Full Length Research Paper

ABSTRACT
HIV remains a major public health problem in Sub-Saharan Africa. About 54.5% of all people living with HIV live in Eastern and Southern Africa. There is no HIV vaccine or cure available yet despite ongoing research to develop one and uptake of vaccines is critical in the global society. It is imperative to describe the perceptions and experiences of the vaccines trial participants, as they may give lessons for COVID-19 vaccine development. A phenomenological qualitative study was conducted to describe the experiences of volunteers who participated in a phase I/II HIV vaccine trial in Tanzania. A purposive sample of 20 of the 60 trial participants was interviewed. Interviews were subjected to thematic-content analysis. The study showed that trial participation was driven by positive expectations related to health and the realization of the need for an effective vaccine to combat HIV. However, fear and concerns about the safety of the trial vaccine were the frequently reported challenges to participation. The significant others and community play an important role in trial participation. The success of a trial depends on direct and indirect participation in trials. Future vaccine trials must promote positive expectations for trial participation and address fears and concerns related to vaccine safety.
Key words: HIV Vaccine trial, participant experiences, COVID-19 vaccine trial, trial benefits and challenges, Tanzania.
INTRODUCTION
HIV pandemic and vaccine development
Since the start of the HIV epidemic, 75.7 million people were infected by the disease globally and in 2019 alone 690 000 lives were lost to HIV (Communications and As people were living with HIV including 1.7 million who were infected in that year alone (UNAIDS, 2020). More than half (54.5%) of all people living with HIV (PLHIV) live Global Advocacy UNAIDS, 2020) of 2019 38.0 million in Eastern and Southern Africa where 700,000 new infections were reported in 2019 (UNAIDS, 2020). In Tanzania, an estimated 1.6 million PLHIV are representing an adult prevalence rate of 4.6%; with 72,000 new infections and 24,000 AIDS-related deaths in 2018(UNAIDS, 2019).
This suggests that a vaccine is needed to avoid further loss of lives since vaccines offer the most cost-effective mechanism to tackle infectious diseases (Pronker et al., 2013). While on average it takes 10.7 years to develop a vaccine it is now decades before an HIV vaccine is found (Pronker et al., 2013). Previous trials such as one conducted in Thailand found 31.2% efficacy brought promises for an effective vaccine although more work is still needed (Koff, 2012). Various social determinants of the willingness to participate including lack of knowledge, hesitance, fear of side effects, perceived risks and benefits of participation were reported as key socio-challenges as key socio-challenges (Detoc et al., 2020; Doshi et al., 2017; Mbunda et al., 2014).
Participants join vaccine trials both for altruistic and non-altruistic motives while safety, fear of being vaccinated with a live and actual HIV vaccine have been reported as barriers and concerns for trial participation in Africa (Chin et al., 2016; Opeyemi et al., 2017; Tarimo et al., 2016). Ongoing and new studies need to consider addressing these and other challenges in vaccine development efforts.
HIV vaccine development lessons for COVID-19 trials
As of 29 July 2020, there were 16,558,289 confirmed cases of corona virus. There were also 656,093 confirmed deaths from COVID-19 in the world since January 2020 when the first cases of corona virus were confirmed outside of China (WHO, 2020). In Tanzania, the first confirmed case from COVID- 19 was in March 2020 (Tarimo et al., 2016). Scholars have linked the COVID-19 pandemic to the HIV pandemic in several ways including its devastating effects, high death rates and the lack of a vaccine or cure (Chenneville et al., 2020; Hargreaves et al., 2020). Therefore the lessons learnt from HIV vaccine development may be crucial in the development of a COVID-19 vaccine. As with the willingness to participate in HIV vaccine trials, close to two-thirds of research participants expressed willingness to participate in COVID-19 vaccine trials (Lin et al., 2020). As in HIV vaccine trials, concerns in COVID-19 vaccine trials have been cited as individual safety, infection, and family members’ concerns (Lin et al., 2020). As of 20 April 2020 there were five COVID-19 vaccine trials at the clinical stage and 71 trials at the exploratory or preclinical evaluation stage (Thanh Le et al., 2020). The scientific community is required to urgently develop a COVID-19 vaccine to stop the high morbidity and mortality (Lurie et al., 2020). However, the COVID-19 vaccine development urgency must derive benefits from the history of HIV vaccine trials such as knowledge, expectations, views and experiences of participants.
