. The IHDS in this study was found to have a sensitivity of 50% and a specificity of 81% for HAND. Neurocognitive impairment still persists in the combination anti-retroviral therapy (CART) era and is better accessed using neuropsychological testing than with screening tests although the former is cumbersome and require expertise and patience on the part of the subjects.
Key words: HIV, neurocognitive disorder, sub-Saharan Africa, dementia tests, neuropsychology.
INTRODUCTION
The Human Immunodeficiency Virus (HIV) is a neurotropic virus and can affect all components of the neuraxis. Sub-Saharan Africa (SSA) accounts for about 12% of the world’s population but contributes about 71% to the global burden of HIV with a significant number of infections occurring in South Africa and Nigeria (Kharsany and Karim, 2016). Some of the documented CNS manifestations in SSA include fulminant encephalopathy, neurologic Immune Reconstitution Syndrome (IRIS), HIV associated Neurocognitive Dysfunction (HAND), CNS opportunistic infection, lymphoma, stroke, vacuolar myelopathy and distal symmetric polyneuropathy (DSPN) (Alkali et al., 2013). The cells of the nervous system express the cytokine receptor, CXCR4, that facilitates the entrance of the virus to the CNS and its effects on the CNS are mediated through direct and indirect mechanisms (Hult et al., 2008; Ellis et al., 2009).
Neurocognitive dysfunction (NCD), one of the manifestations of CNS disease in HIV, is characterized by cognitive, motor and behavioral abnormalities not attributable to any other cause other than HIV (Sanmarti et al., 2014). Prior to 1991, only one form of neurocognitive dysfunction was known and was termed HIV-associated dementia (HAD). It was found predominantly in HIV patients with advanced disease and was associated with motor and behavioral changes (Sanmarti et al., 2014). However, with the widespread use of CART, milder forms of cognitive dysfunction became more common (Heaton et al., 2010). This led to an evolution in the terminology for HAND with the most recent one being the Frascati’s criteria (Antinori et al., 2007). Although HAND was thought to be more common in Europe and North America, it is now being considered equally as prevalent in other regions but may be under-reported and under-diagnosed (Modi et al., 2018). In the United States, the effect of CART on the progression of HAND has also been documented (Robertson et al., 2007; Sacktor et al., 2016).
In Sub-Saharan Africa, data regarding the exact prevalence, profile and effect of HAART on the progression of HAND is sparse. The incidence of HAND in SSA, and globally as well, exhibits wide variation. One of the reasons for this difference lies in the way it is assessed. This could be done with the use of screening tests and confirmatory comprehensive neuropsychological testing for those who have sub-optimal scores that raise suspicion for impairment on screening. It is recommended to screen newly diagnosed patients preferably prior to the commencement of HAART, and to follow up with a neuropsychological evaluation for patients who have abnormal test scores (The Mind Exchange Working Program, 2013). A number of screening tools have been devised for this purpose but neuropsychological test batteries, which are more difficult to administer, are the gold standard. Some of the screening tests employed in HAND research include the HIV Dementia Scale (HDS), IHDS, Mini-mental State Examination (MMSE), Montreal Cognitive Assessment scale (MoCA) and Neuroscreen (Power et al., 1995; Sacktor et al., 2005; Folstein et al., 1975; Nasreddine et al., 2005; Robbins et al., 2007). However, only a few of them like NeuroScreen (in South Africa) and IHDS (in South Africa and Uganda) have been validated in SSA (Sacktor et al., 2005; Robbins et al., 2007). The IHDS is the most widely used screening test in SSA and assesses the cognitive domains that are involved in HAND (Rosca et al., 2021; Mwangala et al., 2019). These deficits consist mainly of mental slowness, attention and memory dysfunction, and impaired executive function (Woods et al., 2009). In the CART era, problems with concentration, attention and memory are increasingly being recognized (Eggers et al., 2017). Screening tests have the advantage of ease of use and can even be administered by non-clinicians whereas neuropsychological tests are more cumbersome and can only be administered by adequately trained personnel. Other impediments to the use of neuropsychological testing in the developing world include overwhelming disease burden for the clinicians, geographical factors and infrastructural deficiencies, adaptation and cultural appropriateness of tests (Robertson et al., 2009; Nyamayaro et al., 2019). Furthermore, they do not have specified cut-off marks like screening tests, but rely on the development of normative data in the environment they are to be used. This data serves as the baseline performance for the population of concern and comparison made with those of patients with adequate matching for age, sex and educational status. To date, only a few countries have test norms collected and published for use in their environment, a gap that neuro-AIDS researchers are striving to fill (Robertson et al., 2016).
