Full Length Research Paper

ABSTRACT
In spite of the well proven benefits of antiretroviral therapy (ART) in prolonging life expectancy, being lost to ART follow-up is a problem to the success of antiretroviral therapy programs in resource limited countries including Ethiopia. Thus the aim of the study was to assess the magnitude and predictors of loss to follow-up among adult ART clients. A case-control study design was employed using patients’ chart review. For each case three controls were selected based on the closest day of enrollment. Both bivariate and multivariate logistic regression was performed to test association. A total of 727 adult patients were started on antiretroviral therapy during the study period. Among these, 80 (11%) were found to be lost from follow up for a period of ≥ 3 months and 240 controls were randomly selected for 80 cases in a ratio of 1:3. Presence of bereavement concern, not being provided with isoniazide (INH) prophylaxis, the presence of side effects and earlier periods after ART initiating were found to be associated with increased odds for being lost to follow up. The proportion of lost to follow up in this study was lower than those figures reported for resource poor countries. Thus, more targeted health education, counseling and follow-up is needed for patients with identified risk factors.
Key words: Antiretroviral therapy (ART), human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS), lost to follow up, Wukro hospital.
INTRODUCTION
Human immunodeficiency virus (HIV) continues to be a major global public health problem, having claimed more than 25 million lives over the past three decades (World Health Organization (WHO), 2006). No region of the world is spared but, developing countries in particular, in sub-Saharan Africa and part of Asia, have much higher rates of infection (WHO, UNAIDS, UNICEF, 2011). The effect of this disease extends to social, economic and political factors threatening the stability of those countries
with high disease burden (Dixon et al., 2001). Because of this unprecedented effect, it prompted a global response which included preventive, treatments and care strategies with the birth of antiretroviral therapy (ART) (WHO, 2010). Although, there is no cure for acquired immunodeficiency syndrome (AIDS), life-prolonging drugs (ART) have become more affordable and accessible to let people living with HIV have healthy and productive lives (Russell et al., 2007).
Ethiopia is one of the few countries with the highest number of people living with HIV/AIDS globally. The estimated number of people living with HIV/AIDS in 2011 was 790,000 and the reported number of people receiving antiretroviral therapy were 222,723 and AIDS deaths were 54,000 (WHO, 2006; WHO, UNAIDS, UNICEF, 2011). Task shifting and decentralization of the service was done in Ethiopia as an initiative to expand the availability of ART (Federal Ministry of Health, 2007; WHO/UNAIDS/UNICEF, 2009; Ministry of Health, 2005, 2006). Despite this, a large number of individuals who initiate ART do not receive long-term follow-up care. Understanding of lost to follow-up (LTFU) at every level is a key to design appropriate intervention and improve HIV care after ART initiation (Rueda et al., 2006). The rate to loss to follow up varied with period of follow up in different studies, for instance. the LTFU rate was 16, 25, and 40% after 6 months, one year and two years, respectively (Rueda et al., 2006; Brinkhof et al., 2008). In South African, nearly 30% were lost to follow-up within three years (Carole Leach-Lemens, 2010). A study conducted in Gonder University hospital in Ethiopia also revealed LTFU of 46% in one year treatment (Wubshet et al., 2012).
Factors such as age, having low baseline CD4-cell count, being ambulatory and financial constraints were found to be predictors for LTFU in many studies (Rueda et al., 2006; Wubshet et al., 2012). Other reasons for LTFU were, improvement in health, adverse effects and feeling sick or being hospitalized (Braitstein et al., 2006; Ammassari et al., 2002). Stigma and social problems such as fear of disclosure and social isolation were also identified as barriers to treatment adherence (Hardon et al., 2007; Ammassari et al., 2001). Patients also reported cost of care and difficulties in taking their drugs when they were among employers or friends as barriers for ad-herence (Zachariah et al., 2006; Forster et al., 2008).
It is a well-established fact that ART reduces mortality from HIV/AIDS related causes (HAPCO, 2010). For patients on ART, retention in care is needed to prevent medication interruptions, maintain immunologic benefits, prevent drug resistance, and monitor the effects of therapy (Ministry of Health, 2005, 2006). Despite the immense benefit of ART care to the patient and entire society, the magnitude and predictors of loss to follow-up of ART clients is not well documented in North Ethiopia, Tigray regional state. Thus this study was aimed to determine the magnitude and factors associated with loss to ART follow-up.
