Full Length Research Paper

ABSTRACT
Despite advancements in treatment and prevention, HIV and other sexually transmitted infections (STI) remain global public health issues. Nearly 40 years on, Thai business establishments are still facing adverse effects of the HIV epidemic. This study assessed HIV knowledge, transmission risk, stigma, and health behavior among a sample of 1,000 workers from the 2019 round of the Bangkok Behavioral Surveillance Survey (BBSS). Results indicate that most workers could identify common routes of HIV transmission but expressed stigmatizing attitudes. Overall, 13.1 and 19.3% had been tested for HIV and STI, respectively, 30.9% binge drank, 14.6% smoked cigarettes in the past month, and 21.6% used condoms consistently. Age, sex, marital status, education, economic status, peers, and level of stress were associated with HIV knowledge and health behavior. Based on the findings, tailored health educational interventions are needed to improve knowledge of HIV/STI, prevent STI, and promote sexual health-seeking behaviors including increasing uptake of HIV counselling and testing (HCT) in the workplace.
Key words: HIV knowledge, HIV testing, sexual behavior, stigma, STI screening, substance use.
INTRODUCTION
The global HIV/AIDS epidemic continues to affect societies around the world. Despite ongoing prevention interventions, HIV/AIDS remains the leading cause of death in low- and middle-income countries. In the workplace, despite the fact that there are effective treatments, HIV reduced productivity, increased staff turnover, increased production costs, and sustained negative prejudice about HIV/AIDS (Chen et al., 2020). Stigma is one of the main reasons for the persistent spread of HIV around the world since fear of being a person living with HIV/AIDS (PLHIV) deters many who suspect they might be infected from seeking diagnosis and treatment (Arimoto et al., 2013). The workplace is one environment where both the owners and co-workers discriminate against PLHIV, and there is less support for “AIDS in the Workplace” programs than existed in past decades (Weihs and Meyer-Weitz, 2016; Hong and Thepthien, 2017).
Vulnerability to HIV and other sexually transmitted infections (STI) of workers in the urban workforce is still a problem. Business establishment workers are often young people who live far from their families, and several studies have documented high-risk behaviors for STI/HIV in this population. A case study in Bangladesh found that major causes of HIV vulnerability of female garment workers are gender inequality, multiple sex partners, drug abuse, and rape violence (Mahmood, 2021). A survey conducted in the Namibian truck transport sector in six companies of different sizes found that risky sexual behavior was quite prevalent, and included having multiple concurrent partners and trading sex for incentives. That study found that drivers and laborers were especially prone to such risk behaviors (Kiderlen et al., 2015). In addition, a study of industrial workers compared migrant workers with local workers, and the prevalence of condom use was very low in both groups, but especially among the migrants. Studies indicate that factory workers' vulnerability to HIV infection is related to distance from family (Kumar et al., 2009). In Thailand, rural to urban migration is an important form of population movement for economic advancement. The migrants aspire to better education in the city, more job opportunities, higher pay, better health services, amenities, and many other perceived benefits of city living (Hong and Thepthien, 2017; Zhang et al., 2020).
Data for 2019 show that there were approximately 38 million PLHIV worldwide. Of these, about 13% did not know their HIV+ status, and about 28% were not yet on anti-retroviral therapy (ART) (Joint United Nations Program on HIV and AIDS [UNAIDS], 2020). The World Health Organization (WHO) estimates that more than 376 million people around the world have at least one of the four most curable STI: chlamydia, gonorrhea, syphilis, and trichomoniasis. Some of these STI can result in serious sexual and reproductive health problems such as infertility, miscarriage, infant death, and mother-to-child transmission of STI. Having an STI significantly increases risk of contracting and transmitting HIV (World Health Organization [WHO], 2018). Thailand has one of the highest rates of HIV prevalence in Asia and the Pacific, accounting for 9% of the total PLHIV caseload in the region. Of the nearly 70 million Thai population, approximately 470,000 are HIV+ while, in 2019, 14,000 PLHIV died from AIDS. Thailand is home to the largest number of PLHIV in the region. In 2020, it was estimated that 5,400 Thais were infected with HIV through unprotected sex, or 90% of all new infections in that year. Sharing needles to inject drugs was distant second route of transmission (UNAIDS, 2020). The prevalence of HIV in Thailand is declining due to successful prevention programs, and studies estimate that nearly 10 million people in Thailand avoided HIV transmission due to primary prevention, while AIDS deaths were reduced (between 2010 and 2018) by one-third (32%), and new HIV infections were reduced by nearly 60%. Nevertheless, incidence of STI (excluding HIV) increased from 18.8 in 2014 to 33.8 per 100,000 population in 2020 (WHO, 2018).
At the time of this study, an estimated 5.2 million Thais were working in Bangkok-based worksites, and this total comprises slightly more males (2.7 million) than females (2.5 million). Still, there is scant data on the prevalence of HIV and STI this worker population. In fact, it can be assumed that people in wage-labor jobs in Bangkok – especially those whose family home is in the provinces – have elevated risk for STI/HIV (Hong and Thepthien, 2017). Studies in the literature have estimated that 8.5% of factory workers in Zimbabwe were HIV+, (McFarland et al., 1999) and as high as 42.7% of textile factory workers in Lesotho were HIV+ (Mabathoana et al., 2019). Migrant workers in new settings are confronted by new customs, languages, and encounters with strangers that were never possible in their home communities. While they may suddenly have a newfound freedom (since their parents/relatives are not looking over their shoulder), the young migrant may also experience considerable fear and anxiety by being in a strange place and not knowing whom to trust. Often, the desire to be accepted by the new peer group leads to risk behavior that would not have been possible back home. The younger female migrant workers are particularly prone to entering into a sexual relationship with a co-worker. Male migrant workers might find it difficult to resist peer pressure to go out drinking and visiting commercial sex establishments. (Nguyen et al., 2012) Thus, being a young, lower-educated migrant worker in the city can be a “perfect storm” for heightened risk of STI and HIV (Nguyen et al., 2012). Often, the worksites for migrant wage laborers are located in suburbs of large cities and, thus, are remote from health centers and clinics. Plus, the need to work seven days a week and take overtime (OT) jobs means that most workers do not have enough free time to visit a clinic or health center to get treatment or prevention supplies (Nguyen et al., 2021; Tran et al., 2019). Baseline knowledge of STI and prevention is also likely to be low and based on word-of-mouth from peers. Thus, countries need to have a policy and programs for health education and services for migrant workers to prevent and treat STI and HIV, as well as other infectious diseases as they emerge (Mullany et al., 2003).