The case of Tanzania’s HIV vaccine development
In 2005 the Tanzanian Ministry of Health established and designated the National Institute for Medical Research- Mbeya Centre, to conduct HIV vaccine trials in Tanzania. Although the site had experience in conducting other clinical studies since 1996, it recognized enormous challenges in the recruitment and retention of HIV vaccine trial participants. One of the studies in Tanzania showed about 50% of the potential eligible volunteers expressed willingness to participate in HIV vaccine trials. This raised the need to conduct an exploratory sub-study to understand the experiences and challenges encountered by the study participants at the clinic and in the community (Mbunda et al., 2014). We adopted an ecological framework to explore the possible factors influencing participants’ expectations, views and experiences at the individual, family, health system and community levels. We believe the findings may be helpful in research to develop a vaccine for a similarly infectious disease, COVID-19. Tanzania has adopted complementary traditional therapies including steaming, using medicinal herbs believed to boost immunity and prevent COVID-19 severity (Kamazima et al., 2020; Mfinanga et al., 2021). This was recommended to be used alongside the modern disease management practices for COVID -19 (Kamazima et al., 2020; Mfinanga et al., 2021). Our study aimed to explore and describe the expectations or motivation for participating in the HIV vaccine trial, to understand the experiences and challenges encountered by respondents during participation in the HIV trial and discuss their relevance for COVID-19 vaccine development.
MATERIALS AND METHODS
Study setting
The study was conducted in the Mbeya region which has a population of 2,707,410 (National Bureau Statistics, 2013). In the study conducted in 2002-2003, HIV prevalence was 16.6% and an incidence of 7% in females and 5% in males at the time of the vaccine launch (Arroyo et al., 2005)however, the prevalence has decreased to 9.3% in 2012 (THIS, 2017).
Vaccine trial
The first vaccine trial conducted by the Mbeya Medical Research Centre was “A phase I/II double-blinded, randomized placebo-controlled clinical trial to evaluate the safety and immunogenicity of a multiclade HIV-1 DNA plasmid vaccine (VRC-HIVDNA016-00-VP) boosted by a multiclade HIV-1 recombinant adenovirus-5 vector vaccine (VRC-HIVADV014-00-VP) in HIV uninfected adult volunteers in East Africa” (RV 172 Protocol, 2004). This was part of a multicenter trial with other research centres in Kenya and Uganda. The trial was sponsored by the U.S. Military HIV Research Program (USMHRP) and it started in July 2006 and was completed in 2008. The data collection for this study was conducted between February and August 2009, the participants were still followed up for safety and immunogenicity.
The recruitment of participants for the vaccine trial involved inviting surrounding communities to the research centre to attend information seminars. The seminars briefed potential participants about the aim and objectives of the study, duration and eligibility criteria. Interested volunteers were registered to attend further briefing sessions where detailed information about the study including the number of visits, number of vaccinations, blood draw, HIV counselling and testing and medical examination were given. The trial involved inoculation of the candidate vaccine (Investigational product) into the participants and subsequent following up and monitoring of participants for immunogenic changes.
Study design and sampling
This was a descriptive qualitative sub-study of the HIV vaccine trial. The sub-study was underpinned by a phenomenological approach to describe the experiences of volunteers who participated in an HIV vaccine trial at Mbeya Medical Research Centre in their natural setting. This method was crucial to understanding participants’ opinions, feelings and experiences and interpreting the meaning of these experiences from the people exposed to the phenomenon (Greenhalgh and Taylor, 1997). Purposive sampling was used to select 20 of the 60 trial participants to obtain participants across diverse demographic backgrounds and those who faced different challenges during the trial. The selection procedure followed the trial enrolments register and followed up trial participation reports. Participants recruited were both males and females of different ages (19-49 years), education levels, marital status and location. The sample also included participants who experienced family and community challenges in recruitment and participation and those who did not report these challenges.
