Full Length Research Paper

ABSTRACT
Nigeria has high burden of HIV/AIDS; antiretroviral therapy (ART) availability, a blessing to HIV patients. Unfortunately, most people do not know their HIV status. Association for Reproductive and Family Health (ARFH), Nigeria introduced mobile free HIV Counseling and Testing (HCT) services to complement its clinic services for HCT uptake. The characteristics of clients patronizing ARFH’s HCT services are assessed. A retrospective review of ARFH’s clinics’ data on HCT services between 2005 and 2011 was undertaken and demographic characteristics of HCT clients were abstracted from the HIV intake register. Descriptive statistics of data were obtained using SPSS version 20.0. Significance of association between socio-demographic characteristics and reasons for HCT uptake were investigated using Chi-square test. The mean age of 6,684 clients was 29.5±9.4 years and 76% were females while 20% positive to HIV. Two-thirds in monogamous marriage and 25% had university/polytechnic education while 41% were artisans and apprentices. Nearness of HCT to patient’s residence and referral from ANC were the major reasons for HCT uptake. Mobile HCT clinic enhanced HCT uptake especially in sexually active age-group. Availability of mobile HCT services will fast-track achieving the first 90 of the 90-90-90-PEPFAR target for the control of HIV/AIDS. Proportion positive to HIV is high.
Key words: HIV counseling and testing (HCT), Nigeria, HIV/AIDS, demographic characteristics, mobile, stand-alone.
INTRODUCTION
The estimate of the 2013 burden of HIV and AIDS showed 3.2 million people consisting of 2.8 million adults aged 15 years and above and 400,000 children aged between 0 and 14 years live with the disease in Nigeria. The adult population of 15 to 49 years has a prevalence rate of about 3.2% and its high mortality had led to an estimated 2 million orphans (National HIV/AIDS Epidemiology and Impact Analysis (NHEIA) Report 2014). HIV Counselling and Testing (HCT) has been reported to be a major intervention strategy that can help to reduce the transmission of HIV (Isara et al, 2009) (Boswell and Baggaley, 2005). Indeed research findings have shown that people who are aware of their HIV-status are more likely to practice safer sex (Marks et al., 2005) and empower the uninfected person to change any risky behaviors associated with HIV. This must informed PEPRAR, who has been in the forefront in the control of HIV/AIDS in Nigeria to set a target for 90% of people to know their HIV status by the year 2020, and 90% of those found positive to be linked to treatment while 90% of those on treatment should have their viral load suppressed. This is coined as PEPFAR’s 90-90-90 principle. In fact, recent information has increased this to 95-95-95.
Unfortunately, a high proportion of the Nigerian population does not know their HIV status and so unable to take advantage of the ART services available in the country. In spite of the clear benefits of HCT, findings show its uptake is low among Nigerians, and there is poor reporting of the characteristics of people accessing it (Adewole and Lawoyin, 2004; NBS and UNICEF, 2017). Folaranmi et al., 2008). The Association for Reproductive and Family Health (ARFH), an indigenous NGO in Ibadan Nigeria with financial support from AIDS Prevention Initiative in Nigeria (APIN) implemented a special program through the provision of free HCT services in private health clinics, market places, and educational institutions with full documentation on reasons for its uptake as part of the innovative strategies to get people to know their HIV status. Descriptive epidemiology of any disease is better understood with a good knowledge of the person who is affected, the place and the time. Therefore, it is imperative to know the demographic characteristics of persons patronizing the HCT clinic. The present study examined the socio-demographic characteristics of clients who accessed the HCT services and their associations with reported reasons for HCT uptake.
METHODOLOGY
This is a retrospective study of clients accessing HIV counseling and testing services at the Association for Reproductive and Family Health stand-alone and mobile HCT clinics between September 2011 and December 2016 in Ibadan. Ibadan is the capital of Oyo State in Nigeria with a population of more than 4 million people. Ethical approval for this study was obtained from the ARFH Ethics Committee of its Board of Scientific Research.
