Full Length Research Paper

ABSTRACT
Tenofovir-based regimen is the preferred first line treatment in Ethiopia despite limited local data on its effectiveness and tolerability over zidovudine-based regimen. Therefore, this study compared the outcomes of tenofovir and zidovudine-based regimens focusing on toxicity driven regimen substitution and mortality. A retrospective cohort study was conducted in Zewditu Memorial Hospital. All ART naïve patients who started ART between August 31, 2010, and August 31, 2013, were included. Data were collected by reviewing of patient’s medical records. Kaplan-Meier test and Cox regression analysis were used to compare survival for toxicity driven substitution and mortality, and to identify the independent predictors respectively. A total of 223 patients were included in this study, among which 164 (73.5%) TDF and 59 (26.6%) AZT-based regimens. A total of 71 (31.8%) primary outcomes such as toxicity driven regimen substitution, mortality, and lost to follow-up were observed, 48(29.3%) among TDF and 23(39.0%) in AZT-based regimens. The risk of toxicity driven regimen substitution was more than five times higher in AZT than TDF group (AHR=5.07, p=0.013). The estimated cumulative mortality at 6, 12, 18 and 24 months was 6, 9, 9 and 9% in TDF group whereas it was 9, 13, 13, and 13% in AZT group. There was no statistically significant difference in mortality and regimen failure between TDF and AZT groups. TDF-based regimen has superior outcome and better survival for toxicity driven regimen change than AZT-based regimen. This study finding supports recommendation of TDF-based regimen as preferred first-line ART.
Key words: antiretroviral therapy (ART), Tenofovir (TDF), Zidovudine (AZT), toxicity driven regimen substitution, Survival.
Abbreviation: ART, Antiretroviral Therapy; AZT, Zidovudine; EFV, Efavirenz; eGFR, estimated Glomerular Filtration Rate; Hgb, Hemoglobin; NVP, Nevirapine; TDF, Tenofovir; WHO, World health organization; ZMH, Zewuditu Memorial Hospital; 3TC, Lamivudine; PYR, Person years.INTRODUCTION
Human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) is the public health problem that has claimed more than 32 million life until 2019 globally. According to the USAID estimate, currently, about 37.9 million people are living with the virus of which more than 50% (20.6 million) are in the Eastern and Southern Africa regions. Ethiopia, as part of this region, is among the highly affected countries with 1.0% national HIV prevalence (UNAIDS, 2019). Besides, HIV/AIDS is among the top ten killer diseases in Ethiopia (FMOH, 2016).
With improved access to antiretroviral therapy (ART) the HIV related mortality and morbidity have significantly reduced (WHO, 2016). However, the success of life-long ART requires safer, more efficacious, and convenient regimens to the patient. Following advances in scientific understanding of HIV prevention, care, and treatment World Health Organization (WHO) frequently treatment guideline update. The revision of the HIV-treatment guideline in 2010 brought several changes to the management of HIV-infected patients. This guideline recommended both zidovudine (AZT) and tenofovir (TDF)-based regimens containing efavirenz (EFV) or nevirapine (NVP) as first-line options (WHO, 2010). However, WHO (2013) consolidated guideline recommend TDF/3TC/EFV regimen as preferred first-line (WHO, 2013). The second consolidated WHO guideline on ART for prevention, care, and treatment was developed in 2016 (WHO, 2016).
Despite TDF being the preferred agent, there are inconsistent findings on the comparative efficacy and safety of TDF compared to AZT-based regimens. There are reports that TDF-based regimens have superior viral load suppression and better tolerability compared to AZT-based regimens (Dadi et al., 2017). However, TDF was associated with a greater decline in renal function and a high risk of proximal tubular dysfunction in naïve HIV patients (Horberg et al., 2010). Furthermore, studies have indicated that the overall difference in mortality between patients taking AZT and those taking TDF is not statistically significant. In a retrospective cohort study from Nigeria, higher immunological and virologic failure was observed in patients taking TDF compared to AZT (Tchetgen et al., 2016). Although in most of the early clinical trials there was no report on discontinuation of TDF due to toxicity (Gallant et al., 2006; Arribas et al., 2008), recently an observational study in a developed setting has reported a significantly high incidence of discontinuation due to TDF-associated toxicities (Costarelli et al., 2016). However, ART outcomes and toxicities in developed countries differ from that in developing countries due to the high prevalence of conditions such as anemia, malnutrition, tuberculosis, and patients’ initial presentation with advanced diseases (Subbaraman et al., 2007).