In spite of advances in HAND research, there remains a lack of consensus on the use of both screening and neuropsychological tests in the assessment of HAND. In this study, we attempted to compare the prevalence rate of neurocognitive impairment using the IHDS to that ascertained using a neuropsychological test battery and to determine the sensitivity and specificity of the screening tool in comparison to the neuropsychological test battery. It also aimed to complement the few studies done in SSA that utilized both a screening test and a NP test battery for evaluating HIV related neurocognitive impairment (NCI).
METHODOLOGY
This was a cross-sectional study conducted at a tertiary teaching hospital, Nnamdi Azikiwe University Teaching Hospital, Nnewi, in South-East Nigeria. The HIV negative participants were matched for age, sex and level of education. Ethical approval was obtained from the ethical committee of the institution and informed consent was obtained from both categories of participants ahead of enrollment.
The HIV positive participants were recruited from the specialized antiretroviral clinic of the hospital which provides comprehensive HIV counseling, care and medication. The HIV negative participants were drawn from the hospital community.
Patients considered eligible for inclusion were between 18 and 65 years of age who gave consent to participate; had no history of drug abuse/alcohol abuse; had no history of mental illness; were not known to have any medical conditions like chronic kidney disease, chronic liver disease, cerebrovascular accident, epilepsy and head trauma; were literate enough to obey instructions with a minimum of completed primary school education. Patients were excluded if they had some physical deformity that could interfere with their abilities to carry out instructions requiring motor activity; and if they had any acute illnesses, delirium and encephalopathy, fever, headache and focal neurologic signs (like cranial nerve 3 or 6 palsy or hemiparesis). Similar criteria were applied to the HIV negative individuals in addition to a negative HIV screening test. Patients’ demographic characteristics were collected using a structured questionnaire which was also designed to assist with identifying inclusion and exclusion criteria. Neurologic examination was performed with emphasis on the pupils, cranial nerve abnormalities, muscle power, tone and reflexes, involuntary movements, cerebellar examination and sensation.
Neuropsychological assessment was done using both the International HIV Dementia Scale and a limited neuropsychological test battery. The IHDS is a screening tool for neurocognitive impairment in HIV and consists of 3 subtests: Timed finger tapping, a measure of motor speed; timed alternating hand sequence test which assesses psychomotor speed, and finally, recall of 4 words in 2 min which assesses memory registration and recall. Performance on each of these subtests is rated on a scale 0 to 4 with a maximal score of 12. The recommended cut-off score of 10 that raises suspicion for neurocognitive impairment was utilized in this study. This was administered only to the HIV positive participants.
The subtests of the neuropsychological test battery were drawn from the WHO/UCLA test battery. The only subtest that was not used from the test battery was the Picture Memory Interference test. The Escala de Inteligencia Wechsler Para Adultos (EIWA) digit symbol and EIWA block design were substituted with the Wechsler Adult Intelligence Scale (WAIS) version for both tests. The functional domains tested by this battery includes motor speed/fine motor control (timed gait, finger tapping, color trails 1 and 2, WAIS block design, WAIS digit symbol, grooved pegboard, trail making A); sustained attention (color trails 1 and 2, trail making A); selective attention (color Trails 2, WAIS digit symbol); cognitive flexibility (color trails 2, WAIS digit symbol); perceptual/motor analysis (WAIS block design); verbal memory (WHO/UCLA Auditory Verbal Learning Test); verbal fluency (verbal fluency, animals and verbal fluency, first names). Those whose performance was 1 SD in 2 or more domains of the battery were categorized as mild cognitive impairment whereas those whose scores were 2 SD or more were categorized as moderate to severe cognitive impairment. The HIV negative participants also had the questionnaire and the neuropsychological test battery administered on them.
Data was collected, scrutinized for normality and analyzed using SPSS version 23.0. Quantitative data was presented as median and interquartile range and analyzed with Mann-Whitney U test. Categorical variables were described using frequency counts and percentages and analyzed with chi-square.