At the height of the HIV epidemic in Thailand, the Ministry of Labor (MOL) collaborated with the Thailand Business Coalition on AIDS (TBCA) to expand HIV education to the lower-income labor force in business establishment and other confined worksites in urban areas around the country. The aim was to motivate the private sector (that is, the worksite owners) to play a bigger role in prevention of STI/HIV for the workforce – to benefit their own labor force as well as the health of society. TBCA developed a handbook and set of standards for AIDS prevention and education (ASO). The TBCA outreach education program received funding from the Global Fund against AIDS, TB and Malaria (GF) and the MOL. In 2008, TBCA had contacted more than 11,000 businesses with a combined total labor force of three million, and invited them to participate in the worker education program. Initial outputs of the program were an increase in workplace policy on HIV prevention, and improved attitudes toward worker education about HIV/AIDS (Chamratrithirong et al., 2017). However, the program was not able to document changes in prevention behavior practices, such as use of condoms in risk situations. It can be assumed, however, that the baseline level of condom use with lovers or acquaintances were quite low in the population of lower-income wage laborers (Sakboonyarat et al., 2021). A foundation for initiating and sustaining prevention behavior for HIV/STI is sound knowledge about routes of transmission and effective methods of prevention. However, the baseline levels of prevention knowledge can differ widely, even in the same subgroups of the population depending on various socio-demographic characteristics (e.g., age, education, marital status, stress level, economic status, etc.) (Cabezas et al., 2013; Yi et al., 2018; Dehghani et al., 2021). Thus, the main objective of this research was to assess the level of knowledge of risk for HIV, stigma, and health behavior of a sample of young wage laborers in worksites of Bangkok.
MATERIALS AND METHODS
Study design and sample
Data were collected from 12 worksites in/around Bangkok during October to December 2019. The survey was part of the HIV/STI Behavioral Surveillance Survey (BSS) that is conducted bi-annually among a cross-sectional sample of ten sentinel groups of the population. This study looked specifically at health status, health behavior, access to health services, knowledge, and concern about health and illness among the sample. The National Statistical Office (NSO) of Thailand reported that, in 2019, there were 5,286,570 laborers in Bangkok. For this study, inclusion criteria were as follows: (1) Age 18 years or older; (2) Thai citizen; (3) Had worked at least six months in the current job; and (4) Could communicate well enough to participate in the survey. All participants signed an informed consent form before filling out the self-administered questionnaire. The protocol for the study was approved by the Ethical Review Committee of Mahidol University (Social Sciences) (MUSSIRB 2019/056 B1).
For this study, the authors used a formula for estimating the adequate sample size using the following parameters: (1) The expected proportion of factory worker with more accurate knowledge of AIDS and STI than the mean = 35.8% (according to a study on the relative importance of AIDS and STI) (Hong and Thepthien, 2017); (2) Knowledge about AIDS and STI in a former establishment in Thailand) Level = 95% absolute precision required = 0.1; and (3) Accuracy required for estimation of 84 employees per worksite, or 1,008 workers in 12, randomly-selected business establishment of 500 workers or more (e.g., factory, assembly plant, retail store, warehouse, etc.). The authors added 5% to the quota sample for each worksite to account for incomplete survey response. At each worksite, the participants were selected using simple random sampling. The selected workers were then invited to a meeting organized by the researchers. All workers were informed of the study objectives, and asked to give their written consent to participate in the study. Participants then filled out a self-administered questionnaire. After checking for completeness, 1,000 questionnaires were suitable for use in the analysis (completion rate 95.6%).
Instrument
The questionnaire is a structured set of close-ended questions which ask about socio-economic characteristics, demographic information, migration status, work history, having close friendships, level of stress, knowledge of HIV/STI, stigma, sex behavior, consumption of alcohol and cigarettes, and history of screening for HIV/STI.
Knowledge about HIV and STI, and stigma
Participants’ knowledge was measured by summing the number of correct response to 11 true/false statements about HIV prevention and transmission (The Joint United Nations Programmed on HIV and AIDS, 2020). These 11 items include knowledge of how HIV can be transmitted (e.g., sharing meals with a PLHIV, mosquito bites, sharing needles, and sexual intercourse), HIV prevention methods (e.g., use of condoms, having one faithful sex partner), and misconceptions about the risk of sex with a healthy-looking person. The possible knowledge score of HIV transmission ranges from 0 to 11 (that is, 1 point for each correct response). Cronbach’s alpha was 0.82 for this scale. HIV-related stigma was measured using a scale adapted from previous studies (Thepthien and Srivanichakorn, 2016). The scale is comprised of three items with two response options: “yes” = 1 and “no” = 0. Total possible scores range from 0 to 3, where a higher score indicates greater perceived HIV-related stigma. Cronbach’s alpha was 0.87 for this scale.
Health conditions and risk behaviors
In this study, participants were asked whether they had sex in the past 12 months, the number of sexual partners, and the use of condoms with their regular partners. The authors also examined the relationship between gender, self-reported health problems, and health risk behaviors. These behaviors have been found to be associated with an increased risk of HIV and STI among lower-income workers and other vulnerable populations. Respondents were asked about alcohol use in the past year, quantity of consumption of alcohol at one sitting, and alcohol consumption in the past month. Respondents were asked about access to condoms, participation in HIV/STI knowledge training, and history of screening for HIV/STI the past year.
Statistical analysis
Data collected were checked manually for completeness and consistency, and then cleaned, categorized, coded, and entered into EPI info version 7. For statistical analysis, data were transferred to SPSS version 24. During the analysis, odds ratios (OR) with 95% CI were calculated to determine the association of selected variables with the outcome variable. Descriptive, bivariate, and multivariate logistic regression analyses were implemented to determine the association between sociodemographic characteristics and health behavior, HIV knowledge, and stigma, adjusting for effects of other relevant variables, regardless of their magnitude of association in the descriptive analysis. A p-value of less than 0.05 was considered to be statistically significant.