Ethiopia has made tremendous progress in the care and treatment of HIV/AIDS by providing free antiretroviral therapy services in public health facilities since 2005. Following the release of the 2013 WHO consolidated guideline (WHO, 2013), Ethiopia adopted its guideline based on this guideline and implemented a TDF-based regimen as the preferred regimen (Ethiopian FMoH, 2014). Following the implementation of the TDF- based regimen, few studies compared the outcomes of TDF and AZT-based regimens in Ethiopia. For example, a study in Jimma University has compared the immunological and clinical outcomes of the two regimens (Ayele et al., 2017), but this study did not investigate outcomes related to regimen substitution or toxicities. In Ethiopia, the expansion of free antiretroviral therapy services is effective in improving quality of life, reducing morbidity and mortality, and increasing productivity in patients infected with HIV. However, there is a need to better understand the long-term outcomes of combination treatment regimens. Therefore, the aim of this study is to determine and compare the outcomes of TDF and AZT-based regimens as first-line ART among treatment naïve HIV/AIDS patients.
METHODOLOGY
Study design and setting
This study is based on a retrospective cohort study design to compare tenofovir and zidovudine- based ART regimens. The study was conducted in Zewditu Memorial Hospital (ZMH) from August 31, 2010, to August 31, 2013. The first ART service was started in Ethiopia in ZMH and still, it is one of the hospitals in Addis Ababa where better ART services are provided. ZMH is administered under the Addis Ababa Health Bureau, Addis Ababa Ethiopia.
Source and study population
The source population was all HIV/AIDS patients attending the ART Clinic at ZMH. Our study population was all treatment naïve HIV/AIDS patients initiated on TDF or AZT-based regimens at ZMH and who fulfill inclusion criteria.
Inclusion and exclusion criteria
All HIV/AIDS patients aged above 15 years old and started TDF or AZT-based regimens at ZMH during the study period were eligible for this study. Patients who had prior ART experience, regimen changed due to tuberculosis treatment and pregnancy, regimen substitution that did not involve TDF or AZT, or regimen substitution with unknown reasons were excluded from the study.
Sample size and sampling technique
The sample size was determined by using a two-population proportion formula through EPI INFO Stat Calc program with the assumption of a 95% level of confidence, power of 80%, 5% of marginal error, and taking prevalence of toxicity-driven regimen substitution of 3% and 8.1% for TDF and AZT-based regimens respectively from a similar study in Africa (Bygrave et al., 2011) and 1:1 ratio between the two cohorts, the sample size was calculated to be 634 (n=317/cohort). However, by taking three years of data from the ART registration book at the ZMH ART clinic, the total number of patients started ART on AZT and TDF-based regimens were 138 and 941 respectively. Due to the small number of patients started on AZT-based regimens, the sample size was reduced using the following sample size reduction formula to 245.
Where n1-the calculated sample size in each group
nt- total calculated sample size
Nr- number of patients in each regimen
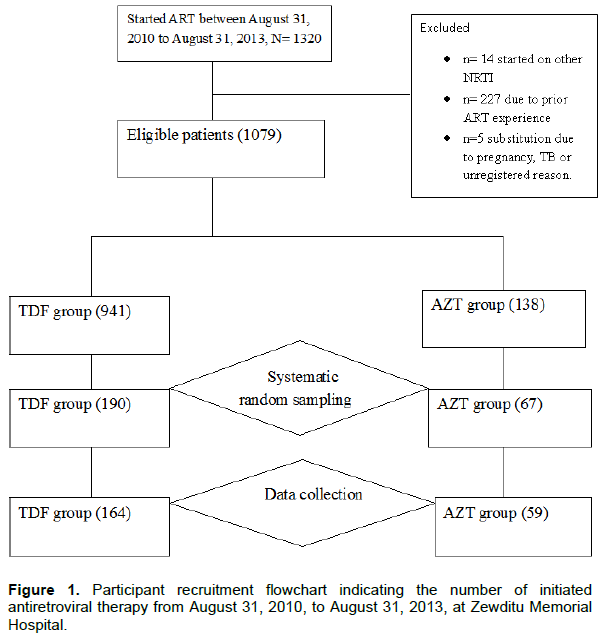
nfinal- corrected final sample size Study samples were selected by using a systematic random sampling method. Therefore, by using sampling interval 2 for AZT (k=2.42) and 6 for TDF (k=5.95), 190 and 67 cases in TDF and AZT groups were reviewed, respectively. Due to lack of major baseline information, empty patient folder, and regimen substitution because of other reasons, the final number of patients in this study was 164 and 59 in TDF and AZT groups respectively (Figure 1).
Study variables
Independent variables of this study include exposure to TDF and AZT, socio-demographic characteristics of participants, and baseline clinical characteristics (CD4 count, hemoglobin, estimated GFR, body weight, WHO clinical stage, presence of opportunistic infections, tuberculosis treatment, concomitant chronic diseases, opportunistic infection prophylaxis, and pregnancy). Primary outcomes of our study are the time to toxicity driven regimen substitution, lost to follow-up, and time to death. Secondary outcome variables include a change in CD4 count, change in hemoglobin, and change in estimated glomerular filtration rate (eGFR).
Data collection procedures
Data were collected by two nurses and two pharmacists working in the ART clinic of ZMH after being trained for one day on the aim of this study and how to fill the required data. The data were collected using a standardized and pretested questionnaire that contained socio-demographic, clinical, laboratory, and ART follow-up information. Patient medical records and ART patients’ information records were used as a source of data.