HCT at ARFH friendly health clinic
The Association for Family and Reproductive Health provides HCT services at its friendly health clinic located at its main office at Ikolaba in Ibadan. There is an awareness advocacy to the general population in Ibadan on the availability of these specific services and people are free to access it daily from 8 am to 5 pm.
HCT mobile clinic
The HCT mobile services targeted general population of men and women at the market places, churches and mosques, students at higher education of learning, out of school youth and artisans. Aside this general population, free HCT services were also carried out during community outreach activities conducted among uniformed service personnel, female sex workers, road transport workers, footballers, men having sex with men, intravenous drug users, hairdresser association, barbers, tailors, patent medicine vendors and people that visited ARFH health clinic for various ailments.
Data management
ARFH has maintained a data base since the commencement of its activities by collecting information on all clients who consented to participate in the program. The information collected from each consenting client was as contained in the national intake forms for Orphans and Vulnerable Children (OVC) programming. The information was contained in a register maintained at each of the ATFH clinic. For this study, data of clients attending the clinics in the last 6 years (2011-2016) was abstracted using a data collection form that contained information on their socio-demographic characteristics and reasons for clients’ accessing HCT services and other relevant variables from the clients’ register.
The data was analyzed using SPSS version 20 and presented in frequency distribution tables and appropriate summary statistics. The Chi-square test was used to determine the significance of the association between clients’ socio demographic characteristics and reasons for HCT uptake at the 5% probability level.
RESULTS
Socio-demographic profile of clients
Table 1 shows the socio demographic characteristics of the 6,684 clients who accessed the HCT services within the six years study period. There were 1,385 cases (342 males and 1043 females) positive to HIV during this period giving an overall proportion of about 21% higher in males (21.5%) than females (20.5%)
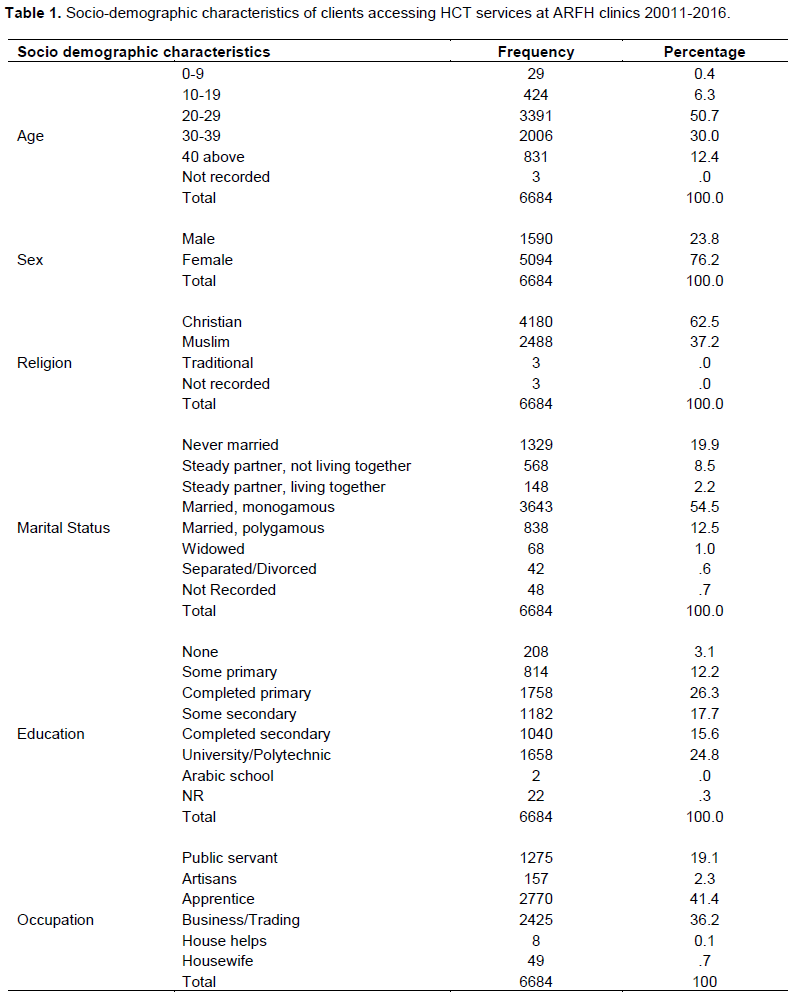
The mean age of all the clients was 29.5 (SD=9.4) years. About 90% were aged between 20 and 40 years while 50% were in the age bracket 20 to 29 years. The sex distribution was in favor of females (76%) and a preponderance of Christians as only about a third of the clients were Muslims. The marital status of the clients shown in panel 4 of Table 1, indicated about two-thirds were married out of whom 81% were in monogamous marriage. About 20% of them were never married while less than 2% were either widowed or divorced or separated.