RESULTS
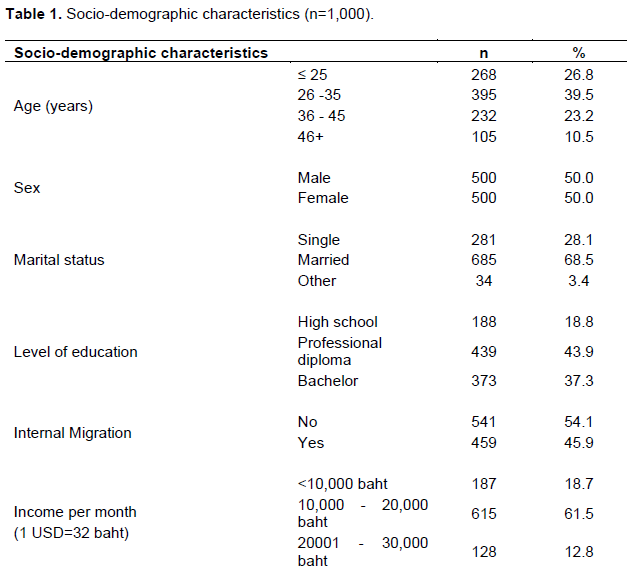
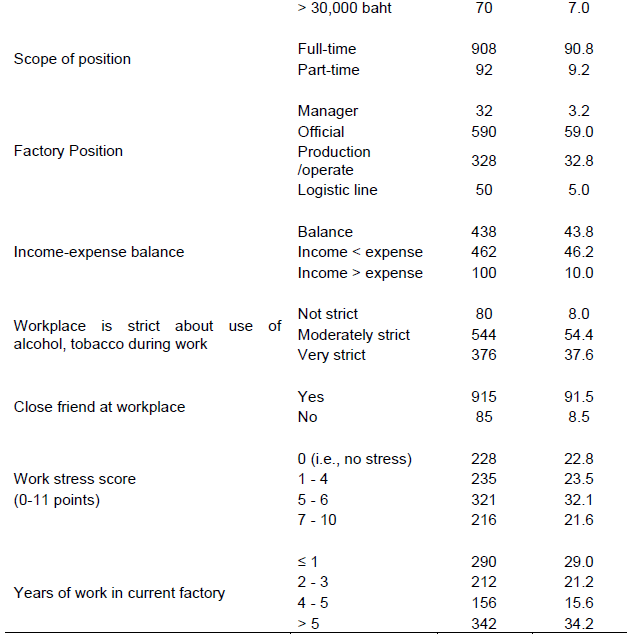
This sample of urban workers had roughly equal proportions of men and women. One in four was age 25 years or less; two-thirds (68.5%) were married; under half (45.9%) were not born in Bangkok; two-thirds had monthly income of 10,000-20,000 baht (1 USD=32 baht); 90.8% were contracted workers; while one in three had worked in the present worksite for more than five years. About half were feeling stressed about work at the time of this survey (late 2019), but most had close friends to rely on (Table 1).
About 73% of males and 63% of females had had sex in the past year (Table 2). Over one in six (15.8%) had multiple sex partners, but male workers were four times as likely to have had that experience in the past year compared to their female counterparts. It was found that only about one in five respondents used condoms for every episode of sex with a regular partner, and that was true for both male and female respondents. Over half the sample (53.5%) had consumed alcohol in the past year, and history of binge drinking was significantly more prevalent for male workers compared to female workers (p-value = 0. 01). Smoking behavior was low overall, but males still had significantly more consumption of tobacco products than females (p-value < 0. 001). Over half the sample (55.3%) had participated in some form of structured education on HIV prevention, and this proportion was roughly equal by gender. One-fourth had ever been tested for HIV, and half that total had been tested in the past year. About one in five had been screened for STI in the past year, and that was similar for males and females.
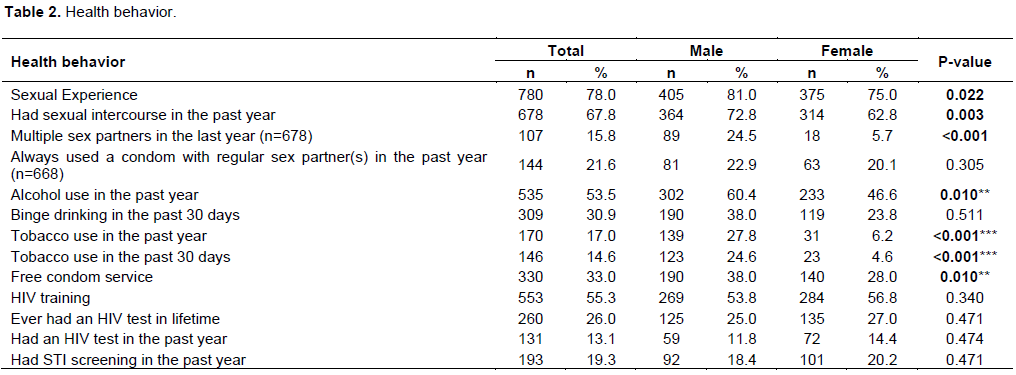
Table 3 presents results for measures of HIV knowledge. Overall, we observed a reasonably high level of knowledge across the 11 items (Mean=9.2, SD=1.54). Nearly all the workers (91.9%) knew that having a mutually-faithful sexual relationship with an HIV-negative partner was a good way to prevent HIV transmission. Similarly, 94.9% knew that using condoms reduces risk of HIV. More than three-fourths (77.0%) knew that a person who looks healthy can also be a PLHIV. Fully 84.2% knew that HIV cannot be transmitted by mosquito bite, and 78.3% did not believe that HIV can be spread by sharing a meal with a PLHIV. Another large majority (85.8%) knew there was no cure for AIDS, and that the emergency contraceptive pill could not prevent HIV infection (94.9%). Fully 83% knew that there was no vaccine or prevent HIV infection, and that washing one’s genitals after sex could not prevent HIV infection (87.6%). Just under three-fourths (73.5%) knew that not wearing a condom during sex with a spouse or lover could spread HIV, and that Thai citizens are eligible for two free HIV tests per year (73.2%). The average AIDS knowledge score for this sample was quite high at 9.2 out of a potential score of 11, and females had significantly higher HIV/AIDS knowledge than their male counterparts.