RESULTS
Socio-demographic variables of the study participants
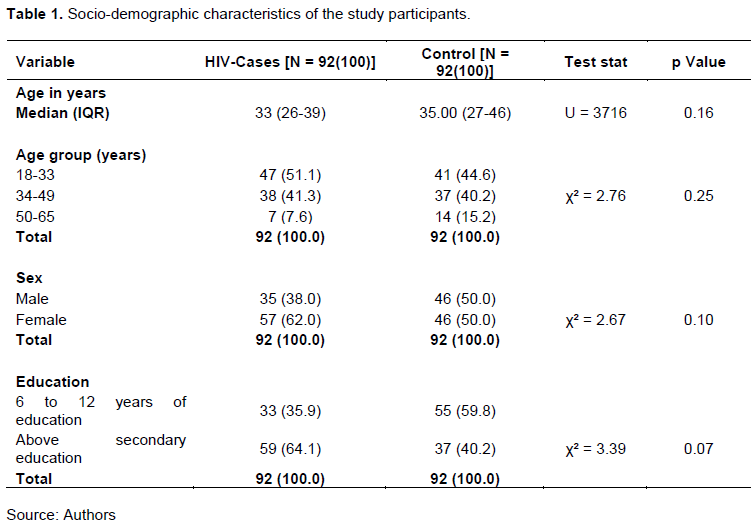
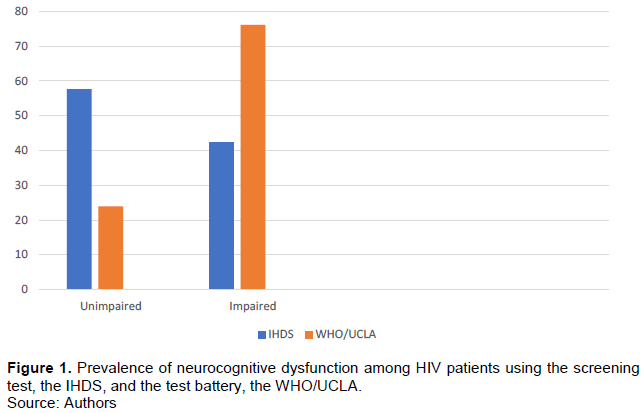
A total of one hundred and eighty-four subjects (184) consisting of ninety-two (92) HIV positive patients (57 females and 35 males) and ninety-two (92) HIV negative subjects (46 females and 46 males) were enrolled into the study (Table 1). The HIV patients comprised of thirty-eight (38) CART-exposed and fifty-four (54) CART naïve patients. The differences between the age, sex and level of education between the HIV positive patients and HIV negative controls were not statistically significant. After the age range of the study participants were further stratified to enable matching by age, the differences between them also were not statistically significant Figure 1 shows the prevalence of cognitive impairment with the IHDS using the recommended cut-off value of 10. Of the 92 HIV positive cases, 39 (42.4%) were found to have scores below 10 and 53 (57.6%) had scores of 10 or more. The raw scores of the HIV positive patients on the test battery were converted to Z scores. Cognitive impairment was defined as scores above 1 SD in at least 2 domains of the test battery. 70 (76.1%) out of the 92 HIV positive patients were found to be impaired; 41(44.6%) had scores that were 1 SD in at least two domains of the test battery (mild cognitive impairment) and 29 (31.5%) had scores that were 2 SD in at least two domains of the test battery.
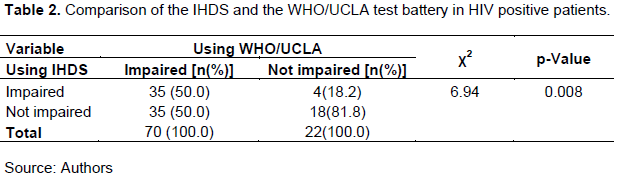
The comparison of the sensitivity and specificity of the IHDS and the neuropsychological test battery of the 39 persons identified as cognitively impaired by the IHDS, 35 were also identified by the WHO/UCLA test battery as cognitively impaired. Of the 70 persons identified as cognitively impaired by the WHO/UCLA test battery, only 35 of them were identified as cognitively impaired by the IHDS. The sensitivity of the IHDS in this study was 50% and specificity was 81%. This is shown in Table 2.