About one-quarter (24%) had a university/polytechnic education while less than one-fifth (16%) completed secondary education, 26% completed primary school education and only 3% had no formal education. The majority of the clients were artisans and apprentices (41%), followed by traders (36%) while public servants constituted 19% of the clients.
Reasons for the uptake of HCT services
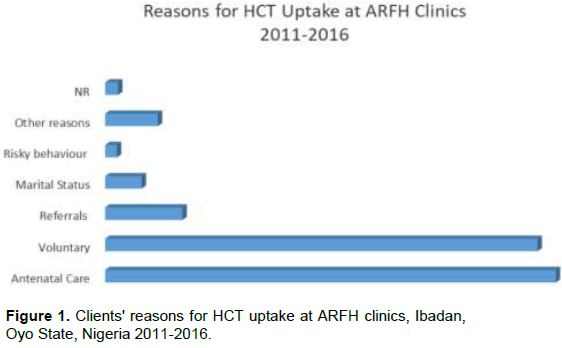
Figure 1 shows antenatall care (42%) and voluntariness (40%) are the major reasons participants came for the HCT services. However, about 16% mentioned other reasons such as: it was part of their marriage requirements, decision when feeling unwell, perceived risky practices, death of partner, pre-requisite to getting a job. Only 1% of the clients did not disclose their reasons for accessing HCT services
Clients' accessibility to HCT clinics
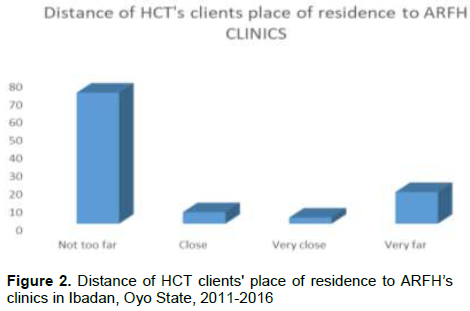
Figure 2 shows that a large proportion of clients (82%) indicated their place of residence was not far to the HCT clinics. A further analysis showed that clients not too far from HCT centers are twice more likely to access HCT than those who lived far away.
Association of clients’ reasons for uptake of HCT and their demographic characteristics
The result of the analysis of the association of reasons for the uptake of HCT and clients’ socio-demographic variables are shown in Table 2. There was a statistically significant association between each of the socio-demographic variables examined and the reasons for accessing HCT services (P<0.0001). Almost two-thirds of clients 40 years and above and 56% of those less than 20 years accessed the services voluntarily compared to 35% of clients in the middle age 20 to 39 years. Whereas about 48% of clients in this latter age group came for HCT services for antenatal care reasons compared to 11% of those above 40 years. Also, the highest proportion who accessed HCT for reasons of risky behaviors were among clients under 20 years of age (3%) and decreased with increase in age with the least (0.4%) among those 40 years and above. The proportion referred for HCT also decreased with age from 9% among clients less than 20 years to 7% of those 40 years and above.