MATERIALS AND METHODS
Study area and setting
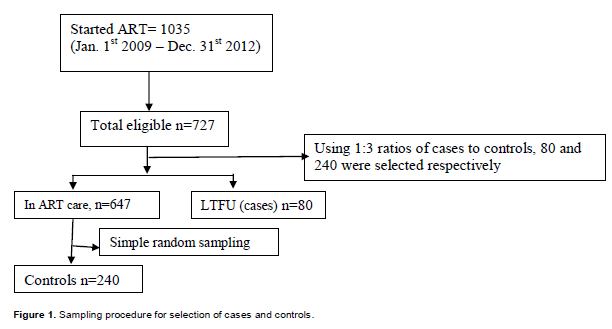
The study was conducted at Wukro primary public hospital. The hospital provides comprehensive HIV/AIDS care such as prevention services, curative and support services by a multi-disciplinary team which comprises a doctor, a nurse, a pharmacy technician, a data clerk, case manager and outreach workers. A case-control study design was employed using patients’ charts to collect data on LTFU among adult patients (>15 years old) enrolled for ART service from January 1st, 2009 to December 31st, 2012. Data extraction format was used to select subjects and an assumption of 1:3 cases to control ratio was applied to make a sample size of 320 using a random sampling technique (Figure 1).
The dependent variable was LTFU; ART clients from treatment to three or more months were considered as LTFU (Bekolo et al., 2013) and coded as “1” otherwise as “0”. The predictor variables include both socio-demographic and clinical factors. The tool was developed by reviewing literatures and from previously tested questionnaire modified in the context of the study.
Data analysis
Data were entered, coded, cleaned and analyzed using SPSS for windows version 16. Descriptive statistics of frequency and proportions were calculated for categorical variables and presented in the form of tables. Multivariable logistic regression model was used to identify the independent predictors of LTFU and 5% of alpha level was used to declare level of significance.
Ethical clearance was secured from the ethical committee of Mekelle University, College of Health Science. All data accessed were kept confidential and patient identifiers were excluded from the data base. Those who already knew the details of the patients and were responsible for their ART treatment were used in the data collection process. Hospital manager and ART team were communicated on how to restart ART for those LTFU.
RESULTS
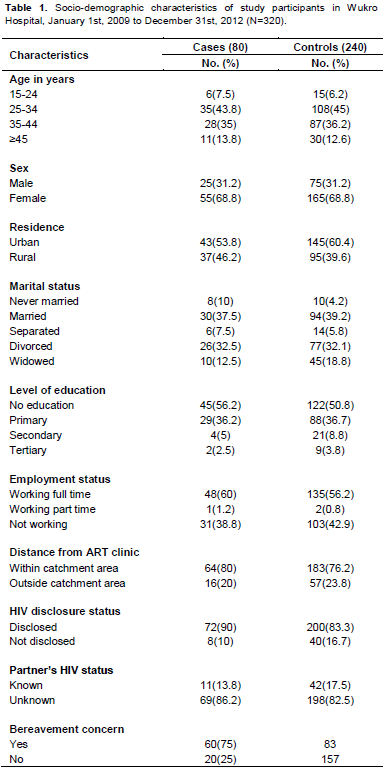
A total of 727 patients aged 15 years and above were on ART during the initiation of the study. Of those ever started, 80 (11%) were found to be LTFU (cases) with response rate of 100% and 240 were controls. Of the final study sample, (n = 320), majority (44.7%) were aged 25 to 34 years at the time of initiation of ART. The median age of patients was 34 years. Women contribute nearly 69% of the patients (Table 1)
Clinical characteristics
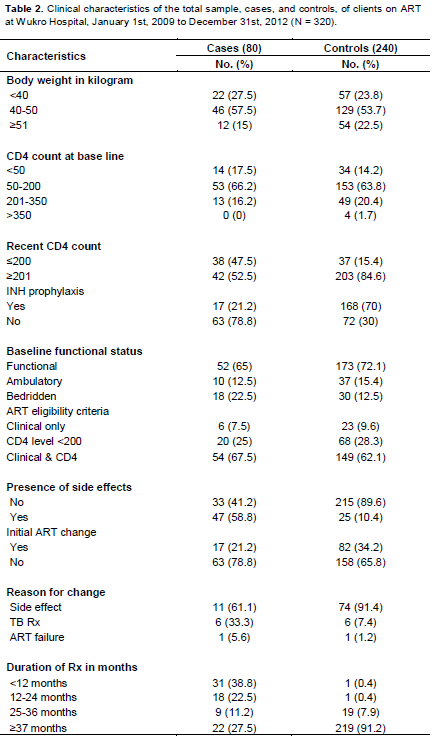
Concerning clinical factors, the mean baseline weight for study participants was 45.4 ± 7.5 kg. At the time of ART initiation; 76.2% of patients were in World Health Organization (WHO) stage III or IV which represent advanced stage of the disease. This was also evidenced by the fact that 79.4% had CD4 count less than 200 cells/ul at the time of initiation of ART (Table 2).