Data analysis
Data were entered into the computer by using EPI INFO Version 3.5.1. Then it was exported to SPSS 20.0 for analysis. Summary descriptive statistics for continuous baseline characteristics and change in CD4 count, eGFR, and hemoglobin at 6, 12, and 24 months were tabulated and the data were assessed for normality. The decision on the assumption of normality was made based on the aggregate results obtained from the Kolmogorov-Smirnov test, skewness and kurtosis statistics, histogram, and quantile plots. Furthermore, critical values estimated 95% range, and the difference in mean and median values was computed from the descriptive table and used as additional evidence for the decision of normality. Continuous variables were described using mean and categorical variables were described using percentages and frequencies. Patients’ characteristics at ART initiation by initial nucleoside reverse transcriptase inhibitor (TDF and AZT) were compared using the chi-square test for categorical variables, independent samples t-test for continuous variables with normal distribution, and Mann-Whitney U test for continuous variables with skewed distribution. The changes in CD4 count, eGFR, and hemoglobin in TDF and AZT groups at 24 months were compared with independent samples t-test but at 6 and 12 months of follow up Mann-Whitney U test was used to compare the changes in the two groups.
Time zero was considered the date of ART initiation and patients were followed for two years. Follow up was censored at the first toxicity driven regimen substitution, death, loss to follow-up, transfer out, or still in care at the database closure. The Kaplan-Meier curve was used to estimate the duration of treatment outcomes. A log-rank test was used to compare survival curves between TDF and AZT based regimens. The Bivariate Cox regression model was used to test the effect of covariates on the outcomes. Variables with p-value ≤ 0.25 in bivariate Cox-regression were considered as candidates for multivariate regression. Hazard ratio with 95% CI was used as a measure of the strength of association and p-value < 0.05 was considered to declare statistical significance.
Ethical considerations
Ethical clearance was obtained from Addis Ababa University, School of Pharmacy ethical review board. Also, permission was obtained from ZMH to access patients’ medical records. The confidentiality of reviewed patient information was maintained through the coding of individual patient data.
RESULTS
Socio-demographic and clinical characteristics
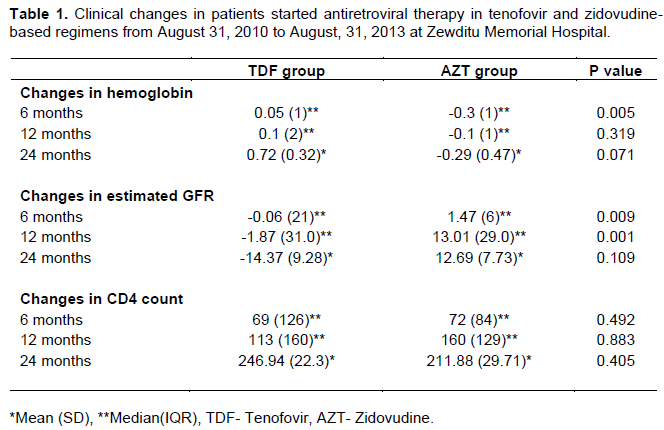
The socio-demographic and baseline clinical characteristics of participants are described in Table 1. In this study, a total of 223 participants were included for final data analysis. The majority of participants were females 119 (53.4%) and the age of less than 40 years 147(65.92%). In this study, 164 (73.54%) patients were on a TDF-based regimen and 173 (77.6%) used EFV as NNRTI backbone. In TDF and AZT groups, the NNRTI EFV was used in 138 (84.1%) and 35 (59.3%) patients respectively. More than half of the patients have started therapy with a baseline CD4 count of 50-199 cells/mm3 and the mean CD4 count of the cohorts was 154.46 cells/mm3 (SD=89.31). Within TDF and AZT groups, 56.7 and 47.5% patients respectively started with baseline CD4 count 50-199 cells/mm3. The overall median (IQR) eGFRs at baseline in TDF and AZT groups were 111.09(37.73) and 99.38((30.05) ml/min respectively. The mean (SD) hemoglobin values in TDF and AZT groups were 13.45(1.83) and 14.6 (1.8) g/dl respectively. There was no statistically significant difference between the two cohorts concerning baseline CD4 count, hemoglobin, and eGFR.
Follow-up and ART outcomes
The mean follow-up duration of the cohort on the TDF- based regimen was 555.54 (SD=254.93) days and on the AZT-based regimen was 489.24(SD=289.78) days with an overall mean of 538.0 (SD=265.54) days. Participants in the TDF-based group stayed on follow-up from a minimum of 30 days and to a maximum of 730 days, while the AZT group stayed for a minimum of 60 days and a maximum of 730 days. Overall, the patients in the TDF group were followed up for a total duration of 25,008.33 PYRs and patients in the AZT group were followed up for 7,900.0 PYRs. The primary outcomes were observed in 71 (31.8%) patients in the two years follow-up of this cohort. Among TDF-regimen based patients, 48(29.3%) patients experienced the primary events including toxicity driven regimen substitution 4(2.4%), death 14(8.5%), and lost to follow-up 30(18.3%). On the other hand, among the AZT regimen-based patients 23(39.0%) patients experienced the event such as toxicity driven regimen substitution 8(13.6%), death 7(11.9%), and lost to follow-up 8(13.6%).
