Full Length Research Paper

ABSTRACT
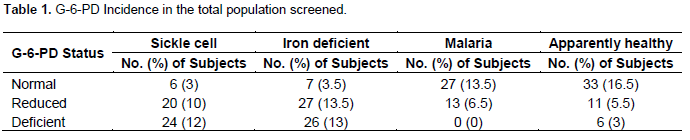
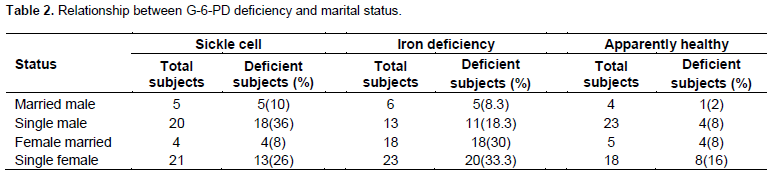
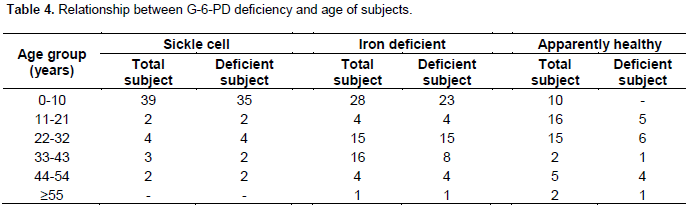
Glucose-6-phosphate dehydrogenase (G-6-PD) deficiency is one of the most well known human genetic defects and could possibly result in acute haemolysis after exposure to various oxidative conditions. This work was therefore carried out to determine the incidence of G-6-PD deficiency in anaemic patients attending General Hospital Kafanchan, Kaduna State, Nigeria. The study group comprised of 50 sickle cell, 60 iron deficient and 40 malaria patients, while 50 apparently healthy individuals served as control. Statistical analyses of the results according to age group, sex, marital status, packed cell volume (PCV) values, G-6-PD activities and genotype revealed 24 (12%), 26 (13%) and 6 (3%) were G-6-PD deficient in sickle cell, iron deficiency anaemia and apparently healthy, respectively. G-6-PD deficiency was absent in all malaria patients screened. In terms of marital status, singles of both males and females recorded higher deficiency than their married counterpart (P < 0.05). Furthermore, the age interval of 0 to 10 years old recorded highest number of G-6-PD deficient subjects in all the anaemic patients (P < 0.05). The study therefore suggests the need for routine G-6-PD screening test on anaemic patients to avoid factors which could further precipitate haemolytic crisis.
Key words: Incidence, glucose-6-phosphate dehydrogenase (G-6-PD), anaemia, haemolysis, Kafanchan, Nigeria.
INTRODUCTION
Glucose-6-phosphate dehydrogenase (G6PD) enzyme catalyzes the first step in the pentose phosphate pathway, leading to production of antioxidants that protect cells against oxidative damage (Luzzatto et al., 2001). G6PD defciency is the most common enzymatic erythrocyte disorder which is linked to the X-chromosome in humans (Elyassi and Rowshan, 2009; Valaes et al., 1998). A G6PD-defcient patient lacks the ability to protect red blood cells against oxidative stresses produced by the administration of certain drugs, metabolic conditions, infections and ingestion of some foods (Cappellini and Fiorelli, 2008; Glader, 2008).
Deficiency in G-6-PD is believed to affect about 100 million people globally (Carter et al., 2002) and the rate of pr-valence is higher among Africans and Asian (Abdulrazzaq et al., 1999). Reports showed that the G6PD A- allele, which contains two mutations, A376G and G202A, is the most common G6PD deficiency va-riant in Africa (Howes et al., 2013; Johnson et al., 2009) and the severity resulting from G-6-PD deficiency varies significantly between races with more severe deficiency occurring in the Mediterranean population and the milder form in the African population (Owa and Osanyituyi, 1988). Several reports have been published on this genetic disorder in various geographic populations (Beutler, 1993). It has been reported in Greece (Stamatoyannopolous, 1971), Romania (McCurdy et al., 1972), Algeria (Nafa et al., 1994), United State (Geskin et al., 2001), Saudi Arabia (Abdulrazzaq et al., 1999) and Nigeria (Abubakar et al., 2005).