The proportion of lost to follow up in this study was 11 and 100% of the lost clients who were reached by the outreach workers and case managers by using telephones and making home visits. Among the LTFU clients, 44% were in the age group 15 to 34, nearly 69% were females, 46% were rural residents and 56% had no education (Table 1).
Factors associated with LTFU
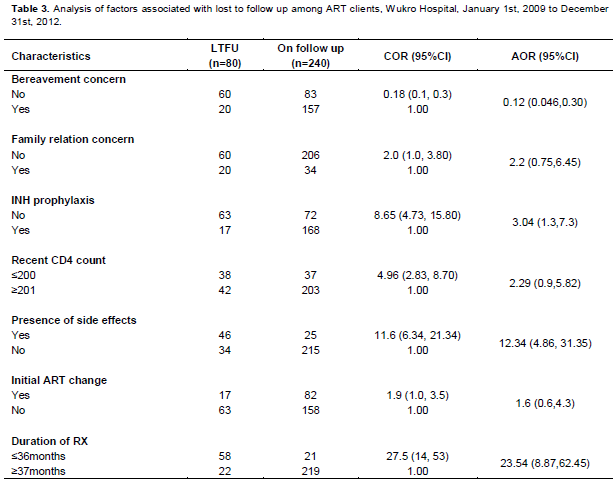
Socio demographic variables were analyzed but were not significant, except grief or bereavement concern and clinical factors such as INH prophylaxis, presence of side effect and duration of follow up were found significantly associated with loss to follow up to ART treatment in the final model. Those who did not feel grief at initiation of ART were less likely to LTFU compared to those who felt grief (AOR = 0.12; 95% CI: 0.046, 0.30). Moreover, those who did not take INH prophylaxis were three times more likely to LTFU (AOR = 3.04; 95% CI: 1.3, 7.3) (Table 3).
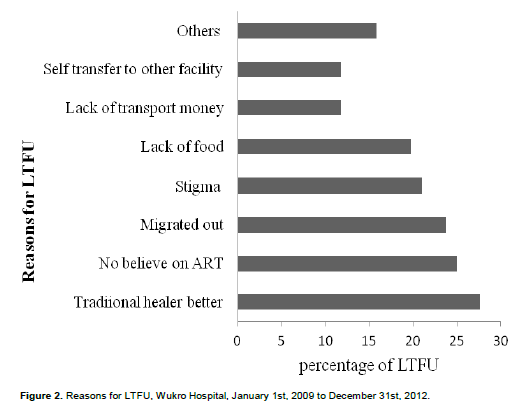
Reasons for LTFU among patients on ART
The tracing result revealed that 76 of them were found to be alive and four were dead. Of those found alive 40 (52.6%) of them restarted treatment in the hospital. The commonest cause (28%) of LTFU was preference of traditional healer (Figure 2).