Time to toxicity-driven regimen substitution
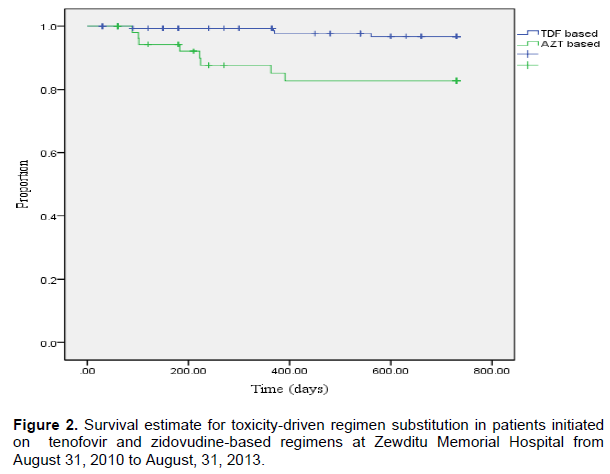
Over the two years of ART, a composite of 12(5.4%) patients had toxicity driven regimen substitution. Of this 4(2.4%) were from TDF and 8(13.6%) from the AZT group. In the TDF group, the estimated toxicity driven regimen substitution was 1, 2, 3 and 3% at 6, 12, 18 and 24 months respectively. In AZT group it was 6, 12, 17, and 17% at 6, 12, 18, and 24 months respectively. The mean time to toxicity driven substitution was 718.26 and 641.83 days in TDF and AZT groups, respectively. The composite rate of toxicity driven regimen substitution for the cohort was 3.65 per 100 PYR (CI 95%: 1.88-6.37). TDF-based regimens were substituted at a rate of 1.6 per 100 PYR (CI 95%: 0.43-4.1) compared with 10.13 per 100 PYR (CI 95%: 4.36-19.95) for AZT-based regimens. Patients exposed to TDF had favorable time to the event, and the difference was significant (p=0.001) as shown by the Kaplan-Meier survival estimate (Figure 2).
Factors for toxicity-driven regimen substitution
In bivariate Cox-regression analysis; sex, age, nucleoside reverse transcriptase inhibitors group, baseline body weight, hemoglobin, and concomitant chronic diseases showed significant association with toxicity driven regimen substitution (p<0.25). Therefore, these variables were retained in the multivariate Cox regression analysis with the treatment groups.
In multivariate analysis, patients in AZT group were 5.07 times more likely to have toxicity driven regimen substitution compared to patients in TDF group (adjusted hazard ratio =5.07, 95% CI:1.4-18.33, p = 0.013) when adjusted for confounders sex, age, hemoglobin, weight and concomitant chronic diseases (Table 1).
Clinical and immunologic outcomes
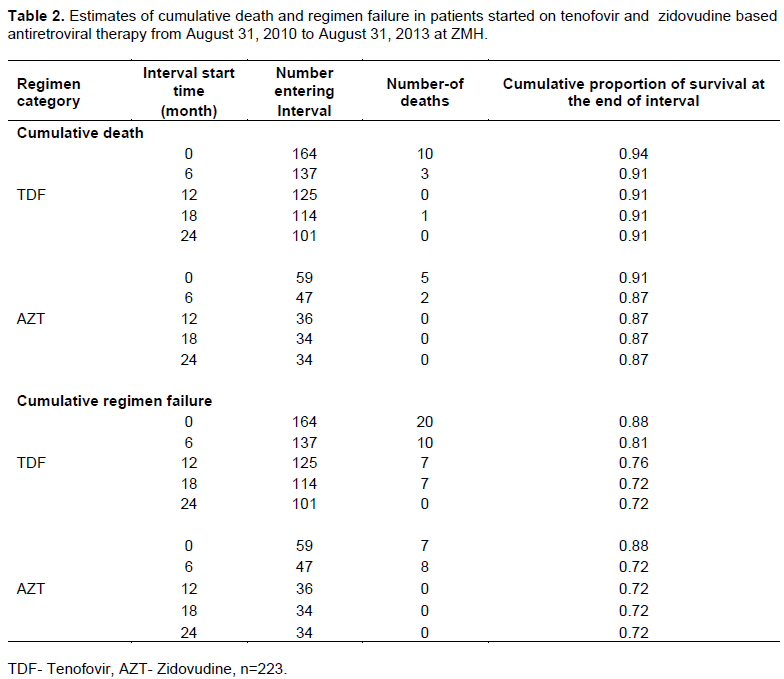
The clinical outcomes were monitored using hemoglobin and eGFR while the immunologic outcome was monitored by CD4 count (Table 2).