In Nigeria, G6PD deficiency occurs in 24% of boys and 5% of girls (Ademowo and Falusi, 2002). It is also known to be a significant cause of anaemia in children, espe-cially neonates (Sodeinde et al., 1995). Yoruba children had the highest prevalence (16.9%) of G6PD deficiency followed by Igede children (10.5%) and children of Igbo (10.1%) and Tiv (5.0%) ethnicity. Igbo children had 0.38 times the odds of being G6PD deficient compared to Yoruba children. The odds for Igede and Tiv children were not significantly different from Yoruba children (Williams et al., 2013).
Haemolytic anaemia due to G-6-PD deficiency could be severe and life threatening (Luzzatto and Testa, 1978). About 25% of adults throughout the country have the sickle cell trait, AS, while the Hb C trait is largely confined to the Yoruba people of southwestern Nigeria in whom it occurs in about 6%. Other variant hemoglobins including beta thalassemia are rare, but alpha thalassemia occurs in 39% (32% with 3 alpha-globin genes; 7% with 2 alpha-globin genes) (Akinyanju, 1989). While screening of patients for G-6-PD deficiency is not a common practice in health-care delivery services of most poor African countries, there is a need for regular screening of individuals particularly malarial and anaemic patients to be able to establish their G-6-PD status. This is to avoid receiving drugs that could further precipitate haemolytic crisis in G-6-PD deficient individuals.
MATERIALS AND METHODS
Study subjects
This study was carried out on a total of 150 anaemic patients attending general Hospital Kafanchan, Kaduna State, North-Central Nigeria. The patients consist of 50 sickle cell anaemia, 60 Iron defi-cient anaemia and 40 Malaria patients while 50 apparently healthy individuals served as control. 113 of the subjects were females and 87 were males selected on age ranging from 0 to 75 years old.
Sample collection and analysis
The blood samples (5 ml) from each subject were collected through venepuncture from the antecubital vein of the forearm into dipotassium ethylene diaminetetracetic acid containers. The collected samples were screened immediately for G-6-PD using methaemoglobin reduction test (Brewer et al., 1962), serum ferritin radioimmunoassay test was used in the determination of iron deficiency. Malaria test strips were used to confirm malarial infection in the study group, genotype screening was used to confirm the sickle cell (SS) status of the studied group not under blood transfusion, while packed cell volume (PCV) of all the sampled patients was determined using microhaematocrit reader. The data were subjected to statistical analysis.
RESULTS
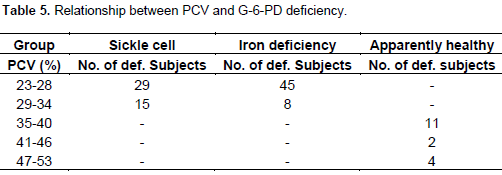
The results obtained are presented in Tables 1 to 5. The values are classified on the basis of sex, marital status, PCV values, G-6-PD activity and genotype.
DISCUSSION
The overall incidence of G-6-PD deficiency in the total population sampled has shown that Iron deficiency anaemic patients recorded highest prevalence while no deficiency was recorded among the malaria patients screened. The NADPH, a required co-factor in many bio-synthetic reactions, maintains glutathione in its reduced reduced form. Reduced glutathione acts as a scavenger for free radicals, and thus helps reduce oxidized haemoglobin to free haemoglobin; otherwise oxidized haemoglobin will precipitate as Heinze bodies. While many other body cells have other mechanisms of generating NADPH, the red blood cells rely completely on G6PD activity because it is the only source of NADPH that protects the cell against oxidative stress (Obasa et al., 2011).
Iron deficiency anemia is the most common form of anemia. Iron deficiency causes approximately half of all anemia cases worldwide, and affects women more often than men (Stoltzfus, 2001). Iron is a key part of red blood cells. Without iron, the blood cannot transport oxygen effectively. One means of loosing iron is through bleeding. There are various ways of loosing iron which include heavy, long, or frequent menstrual periods in women, cancer in the esophagus, stomach, small bowel, or colon, esophageal varices, usually from cirrhosis, the use of aspirin, ibuprofen, or arthritis medicines for a long time, which can cause gastrointestinal bleeding and peptic ulcer disease (Wikipaedia). Consequently, the higher incidence of G6PD deficiency was recorded in females with iron deficiency and therefore anaemia will be more severe in women than men.
Although most cases of iron-deficiency anaemia are mild and rarely cause complications, additional effect of G6PD deficiency might trigger severe anaemia, since iron can be converted to radicals which could result to oxi-dative damage of the erythrocyte's membrane (Beutler, 1994) contributing to abnormal red blood cell breakdown.
