ABSTRACT
The world is making significant progress in reducing the number of women and children dying from preventable causes. Bangladesh is also on track. The objective of this study was to strengthen maternal and child health service delivery in Kapasia and Sreepur Upazila of Gazipur district using SARA tool. The present assessment was a cross-sectional quantitative assessment. This evaluation was performed between January 2015 and December 2015. A sample of 50 health facilities was randomly evaluated. Sixty-two percent of all facilities (n = 50) in the study area were ready to provide general services such as basic services, basic equipment, standard precautions for infection prevention and diagnostic capacity, and essential medicines for patients. The family planning readiness score was 84%, but the antenatal service readiness score was 53% (n = 36). The basic preparation score for emergency obstetric care was 66% among facilities providing delivery services (n = 16). It should be noted that no health center had all the items available for basic obstetric care. Among all health facilities (n = 50), only 28% of health facilities had a full obstetric care service. The child immunization readiness score for Kapasia and Sreepur was 82%; however, only 4% of the facilities had all the trace elements available for child immunization services (n = 36). The total availability of services and the availability of health facilities to provide maternal and child health services did not reach the level necessary to meet future goals. Problems were identified and should be addressed accordingly. A large-scale census survey of all facilities in the study area would provide a better understanding of service availability and readiness.
Key words: Service availability, service readiness, maternal and child health services, Bangladesh health system, SARA tool.
In 2015, there were about 45% of deaths among children under five during their first month of life around the world. 17,000 fewer children die every day from 1990, but still, more than six million children die before their fifth birthday each year. Although, global progress is determined, an increasing proportion of child mortality is found in sub-Saharan Africa and South Asia. Four out of five deaths among children under five occur in these areas. Children born in poverty, almost twice as likely to die before their fifth birthday as children of wealthier families. Children of mothers, including educated mothers with only primary education, are more likely to survive than children of uneducated mothers (Health-United Nations Sustainable Development, 2017). Worldwide, maternal mortality has declined by 50% since 1990. In East Asia, North Africa and South Asia, the maternal mortality rate has declined by two-thirds. But the ratio of maternal mortality, the proportion of mothers who do not survive childbirth compared with those who do - in developing regions is still 14 times higher than in developed regions.
More women receive antenatal care. In developing regions, increased antenatal care rose from 65% in 1990 to 83% in 2012, and only half of women in developing regions receive the amount of recommended medical care they need. Fewer teenagers involve children in most developing regions, but progress has declined. The large increase in contraceptive use in the 1990s did not come together in the 2000s. Slow to meet the need for family planning is greater than the number of women, but demand is growing at a rapid pace (Health-United Nations Sustainable Development, 2017). Women and children around the world die from preventable causes and have declined considerably over the years. In Bangladesh, the maternal mortality ratio (MMR) is 176 deaths per 100,000 live births, which show a decline of 69.1% in 25 years between 1990 and 2015 (WHO, 2015a). Demographic and health data show that neonatal mortality is 28 per 1,000 live births; the infant mortality rate is 38 per 1,000 live births; the under-five mortality rate (U5MR) is 46 per 1,000 live births and the infant mortality rate is 8 per 1,000 children (NIPORT et al., 2015).
In Bangladesh, the infant mortality rate (U5MR) is 38 per 1,000 live births in 2015 and in 1990 it was 144 per 1,000 live births. The annual reduction rate (ARR) is 5.4% (WHO, 2015b). The World Health Organization (WHO) has formed the Committee on Information and Accountability for Women's and Children's Health (COIA) and includes leaders and experts from Member States and multiple agencies and the health of the parties, academia, civil society and the private sector. The committee focuses on the accountability framework, which includes three interrelated processes that oversee, review and act (WHO, 2011). Many countries, including Bangladesh, already have some sort of monitoring system in place. However, most of the monitoring system is not coordinated. Different donors have different monitoring frameworks that create a problem. For this reason, WHO developed a framework for follow-up and review called the Service Availability and Readiness Assessment (SARA) “(WHO/SARA, 2015)”.