Factors for toxicity-driven regimen substitution
In bivariate Cox-regression analysis; sex, age, nucleoside reverse transcriptase inhibitors group, baseline body weight, hemoglobin, and concomitant chronic diseases showed significant association with toxicity driven regimen substitution (p<0.25). Therefore, these variables were retained in the multivariate Cox regression analysis with the treatment groups.
In multivariate analysis, patients in AZT group were 5.07 times more likely to have toxicity driven regimen substitution compared to patients in TDF group (adjusted hazard ratio =5.07, 95% CI:1.4-18.33, p = 0.013) when adjusted for confounders sex, age, hemoglobin, weight and concomitant chronic diseases (Table 1).
Clinical and immunologic outcomes
The clinical outcomes were monitored using hemoglobin and eGFR while the immunologic outcome was monitored by CD4 count (Table 2).
Change in hemoglobin
The median (IQR) hemoglobin levels at 6, 12 months were 13.8 (1.88), and 13.7 (2) g/dl in TDF and 14.3(2.3) and 14.5 (4.35) g/dl in AZT groups respectively. At the end of 24 months follow up, the mean (SD) hemoglobin levels were 14.15 (1.32) and 13.84 (1.32) g/dl in TDF and AZT groups respectively. The change in hemoglobin at 6 months showed a significant reduction from baseline in the AZT group (p= 0.005), however, the change in hemoglobin at 12 and 24 months of follow up did not show statistically significant differences among TDF and AZT groups (Table 2).
Change in glomerular filtration rate
In TDF group the median (IQR) eGFR levels were 112.35 (38.29), 109.56 (38.28) and 107.8 (32.62 ml/min at 6, 12 and 24 months respectively. On the other hand, the median (IQR) eGFR levels were 105.74 (30.76), 104.71 (33.9), and 116.44 (25.5) ml/min at 6, 12, and 24 months respectively in the AZT group. The change in eGFR at 6 and 12 months of follow up showed a significant reduction from baseline in the TDF group as compared to the AZT group.
Change in CD4 count
The median (IQR) CD4 counts at 6 and 12 months were 205 (165) and 266 (202) cells/mm3 in TDF and 247 (106) and 273 (167) cells/mm3 in AZT groups respectively. At the end of the follow-up, the mean (SD) CD4 counts were 414.47 (208.54) and 387.54 (144.12) cells/mm3 in TDF and AZT groups respectively. The changes in CD4 count showed no statistically significant difference between TDF and AZT groups.
Mortality and regimen failure
In the TDF group, the estimated cumulative mortality was 6, 9, 9, and 9% at 6, 12, 18, and 24 months respectively. In the AZT group, the estimated mortality was 9, 13, 13, and 13% at 6, 12, 18, and 24 months respectively. On the other hand, the cumulative regimen failure in the TDF group was 12, 19, 24, and 28% at 6, 12, 18, and 24 respectively. The cumulative regimen failure in the AZT group was 12, 28, 28, and 28% at 6, 12, 18, and 24 months respectively (Table 2).
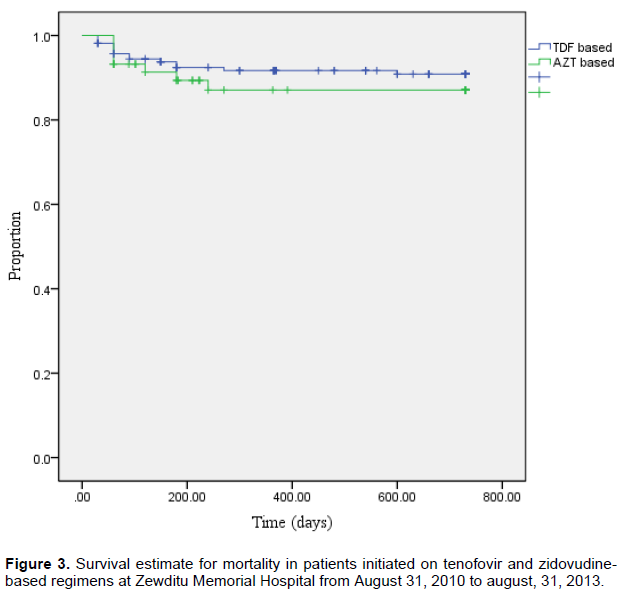
The overall rate of mortality for the cohort was 6.38 deaths per 100 PYRs (CI 95%: 2.55-15.65). The mortality rate in the AZT group was 8.86 death per 100 PYRs (CI 95%: 3.55-18.26) which is higher than in the TDF-based group which is 5.6 death per 100 PYRs (CI 95%: 3.06-9.39). The mean time to death was 676.82days (95% CI:649.56-704.07) and 651.06 days (95% CI:596.25- 705.86) for TDF and AZT groups respectively. The time to death between the two cohort groups did not show a statistically significant (p=0.426) difference (Figure 3). On the other hand, the meantime to regimen failure was 597.99 days (95% CI: 561.57-634.42) and 570.8 days (95% CI: 501.61- 639.99) for TDF and AZT-based regimens respectively (p=0.876).