DISCUSSION
The prevalence rate of NCI in this study with the IHDS was found to be 42.4% using the recommended cut-off point of 10. The prevalence of 42.4% in this study is close to 42.3% for pre-CART patients reported in a meta-analysis in sub-Saharan Africa (Habib et al., 2013). The prevalence in this study is however for both CART-exposed and CART naïve patients limiting direct comparison. Our finding of 42.4% was however lower than the prevalence rates of 54.3% (for CART-exposed) and 67.8% (CART status unspecified) reported in two previous studies in Nigeria that utilized the IHDS (Oshinaike et al., 2012; Osaigbovo, 2018). The higher prevalence reported in these later studies compared to that in the meta-analysis may be indicative of the fact that recent studies are utilizing more sensitive tests to detect HAND than was possible in the pre-CART era. Globally, the rates of cognitive impairment in the CART era is thought to be somewhere between 15 to 55% although a prevalence rate as high as eighty-eight percent (88%) has been reported in Africa (Sacktor, 2018; Mugendi et al., 2019). The variation in prevalence rates between Africa and elsewhere could possibly be the result of differences in viral clades, heterogeneity of the study samples and the tools employed in assessment of cognition.
Regarding the IHDS, several cut-off points have been investigated and a cut-off of 10 was found in another meta-analysis to have a sensitivity of 0.646 and specificity of 0.647 for detecting HAND and is most widely used (Rosca et al., 2021). To emphasize its diagnostic utility, it had been compared to the MMSE and found to be more sensitive to cognitive impairment in HIV patients (Oshinaike et al., 2012; Nyudo et al., 2016; Kami-Onaga et al., 2018). However, a meta-analysis of the various screening tests employed in the diagnosis of HAND in SSA produced variable results with no consensus on the optimal screening test for the diagnosis of HAND (Haddow et al., 2013). Some of them, however, are considered more sensitive than the others.
Several neuropsychological test batteries have been employed for the diagnosis of HAND. Most of them, however, are difficult to administer and are yet to be validated in SSA. The choice of the test battery employed in this study stems from the fact that it was formulated to be culture fair, included domain subtests that are less dependent on language abilities and incorporated items that are universally recognizable; two African countries were also part of the pilot phase of its trial (Maj et al., 1993, 1994). Some of the subtests included, for example, the WHO/UCLA auditory verbal learning test were specifically designed for this battery. Unlike the Rey-Auditory verbal learning test it is modeled after it includes only items that are universal. Apart from the WHO/UCLA Auditory Verbal Learning Test component, other subtests do not require translation to language of the test taker. It also contains the grooved pegboard, the most commonly used test of motor function in studies that used comprehensive testing in SSA (Mwangala et al., 2019). Although neuropsychological testing is more sensitive to cognitive impairment in HIV, it is more likely to overestimate it by about 8 to 13% (Nightingale et al., 2014). This is especially with regards to mild forms of impairment with scores between 1 and 2 SD in two or more domains. This is because the more domains that are tested, the higher the likelihood of getting an abnormal test score and declaring a normal individual impaired - a false positive result (Rosca et al., 2021). However, they are more likely to detect impairment if present since most of them can assess the different functional domains involved in the pathogenesis of HAND.
Despite the utility of the IHDS in the assessment of HAND, it still falls short of the ideal screening tool. In this study, the prevalence rate of cognitive impairment (42.4%) using IHDS is far below 76.1% obtained with the neuropsychological test battery and the battery was able to detect 90% of those found impaired on the screening test. These facts highlight the superiority of neuropsychological testing. The sensitivity of the IHDS in this study was 50% and specificity was 81% which is not an optimal result for a screening test. The sensitivity and specificity in this study compares favourably well with that (68 and 86% respectively) in a previous study conducted in South Africa (Joska et al., 2016). The IHDS in this study was found to have a positive predictive value of 90% and a negative predictive value of 34%. The cognitive domains involved in HIV- associated neurocognitive dysfunction include executive function, episodic memory, speed of information processing, motor skills, attention and working memory and language and sensory perception (Sanmarti et al., 2014). Furthermore, to effectively assess HAND, it should be ascertained that impairment cuts across at least 2 of these domains (Antinori et al., 2007). Most screening tools are not extensive enough to assess all of these domains and therefore cannot be used to classify patients using the Frascati’s criteria for the diagnosis of HAND. The IHDS, for instance, assesses only memory, psychomotor functioning and motor speed (Sacktor et al., 2005). Another shortcoming of screening tests is that some of them are more suited for assessment of cognitive domains that are less likely to be involved in HAND. HAND is thought to present in its initial phase as a subcortical dementia although at a mixed pattern has become more common in the CART era (Sacktor, 2018). Although screening tests can be deployed easily in the clinic setting and administered by non-clinicians, this convenience is faltered by their lack of sensitivity.