Data collection
A data collection semi-structured tool was developed with guiding questions covering participant expectations and experiences in participation. Investigators explained the study to potential respondents and those interested signed the informed consent forms before the interviews commenced. The first author conducted in-depth interviews (IDIs). Probing allowed interviews to clarify any issues and also get new information. Issues raised in one interview were also given an opportunity for verification, confirmation or rebuttal as appropriate in successive interviews. The guide focused on the lived experiences of the respondents as participants in the trial. All interviews were conducted in private and quiet rooms. The interviews were conducted in Kiswahili, Tanzania’s national language and were audio-recorded with the permission of the participants. Data were transcribed verbatim and then translated back from Kiswahili to English. The transcribed and translated interview data were subjected to cleaning and accuracy confirmation before analysis. This involved an independent transcriber randomly selecting and examining three transcripts and finally comparing them with the original script to identify and edit any deviations.
Data analysis
Data were analyzed using thematic-content analysis. The analysis of data started with ordering data into codes which were then ordered into categories. We had pre-selected themes, but these were refined and new ones emerged as data showed different twists. Categories of data formed a theme that either fit into a pre-defined theme or a new theme if this did not fall into the pre-selected themes. In most cases, a theme would be confirmed or developed with at least half the participants subscribing to it. However, the level of detail thick descriptions and experiences were considered in determining whether the subject made a theme or not. The researchers discussed these to confirm alignment or divergence (Tong et al., 2007). Through an iterative constant comparison approach (Braun and Clarke, 2006; Fereday, 2006), the researchers analyzed the data and resolved any disagreements by mutually agreeing.
Ethical considerations
The study received ethics clearance from the Mbeya Regional Medical Research Ethics Committee (MMREC), Reference number MRH/E.10/10/2 and the permission to conduct the study was obtained from the local authorities at Mbeya Medical Research Centre. All study procedures were performed in accordance with the relevant guidelines and regulations in human subject research.
RESULTS
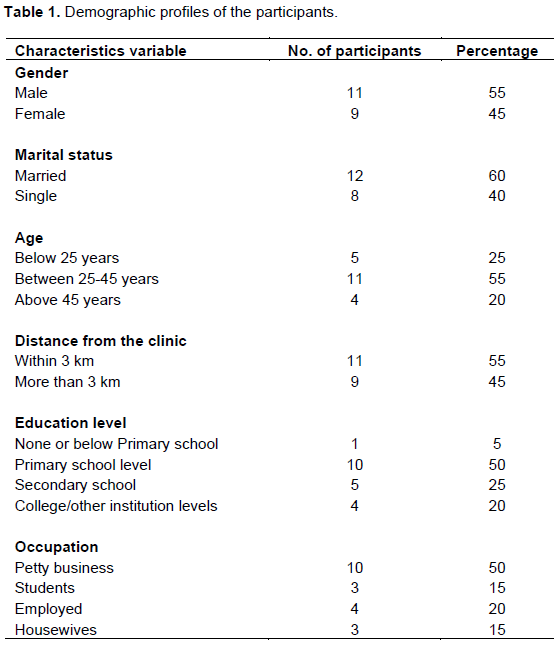
Five themes related to expectation and experiences in HIV vaccine trial participation were found and categorized into the following sub-headings: 1) Expectation and motivation to participate; 2) Individual and Public health benefits to participants; 3) Safety of the vaccine; 4) Experiences with clinical procedures; 5) Experiences in the family and community. We present each theme below. Table 1 shows the demographic characteristics of the participants of the 20 participants 11 were males 12 were married, 5 were adolescents, 11 participants were between 25 and 45 years and only 5 participants had tertiary education.