DISCUSSION
This study intended to investigate the magnitude of LTFU and the associated factors among ART clients at Wukro Hospital. This study reported 80 (11%) LTFU. A similar finding was reported by a study conducted in Jimma University Hospital which was at 13.6% (Deribe et al., 2008). In this study, the proportion of lost to follow up in the first year was nearly 39% which is consistent with the range of 15 to 40% of LTFU among sub-Saharan Africa countries (Stringer et al., 2006). However, the overall reported prevalence in this study was lower than reported sub Saharan Africa countries. This difference might be brought by the inconsistency in time interval used to define the time for follow up time which is three months in our study, while other studies used two months in Zambia (Chi et al., 2010), and six months in West Africa (Ekouevi et al., 2010). The possible explanation for this relatively low rate of LTFU may be the advancement of care and interdisciplinary team work in delivering care and support service. On top of this, the food by prescription program might contribute patients to be retained in care. Besides, the study area is the place where more projects takes place and it is also a demographic surveillance study site of Mekelle University and the community is assumed to be more exposed to information regarding the advantage of adhering to ART.
Most of the study subjects (76.2%) had advanced stage of AIDS (stage III or IV) on initial presentation to the ART clinic and 79.4% had baseline CD4 cell < 200/μl. This is in line with the global progress on AIDS report (WHO/UNAIDS/UNICEF, 2009). Fear of stigma and discrimination or insufficient decentralization of ART clinics might hinder early presentation of patients to ART clinic. This was reported as a reason for LTFU by 21% of
study participants and fear of stigma and discrimination
was also reported if treated at nearer centers.
In this study, being bereaved at initiation of ART, taking INH prophylaxis, presence of side effect and duration of ART follow up were found to be independent predictors of LTFU. A wider confidence interval was observed which might be due to small sample size study. Accordingly, those who did not feel grief at the time of ART initiation were less likely to LTFU (AOR = 0.12; 95% CI: 0.046, 0.30). Grief may discourage patients on ART to adhere to their treatment because of the continuous emotional burden. A systematic review also revealed that depression was highly prevalent in individuals with HIV (Rabkin, 2008) and often accompanied by bereavement (Haight and Gibson, 2005). As a consequence, it may cause delays in initiation of anti-retroviral treatment and affects adherence to treatment and reduces important self-care behaviors (Horberg et al., 2008; Vranceanu et al., 2008) in individuals. Bias might be introduced; being bereavement was measured on self report of patients.
INH prophylaxis in our study was a strong predictor of lose to follow up, indicating that patients not on INH prophylaxis were three times more likely to be lost from ART follow up (AOR = 3.04; 95% CI:1.3,7.3). Initiation of
INH which is recommend by the National Treatment Guideline may have an indirect effect on patient retention since it decreases the occurrence of tuberculosis disease which is a common cause of morbidity and mortality for HIV patients on ART (Federal Ministry of Health, 2007). Existing interventions such as management of opportunistic infections could encourage patients to engage in care and could need greater effort to retain patients from the beginning of HIV care and after ART initiation.
Presence of ART drugs side effects was also one of the factors significantly associated with LTFU (AOR = 12.34: 95% CI: 4.86, 31.35) which is supported by a finding from South Africa (Ive et al., 2007). This implies the need for health professionals to identify and give special attention and closer follow-up for patients who have treatment side effects. Duration of ART treatment was also found to be a significant determinant of loss to follow up. Patients who had duration of follow-up three years and below had significantly more chance of getting lost from follow up (AOR = 23.54; 95% CI:8.87, 62.45). This is scientifically agreeable in that patients on ART get stabilized on the ART care as the duration of follow up gets longer (Sieleunou et al., 2009).
Understanding of the reasons for not returning to care is important to look at alternative strategies on ART programs. This study found that preference for traditional healers is commonest reason for LTFU. Similarly, other studies reported self-transfer to other facility, cost of care, access to ART, acceptance to ART as a reason for not returning to the health care (Hardon et al., 2007; Zachariah et al., 2006; Forster et al., 2008). In this regard, efforts to decentralization of services, task shifting to lay care providers, longer drug refill periods for stable patients, as well as provision of transport need to be addressed to tackle the problems.