Predictors of mortality
In bivariate Cox regression analysis age, sex, baseline estimated GFR, CD4 count, opportunistic infections, WHO stage, weight, tuberculosis treatment, and non-nucleoside reverse transcriptase inhibitors were associated with mortality (p < 0.25). These variables were retained in the multivariate Cox regression model in addition to the nucleoside reverse transcriptase inhibitor groups. The hazard for mortality among TDF and AZT groups did not show a statistically significant difference (AHR= 2.1, p = 0.188).
DISCUSSION
The present study investigated comparative outcomes of TDF-and AZT-based antiretroviral treatment in HIV/AIDS patients in Ethiopia in terms of toxicity driven regimen substitution, morality, and lost to follow-up. The number of participants on TDF was higher than the AZT-based regimen which is due to the WHO recommendation TDF/3TC/EFV based regimen as the preferred regimen at the time (WHO, 2010, 2013). More than half of patients have started therapy with a baseline CD4 count 50-199 cells/mm3 and the mean CD4 count of the cohorts was 154.46 cells/mm3. Within TDF and AZT groups, 56.7 and 47.5% patients respectively started with baseline CD4 count 50-199 cells/mm3. The baseline CD4 count for most patients was low, which may be associated with eligibility criteria during the study period (CD4 below 350 copies/mm3) or lack of awareness of society for early HIV testing (WHO, 2010). Assessment of baseline CD4 count, hemoglobin, and eGFR between did not indicate a statistically significant difference between TDF and AZT cohorts.
Analysis of the primary outcomes indicated that in the two years follow-up, 48(29.3%) of TDF-based groups experienced the primary events including toxicity driven regimen substitution while 23(39.0%) of AZT- based groups experienced the event such as toxicity driven regimen. The mean time to event for toxicity driven substitution was 718.26 and 641.83 days in TDF and AZT groups respectively. This shorter time to toxicity driven regimen substitution in the AZT group is consistent with the study finding in Zimbabwe which reported time to toxicity driven regimen in the AZT group 388 day and in the TDF group 618 days (Mudzviti et al., 2015). However, our finding, in contrast, to study in South Africa that reported a shorter time to toxicity driven regimen change in the TDF group (1.5 years) than AZT group(2 years) (Njuguna et al., 2013). Multivariate analysis for independent predictors indicated that patients in the AZT group were 5 times more likely to have toxicity driven regimen substitution compared to patients in the TDF group when adjusted for sex, age, hemoglobin, weight, and concomitant chronic diseases. Our findings are supported by different studies in several countries in Africa (Ethiopian FMoH, 2014; Mudzviti et al., 2015; Njuguna et al., 2013; Moh et al., 2005) that reported a higher risk of toxicity driven regimen substitution in the AZT-based regimen as compared to the TDF-based regimen.
Analysis of clinical and immunological responses was performed in our study. The change in hemoglobin at 6 months showed a significant reduction from baseline in the AZT group, however, the change in hemoglobin at 12 and 24 months of follow up did not show statistically significant differences among TDF and AZT groups. This may be explained by the fact that AZT associated anemia is an early side effect that occurs in the first 6 months (Moh et al., 2005). The change in eGFR at 6 and 12 months of follow up showed a significant reduction from baseline in the TDF group as compared to the AZT group. This finding is similar to the results of other studies (Horberg et al., 2010; Pozniak et al., 2006), in which significantly lower change in eGFR was observed in patients treated with TDF- based regimens. However, the study in Zambia (Moh et al., 2005), found no significant difference between TDF and AZT groups at 6 and 12 months of follow up. These inconsistencies among studies on the renal function may be associated with differences in the socio-demographic characteristics of participants and lack of accurate documentation of laboratory results.
Similarly, the changes in CD4 count showed no statistically significant difference between TDF and AZT groups. Our finding is consistent with similar studies in Eritrea (Medhanie et al., 2015) and India (Bygrave et al., 2011; Hemasri et al., 2016). On the other hand, studies in Ethiopia (Ayele et al., 2017), and South Africa (Velen et al., 2013) reported a better immunological response in TDF than the AZT group. The possible reason for this difference is likely the initiation of more patients with considerably better health status in the AZT group as compared to the TDF group in the present study. The mortality rate in AZT-based groups (8.86 death per 100 PYR) was higher than in the TDF-based group (5.6 death per 100 PYR) but there was no statistically significant difference in mean time to death between TDF and AZT groups. Similar studies also reported no significant difference among TDF and AZT-based cohorts (Njuguna et al., 2013; Chi et al., 2012; Ayele et al., 2017). Cox regression analysis for predictors of mortality indicated no statistically significant difference in hazard for mortality among TDF and AZT groups. There are inconsistencies among studies on the hazards of mortality among the AZT and TDF-based regimens. Similar to our finding no difference in hazards to mortality was reported by many studies (Bygrave et al., 2011; Chi et al., 2012; Ayele et al., 2017. However, a higher risk of mortality in TDF than the AZT group was reported in Sub-Sahara Africa (Asiimwe et al., 2016), and in Nigeria (Eguzo et al., 2015; Odafe et al., 2012), while another study in South Africa reported a higher risk of mortality in AZT than TDF group (Velen et al., 2013). These inconsistent findings might be due to differences in methods used, socio-demographic factors, and sample size of study populations.