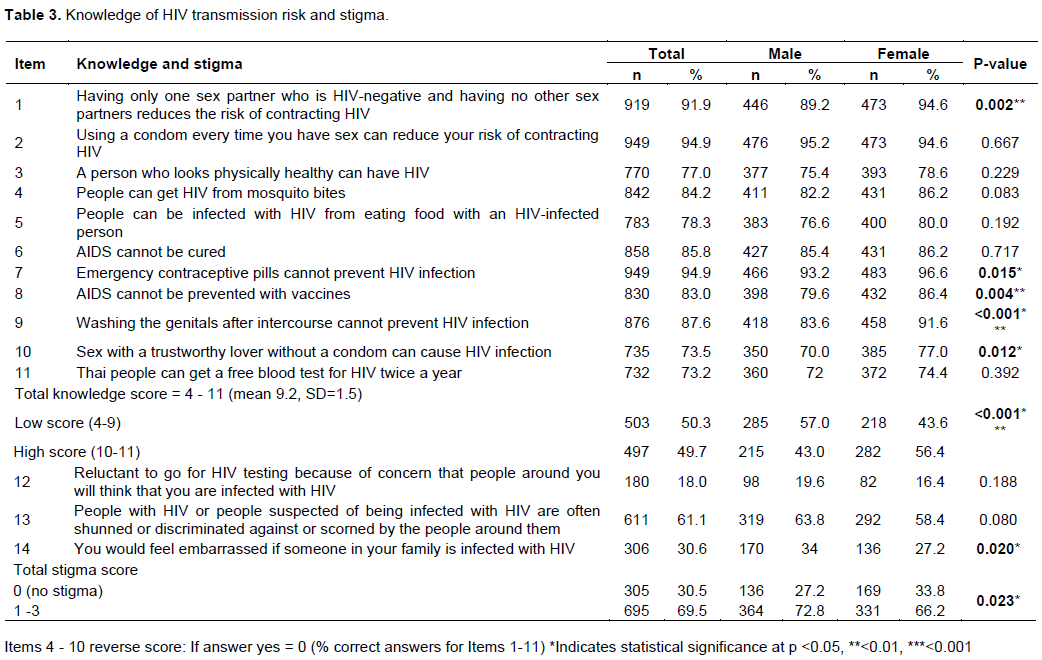
Under one in five (18.0%) were reluctant to go for HIV testing out of fear that someone they knew might see them and suspect that they had HIV. Indeed, over three-fifths (61.1%) believed that Thai society looks down on PLHIV or persons suspected of being infected, and nearly one-third (30.6%) would feel ashamed if a family member was a PLHIV. A similar proportion felt there was no longer any stigma about PLHIV, but more female respondents felt that way than their male counterparts, and that difference was statistically significant.
Table 4 presents results from the logistic regression which modeled the socio-demographic characteristics of the sample with the HIV/AIDS knowledge score, risk behavior, and stigma. Those with lower-than-average knowledge scores were younger (AOR 1.14; 95% CI 0.06 - 1.88), male (AOR 0.58; 95% CI 0.45 - 0.75), had educational attainment of less than bachelor’s degree (AOR 2.45; 95% CI 1.71 - 3.52), had migrated (AOR 1.66; 95% CI 1.25 - 2.19), had migrated to Bangkok from another province (AOR 1.36; 95% CI 1.06 - 1.75), had inadequate income to meet daily needs (AOR 2.23; 95% CI 1.27 - 3.89), had no close friends (AOR 1.62; 95% CI 1.03 - 2.56), experienced a moderate level of stress(AOR 1.47; 95% CI 1.05 - 2.07), and had worked in the current establishment for less than one year. The factor that was positively associated with (non-)stigma was being female (AOR 0.73; 95% CI 0.56 - 0.96), and factors associated with having more than one sex partner in the past year include age 26-45 years, being male, being married (AOR 2.85 ; 95% CI 1.59 - 5.09), having completed vocational education (AOR 1.98; 95% CI 1.24 - 3.18), and not having enough income to make ends meet (AOR 1.76; 95% CI 1.14 2.72).
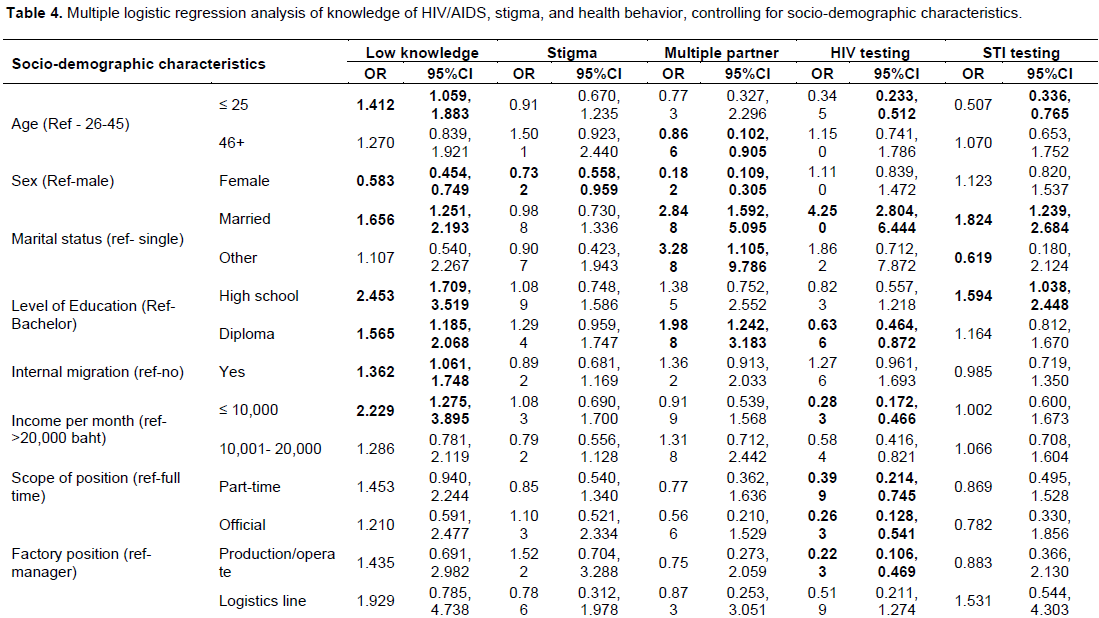
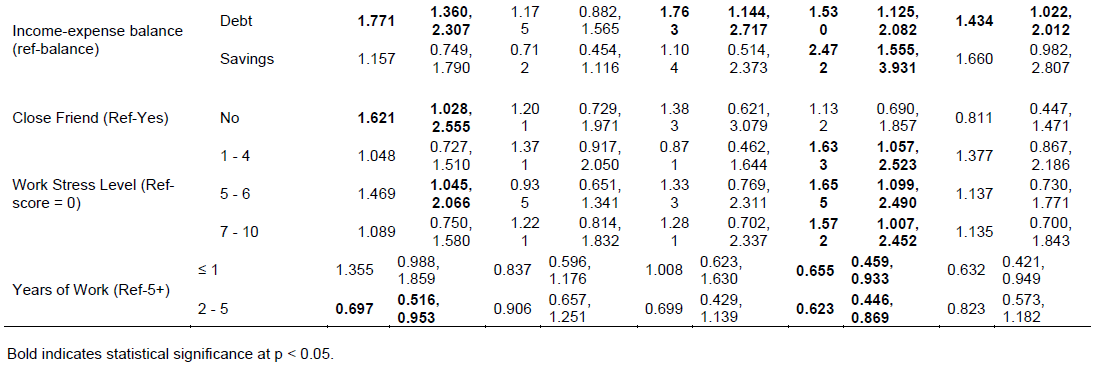
Factors associated with being tested for HIV in the past year include age 26 years or older, being married (AOR 4.25; 95% CI 2.80 - 6.44), having education at the level of a bachelor’s degree, having monthly income of more than 20,000 baht, working in a full-time capacity, having a management position, having an imbalance between income and expenditures, feeling stress at work (AOR 1.63; 95% CI 1.06 - 2.52), and having worked for the current employer for five years or more. Factors that were positively associated with history of screening for STI in the past year include age 26 years or older, being married (AOR 1.82; 95% CI 1.24 - 2.68), having only completed high school education (AOR 1.59; 95% CI 1.04 - 2.45), and being in debt (AOR 1.43; 95% CI 1.02 - 2.01).
DISCUSSION
Behaviors associated with HIV infection, stigma, and accurate knowledge of HIV/STI among economically- and socially-disadvantaged populations, such as industrial wage laborers in developing countries, remains a challenge. In this study, we observed differentials in stigma associated with HIV/STI among the sample of workers: Female workers had significantly less stigma toward PLHIV than their male counterparts. In addition, factors associated with a lack of accurate knowledge of HIV/STI include being male, being younger than 26 years, having less than bachelor’s degree education, being married, being a migrant, having lower economic status, having close friends, feeling stress at work, and having shorter duration of employment in the current workplace. This study highlights the need to design educational intervention measures to reduce stigma, combat HIV risk behavior, promote knowledge about HIV/ STI, and encourage annual health check-ups in this population to protect them from contracting HIV and STI.