Currently, the approach towards detection and management of HAND is to first administer screening tools followed by NP testing for those who have scores suspicious for neurocognitive impairment (The Mind Exchange Working Program, 2013). However, as this work reveals, it is possible that patients who have optimal scores on screening tests, and are excluded for more comprehensive testing, could still have NCI. This approach seeks to exclude those found to be falsely labeled as impaired (the false positive cases) but fails to address those erroneously declared as unimpaired (false negative cases) on screening. For instance, some HIV positive individuals who screened negative on the IHDS at a cut-off of 10 still performed badly on tests of executive function in South Africa (Joska et al., 2011). Adopting this recommendation could mean exclusion of the latter subset of patients, those found negative on screening and who may be at risk of progressing to more significant impairment, from further evaluation with neuropsychological testing. Devising more sensitive screening tests or limited and brief neuropsychological test batteries that incorporates subtests that are culture fair would be ideal. Such tests that are less prone to influence by language and educational status and excludes tests with high degree of abstraction will ensure that candidates who are at risk of impairment are not missed. Another approach that combines multiple screening tests like the IHDS and MoCA or the cognitive assessment tool-rapid version (CAT-rapid) could improve the accuracy of screening tests for the detection of cognitive impairment in HIV patients (Joska et al., 2016; Rosca et al., 2021).
LIMITATION
Neuroimaging is essential for ruling out co-morbidities and confounders in the assessment of HAND but was not utilized in this study due to cost. However, symptoms like headache, fever, early morning vomiting and neurologic signs like asterixis, myoclonus, ocular motor signs and spasticity that may suggest an alternative diagnosis were sought for and used to exclude patients. The length of time required for the administration of the neuropsychological test battery used was long and a few patients opted out because of that. It may therefore not be ideal for routine use in the clinical setting.
CONCLUSION
Neurocognitive impairment still persists in the cART era in SSA although its prevalence is very likely underestimated. Although a number of studies have been done with screening tests, it is obvious that they are not ideal for delineating cognitive impairment in HIV patients, especially, the mild forms. Screening in SSA should focus on the development and adaptation of tests that are sensitive to HIV related cognitive impairment. This may mean the addition of for example, the grooved pegboard to a screening test. Collection of normative data on these subtests may also have to be done to enable appropriate interpretation. This approach may hold potential for the development of concise, convenient and reliable screening tests for HAND in SSA.
CONFLICT OF INTERESTS
The authors have no conflict of interest to disclose.
ACKNOWLEDGEMENT
The authors thank all the subjects who volunteered time out of their very busy schedule to participate in this study. They are also grateful to the hospital’s ethical committee for approving the study and the antiretroviral clinic that allowed us to utilize their facility.