CONCLUSION
The level of lost to follow up was 11%. Most of the clinical factors were found major predictors to LTFU. Though some socio-demographic factors were associated with LTFU in other studies, none was found significant in this study except being grieved. This relatively low rate of LTFU may imply the improvement of quality care and decentralization of services as well as the increasing community awareness. Since the clinical factors were found significant, care providers working in ART and counseling service should work on the risk factors to increase retention of ART patients.
ACKNOWLEDGEMENT
The authors would like to acknowledge Mekelle University, College of Health Sciences for facilitating the study. Also, we would like to thank the staffs of Wukro Hospital and data reviewers for their substantial contribution to the success of the research. Last but not least, we would like to appreciate colleagues who edited the manuscript.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
REFERENCES
|
Ammassari A, Antinori A, Cozzi-Lepri A, Trotta MP, Nasti G (2002). Relationship between HAART adherence and adipose tissue alterations. J. Acquir. Immune Defic. Syndr. 31:140-144. Crossref |
||||
|
Ammassari A, Murri R, Pezzotti P, Trotta MP, Ravasio L (2001). Self-reported symptoms and medication side effects influence adherence to highly active antiretroviral therapy in persons with HIV infection. J. Acquir. Immune Defic. Syndr. 28:445-449. Crossref |
||||
|
Bekolo CE, Webster Jayne, Batenganya M, Sume GE and Kollo B (2013). Trends in mortality and loss to follow-up in HIV care at the Nkongsamba Regional hospital, Cameroon. BMC Res. Notes 6:512. Crossref |
||||
|
Braitstein P, Brinkhof MWG, Dabis F, Schechter M, Boulle A (2006). Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. The Lancet 367:817-824. Crossref |
||||
|
Brinkhof MW, Dabis F, Myer L, Bangsberg DR, Boulle A, Nash D, Schechter M, Laurent C, Keiser O, May M, Sprinz E, Egger M, Anglaret X (2008). Early loss of HIV-infected patients on potent antiretroviral therapy programs in lower-income countries. Bull. World Health Organ. 86(7):559-67. Crossref |
||||
| Carole Leach-Lemens (2010). Loss to follow-up high in South African public sector ARV programs. International Epidemiologic Databases to Evaluate AIDS collaboration of South Africa. | ||||
|
Chi BH, Cantrell RA, Mwango A, Westfall AO, Mutale W (2010). An empirical approach to defining loss to follow-up among patients enrolled in antiretroviral treatment programs. Am. J. Epidemiol. 171(8):924-31. Crossref |
||||
|
Deribe K, Hailekiros F, Biadgilign S, Amberbir A, Beyene BK (2008). Defaulters from antiretroviral treatment in Jimma University Specialized Hospital, Southwest Ethiopia. Trop. Med. Int. Health 13:328-333. Crossref |
||||
|
Dixon S, McDonald S, Roberts J (2001). HIV/AIDS and development in Africa. J. Int. Dev. 13:381-389. Crossref |
||||
|
Ekouevi DK, Balestre E, Ba-Gomis FO, Eholie SP, Maiga M, Amani-Bosse C, Minga A, Messou E, Sow PS, Lewden C, Traoré HA, Bissagnene E, Dabis F (2010). Low retention of HIV-infected patients on antiretroviral therapy in 11 clinical centers in West Africa. Trop. Med. Int. Health 15(1):34-42. Crossref |
||||
| Federal Ministry of Health (FMH) (2007). Antiretroviral treatment program implementation guideline in Ethiopia. Available at: http://www.who.int/hiv/pub/guidelines/ethiopia.pdf | ||||
|
Forster M, Bailey C, Brinkhof MWG, Graber C, Boulle A, Spohr M, Balestre E, May M, Keiser O, Jahn A, Egger M (2008). Electronic medical record systems, data quality and loss to follow-up: survey of antiretroviral therapy programmes in resource-limited settings. Bull. World Health Org. 86:939-947. Crossref |
||||