Information on the supply and quality of health services is necessary for the management, monitoring and evaluation of health systems. With the increasing demand for accountability and the need to demonstrate results at the national and global levels, information is needed to track how health systems respond to increased inputs and improved processes over time and the impact that such inputs and processes have to improve health outcomes. The basic framework of SARA is to strengthen the common ground for monitoring, evaluation and review of the National Health System. SARA was designed to serve as a systematic tool to support annual data verification and service delivery at the facility level. SARA-based data provide evidence on the progress of the health system to inform the annual health sector review and identify gaps and weaknesses in the sub-optimization of service delivery and intervention coverage that should be addressed and provide a basis for planning and monitoring intervention on the scale and service to improve delivery. In Bangladesh, very few evaluations are still in place to monitor, review and evaluate the delivery of maternal health services for children using the SARA tool. Therefore, the present study aims to enter SARA to improve the monitoring and evaluation of the provision of health services for mothers and children in the rural community of Gazipur district, Bangladesh.
Two Upazila (Kapasia and Sreepur) of Gazipur district was considered as our evaluation area. Kapasia Upazila covers an area of ​​236.75 km2 with a population of 353,160 inhabitants. There are 71,896 households in this Upazila and the population density is 1491 per square kilometre. There are 11 unions in Kapasia Upazila (Local Health Bulletin, 2015). Sreepur Upazila covers an area of 462.00 km2 with a population of 547,795 inhabitants. There are 118,549 households in this Upazila and population density is 1186 per square kilometre. There are 9 unions in Sreepur Upazila (Local Health Bulletin, 2015). This study was a cross-sectional quantitative evaluation. The study was divided into two parts: service availability (SA) and service readiness (SR). This evaluation was carried out between January 1, 2015 and December 31, 2015. Different types of health facilities included in the study were public health facilities: Upazila Health Complex (UHC), Union Sub-centers (USC), Community Clinic (CC) and Private Clinic (PC). At first, the sampling frame of both Upazilas including public and private facilities was carried out.
Stratified random sampling was then performed. This study included private clinics with inpatient and outpatient departments. A total of 50 health centers were visited, of Community Clinic (CC) and Private Clinic (PC). At first, the sampling frame of both Upazilas including public and private facilities was carried out. Stratified random sampling was then performed. This study included private clinics with inpatient and outpatient departments. A total of 50 health centers were visited, of which 25 were from Kapasia and 25 were from Sreepur. 50 of these facilities, there are 2 health complex Upazila, 4 union sub-centers, 30 community clinics and 14 private clinics. The principal investigator along with two research assistants spent a full day evaluating each of the health centers. The administrative head of each health center was interviewed thoroughly. As an example, Upazila Health and Family Planning Officer (UH & FPO) was interviewed at the UHC and the Community Health Services Provider (CHCP) was interviewed at CC. The data were collected during two months from April 1 to May 31, 2015 through a paper based questionnaire.
Data collection technique
Questions related to the various health services were asked in detail when necessary. For example, in the Upazila Health Complex, the EPI technician was asked about the carrier of the vaccine and the temperature control of the refrigerator, while the trader was asked about the availability and depletion of the medications. At the community clinic, CHCP was asked about antenatal care and family welfare assistant (FWA) also asked for information about family planning services. Data collected at community clinics and subcenters were verified at the Upazila Health Complex with a statistician who is responsible for entering data into District Health Information System-2 (DHIS-2) software.
Data entry and quality assurance
Prior to the official data collection, the questionnaire was modified according to the supervisor's direction and the SARA guideline. To ensure the quality of the data, the research team performed a demonstration at the Gazipur Sadar Upazila Health Complex. The data collectors were trained in two phases to ensure the quality of data collection, firstly before the pretest to define and how to use the tools, and secondly, immediately before the main survey on the basis of field experience. The principal investigator re-examines the data at various control points of data collection, data entry, and data cleaning. Data ware entered into Microsoft Excel directly by data collectors after data collection, helping to protect them from error. Coding was performed. All questionnaires were kept in a safe place to ensure confidentiality. Only the principal investigator has access to these questionnaires for cross-checking or validation of the data, if necessary. The data were analyzed using Microsoft Excel, version 2013.