REFERENCES
|
Alkali NH, Bwala SA, Nyandaiti YW, Danesi MA (2013). NeuroAIDS in sub-Saharan Africa - A clinical review. Annals of African Medicine 12(1):1-10. |
|
|
Antinori A, Arendt G, Becker JT, Brew BJ, Byrd DA, Cherner M, Clifford DB, Cinque P, Epstein LG, Goodkin K, Gisslen M, Grant I, Heaton RK, Joseph J, Marder K, marra CM, McArthur JC, Nunn M. Price RW, Pulliam K, Robertson KR, Sacktor N, Valcour V, Wojna VE (2007). Updated research nosology for HIV-associated neurocognitive disorders. Neurology 69(18):1789-1799. |
|
|
Eggers C, Arendt G, Hahn K, Husstedt I, Maschke M, Neuen-Jacob E, Obermann M, Rosenkranz T, Schielke E, Straube E (2017). HIV-1 associated neurocognitive disorder: epidemiology, pathogenesis, diagnosis, and treatment. Journal of Neurology 264:1715-1727. |
|
|
Ellis RJ, Calero P, Stockin M (2009). HIV infection and the central nervous system: a primer. Neuropsychology Review 19(2):144-151. |
|
|
Folstein MF, Folstein SE, McHugh PR (1975). Mini-mental state": A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research 12(3):189-198. |
|
|
Habib AG, Yakasai AM, Owolabi LF, Ibrahim A, Habib ZG, Gudaji M, Karaye KM, Ibrahim DA, Nashabaru I (2013). Neurocognitive impairment in HIV-1-infected adults in Sub-Saharan Africa: a systematic review and meta-analysis. International Journal of Infectious Disease 17(10):820-831. |
|
|
Haddow LJ, Floyd S, Copas A, Gilson RJ (2013). A systematic review of the screening accuracy of the HIV Dementia Scale and International HIV Dementia Scale. PLoS One 8(4). |
|
|
Heaton RK, Clifford DB, Franklin DR, Woods SP, Ake C, Vaida F, Ellis RJ, Letendre SL, Marcotte TD, Atkinson JH, Rivera-Mindt M, Vigil OR, Taylor MJ, Collier AC, Marra CM, Gelman BB, McArthur JC, Morgello S, Simpson Dm, McCutchan JA, Abramson I, Gamst A, Fennema-Notestine C, Jernigan TL, Wong J, Grant I; CHARTER Group (2010). HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: Charter Study. Neurology 75(23):2087-2096. |
|
|
Hult B, Chana G, Masliah E, Everall I (2008). Neurobiology of HIV. International Review of Psychiatry 20(1):3-13. |
|
|
Joska JA, Westgarth-Taylor J, Hoare J, Thomas KG, Paul R, Myer L, Stein DJ (2011). Validity of the international HIV dementia scale in South Africa. AIDS Patient Care STDS 25(2):95-101. |
|
|
Joska JA, Witten J, Thomas KG, Robertson C, Casson-Crook M, Roosa H, Crreighton J, Lyons J, Sacktor NC (2016). Comparison of five brief screening tools for HIV-associated neurocognitive disorders in the USA and South Africa. AIDS Behaviour 20(8):1621-1631. |
|
|
Kami-Onaga K, Tateyama M, Kinjo T, Parrott G, Tominaga D, Takahashi-Nakazato A, Nakamura H, Tasato D, Miyagi K, Maeda S, Arae H, Uehara H, Miyagi K, Haranaga S, Fujita J (2018). Comparison of two screening tests for HIV-associated neurocognitive disorder in suspected Japanese Patients with respect to cART usage. PLos One 13(6). |
|
|
Kharsany A, Karim Q (2016). HIV infection and AIDS in Sub-Saharan Africa: current status, challenges and opportunities. Open AIDS Journal 10:34-48. |
|
|
Maj M, Elia LD, Satz P, Janssen R, Zaudig M, Uchiyama C, Starace F, Galderisi S, Chervinsky A (1993) Evaluation of two new neuropsychological tests designed to minimize cultural bias in the assessment of HIV-1 seropositive persons: a WHO study. Archives of Clinical Neuropsychology 8(2):123-135. |
|
|
Maj M, Satz P, Janssen R, Zaudig M, Starace F, D'Elia L, Sughondhabirom B, Mussa M, Naber D, Ndetei D (1994). WHO neuropsychiatric AIDS study, cross-sectional phase II. neuropsychological and neurological findings. Archives of General Psychiatry 51(1):51-61. |
|
|
Modi G, Mochan A, Modi M (2018). Neurological manifestations of HIV. In: Advances in HIV and AIDS control, Samuel Okware, IntechOpen, London. |
|
|
Mugendi A, Kubo M, Nyamu D, Mwaniki L, Wahome S, Haberer J (2019). Prevalence and correlates of neurocognitive disorders among HIV patients on antiretroviral therapy at a Kenyan hospital. Neurology Research International. |
|
|
Mwangala P, Newton C, Abas M, Abubakar A (2019). Screening tools for HIV-associated neurocognitive disorders among adults living with HIV in Sub-Saharan Africa: a scoping review. AAS Open Research 30(1):1-22. |