| Haight B, Gibson F (2005). Group Psychotherapy. Burnside's working with older adults: Group process and technique. Chapter 18. 4th ed. Jones and Bartlett Publishers. Boston, Massachusetts. p. 234. | ||||
| HAPCO (2010). Monthly HIV Care and ART Update. Retrieved from www.Hapco.Gov.et | ||||
|
Hardon AP, Akurut D, Comoro C, Ekezie C, Irunde HF (2007). Hunger, waiting time and transport costs: time to confront challenges to ART adherence in Africa. AIDS Care 19:658-665. Crossref |
||||
|
Horberg MA, Silverberg MJ, Hurley LB, Towner WJ, Klein DB, Bersoff-Matcha S, Weinberg WG, Antoniskis D, Mogyoros M, Dodge WT, Dobrinich R, Quesenberry CP, Kovach DA (2008). Effects of depression and selective serotonin reuptake inhibitor use on adherence to highly active antiretroviral therapy and on clinical outcomes in HIV-infected patients. J. Acquir. Immune Defic. Syndr. 47(3):384-90. Crossref |
||||
| Ive P, Conradie F, Xaba S, Sanne I (2007). Causes of loss to follow up in patients taking antiretroviral therapy in the national rollout program of South Africa. The 3rd IAS Conference on HIV Pathogenesis and Treatment. Rio de Janeiro, Brazil. Available at: http://jid.oxfordjournals.org/content/suppl/2012/10/12/jis635.DC1/jis635supp.pdf | ||||
| Ministry of Health (2005, 2006). Annual HIV/AIDS monitoring and evaluation report: Addis Ababa, Ethiopia. | ||||
|
Rabkin JG (2008). HIV and depression: review and update. Curr. HIV/AIDS Rep. 5:163-71. Crossref |
||||
|
Rueda S, Park-Wyllie LY, Bayoumi AM, Tynan AM, Antoniou TA (2006). Patient support and education for promoting adherence to highly active antiretroviral therapy for HIV/AIDS. Cochrane Database Syst. Rev. 3:CD001442. Pubmed |
||||
|
Russell S, Seeley J, Ezati E, Wamai N, Were W, Bunnell R (2007). Coming back from the dead: living with HIV as a chronic condition in rural Africa. Health Policy Plan. 22(5):344-347. Crossref |
||||
|
Sieleunou I, Souleymanou M, Schonenberger AM, Menten J, Boelaert M (2009). Determinants of survival in AIDS patients on antiretroviral therapy in a rural centre in the Far-North Province, Cameroon. J. Trop. Med. Int. Health 14(1):36-43. Crossref |
||||
|
Stringer JS, Zulu I, Levy J, Stringer EM, Mwango A, Chi BH (2006). Rapid scale-up of antiretroviral therapy at primary care sites in Zambia: feasibility and early outcomes. JAMA. 296:782-93. Crossref |
||||
|
Vranceanu AM, Safren SA, Lu M, Coady WM, Skolnik PR, Rogers WH (2008). The relationship of post-traumatic stress disorder and depression to antiretroviral medication adherence in persons with HIV. AIDS Patient Care STDS. 22:313-21. Crossref |
||||
| WHO, UNAIDS, UNICEF (2011). Global HIV/AIDS Response: Epidemic update and health sector progress towards universal access: Progress Report 2011. Geneva. 2011. Available at: http://www.who.int/hiv/pub/progress_report2011/en/WHO/UNAIDS/UNICEF (2009). Towards universal access: scaling up priority HIV/AIDS interventions in the health sector; Progress report. | ||||
| World Health Organization (WHO) (2006). Antiretroviral drugs for treating pregnant women and preventing HIV infection in infants in resource-limited settings: towards universal access. | ||||
| World Health Organization (WHO) (2010). A Sustainable Health Sector Response to HIV. Global health sector strategy on HIV/AIDS for 2011-2015. | ||||
|
Wubshet M, Berhane Y, Worku A (2012). High Loss to follow up and Early Mortality Create Substantial Reduction in Patient Retention at Antiretroviral Treatment Program in North-West Ethiopia. ISRN AIDS Volume 2012. Pubmed |
||||
|
Zachariah R, Harries AD, Manzi M, Gomani P, Teck R (2006). Acceptance of anti-retroviral therapy among patients infected with HIV and tuberculosis in rural Malawi is low and associated with cost of transport. PLoS ONE 1:e121. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