Brief description of assessment tool
SARA is a tool to evaluate health facilities designed to evaluate and monitor the availability of health service and preparedness and generate evidence to support planning and management of the health system. SARA has also been designed to create a systematic set of indicators to track the availability and preparation of the service. The objective of the study was to obtain reliable and regular information on service delivery such as availability of human resources and basic infrastructure, availability of basic equipment, basic facilities, essential medicines, diagnostic capabilities and specific health services like basic health care interventions, family planning, child health services, basic and comprehensive emergency obstetric care. For the evaluation of the facilities, a modified version of the WHO recommended SARA tool was used.
The SARA survey is designed to generate a set of basic indicators on key inputs and outputs of the health system that can be used to measure progress in strengthening the health system over time. The tracer indicators are intended to provide objective information on whether or not an installation meets the conditions required to support the provision of basic or specific services with a consistent level of quality and quantity. Summary or composite indicators, also called indexes, can be used to summarize and communicate information on multiple indicators and indicator domains. Indexes can be used for general availability and service-specific availability. The general services include basic services, basic equipment, standard precautions for infection prevention, diagnostic capacity and essential drugs. The tracer indicators for basic services are the energy source, improved water source within 500 m of the facility, consultation room with auditory and visual privacy for patient consultations, access to adequate sanitation facilities for clients, communication equipment (Telephone/Mobile phone or SW radio), internet access and emergency transport.
Plotter indicators for basic equipment are adult scale, child scale, thermometer, stethoscope, blood pressure apparatus and light source. The follow-up indicators for standard precautions for infection prevention are the safe final disposal of sharps, safe final disposal of infectious waste, appropriate storage of sharp residues, adequate storage of infectious waste, disinfectant, single use-disposable or disposable syringes water or alcohol-based hand rub, latex gloves and guidelines for standard precautions. The traceability indicators for the diagnostic capacity are hemoglobin, glycaemia, diagnostic ability of malaria, urine dipstick-glucose, the diagnostic capacity of HIV, rapid syphilis test and urine test for pregnancy. Follow-up