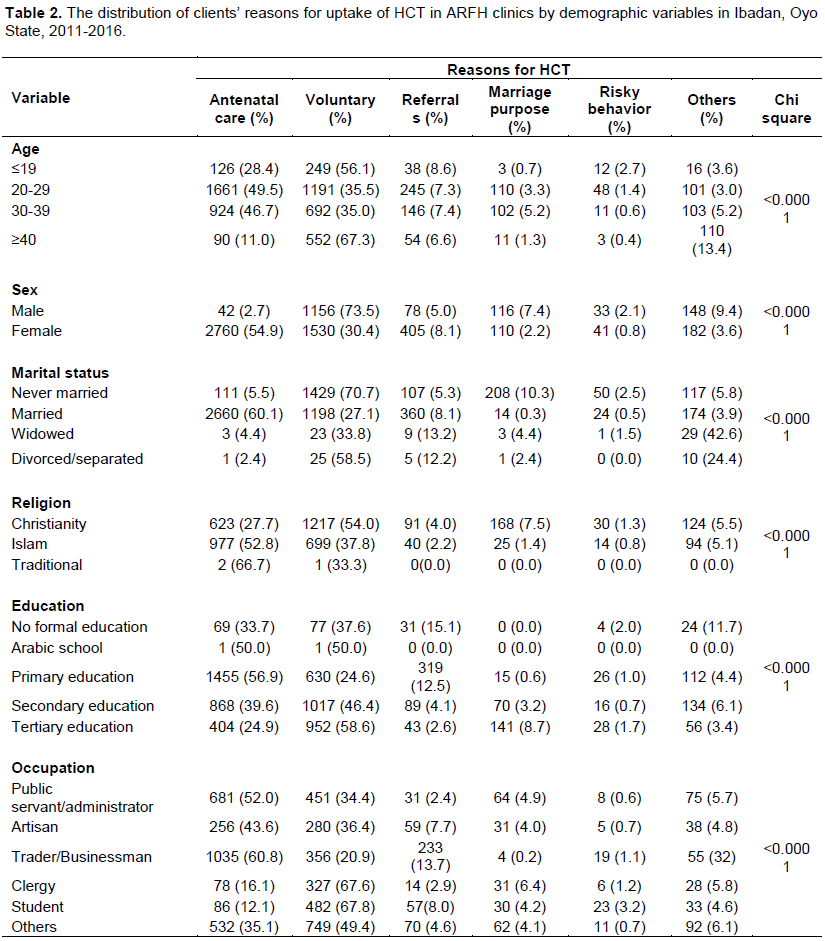
The sex differential showed 73% of males accessed HCT voluntarily compared to only 30% of females whose majority came because of antenatal services. The females had higher proportion of referrals than males.
The majority of married clients accessed HCT for antenatal reasons (60%) while it was mainly voluntary among those who never married (71%) and those widowed accessed HCT services either because of other reasons (43%) or voluntarily (34%). The majority of those divorced or separated accessed HCT voluntarily (59%)
The association of reasons for uptake of HCT services and religion was also statistically significant (P<0.05). A higher proportion of Christians did so voluntarily (54%) compared to less than 40% of Muslims. The proportion of clients who accessed HCT services for marriage purposes was generally low but higher among Christians (8%) than Muslims (1.4%)
Panel 5 of Table 2 also showed that clients with tertiary education had the highest proportion (59%) accessing HCT services voluntarily while clients with only primary education had the highest percentage who came for HCT services for reason of antenatal care (57.0%). On the other hand, clients with no formal education (15%) had the highest proportion who were referred. Also, those with tertiary education had the highest proportion who accessed HCT for marriage purposes (9%) and decreased with decrease in level of education as there was none among those with Arabic or no formal education.
DISCUSSION
The present study utilized a secondary data, a type of data often derided for incompleteness and inaccuracies. But the ARFH clinic database, generated from its stand-alone and mobile HCT clinics has benefited immensely from modern computer technology and dedicated staff who ensured all records are entered on daily basis which is followed by regular data quality assessment by a supervisor. Therefore, this routinely collected data, although from a non-probability sample of the general population can be a reliable source of data that can inform HCT uptake. In fact it is comparable with other studies on HCT uptake that used primary data but limited to specific segments of the population such as school adolescents, corps members and pregnant women (Asante, 2013; Paz-Soldan et al., 2005).