Expectation and motivation
Some of the respondents, who thought they were at risk of acquiring HIV, believed that they will be protected from HIV infection. This is despite them not being aware if they were receiving a real vaccine or a placebo. A 25-year-old single female’s assertion illustrates that:
“I believe the vaccine must have some protective effect” and a 24 years old male college student said, “...if we were allowed to choose I wanted to get the real vaccine… I know it will add some immunity in the body…”. A 45-year-old married woman who did not have health insurance asserted; “My biggest motivation was free medical health care…”
This illustrates that participants may have joined the study with the hope that if they were in the vaccine arm, they would be protected against HIV infection.
Individual and public health benefits to participants
Participants’ participation was driven by positive expectations related to health such as the need to conduct HIV testing. The study offered free HIV testing and through this, participants had an opportunity to know their HIV status and receive free medical care as part of the benefits of participating in the study. Respondents appreciated the safety measures are taken, the follow-up and health care services being provided by the research team when the participants fell sick. For instance, a 49-year-old married father of three who lived on a shoe shining business had some serious health problems for which the study team provided the necessary medical care that he appreciated. He said:
If I were not a participant in [the] research centre I would
have been dead by now because with that sickness (seizures due to an infection in the brain), I would not have that amount of money needed to go to Dar-es-Salaam for treatment, but with the support of [the] research centre, look at me as you can see, I am healthy and feeling good again.
A 45-year married man explains “…the care we are getting here is not available in the public hospitals… so I see it as a big advantage for my being in the study”.
Some participants joined the study with a motive to be part of the world’s efforts in finding an effective vaccine for HIV which they viewed as beneficial to the future generation. “…I thought if the vaccine will be successful it will benefit me and if not me then my children or grandchildren” [Female, 45 years]. Another participant said, “HIV is a difficult disease …. other prevention methods have failed… people are still acquiring the disease… if we get the vaccine it will be the solution to stop the spread of HIV” [Male 44 years, area leader].
Safety of the vaccine
Despite the positive motivations described above, most participants had concerns about the safety of the vaccine that was being tested. Participants believed that all vaccines contained some formations of the virus or bacteria in question that would potentially infect them. A 44-year-old married man who was an area leader remarked,
We used to know that vaccines are made from the bacteria or the virus responsible for the disease intended to be prevented… so we thought the same applies to [the] HIV vaccine…but the doctors explain[ed] everything.
This concern was raised by many participants in the consultation meetings to the extent that the trial management officers realized the need to clarify which they did. Most respondents did not experience any serious side effects from the vaccination, apart from mild headache and pain at the site of injection, for example, a 40-year-old female vendor remarked; “….I did not feel anything apart from mild pain at the site of injection”. A 42-year-old housewife stated that “…It was nothing serious ….I had a headache ….it lasted for like four hours… that was all”.
Participants had different perceptions regarding vaccine-induced positivity (the false positive); many did not have problems with this situation while a few were concerned. A 31-year-old female secretary explained, “… I thought it was just fine, so long as it is not a real infection”. Others felt that there was something hidden behind this positivity. For example, a 24-year-old young man said; “False-positive mmh! … you never know…honestly, I was worried …three months after the vaccination I went to a VCT centre to test my blood, just to check if I will test positive or not”.
Experiences with clinical procedures
The time spent at the clinic to complete all procedures in a visit was described as “too long”, especially in the initial visits. Participants had to go through the consenting process, medical examination and the counselling procedures. Normally participants would take about 6-8 hours to complete all procedures on the first day. A 45-year-old man raised the following complaint; “…waiting time was too long in some of the visits, like in one visit I remember coming at 08:00… and I left the clinic at 15:30…”
Participants felt that the amount of time the trial was taking unfairly competed with their work demands as a working male remarked, “…this is not convenient for someone who is employed”. Although some felt it was okay as one young man, a labourer observed: “…Initially, appointments were like too long…though not to the level of inconveniencing my duties…”.
For participants living close to the clinic and were self-employed people who could structure their work activities alongside trial visits, there was no concern with time. A 33-year-old entrepreneur/business owner remarked… “It was fine with me… I just live behind the clinic and am not so busy in most of the mornings”.