indicators for essential drugs are amitriptyline compressed, amoxicillin suspension, amoxicillin tablets, ampicillin injection, gentamicin injection, ceftriaxone injection, salbutamol inhaler, beclomethasone inhaler, enalapril tablet or alternative ACE inhibitor, glibenclamide tablet, metformin tablet, regular insulin, omeprazole or alternative tablet, oral rehydration solution, paracetamol tablet, zinc sulfate tablet, ibuprofen tablet and fluoxetine tablet.
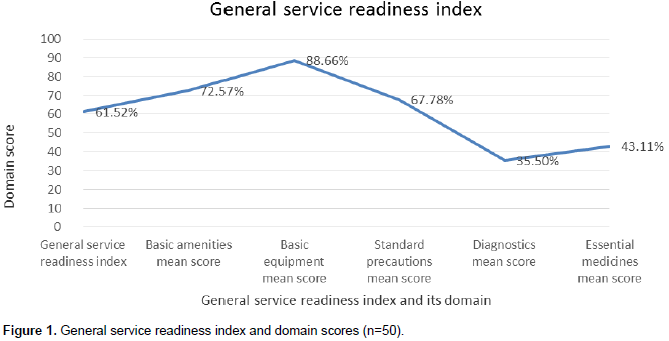
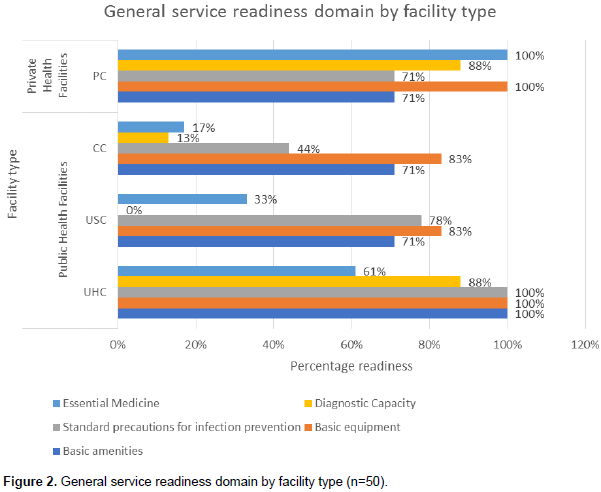
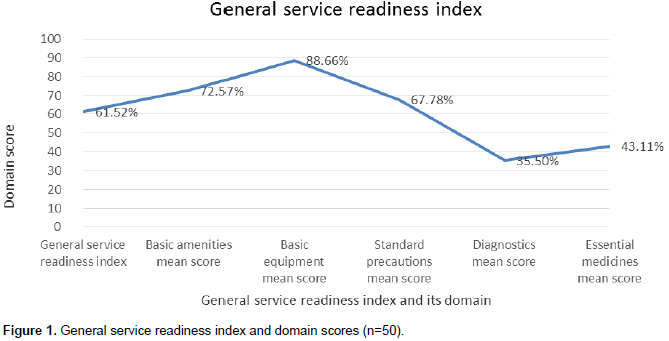
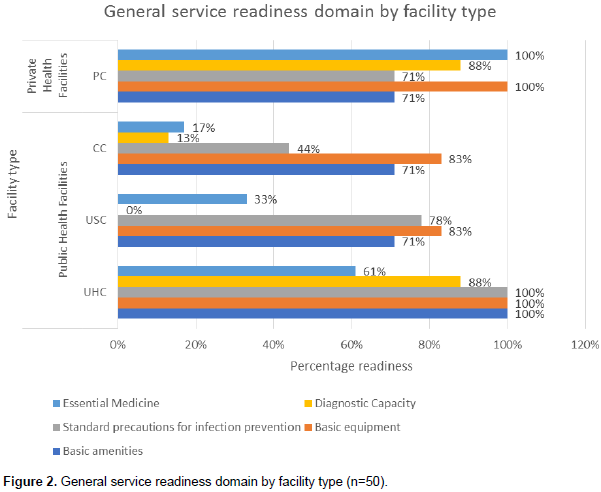
The general service readiness index for Kapasia and Sreepur Upazila was 62% where the highest contributor was basic equipment domain (89%) and the lowest was the diagnostic capacity (36%) of all health facilities (Figure 1). Tracer items for essential medicines were the lowest in CC (17%). USC was not yet ready for providing any diagnostic test (0%) (Figure 2). Specific services include family planning services, antenatal care services, basic obstetric care services, comprehensive obstetric care services, child immunization services, and preventive and curative care services for children. Follow-up indicators for the availability of family planning services are combined oral contraceptive pills, progestin contraceptive pills, combined injectable contraceptives, combined progestin-injectable contraceptives, intrauterine contraceptive device implants, cycle beads for the standard day method, emergency contraceptive pills, male sterilization, female sterilization, male condoms and female condoms.
Follow-up indicators for the preparation of family planning services are trained personnel and guidelines on family planning, trained family planning personnel in the last two years; blood pressure equipment and apparatus; medications and commodities-combined oral contraceptive pills, injectable contraceptives and condoms. The follow-up indicators for the availability of antenatal care services are iron supplementation, folic acid supplementation, intermittent preventive treatment (IPT) for malaria, tetanus toxoid vaccination, monitoring of hypertensive pregnancy disorder and supply of misoprostol tablets for births at home. The follow-up indicators for the preparation of prenatal care services are guidelines on antenatal care (ANC), staff trained in the ANC in the last two years; equipment-blood pressure apparatus; diagnosis: hemoglobin, urine strip protein; medicines and commodities-iron pills, folic acid tablets. Tracer indicators for the availability of basic obstetric care services are the parenteral administration of antibiotics, parenteral administration of oxytocin, parenteral administration of anticonvulsants, and assisted vaginal delivery.