The clear implication of our findings in the Ethiopian HIV/AIDS population is that TDF-based regimen has a superior safety and similar effectiveness compared to AZT-based regimen, which re-enforces WHO recommendations on the use of TDF as preferred first-line ART regimen in resource-limited settings. Our study used cohort study design which is one of the best options to perform comparative observational studies; however, our study has certain limitations due to the retrospective nature of study design and small sample sizes which may affect generalization. Virological outcomes and adherence were not also assessed in this study. Future prospective studies in a large population may be necessary.
CONCLUSION
In our study, the TDF-based regimen has shown lesser toxicity-driven regimen substitution and extended time to toxicity-driven regimen substitution compared to the AZT-based regime. The two regimens did not differ in mortality, and change in CD4 count and hemoglobin at the end of follow up, with the better effect of the TDF group on eGFR at 6 and 12 months of follow up. The results collectively indicate the superiority of safety profiles and comparative effectiveness of the TDF-based regimen which re-enforces the latest WHO recommendation in resource-limited settings that is implemented in Ethiopia.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Arribas JR, Pozniak AL, Gallant JE, Dejesus E, Gazzard B, Campo RE, Chen SS, McColl D, Holmes CB, Enejosa J, Toole JJ CA (2008). Tenofovir disoproxil fumarate, emtricitabine, and efavirenz compared with zidovudine/lamivudine and efavirenz in treatment-naive patients: 144-week analysis. JAIDS Journal of Acquired Immune Deficiency Syndromes 47(1):74-78. |
|
|
Asiimwe SB, Kanyesigye M, Bwana B, Okello S, Muyindike W (2016). Predictors of dropout from care among HIV-infected patients initiating antiretroviral therapy at a public sector HIV treatment clinic in sub-Saharan Africa. BMC Infectious Diseases 16(1):1-10. |
|
|
Ayele T, Jarso H, Mamo G (2017). Immunological outcomes of Tenofovir versus Zidovudine based regimens among people living with HIV / AIDS : a two years retrospective cohort study. AIDS Research and Therapy 14(1)5. |
|
|
Ayele T, Jarso H, Mamo G (2017). Clinical Outcomes of Tenofovir Versus Zidovudine-based Regimens Among People Living with HIV / AIDS : a Two Years Retrospective. Open Aids Journal 11:1-11. |
|
|
Bygrave H, Ford N, Cutsem GV, Hilderbrand K, Jouquet G, Goemaere E (2011). Implementing a tenofovir-based first-line regimen in rural Lesotho, clinical outcomes and toxicities after two years. JAIDS Journal of Acquired Immune Deficiency Syndromes 56(3):e75-e78. |
|
|
Chi BH, Mwango A, Giganti MJ, Sikazwe I, Moyo C, Schuttner L (2012). Comparative outcomes of tenofovir- and zidovudine-based antiretroviral therapy regimens in Lusaka, Zambia. Journal of Acquired Immune Deficiency Syndromes 58(5):475-81. |
|
|
Costarelli S, Cozzi-lepri A, Lapadula G, Bonora S, Madeddu G, Maggiolo F, Antinori A, Galli M, Di Perri G, Viale P (2016). Long-Term Durability of Tenofovir-Based Antiretroviral Therapy in Relation to the Co- Administration of Other Drug Classes in Routine Clinical Practice. PloS ONE 11(10):e0160761. |
|
|
Dadi TL, Kefale AT, Mega TA, Kedir MS, Addo HA, Biru TT (2017). Efficacy and Tolerability of Tenofovir Disoproxil Fumarate Based Regimen as Compared to Zidovudine Based Regimens: A Systematic Review and Meta-Analysis. AIDS Research and Treatment 2017. |
|
|
Eguzo KN, Lawal AK, Umezurike CC, Eseigbe CE (2015). Predictors of Loss to Follow-up Among HIV-infected Patients in a Rural South-Eastern Nigeria Hospital: A 5-year Retrospective Cohort Study. Annals of Medical and Health Sciences Research 5(6):373-378. |
|
|
Ethiopian FMoH (2014). National Guidelines for Comprehensive Hiv Prevention, Care and Treatment. |
|
|
Federal Ministry of Health (FMOH) (2016). Health and Health Related Indicators 2008 EFY (2015/2016). |
|
|