A few participants expressed concerns with the amount of blood drawn for laboratory tests. A 34-year-old woman vending food expressed “… The blood taken is too much …what if someone has low levels of blood”! (The blood drawn per visit was about 140-150 mls); these concerns from participants illustrate participants’ challenges with the clinical aspects of the procedures that required clear explanations. Many participants addressed their fears and concerns by using information they recalled from the information sessions.
One of the challenges reported was the timing of trial visits. Morning visits for scheduled procedures were challenging for people who were employed and students. A 24 years old college student reported the timing challenge:
“…my appointments were mostly on Monday or Tuesday, these days we are busy at the college… so I would come late to the clinic… or choose to miss some sessions…”
Participants mentioned that it was challenging to participate and remain in the study until the end, due to the rumours and misconceptions in the community about the vaccine.
“We were so much insulted by our neighbours...they said to us… You are even told not to become pregnant…but you are still blind … actually, it needed one to be strong to stay in the study to the end”. [Female 27 years]
Experiences in the family and community
Participants reported having difficult times with their spouses, families and friends as there was a stigma attached to participating in the trial. Participants’ significant others questioned why the trial was being conducted in Africa with some comparing participants with sacrificed guinea pigs. A 23-year-old single lady reported that:
Friends and neighbours said we are being injected with HIV, we will soon fall sick, we are very stupid to involve ourselves in something very risky, why are the whites (the people sponsoring the trial) not conducting this trial in their own countries! They are coming to Africa to kill us…”
In some couples where one participated whilst the other partner did not, it led them into serious problems in their marriages. A married 38-year-old male participant who was a vendor explained that;
My wife and I had a serious quarrel about my participation in this trial, especially after hearing the rumours concerning the vaccine; she would not allow me to touch her (have sex with her) because she thought I am already infected by the virus from the vaccine… The PI explained to us and together we went through the informed consent form…. she understood and things went back to normal. But I tell you it was very tough at home… (laughter).
Some respondents pointed out that they did not care much about what other people thought or said, as long as their spouses supported them in participating in the trial. A 28-year-old man, a taxi driver explained:
“My wife and relatives had no problems because they know and trust me that, I would not put myself in danger … that was all that mattered to me; other people were just talking… I just ignored them”
DISCUSSION
The study explored the expectations and experiences of HIV vaccine trial participants. Five themes emerged around positive and negative trial expectations, trial public health benefits to participants, safety issues and the impact of clinical procedures on participants’ routine lives. We interpret the findings in terms of the on-going HIV vaccine development and draw lessons for COVID-19 vaccine trial development. The findings help in understanding participants as vital contributors to vaccine development. We found that the success of a trial depends on not only participants but also significant others. This demonstrates that the success of any vaccine trial is not solely on the drug but on a holistic consideration of participants, community members and collaborators. We learnt that vaccine trial development has multiple players who influence the trial success or failure. Direct players include participants themselves while indirect players include spouses, family, community, dropped participants, organizers - local and international collaborators (Mills et al., 2004; Newman et al., 2006; Thabethe et al., 2018).
We found that participant and community’s beliefs, myths, concerns and fear of being inoculated with a live HIV virus and the concern that the trial was sacrificing Africans as guinea pigs is not a new fear. Other studies reported the same concerns before (Mills et al., 2004; Newman et al., 2006).
The launch of vaccine trials for COVID-19 has not been without the same challenges including hesitancy and fear of the unknown if one gets vaccinated (Detoc et al., 2020). Demystifying myths through a program of education is required to ensure participants and their communities are properly educated on trials (Tarimo et al., 2016). Building communities of trust is crucial for the success of vaccine trials. As the world gears up for a vaccine for COVID-19 lessons learnt in the search for an HIV vaccine trial are hugely important today.