Although industrial wage laborers are at risk for HIV and STI, they are no longer recognized as an important population in the HIV/STI prevention strategy in Thailand. At the time of this study, health promotion programs in this population focus primarily on occupational health and the environment. Nevertheless, the findings from this study highlight the fact that workers continue to practice risk behavior for STI and HIV. They harbor negative prejudices about PLHIV, and have insufficient knowledge about the prevention of HIV and STI. This study found that HIV/AIDS knowledge among this sample of Thai workers was greater than that for migrant workers in Myanmar, Vietnam, Nepal, China, and Cambodia (Nishigaya, 2002; Mullany et al., 2003; Hesketh et al., 2005; Puri and Cleland, 2006; Yang and Xia, 2006; Karki, 2014; Pham et al., 2019). However, the findings of these cross-national studies may differ due to variations of demographics and workplace contexts, and the instruments used to assess HIV/AIDS knowledge (Chamratrithirong et al., 2017). This study of Thai workers in Bangkok found that females were more knowledgeable about HIV transmission, and practiced more protective behaviors than males. That finding differs from previous studies which found that males were more knowledgeable about HIV transmission and practiced more prevention than females (Dehghani et al., 2021; Nguyen et al., 2021). One explanation is that the level of education affects knowledge which, in turn, can positively affect preventive behavior (Cabezas et al., 2013). In this study, significantly more female subjects had a bachelor's degree than their male counterparts, thus introducing a gender bias. Also, workers who were born in Bangkok had more knowledge about HIV/AIDS than workers who migrated from another province in Thailand. The Thai authorities are always on the alert for the potential for migrant workers to spread disease – especially cross-border migrants. Part of that bias is the belief that migrants will practice less health behavior and have greater background prevalence of infectious disease than Thais who are not migrants. Yet, this study exposed the fact that even among the population of non-migrant Thai workers, there are deficiencies in knowledge about HIV/STI prevention and such services as the free, semi-annual HIV screening service which all Thai citizens have the right to access.
The stigma associated with AIDS and PLHIV hinders access to HIV testing services and continuation of ART in all regions of the world. In addition, it is clearly seen that stigma associated with HIV is the leading cause of delays in seeking HIV testing and/or avoidance of other needed health care services (Pulerwitz et al., 2010; Stutterheim et al., 2017). A multi-national study found that lower-income workers held the view that PLHIV or those suspected of being HIV+ were looked down upon (Sprague et al., 2011; Weihs and Meyer-Weitz, 2016; Utuk et al., 2017). The stigma associated with HIV/AIDS was high in China, the USA, and Hong Kong where the public viewed HIV/AIDS more negatively than other chronic conditions or illness (Rao et al., 2008). In the US study, one-third of adults reported a negative attitude toward PLHIV (Beer et al., 2019). A Thai study found that stigma was identified as a significant factor in low uptake of HIV testing (Musumari et al., 2020). That is one explanation why PLHIV have such low CD4 counts when they finally start ART. The problem of stigma in the workplace not only affects workers, but also reduces the opportunity for the employer to play a more active role in promoting the health of their labor force (Bashir, 2011; Arimoto et al., 2013; Thepthien and Srivanichakorn, 2016; Muwanguzi et al., 2021). Thailand has designated reducing HIV/AIDS stigma as one of the main goals of the National Strategic Plan for AIDS Prevention and Response (Siraprapasiri et al., 2020). Thailand is implementing that plan in cooperation with the International Labor Organization, UNAIDS, employers’ associations, NGOs, and the national network of PLHIV. They have developed National Guidelines for the Prevention and Management of AIDS in the Workplace. In addition to reducing HIV/AIDS stigma, this effort is being implemented in tandem with the campaign to build a mechanism for PLHIV rights protection as a key part of Thailand's action plan to end AIDS. However, the present study did not examine the statistical relationship between stigma and uptake of HIV and STI screening services.