Follow-up indicators for the preparation of basic obstetric care services are trained personnel and guidelines for the integrated management of pregnancy and childbirth (IMPAC), staff trained in IMPAC in the last two years; emergency transport equipment, sterilization equipment, examination light, delivery container, suction device (mucus extractor), manual vacuum extractor, vacuum cleaner or D & C kit, neonatal bag and mask, delivery bed, partograph, gloves, blood pressure apparatus; medications and commodities: antibiotic ointment for the newborn, uterotonic injectable, injectable antibiotic, magnesium sulfate (injectable), diazepam (injectable), skin disinfectant, infusion intravenous solution. Follow-up indicators for the full availability of obstetric care services are the cesarean section, blood transfusion, and basic emergency obstetric care. The follow-up indicators for the preparation of comprehensive obstetric care services are CEmOC guidelines, CEmOC trained personnel, trained personnel in surgery, trained personnel in anesthesia; equipment-anesthesia equipment, incubator; diagnosis-blood test, cross-matching test; medicines and commodities: sufficiency of blood supply, the safety of blood supply.
Indicators for monitoring the availability of child immunization services are routine infant immunization services, routine measles immunization, Routine DPT-Hib-HepB immunization, routine polio vaccination, BCG vaccination, rotavirus immunization and immunization against pneumococcus. Follow-up indicators for the preparation of child immunization services trained staff and guidelines: guidelines for EPI, EPI trained personnel; Equipment- cold box/vaccine carrier with ice packs, refrigerator, sharps container, single use of syringes, vaccination cards; medicines and commodities-measles vaccine, DPT-Hib + HepB vaccine, polio vaccine, BCG vaccine. Indicators for monitoring the availability of preventive and curative care services for children are curative care for children under 5 years of age, diagnosis and treatment of malnutrition, vitamin A supplements, iron supplements, ORS and zinc supplements, growth monitoring and treatment of pneumonia. Follow-up indicators for the preparation of preventive and curative health services for children's health are: trained staff and guidelines: guidelines for IMCI, guidelines for growth monitoring, staff trained in IMCI, trained personnel in monitoring growth; equipment-children's and children's scale, length/height measuring equipment, thermometer, stethoscope, growth chart; diagnosis: hemoglobin (Hb), fecal test parasite (general microscopy), diagnostic capacity of malaria; medications and commodities-oral rehydration solution pack, amoxicillin dispersible tablet or syrup, co-trimoxazole syrup/suspension, paracetamol syrup, vitamin A capsules, mebendazole/albendazole tablet, zinc sulfate tablet or syrup.
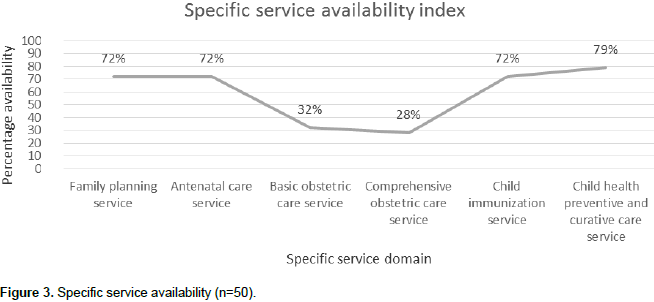
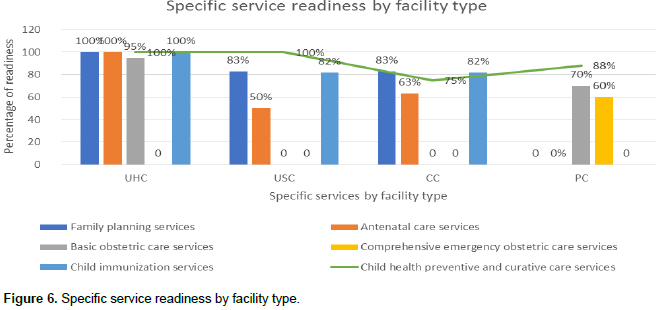
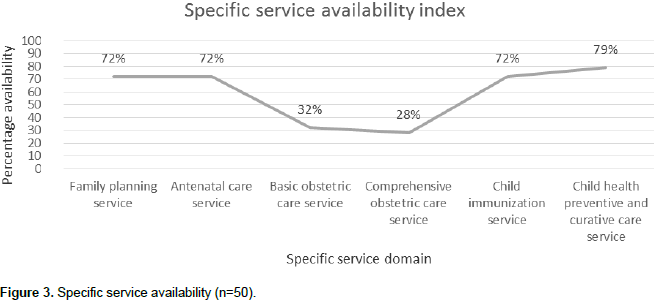
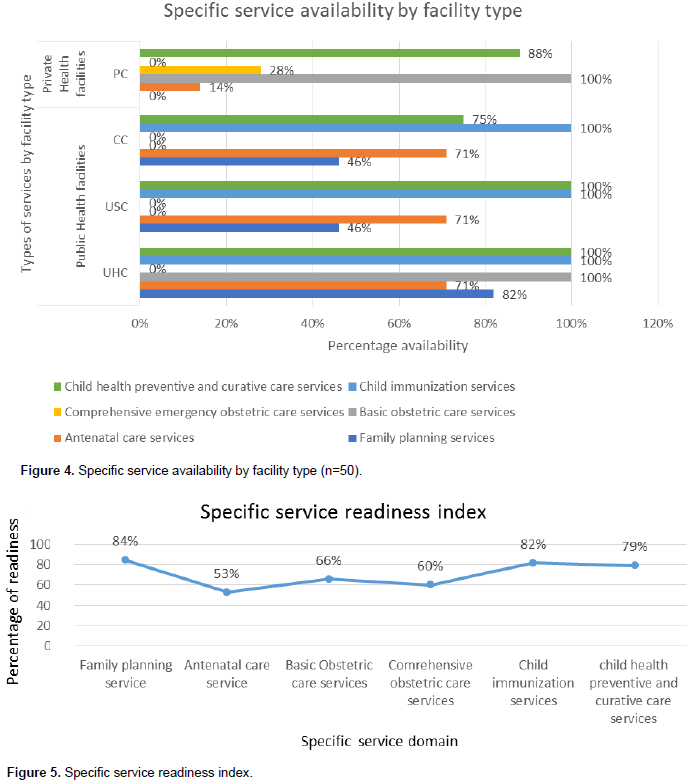