|
|
Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, Chertkow H (2005). The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. Journal of American Geriatric Society 53(4):695-699. |
|
|
Nightingale S, Winston A, Letendre S, Michael BD, McArthur JC, Khoo S, Solomon T (2014). Controversies in HIV-associated neurocognitive disorders. Lancet Neurology 13(11):1139-1151 |
|
|
Nyamayaro P, Chibanda D, Robbins R, Hakim J, Gouse H (2019). Assessment of neurocognitive deficits in people living with HIV in Sub Saharan Africa. The Clinical Neuropsychologist 33(1):1-26. |
|
|
Nyudo A, Ndetei D, Othieno C, Mathai A (2016). The performance of International HIV dementia scale (IHDS) versus Mini Mental Status Examination Scale (MMSE) in assessment of HIV- associated neurocognitive disorders (HAND) among HIV-infected Tanzanian adults: a Case-Control Study. Tanzania Medical Journal Tanzania Medical Journal 28(2):49-65. |
|
|
Osaigbovo OG (2018). The International HIV Dementia Scale, a valuable screening instrument for HIV-associated neurocognitive disorder (HAND) in HIV infected adults in north-central Nigeria. African Journal of Medicine and Medical Sciences 47(2):65-71. |
|
|
Oshinaike OO, Akinbami AA, Ojo OO, Ojini IF, Okubadejo UN, Danesi AM (2012). Comparison of the Mini-mental State Examination Scale and the International HIV Dementia Scale in assessing cognitive function in Nigerian HIV patients on antiretroviral therapy. AIDS Research and Treatment 2012(2090-1240):581531. |
|
|
Power C, Selnes OA, Grim JA, McArthur JC (1995). HIV Dementia Scale: a rapid screening test. Journal of Acquired Immune Deficiency Syndrome and Human Retrovirology 8(3):273-278. |
|
|
Robbins RN, Gouse H, Brown HG, Ehlers A, Scott TM, Leu CS, Remein RH, Mellins CA, Joska JA (2007). A mobile app to screen for neurocognitive impairment: preliminary validation of NeurosScreen among HIV-infected South African Adults. JMIRM Health 6(1):1-13. |
|
|
Robertson KR, Nakasujja N, Wong M, Musisi S, Katabira E, Parsons TD, Ronald A, Sacktor N (2007). Pattern of neuropsychological performance among HIV positive patients in Uganda. BMC Neurology 7(8):1-7. |
|
|
Robertson K, Liner J, Heaton R (2009). Neuropsychological assessment of HIV-infected populations in international settings. Neuropsychology Review 19(2):232-249. |
|
|
Robertson K, Jiang H, Evans SR, Marra CM, Berzins B, Hakim J (2016). International neurocognitive normative study: neurocognitive comparison data in diverse resource-limited settings: AIDS Clinical Trials Group A5271. Journal of Neurovirology 22(4):472-478. |
|
|
Rosca EC, Tadger P, Cornea A., Tudor R, Oancea C, Simu M (2021). International HIV Dementia Scale for HIV-associated neurocognitive disorders: A systematic review and meta-analysis. Diagnostics (Basel) 11(6):1- 24. |
|
|
Sacktor NC, Wong M, Nakasujja N, Skolasky RL, Selnes OA, Musisi S, Robertson K, McArthur JC, Ronald A, Katabira E (2005). The International HIV Dementia Scale: a new rapid screening test for HIV Dementia. AIDS 19(3):1367-1374. |
|
|
Sacktor N, Skolasky R, Seaberg E, Munro C, Becker J, Martin E, Ragin A, Levine A, Miller E (2016). Prevalence of HIV-associated neurocognitive disorders in the Multicenter AIDS Cohort Study. Neurology 86(4):334-340. |
|
|
Sacktor N (2018). Changing clinical phenotypes of HIV-associated neurocognitive disorders. Journal of Neurovirology 24:141-145. |
|
|
Sanmarti M, Ibáñez L, Huertas S, Badenes D, Dalmau D, Slevin M, Krupinski J, Popa-Wagner A, Jaen A (2014). HIV-associated neurocognitive disorders. Journal of Molecular Psychiatry 2(2):1-10. |
|
|
The Mind Exchange Working Group (2013). Assessment , diagnosis , and treatment of HIV-associated neurocognitive disorder?:A consensus report of the Mind Exchange Program. Clinical Infectious Disease 56(7):1004 -1017. |
|
|
Woods SP, Moore DJ, Weber E, Grant I (2009). Cognitive neuropsychology of HIV-associated neurocognitive disorders. Neuropsychology Review 19(2):152-168. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