This study found that less than one in five workers had been screened for STI in the past year. Untreated, chronic STI can cause female infertility, pelvic inflammatory disease (PID), pathology of the reproductive system, and ectopic pregnancy. In addition, certain STI (that is, HPV, or genital warts) can increase the risk of cervical cancer (Francisco-Natanauan et al., 2021; Weinstock et al., 2021). Thailand has experienced an increase in STI in the past. The highest population prevalence of STI (excluding HIV) was reached in 1986, with a morbidity rate of 7.85 per 1,000 population. Perhaps due to the HIV prevention program and 100% “condom only” strategy, STI morbidity has steadily declined since the mid-80s to less than 20 per 100,000 population in the 21st century. However, in the past 5-10 years, incidence and prevalence of STI has started to increase again, mostly among the younger generation who never experienced the Thai HIV epidemic first-hand. The Bureau of Epidemiology of the Thai Ministry of Public Health (MOPH) reported that the STI morbidity rate during 2014-2019 increased from 18.8 to 33.8 per 100,000 population (Sawadcharoenying, 2020). The most common STI in Thailand was gonorrhea, followed by syphilis, and the sub-groups with the highest rates of STI were younger, working-age persons (whose morbidity rate increased from 54.2 to 124.6 per 100,000 population) (Division of AIDS and STIs, Department of Disease Control, 2021). The Thai national STI prevention and control program was launched nearly 90 years ago. Initially, the program had a vertical structure with its own network of offices, labs, and personnel based throughout the country in provincial health offices and some district facilities. Later, after the HIV epidemic occurred, STI control was merged with the AIDS control program due to the large number of sexually-transmitted HIV infections. The MOPH created the Bureau of AIDS, STI, and TB (BATS) as an integrated agency to address both STI and HIV. Since then, BATS has played the major role in national surveillance, prevention, and control of STI, and overall performance monitoring. Over the years, the emphasis of the Thai AIDS program shifted more to HIV prevention (and less to direct STI control) since many of the key interventions for HIV prevention would also prevent STI (e.g., condoms, faithful monogamy, reduction of casual/commercial sex, etc.). At the time of this study, national syphilis screening was only conducted as a routine service for pregnant women during ante-natal care (ANC) in public health facilities. However, there was little funding for active STI case finding and contact tracing as had been done in the past. This is a policy gap that has blunted the performance of the STI control effort in Thailand, which is now paying the price with a return to rising STI caseloads. More ominously, with the return of STI as a health problem of the new generation of the sexually-active, HIV will now have more opportunity to spread since STI increase the risk of contracting and transmitting HIV by many orders of magnitude (Sawadcharoenying, 2020).
The multivariate analysis identified socio-demographic differentials with regard to knowledge of HIV/AIDS and HIV/STI prevention. There were also differentials on perception of stigma and risk behavior of co-workers. These findings are consistent with previous studies suggesting that interventions to promote knowledge of HIV/STI may be implemented across a number of platforms to reach younger people where they work (Virakul and McLean, 2010). Although the effectiveness of the studies on each platform may require further analysis, it is worth noting that there are several lessons from past experience that may help design intervention formats, including the following: (1) The need for community-based engagement by mobilizing grassroots health workers to play an more active role in mentoring lower-income workers; (2) The need to take into account the socio-demographic-cultural factors which influence health-seeking behaviors of workers; and (3) The need to integrate technology to manage information. For example, due to the universal use of smartphones among the Thai working-age population, there should be a mobile phone application for periodic monitoring of health status and workplace knowledge (Spring et al., 2013). In addition, given the widespread use of social media and the widespread access to the Internet in urban Thailand, online information campaigns are essential in directing workers to reliable sources of information on HIV/STI, reducing negative views on AIDS/PLHIV, reducing risk behaviors, and steering people to effective health care services.
The findings indicate gaps in policy and access for workers to health services in the workplace. Every worksite is required to conduct annual health checks for employees (including ANC) in accordance with the Thai Occupational Health and Safety Act. Therefore, investment from employers may be needed to create opportunities to educate workers on STI prevention, especially in business establishments whose workers are risk-prone. It is also possible to provide incentives for local community health workers to educate the workplace labor force on STI prevention and sexual health during their routine outreach activities (Baker et al., 2004; Mahajan et al., 2007). In Thailand, HIV testing and treatment is available free of charge through public health services, but the challenge is to make workers aware that highly effective and free-of-charge screening and treatment are available. The employers should play a more important role in communicating these benefits to their employees. Thailand's labor policy clearly states that workers should know their HIV serostatus so that, if they become infected, they know at the earliest stage possible in the course of the infection, since ART is more effective the earlier it is administered. It goes without saying that worksites should never negatively discriminate against PLHIV, and there should never be compulsory HIV testing of the workforce or job applicants.
LIMITATION OF STUDY
This study has some limitations. First, the survey was conducted in the capital city (Bangkok), and findings may differ if the data were collected in provincial urban areas or, especially, rural worksites. Therefore, the findings cannot be extrapolated beyond that of the Bangkok business-establishment work environment. The data collection was done in 2019 and, thus, is almost two years old (at the time of this writing). Second, there may be recall bias. A cross-sectional study is weak in that it cannot reliably point to cause-effect relationships between factors and outcomes. In addition, there may be other factors, such accessibility to mass media, attitudes towards HIV infection, etc., not included in the questionnaire which has important effects on knowledge of STI, stigmatization, and risk behaviors, among other factors. There are environmental factors such as workplace conditions, health service providers, and workplace policy that can affect knowledge, attitudes, and behavior, and these were not measured or controlled for in this study. Finally, the study questionnaire did not ask about multiple risk behaviors that could affect knowledge of HIV/STI, stigmatization, and risk/prevention behaviors, such as the use of addictive drugs or same-sex sexual intercourse. Additionally, respondents are likely to under-report (rather than exaggerate) sexual behavior and substance use.