Gallant JE, DeJesus E, Arribas JR, Pozniak AL, Gazzard B, Campo RE, Lu B, McColl D, Chuck S, Enejosa J, Toole JJ (2006). Tenofovir DF Tenofovir DF, Emtricitabine, and Efavirenz vs. Zidovudine, Lamivudine, and Efavirenz for HIV. New England Journal of Medicine 354(3):251-260. |
|
|
Hemasri M, Sudhapoornima P, Sowmya Sri CH, Ramya S, Avinash KKB (2016). Safety and Effectiveness of Anti-Retroviral Drug Regimens Zln and Tle in Tertiary Care Teaching Hospital : A Prospective Observational Study. Journal of Pharmacy and Biological Sciences 11(2):88-96. |
|
|
Horberg M, Tang B, Towner W, Silverberg M, Bersoff-matcha S, Hurley L, Chang J, Blank J, Quesenberry Jr C, Klein D (2010). Impact of Tenofovir on Renal Function in HIV-Infected, Antiretroviral-Naive Patients. JAIDS Journal of Acquired Immune Deficiency Syndromes 53(1):62-69 |
|
|
Medhanie EK, Lukman M, Massi MN, Marianti A (2015). Effectiveness of Tenofovir (TD ) / Emtricitabine (FTC) Versus Zidovudine (AZT) / Lamivudine (3TC) in Combination with Efavirenz (EFV) IN Antiretroviral-Naive HIV-Infected Patients IN Eritrea. International Journal of Pharmaceutical and Clinical Research 7:364-7. |
|
|
Moh R, Danel C, Sorho S, Sauvageot D, Anzian A, Minga A, Gomis OB, Konga C, Inwoley A (2005). Haematological changes in adults receiving a zidovudine-containing HAART regimen in combination with cotrimoxazole in Côte d'Ivoire. Antiviral Therapy 10(5):615-24. |
|
|
Mudzviti T, Mudzongo NT, Gavi S, Chimbetete C (2015). A Time to Event Analysis of Adverse Drug Reactions Due to Tenofovir , Zidovudine and Stavudine in a Cohort of Patients Receiving Antiretroviral Treatment at an Outpatient Clinic in Zimbabwe. Pharmacology and Pharmacy 6(03):201. |
|
|
Njuguna C, Orrell C, Kaplan R, Bekker L, Wood R, Lawn SD (2013). Rates of Switching Antiretroviral Drugs in a Primary Care Service in South Africa before and after Introduction of Tenofovir. PLoS ONE 8(5):e63596. |
|
|
Odafe S, Torpey K, Khamofu H, Ogbanufe O, Oladele EA, Kuti O (2012). The Pattern of Attrition from an Antiretroviral Treatment Program in Nigeria. PLoS ONE 7(12):1-7. |
|
|
Pozniak AL, Gallant JE, DeJesus E, Arribas JR, Gazzard B, Campo RE, Chen SS, McColl D, Enejosa J, Toole JJ CA (2006). Tenofovir disoproxil fumarate, emtricitabine, and efavirenz versus fixed-dose zidovudine/lamivudine and efavirenz in antiretroviral-naive patients: virologic, immunologic, and morphologic changes--a 96-week analysis. JAIDS Journal of Acquired Immune Deficiency Syndromes 43(5):535-540. |
|
|
Subbaraman R, Chaguturu SK, Mayer KH, Flanigan TP KN (2007). Adverse effects of highly active antiretroviral therapy in developing countries. Clinical Infectious Diseases 45(8):1093-1101. |
|
|
Tchetgen EJT, Agbaji OO, Link C, Scarsi KK, Eisen G, Darin KM (2016). Superior Effectiveness of Zidovudine Compared With Tenofovir When Combined With Nevirapine-based Antiretroviral Therapy in a Large Nigerian Cohort The Harvard community has made this article openly Tenofovir When Combined With Nevirapine-based Antiretrovi. Clinical Infectious Diseases 62:512-8. |
|
|
UNAIDS (2019). UNAIDS DATA 2019. |
|
|
Velen K, Lewis JJ, Charalambous S, Grant AD, Churchyard GJ, Hoffmann CJ (2013). Comparison of Tenofovir , Zidovudine , or Stavudine as Part of First-Line Antiretroviral Therapy in a Resource- Limited-Setting : A Cohort Study. PLoS ONE 8(5):4-11. |
|
|
World Health Organization (WHO) (2010). Antiretroviral Therapy For HIV Infection in Adults And Adolescents; Recommendations for a public health approach -2010 revision. World Health Organization. |
|
|
World Health Organization (WHO) (2013). Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV; Infection Recommendations for a Public Health Approach. |
|
|
World Health Organization (WHO) (2016). Consolidated Guiedlines on The Use of Antiretroviral Drugs fro treating and preventing HIV infection: Recommendations for A Public Health Approach. 2nd ed. Genena: WHO. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