Those participants referred to investigators as foreigners to them suggest that trials’ investigators must have a shared identity with participants. Previous studies in South Africa also reported on challenges of mistrust as a result of a racial identity that was not shared between black African participants and foreign investigators (Thabethe et al., 2018). Continuous education of the community would go a long way in clearing the misconceptions and avoiding such misconceptions from wrongly influencing participants. For example, vaccine trials for COVID-19 which some two French doctors suggested must be tested in Africa, were actually conducted first in China and the developed world before any was launched in Africa (BBC, 2020; Coutinho and Dtm, 2020). This was followed by an educational announcement by the WHO Director-General in setting the record straight that vaccine development would not be any racial but would follow established ethical protocols.
The researchers are urged to build communities of practice and meaningful collaborations with local settings and communities for proper information dissemination and meaningful involvement of local people in trials. Examples of meaningful involvement include setting up community management and information dissemination teams helps bringing the communities to plan and contribute to the trial. We also learnt that participants join the study for exterior motives such as to benefit humanity, to be part of the world’s efforts to fight the HIV epidemic and protect future generations. A similar study in Kenya found that one-fifth of their participants were motivated by the need to find a vaccine for future generations (Nyaoke et al., 2017). The ravaging effects of the HIV infection in the research community ignited participation out of altruism. Likewise, the shocking death toll, excruciating pain with which COVID-19 brought may easily help to motivate participants to participate in the trial where they do not know if the vaccine will be safe for them or not. Such altruistic behaviour is commendable and must be supported.
The public health benefits that were brought with the trial, such as free HIV testing and health insurance were not much cited by participants as motivations but benefits which came the way of participants. Other studies in Tanzania have similarly reported participants expressing gratitude for medical insurance as a key benefit (Tarimo et al., 2019). This may be because of a lack of health insurance among people in resource-limited countries and communities. As a result, study investigators must ensure that such participants from low-income groups who volunteer are properly protected and understand the study aim, procedures and possible harm. Participants for COVID-19 vaccine trials may also have similar considerations of threats and benefits that they need to weigh in the trial. Providing the best available health insurance to participants during the COVID-19 trials should be a priority during the COVID-19 pandemic even at a time when the health system is overwhelmed by challenges including laboratory, human resources and hospital bed shortages. The organizations of the vaccine trials require careful analysis of participants and their needs. In our study, the timing of visits to the clinic (morning hours and weekdays) brought some inconvenience to participants like students, employees and other participants with competing for daily schedules. A similar challenge has been reported in the previous phase I/II, by Getz and Campo (2017). We recommend addressing such challenges in the best possible ways where possible, introducing some form of flexibility to participants such as weekend or late evening attendance. It becomes evident that more and detailed information or clarifications about the trial procedures and outcomes are needed during the educational and information seminars to deal with volunteers’ worries and concerns on vaccine safety. This underlines the importance of improving the package of information to the volunteers. For instance, information on the nature of the candidate vaccine to assure the volunteers that they will not get an infection due to participation and also the vaccine-induced positivity due to antibodies from the vaccine. Information is power, if participants are empowered with the correct information, they withstand unnecessary misinformation, myths and misconceptions from community members and also help educate them including accepting trial procedures in future studies.
LIMITATIONS OF THE STUDY
The study has its limitations. Firstly, the study was conducted three years post participation in the trial and the participant’s stories may have been subject to recall bias. Participants may have only concentrated on what they remembered most, leaving other stories which may have been important to the researchers. However, participant responses during our study did not show any signs of recall challenges. Secondly, the opinions and experiences gathered with regards to the rumours and misconceptions about the trial in the community were only collected from the people who participated in the study.
The study should have also interviewed community members to triangulate information with that obtained from participants for a more understanding of issues related to participation in vaccine trials. Despite these, we believe that we obtained a balanced view of the expectations and experiences of participation in the study. We also believe that these expectations and experiences are crucial for COVID-19 and other diseases vaccine trial development.