The line graph shows that only 28% health facility had available comprehensive emergency obstetric care service. Highest service available for child health preventive and curative care (79%) (Figure 3). Public health facilities were not yet to be available for comprehensive emergency obstetric care services. On the other hand, private health facilities had no family planning and child immunization services (Figure 4). Among the facilities offering maternal and child health services, family planning service readiness score was 84%, child immunization service readiness score was 82%, child health preventive and curative care service readiness score was 79%, basic emergency obstetric care service readiness score was 66%, comprehensive obstetric care service readiness score was 60%, but antenatal care service readiness score (53%) was the lowest among specific service readiness domain (Figure 5). In case of antenatal care services, though 14% private health facilities had available this services, but they were not yet to ready for providing that services (Figure 6).

For the facility readiness assessment, the 73% basic service domain score indicates that approximately two-thirds of the facilities in the study area had basic amenities including adequate sanitation facilities, privacy room, source of improved water, and 64% had a computer with internet, only 40% (2 UHC, 4 USC and 14 Private Hospitals) had an adequate power source to use them correctly. The overall basic equipment proficiency score of 89% indicates that most health facilities had the necessary equipment to provide services to people. However, using of that equipment was not seen by the study team while health care providers were observed when patients came to look for any service. Only 4% of Kapasia and Sreepur facilities had guidelines that are necessary for standard precautions for infection prevention. This is reflected in their daily practice as well. Although almost 92% of the facilities had adequate storage of infectious and wastes, many said they sent their used needle to the Upazila Health Complex for final disposal. The overall 43% score for essential medicine indicates that in the current area 43% of facilities had essential drugs. But it is alarming that only 28% had all the essential drugs available at the time of this evaluation.
The reason for this shortage was the inadequate supply of medicines by a quarter. At each community clinic in Kapasia Upazila, there was no supply of any medication during the last three months. However, in some cases, the unnecessary use of medicine by patients can also cause shortages of medications. The patient was happy to receive treatment and the community clinic was known to all people in the community (Karim et al., 2015). CHCP failed to properly answer how many drops make a milliliter (field observation). The 62% overall service readiness index score refers to the fact that 62% of all facilities in the study area were ready to provide general services such as basic services, basic equipment, standard precautions for infection prevention and diagnostic capacity and essential medicines to the patients. As only 2 UHC and few private hospital had the diagnostic capability and all basic services, the overall percentage became low.