A very high proportion of HCT clients in this study reported that their places of residence were not too far to the HCT clinics. Distance between respondents’ place of residence and the clinic could therefore be a proximate determinant for accessing HCT services. And so, the introduction of the free mobile HCT service, which was brought to the vicinities of institutions, must have been responsible for the large number of clients reported in this study. And therefore, it is not a surprise that as large as 82% indicated nearness to the HCT centre as reasons for their uptake. This is similar to another study conducted in sub Saharan Africa which reported that the roll-out of various HIV testing initiatives such as opt-out providers initiated HIV testing and mobile HIV testing improved uptake of HIV testing by being available at their doorsteps (Ogbo et al., 2017). Although, there was no disaggregation of the data by stand alone and mobile HCT yet anecdotal information confirmed a phenomenal increase in the number of clients accessing HCT at the stand alone centers which was less than 200 annually prior to 2005 when the free HCT service was introduced. This finding of nearness to HCT facilities also informs policy makers to incorporate HCT services in Primary Health Care Centers which is the nearest health service provider to the community in Nigeria.
This study also revealed that more than 90% of HCT clients were between 20 and 40 years of age which is consistent with previous studies (Ibrahim et al., 2013). The major explanations have been that risky sexual behaviors and contraction of marriages are common in this age group. This is also the most sexually active age group in Nigeria and they contribute immensely to the workforce. Also, this study found about half of those who had HCT was in the age group 20 to 29 years also corroborated other studies that reported young people 15 to 24 years old accounted for over 40% of all new HIV infections among adults (Matseke et al., 2016). A Nigeria study had reported this is the age group at most risk of HIV infections and this may be due to a multiplicity of factors such as early sexual experimentation, multiple sexual partnerships, and inconsistent use of condoms (Patrick et al., 2012). The low frequency of uptake by people over 40 years could mean that at this age most families have greater responsibilities building their families in terms of children education, providing adequate shelter and transportation with little time for irresponsible sexual behavior that could increase their risk of HIV/AIDS.
Also, the preponderance of females found in this study is not surprising as previous studies have shown that females often seek medical help than males (Oliver et al., 2005). In this study, the fact that the majority of the females accessed HCT for ANC may also explain the preponderance of females and this could be in response to the policy that women attending ante natal clinics must also receive HCT services (Ibrahim et al., 2013). So the availability of HCT at ANC clinic was a great opportunity for up taking HCT services for such women. Our finding is also consistent with an earlier study which reported females accounted for a high proportion of those who had HCT (Cockcroft et al., 2007). The study implicated the perceived higher risk of HIV infection among females as a probable reason for a higher proportion of women taking up HCT than their male counterparts (Magadi, 2011).
This study also revealed that a higher proportion of Christians visited the HCT clinics voluntarily compared to Muslims, the two major religions in Nigeria. This is also consistent with previous studies who reported more Christians accessed HCT for marriage purposes as observed in this study as well (Amu et al., 2013). The major reasons Christians access HCT is for marriage purposes, a requirement by most churches prior to conducting marriages and this is consistent with the study conducted by (Amu et al., 2013).
This study also revealed that majority of clients attained at least a primary school level education and this corroborates a previous study which reported educational level was associated with decision for a young male or female who feels at risk took the bold step to know his/her HIV status (Amu et al., 2013). In fact it is a well known dictum that education buys awareness.
The present study has shown an alarming proportion (about a fifth) of clients was positive to HIV. This is similar to 22.9% who were reported among the MSM and 19.4% among female sex workers, the most at risk population in Nigeria (Federal Ministry of Health, 2014). It is embarrassing that despite increasing efforts made by the government to control the HIV epidemic, the current rate from this haphazard sample of the general population in Ibadan, suggested there is need for more than behavioral strategy to reduce HIV in Nigeria.
CONCLUSION AND RECOMMENDATION
This study has shown that the mobile HCT initiative by ARFH could facilitate the uptake of HCT and achieve the first 95 of the 95-95-95 UNAIDS ambition.
Socio demographic characteristics of HCT clients were found to be associated with the reasons (ANC, Voluntary, Referral, risky practices, job purpose, and partner died) for accessing HCT. The most pronounced reasons were antenatal care and personal decision. Also, education, sex, marital status, religion and age were the most influential demographic variables with the reasons for the uptake of HCT. Accessibility of clients’ to HCT centers was also a good determinant of HCT uptake. Although this sample may suffer from self-selection, the high proportion of positives to HIV detected is an indication that the HIV epidemic is yet to be controlled as the clients were from the general population.