CONCLUSION
The study contributes to the understanding of HIV vaccine trial participants’ experiences and challenges encountered during participation in the trial. Areas of concern were identified and these need to be addressed by the research teams such as the provision of adequate information about HIV vaccine trials and also capacitating the communities with basic information about HIV vaccine trials. The information gathered is crucial in designing and implementing HIV and COVID-19 vaccine trial development. We recommend vaccine trial investigators to proactively address possible rumours and misconceptions, through a continuous education program to the communities where a vaccine trial takes place. Additionally, the use of media like television and radio programs for community education may be tested to help with information dissemination. The findings of this study are crucial to prepare for future HIV and COVID-19 vaccine trials.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEGEMENT
This research was funded by the National Institute for Medical Research- Mbeya Medical Research Centre (NIMR-MMRC).
REFERENCES
|
Arroyo MA, Hoelscher M, Sateren W, Maboko L, Hoffmann O, Kijak G, Robb M, Birx DL, Mccutchan FE (2005). HIV-1 diversity and prevalence differ between urban and rural areas in the Mbeya region of Tanzania. February, pp. 1517-1524. |
|
|
BBC (2020). Coronavirus: Africa will not be testing ground for vaccine. Says WHO. BBC.com. |
|
|
Braun V, Clarke V (2006). Using thematic analysis in psychology. Qualitative Research in Psychology 3(May 2015) :77-101. https://doi.org/10.1191/1478088706qp063oa |
|
|
Chenneville T, Gabbidon K, Hanson P, Holyfield C (2020). The impact of COVID-19 on HIV treatment and research: A call to action. In International Journal of Environmental Research and Public Health. |
|
|
Chin LJ, Berenson JA, Klitzman RL (2016). Typologies of altruistic and financial motivations for research participation: A qualitative study of MSM in HIV vaccine trials. Journal of Empirical Research on Human Research Ethics 11(4) :299-310. |
|
|
Communications and Global Advocacy UNAIDS (2020). UNAIDS FACT SHEET. Global HIV Statistics. Ending the AIDS Epidemic, pp. 1-3. |
|
|
Coutinho BA, Dtm MMPH (2020). Covid-19 in Africa: Scenarios and Signposts COVID-19 in Numbers Africa Has Growing Clinical Trial Experience Which. 10119. |
|
|
Detoc M, Bruel S, Frappe P, Botelho-Nevers E, Gagneux-Brunon A (2020). Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine, 38(45):7002-7006. 2020.04.23.20076513. |
|
|
Doshi M, Avery L, Kaddu RP, Gichuhi M, Gakii G, Du Plessis E, Dutta S, Khan S, Kimani J, Lorway RR (2017). Contextualizing willingness to participate: recommendations for engagement, recruitment & enrolment of Kenyan MSM in future HIV prevention trials. BMC Public Health 17(1) :1-12. |
|
|
Fereday J (2006). Demonstrating Rigor Using Thematic Analysis?: A Hybrid Approach of Inductive and Deductive Coding and Theme Development. International Journal Of Qualitative Methods 5(1) :80-92. 80-92. |
|
|
Getz KA, Campo RA (2017). Trial watch: Trends in clinical trial design complexity. Nature Reviews Drug Discovery 16(5):307-308. |
|
|
Greenhalgh T, Taylor R (1997). How to read a paper: Papers that go beyond numbers (qualitative research). BMJ Clinical Research, 26(2):54-60. |
|
|
Hargreaves J, Davey C, Auerbach J, Blanchard J, Bond V, Bonell C, Burgess R, Busza J, Colbourn T, Cowan F, Doyle A, Hakim J, Hensen B, Hosseinipour M, Lin L, Johnson S, Masuka N, Mavhu W, Mugurungi O, Yekeye R (2020). Three lessons for the COVID-19 response from pandemic HIV. The Lancet HIV 7(5):e309-e311. |