Family planning readiness score of 84% indicates that almost the facilities had family planning services available (Taylor et al., 1974).
The percentage of facilities with all items was very low that is only 6% because we were considering all the services including IUD, implant, sterilization whereas only at UHC all these services were available. But most of our facilities include community clinics where only male condom and pill was available. Child health immunization readiness score was 82%. Child health preventive and curative care readiness score of 79% indicate that majority of the child got basic preventive care from the facilities. It might contribute to the reduction of child mortality and morbidity of the study area. Though antenatal care service availability score was 72% but readiness score was 53%. Antenatal care service is essential for safe pregnancy outcome (Pervin et al., 2012). No comprehensive emergency obstetric care services were available in any public health facilities. Though in Upazila health complex there were all facilities available for conducting caesarean section except anesthesia facilities. Different countries in the world like Uganda, Tanzania, Sierra Leone, Zambia, Togo, Niger, Mauritania, Kenya, the Democratic Republic of the Congo, Burkina Faso, and Benin have already adopted SARA tool in their health statistics and information systems.
Though health facilities survey was conducted in Bangladesh (NIPORT et al., 2016), but this study gives a different dimension emphasizing rural health facilities regarding MCH services considering global standard. They have to ensure safe motherhood (Ahmed et al., 2012; Rahman et al., 2011; Baqui et al., 1998; Haque et al., 1997). They have achieved MDG 4 within last 25 years. Though, baseline data were very high in comparison to current status. It is undoubtedly a great achievement. But it is quite low in comparison to developed countries. It was the first step. It was very much quantitative rather qualitative improvement. But to reach the future targets, SDG need more emphasis on qualitative improvement, because resources are always limited. It is very much true in case of our developing country, Bangladesh. Our journey is 30 years long journey.
They have the budgetary constraint, lack of proper implementation of health policy and in need, but have to go a long distance to achieve our targets. So our monitoring system, should be strengthen with proper utilization of limited resources. There were some limitations in the evaluation tool. This tool was not validated in our country. Since a sample of health centers in the study area was selected instead of a census of all facilities, the service availability data may not give an accurate measurement. There is need to face some challenges while conducting the evaluation. Some community clinics and union sub-centers are located in areas of difficult access where transportation was not available and the communication system was very poor. Managing time was a tough job because government facilities work until 2.30 p.m.
The overall availability of services and the readiness of health facilities to provide maternal and child health services did not reach the goal needed to meet future goals. But at the same time, people in the community were also aware of the available services related to maternal and child health services. Therefore, if quality care were maintained it would be fruitful. Problems were identified and should be addressed accordingly. A large-scale census survey of all facilities in the study area would give a better understanding of service availability and readiness. Treatment should be managed by at least one primary care physician at all levels. Community clinics should be strengthened. Safe home delivery practices can be initiated from community clinics. These may be a better preventive care center. The anesthesiologist must be available at public health facilities at least Upazila health complex. The results shall contribute significantly to the overall improvement in maternal and child health not only in Bangladesh, but also on the global platform. Finally, all these efforts will serve as a catalyst for better health for the future Bangladesh that achieves the goal of sustainable development.
The authors have not declared any conflict of interests.
The authors are grateful to Dr. Sharmin Parveen, head of the Department of Health Informatics at the Bangladesh University of Health Sciences in Bangladesh.
REFERENCES
|
Ahmed T, Mahfuz M, Ireen S, Ahmed AS, Rahman S, Islam MM, Alam N, Hossain MI, Rahman SM, Ali MM, Choudhury FP (2012). Nutrition of children and women in Bangladesh: trends and directions for the future. J. Health Popul. Nutr. 30(1):1-11.