It is recommended that HCT program be incorporated into other health services clinics to give individuals irrespective of their sex, marital status and age the opportunity to be tested for HIV so as to encourage early detection and treatment in order to reduce re-infection.
REFERENCES
|
Adewole DA, Lawoyin TO (2004). Characteristics of volunteers and non-volunteers for voluntary counseling and HIV testing among unmarried male undergraduates. African Journal of Medicine and Medical Sciences 33(2):165-170. |
|
|
Amu EO, Ijadunola KT, Bamidele JO, Odu OO (2013). Barriers to and determinants of HIV counselling and testing among adults in Ayedaade Local Government Area, Osun State, Nigeria. Journal of Medical Sciences 13(8):803-808. |
|
|
Asante KO (2013). HIV/AIDS knowledge and uptake of HIV counselling and testing among undergraduate private university students in Accra, Ghana. Reproductive Health 10(1):17. |
|
|
Boswell D, Baggaley R (2005). Voluntary counselling and testing and young people: a summary overview, VCT Toolkit, (Family Health International, 2002. |
|
|
Cockcroft A, Andersson N, Milne D, Mokoena T, Masisi M (2007). Community views about routine HIV testing and antiretroviral treatment in Botswana: signs of progress from a cross sectional study. BMC International Health and Human Rights 7(1):5. |
|
|
Magadi MA (2011). Understanding the gender disparity in HIV infection across countries in sub-Saharan Africa: evidence from the Demographic and Health Surveys. Sociol Health Illness 33(4):522-39. Federal Ministry of Health (2014). Integrated Biological and Behavioural Surveillance Survey. |
|
|
Ibrahim M, Ipadeola O, Adebayo S, Fatusi A (2013). Socio-demographic determinants of HIV counseling and testing uptake among young people in Nigeria. International Journal of Prevention and Treatment 2(3):23-31. |
|
|
Isara AR, Bello OB, Okojie OH, Omofonwan I, Omoniyi I, Omorayi M. (2009) Knowledge, Attitude and Practice of Voluntary Counselling and Testing for HIV/AIDS among students in the University of Benin, Benin City, Nigeria. Journal of Community Medicine and Primary Health Care 21:27-34. |
|
|
Marks G, Crepaz N, Senterfitt JW, Janssen RS (2005). Meta-analysis of high-risk sexual behavior in persons aware and unaware they are infected with HIV in the United States: implications for HIV prevention programs. JAIDS Journal of Acquired Immune Deficiency Syndromes 39(4):446-453. |
|
|
Matseke G, Peltzer K, Mohlabane N (2016). Clients' perceptions and satisfaction with HIV counselling and testing: A cross-sectional study in 56 HCT sites in South Africa. African Journal of Primary Health Care and Family Medicine 8(1):1-7. |
|
|
National Agency for the Cotrol of AIDS (NACA) (2014). National HIV/AIDS Epidemiology and Impact Analysis (NHEIA) Report Nigeria. |
|
|
Ogbo FA, Mogaji A, Ogeleka P, Agho KE, Idoko J, Tule TZ, Page A (2017). Assessment of provider-initiated HIV screening in Nigeria with sub-Saharan African comparison. BMC Health Services Research 17(1):188. |
|
|
Oliver MI, Pearson N, Coe N, Gunnell D (2005). Help-seeking behaviour in men and women with common mental health problems: cross-sectional study. The British Journal of Psychiatry 186(4):297-301. |
|
|
Patrick ME, O'Malley PM, Johnston LD, Terry-McElrath YM, Schulenberg JE (2012). HIV/AIDS risk behaviors and substance use by young adults in the United States. Prevention Science 13(5):532-538. |
|
|
Paz-Soldan V, Kasote A, Tsui A (2005). HIV voluntary counseling and testing service preferences in a rural Malawi population. AIDS and Behavior 9(4):475-484. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