|
|
Kamazima SR, Kakoko DCV, Kazaura M (2020). Manifold Tactics are used to Control and Prevent Pandemics in Contemporary Africa": A Case of Tanzania's Fight against COVID-19. International Journal of Advanced Scientific Research and Management 5(11):20. |
|
|
Koff WC (2012). HIV vaccine development: Challenges and opportunities towards solving the HIV vaccine-neutralizing antibody problem. Vaccine 30(29):4310-4315. |
|
|
Lin D, Sun S, Operario D, Normal B (2020).Willingness to Participate in a COVID-19 Vaccine Trial Among Young Adults in China. Available at SSRN 3615937. |
|
|
Lurie N, Saville M, Hatchett R, Halton J (2020).Developing Covid-19 vaccines at pandemic speed. New England Journal of Medicine 382(21):1969-1973. |
|
|
Mbunda T, Bakari M, Tarimo EA, Sandstrom E, Kulane A (2014). Factors that influence the willingness of young adults in Dar es Salaam, Tanzania, to participate in phase I/II HIV vaccine trials. Global Health Action 7(1):22853. |
|
|
Mfinanga SG, Mnyambwa NP, Minja DT, Ntinginya NE, Ngadaya E, Makani J, Makubi AN (2021). Correspondence Tanzania ' s position on the COVID-19 pandemic. The Lancet 6736(21):6736. |
|
|
Mills E, Cooper C, Guyatt G, Gilchrist A, Rachlis B, Sulway C, Wilson K (2004).Barriers to participating in an HIV vaccine trial: a systematic review. Aids 18(17):2235-2242. |
|
|
Newman PA, Duan N, Roberts KJ, Seiden D, Rudy ET, Swendeman D, Popova S (2006).HIV vaccine trial participation among ethnic minority communities: Barriers, motivators, and implications for recruitment. Journal of Acquired Immune Deficiency Syndromes |
|
|
Nyaoke BA, Mutua GN, Sajabi R, Nyasani D, Mureithi MW, Anzala OA (2017). Volunteer motivators for participating in HIV vaccine clinical trials in Nairobi, Kenya. PLoS One. |
|
|
Opeyemi US, Kayode AF, Nafisat UI (2017). O16.6 Willingness of young persons in south-western nigeria to participate in early hiv vaccine trials. |
|
|
Pronker ES, Weenen TC, Commandeur H, Claassen EHJHM, Osterhaus ADME (2013). Risk in Vaccine Research and Development Quantified. PLoS One. |
|
|
Tarimo EAM, Bakari M, Kakoko DCV, Kohi TW, Mhalu F, Sandstrom E, Kulane A (2016). Motivations to participate in a Phase I/II HIV vaccine trial: A descriptive study from Dar es Salaam, Tanzania. BMC Public Health. |
|
|
Tarimo EAM, Ambikile J, Munseri P, Bakari M (2019). Perception of potential harm and benefits of HIV vaccine trial participation: A qualitative study from urban Tanzania. PLoS One. 1 |
|
|
Thabethe S, Slack C, Lindegger G, Wilkinson A, Wassenaar D, Kerr P, Bekker LG, Mngadi K, Newman PA (2018). "Why Don't You Go Into Suburbs? Why Are You Targeting Us?": Trust and Mistrust in HIV Vaccine Trials in South Africa. Journal of Empirical Research on Human Research Ethics. |
|
|
Thanh Le T, Andreadakis Z, Kumar A, Gómez RR, Tollefsen S, Saville M, Mayhew S (2020). The COVID-19 vaccine development landscape. In Nature reviews. Drug Discovery 19(5):305-306. |
|
|
THIS (2017). December 2017 Tanzania Hiv Impact Survey (THIS). December 2017 :2016-2017. |
|
|
Tong A, Sainsbury P, Craig J (2007). Consolidated criterio for reporting qualitative research (COREQ): a 32- item checklist for interviews and focus group. International Journal of Qualitative in Health Care 19(6):349-357. |
|
|
UNAIDS (2019). Global plan Country fact sheet-Tanzania. |
|
|
UNAIDS. (2020). AIDS Fact sheet: Global HIV statistics. |
|
|
World Health Organization (WHO) (2020). Coronavirus Disease 2019. In WHO (Vol. 14, Issue 6). |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