Crossref
|
|
|
|
Baqui AH, Black RE, Arifeen SE, Hill K, Mitra AN, Sabir AA (1998). Causes of childhood deaths in Bangladesh: results of a nationwide verbal autopsy study. Bull. World Health Organ. 76(2):161-171.
|
|
|
|
|
Haque ZA, Leppard M, Mvalanker D, Akhter HH, Chowdhury TA (1997). Safe motherhood programme in Bangladesh. Dhaka: Ministry of Health and Family Welfare, USAID, World Bank and CIDA.
|
|
|
|
|
Health-United Nations Sustainable Development (2017). Goal 3: Ensure healthy lives and promote well-being for all at all ages. Available at:
View.
|
|
|
|
|
Health Bulletin (2015). Management Information System (MIS). Directorate General of Health Service (DGHS). Ministry of Health and Family Welfare (MOHFW).
|
|
|
|
|
Karim RM, Abdullah MS, Rahman AM, Alam AM (2016). Identifying role of perceived quality and satisfaction on the utilization status of the community clinic services; Bangladesh context. Bangl. Med. Res. Counc. Bull. 41(1):1-12.
Crossref
|
|
|
|
|
Local Health Bulletin (2015). Kapasia Upazila Health Complex. Management Information System (MIS). Directorate General of Health Service (DGHS). Ministry of Health and Family Welfare (MOHFW).
|
|
|
|
|
Local Health Bulletin (2015). Sreepur Upazila Health Complex. Management Information System (MIS). Directorate General of Health Service (DGHS). Ministry of Health and Family Welfare (MOHFW).
|
|
|
|
|
National Institute of Population Research and Training (NIPORT), Mitra and Associates, and ICF International (2015). Bangladesh Demographic and Health Survey 2014: Key Indicators. Dhaka, Bangladesh, and Rockville, Maryland, USA: NIPORT, Mitra and Associates, and ICF International.
|
|
|
|
|
National Institute of Population Research and Training (NIPORT), MEASURE Evaluation, and icddr,b. (2012). Bangladesh Maternal Mortality and Health Care Survey 2010. Dhaka, Bangladesh: NIPORT, MEASURE Evaluation, and icddr,b.
|
|
|
|
|
National Institute of Population Research and Training (NIPORT), Associates for Community and Population Research (ACPR), and ICF International (2016). Bangladesh Health Facility Survey 2014. Dhaka, Bangladesh: NIPORT, ACPR, and ICF International.
|
|
|
|
|
Pervin J, Moran A, Rahman M, Razzaque A, Sibley L, Streatfield PK, Reichenbach LJ, Koblinsky M, Hruschka D, Rahman A (2012). Association of antenatal care with facility delivery and perinatal survival - a population-based study in Bangladesh. BMC Preg. Childbirth 12:111.
Crossref
|
|
|
|
|
Rahman A, Moran A, Pervin J, Rahman A, Rahman M, Yeasmin S, Begum H, Rashid H, Yunus M, Hruschka D, Arifeen S.E, Streatfield PK, Sibley L, Bhuiya A, Koblinsky M (2011). Effectiveness of an integrated approach to reduce perinatal mortality: recent experiences from Matlab, Bangladesh. BMC Publ. Health 11:914.
Crossref
|
|
|
|
|
Taylor HCJ, Rosenfield AG (1974). A family planning program based on maternal and child health services. Am. J. Obstet. Gynecol. 120:733-745.
Crossref
|
|
|
|
|
World Health Organization (WHO) (2011). Keeping promises, measuring results: Commission on information and accountability for Women's and Children's Health.
|
|
|
|
|
World Health Organization (WHO) (2015a). Levels and Trends in Child Mortality: 1990-2015: estimates from WHO, UNICEF, UN, World Bank Group and the United Nations Population Division.
|
|
|
|
|
World Health Organization (WHO) (2015b). Trends in maternal mortality: 1990-2015: estimates from WHO, UNICEF, UN, World Bank Group and the United Nations Population Division.
|
|
|
|
|
World Health Organization (WHO) /Service Availability and Readiness Assessment (SARA) (2015). An annual monitoring system for service delivery Reference Manual, Version 2.2. Health Statistics and Information Systems, WHO. Available at:
View
|
|