CONCLUSION
This study found gaps in knowledge and stigma surrounding HIV/AIDS, risky sexual behavior, substance abuse, prevention of HIV/STI, and other factors in a sample of industrial wage laborers in Bangkok, Thailand. Based on the findings, tailored educational interventions are needed to improve knowledge of HIV/STI, prevent infectious disease, decrease alcohol and tobacco use, and promote healthy lifestyles.
RECOMMENDATIONS
The results of this study have implications for several aspects of public health and policy. This study exposed gaps in knowledge about HIV/STI, stigma, risk behavior, and health check-ups among industrial wage laborers in Bangkok. Thus, there is a need for health education programs to increase knowledge on preventing HIV infection, reducing stigma, and the importance of knowing one’s HIV serostatus at the earliest possible time after infection. Health education programs must intensify the focus on regular and consistent condom use, and the signs, symptoms, and prevention of common STI. The results of the multivariate regression model suggest the need for more intensive interventions for youth, female workers with lower education, persons with lower socioeconomic status, and migrant laborers. Policies that can improve and promote reproductive health and prevention of HIV/STI are urgently needed for this population.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Arimoto Y, Ito S, Kudo Y, Tsukada K (2013). Stigma, social relationships, and HIV testing in the workplace: Evidence from South Africa. |
|
|
Baker S, Sartsara S, Rumakom P, Guest P, Schenk KD, Pramualratana A, Suparat S, Surachai P, Moonmeung S(2004). Using incentives to encourage AIDS programs and policies in the workplace: A study of feasibility and impact in Thailand. |
|
|
Bashir S (2011). HIV/AIDS stigma at the workplace: Exploratory findings from Pakistan. SAHARA-J. Journal of Social Aspects of HIV/AIDS 8(3):156-161. |
|
|
Beer L, McCree DH, Jeffries IV WL, Lemons A, Sionean C (2019). Recent US Centers for Disease Control and Prevention activities to reduce HIV stigma. Journal of the International Association of Providers of AIDS Care (JIAPAC) |
|
|
Cabezas MC, Fornasini M, Dardenne N, Borja T, Albert A (2013). A cross-sectional study to assess knowledge about HIV/AIDS transmission and prevention measures in company workers in Ecuador. BMC Public Health 13(1):1-9. |
|
|
Chamratrithirong A, Ford K, Punpuing S, Prasartkul P (2017). A workplace intervention program and the increase in HIV knowledge, perceived accessibility and use of condoms among young factory workers in Thailand. SAHARA-J: Journal of Social Aspects of HIV/AIDS 14(1):132-139. |
|
|
Chen D, Luo G, Meng X, Wang Z, Cao B, Yuan T, Xie Y, Hu T, Chen Y, Ke W, Wang Z, Zou H (2020). Efficacy of HIV interventions among factory workers in low-and middle-income countries: A systematic review. BMC Public Health 20(1):1-12. |
|
|
Dehghani B, Shahsavani Z, Dehghani A (2021). HIV/AIDS awareness and attitudes among factory workers in Shiraz, Iran. Journal of Current Biomedical Reports. |
|
|
Division of AIDS and STIs, Department of Disease Control, Ministry of Public health, Thailand (2021). Five mains of STIs report cases in Thailand. |
|
|
Francisco-Natanauan P, Leatherman-Arkus N, Pantell RH (2021). Chlamydia and gonorrhea prevalence and treatment in detained youths: Strategies for improvement. Journal of Adolescent Health 68(1):65-70. |
|
|
Hesketh T, Zhang J, Qiang DJ (2005). HIV knowledge and risk behaviour of female sex workers in Yunnan Province, China: Potential as bridging groups to the general population. AIDS Care 17(8):958-966. |
|
|
Hong SA, Thepthien BO (2017). HIV risk-related sexual behavior by cohabiting partner status among factory workers: Results from the 2015 Bangkok Behavioral Surveillance Survey (BBSS). Cogent Social Sciences 3(1):1364070. |
|
|
Karki TB (2014). Correlation between knowledge, attitude and practices on HIV and AIDS: Cases from the Kathmandu Valley. Journal of Nepal Health Research Council 12(26):24-9. |
|
|
Kiderlen TR, Conteh M, Roll S, Seeling S, Weinmann S (2015). Cross-sectional study assessing HIV-related knowledge, attitudes and behavior in the Namibian truck transport sector: Readjusting HIV prevention programs in the workplace. Journal of Infection and Public Health 8(4):346-354. |
|
|
Kumar A, Deb M, Saha MK, Chakraborty S, Bhattacharya SK, Detels R (2009). HIV transmission potential among local and migrant factory workers in Kolkata, India. AIDS and Behavior 13:928-938. |
|
|
Mabathoana RS, Van Wyk C, Adefuye AO (2019). Factors influencing HIV risk-taking behaviours amongst textile factory workers living with HIV in Lesotho. The Pan African Medical Journal, 33. |
|
|
Mahajan AP, Colvin M, Rudatsikira JB, Ettl D (2007). An overview of HIV/AIDS workplace policies and programmes in southern Africa. AIDS 21:S31-S39. |
|
|
Mahmood S (2021). Female Garment Workers' Understandings of HIV in Bangladesh. American Journal of Public Health 9(2):81-89. |
|
|
McFarland W, Gwanzura L, Bassett MT, Machekano R, Latif AS, Ley C, Julie P, Rae LB, Katzenstein D (1999). Prevalence and incidence of herpes simplex virus type 2 infection among male Zimbabwean factory workers. Journal of Infectious Diseases 180(5):1459-1465. |
|
|
Mullany LC, Maung C, Beyrer C (2003). HIV/AIDS knowledge, attitudes, and practices among Burmese migrant factory workers in Tak Province, Thailand. AIDS Care 15(1):63-70. |
|
|
Musumari PM, Techasrivichien T, Srithanaviboonchai K, Tangmunkongvorakul A, Ono-Kihara M, Kihara M (2020). Factors associated with HIV testing and intention to test for HIV among the general population of Nonthaburi Province, Thailand. PloS One, 15(8):e0237393. |
|
|
Nguyen DN, Vu HM, Muwanguzi PA, Bollinger RC, Ray SC, Nelson LE, Kiwanuka N, Bauermeister JA, Sewankambo NK (2021). Drivers and barriers to workplace-based HIV self-testing among high-risk men in Uganda: A qualitative study. BMC Public Health 21(1):1-13. |
|
|
Nguyen QN, Nguyen CT, Do HT, Vu TMT, Ho RC (2021). Gaps in Knowledge about HIV and Sexually Transmitted Infections among Industrial Workers in Northern Vietnam. AIDS and Behavior pp. 1-8. |
|
|
Nguyen VH, Dunne MP, Debattista J, Nguyen TH, Dao TMA (2012). Social contexts of risk behaviors for HIV among male, unskilled, unregistered laborers in urban Vietnam. Qualitative Health Research 22(7):871-879. |
|
|
Pham KTH, Nguyen LH, Vuong QH, Ho MT, Vuong TT, Vu GT, Ho R (2019). Health inequality between migrant and non-migrant workers in an industrial zone of Vietnam. International Journal of Environmental Research and Public Health 16(9):1502. |
|
|
Pulerwitz J, Michaelis A, Weiss E, Brown L, Mahendra V (2010). Reducing HIV-related stigma: Lessons learned from Horizons research and programs. Public Health Reports 125(2):272-281. |
|
|
Puri M, Cleland J (2006). Sexual behaviour and perceived risk of HIV/AIDS among young migrant factory workers in Nepal. Journal of Adolescent Health 38(3):237-246. |
|
|
Rao D, Angell B, Lam C, Corrigan P (2008). Stigma in the workplace: Employer attitudes about people with HIV in Beijing, Hong Kong, and Chicago. Social Science & Medicine 67(10):1541-1549. |
|
|
Sakboonyarat B, Mungthin M, Nelson KE, Rangsin R (2021). Rising prevalence of HIV infection and associated risk factors among young Thai Men in 2018. Scientific Reports 11(1):1-10. |
|
|
Sawadcharoenying P (2020). Prevention and control implemented by the Division of AIDS and STI during 2010-2019. Thai AIDS Journal 32(3):94-113. |
|
|
Siraprapasiri T, Srithanaviboonchai K, Chantcharas P, Suwanphatthana N, Ongwandee S, Khemngern P, Patchara B, Pia M, Nyblade L (2020). Integration and scale-up of efforts to measure and reduce HIV-related stigma: Experience of Thailand. |
|
|
Sprague L, Simon S, Sprague C (2011). Employment discrimination and HIV stigma: Survey results from civil society organizations and people living with HIV in Africa. African Journal of AIDS Research 10(sup1):311-324. |
|
|
Spring B, Duncan JM, Janke EA, Kozak AT, McFadden HG, DeMott A, Pictor A, Epstein LH, Siddique J, Pellegrini CA, Buscemi J (2013). Integrating technology into standard weight loss treatment: Randomized controlled trial. JAMA Internal Medicine 173(2):105-111. |
|
|
Stutterheim SE, Brands R, Baas I, Lechner L, Kok G, Bos AE (2017). HIV status disclosure in the workplace: Positive and stigmatizing experiences of health care workers living with HIV. Journal of the Association of Nurses in AIDS Care 28(6):923-937. |
|
|
The Joint United Nations Programme on HIV and AIDS (UNAIDS). (2020) UNAIDS data 2020. Geneva: UNAIDS; 2019. |
|
|
Thepthien BO, Srivanichakorn S (2016). Societal awareness of stigma and discrimination against persons living with Human Immunodeficiency Virus (HIV) (PLHIV): Experience of clinicians, PLHIV, general population, and persons who are vulnerable to HIV. Journal of AIDS and HIV Research 8(4):25-37. |
|
|
Tran BX, Vo T, Dang AK, Nguyen QN, Vu GT, Vu LG, Khanh ND, Carl AL, Cyrus SHH, Ho R (2019). Characterizing unsafe sexual behavior among factory workers in the context of rapid industrialization in northern Vietnam. International Journal of Environmental Research and Public Health 16(24):5085. |
|
|
Utuk IG, Osungbade KO, Obembe TA, Adewole DA, Oladoyin VO (2017). Stigmatising attitudes towards co-workers with HIV in the workplace of a metropolitan state, Southwestern Nigeria. The Open AIDS Journal 11:67. |
|
|
Virakul B, McLean GN (2010). Re?visiting HIV/AIDS in the workplace and HR work in Thai business organizations. Journal of Global Responsibility. |
|
|
Weihs M, Meyer-Weitz A (2016). Barriers to workplace HIV testing in South Africa: A systematic review of the literature. AIDS Care 28(4):495-499. |
|
|
Weinstock HS, Kreisel KM, Spicknall IH, Chesson HW, Miller WC (2021). STI Prevalence, Incidence, and Costs in the United States: New Estimates, New Approaches. Sexually Transmitted Diseases 48(4):207. |
|
|
World Health Organization (WHO) (2018) Report on global sexually transmitted infection surveillance, 2018. Geneva. |
|
|
World Health Organization (WHO) (2016). Global health sector strategy on sexually transmitted infections: 2016-2021: Towards ending STI. Geneva. |
|
|
Yang X, Xia G (2006). Gender, work, and HIV risk: determinants of risky sexual behavior among female entertainment workers in China. AIDS Education and Prevention 18(4):333-347. |
|
|
Yi S, Tuot S, Chhoun P, Pal K, Chhim K, Ngin C, Brody C (2018). Sexual behaviors, HIV knowledge, HIV testing attitudes and recent sHIV testing among female entertainment workers in Cambodia: A cross-sectional study. PLoS One 13(7):e0198095. |
|
|
Zhang M, Anglewicz P, VanLandingham M (2020). Migration and sexual partnerships among unmarried young men in Thailand: A longitudinal approach. International Journal of Public Health 65(9):1681-1688. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