Sickle cell anaemic patients recorded the highest prevalence, the sickle cell morphology already predetermines their dysfunctional capacity, with G-6-PD deficiency however, there is an additional stress to this group of patients since the free radical generated either by a parasitic infection or administration of offensive drugs can destroy some of the circulating normal red blood cells.
The absence of G6PD deficiency in malaria patients is not surprising as haemolysis affects mature red blood cells more readily as there are fewer of them to host ma-laria parasites (Stephen et al., 1986). Moreover, malaria parasites could not thrive in immature red blood cells, thus, when an infected RBC dies before the parasite is ready, the malaria parasite dies as well (Stocker et al., 1985) there by inhibiting the chances of exerting a disease state and subsequent manifestation of typical symptoms. The study is also in agreement with the in vitro work of Capellini and Fiorelli (2008) who reported that malaria parasites grow slowest in G6PD-deficient cells. However, since malaria still sequester in the liver, affected persons could become very ill from haemolysis and G6PD patients are contraindicated to anti-malaria. The higher prevalence of G6PD-deficiency in subjects of 0 to 10 years is alarming since G6PD deficiency pre-disposes neonates to neonatal jaundice and sensitivity to certain drugs. Also, untreated neonatal jaundice may lead to hidden risk for Kernicterus (Kaplan and Hammerman, 2004). There is therefore a need to pay special attention to this age group which are selected by the Padiatrics.
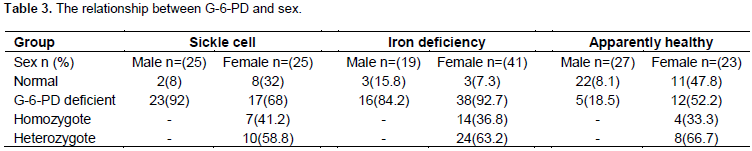
The higher incidence recorded in male subjects correlates with the established fact being X-linked, G6PD deficiency allele confers a selective advantage (Allison, 1960) though genetic heterogeneity may result in varying degree of haemolysis across individuals. However, the proportion of female subjects recorded in this study gives room for concern due to possible unfavourable lyoni-sation, where random inactivation of an X-chromosome in certain cells creates a population of G6PD-deficient red blood cells (Beutler, 1993; 1962; Beutler et al., 1962).
Also G-6-PD is known to generate reduced glutathione (GSH) which are free radical scavengers, however due to the deficiency of G-6-PD, the ability to generate GSH from its oxidized form (GSSG) is lost (Beutler, 1994), thus worsening the anaemia. This observation also correlates with higher number of iron deficient anaemic patients having lowest PCV value as compared to sickle cell anaemic patients.
CONCLUSION
Incidence of G-6-PD deficiency is higher in the iron deficient and absent in malaria patients. Therefore, there is a need for screening anaemic patients as part of the overall health and welfare service to avoid further complications.
ACKNOWLEDGEMENT
The authors are grateful to the management of the General Hospital Kafanchan for giving the permission to carry out the studies and all the Staff of Chemical pathology of the same hospital for their technical assistance.
CONFLICT OF INTEREST
The authors declared no conflict of interest.
REFERENCES
|
Abdulrazzaq YM, Micallef R, Qureshi M, Dawodu A, Ahmed I, Kdikr A, Bastaki SM, Al Khayat A, Bayoumi RI (1999). Diversity in expression of G6PD deficiency in females. Clin. Genet. 53(1):13-9. PMID 10066026 Crossref |
||||
| Abubakar A, Musa A, Iliyasu B, Adetunji H, Olaniru O, Akande T, Mokogwu ATH (2005). Incidence of G6PD deficiency in apparently healthy individuals on some parts of North central Nigeria. J. Med. Lab. Sc. 14(2):29-54. | ||||
|
Ademowo OG, Falusi AG (2002). Molecular epidemiology and activity of erythrocyte G6PD variants in a homogeneous Nigerian population. East Afr. Med. J. 79(1):42-44] Crossref |
||||
|
Akinyanju OO (1989). A profile of sickle cell disease in Nigeria. Ann. N. Y. Acad. Sci. 565:126-36 Crossref |
||||
|
Allison AC (1960). Glucose-6-phosphatase dehydrogenase deficiency in red blood cells of East Africans. Nature 186:531. Crossref |
||||
| Beutler E (1962). Biochemical abnormalities associated with hemolytic states. In: Weinstein IM, Beutler E (ed): Mechanisms of anemia in man. New York: McGraw-Hill. P 195. | ||||
|
Beutler E (1993). Study of G6PD deficiency, History and Mol. Biol. Am. J. Haematol. 42:53-58. Crossref |
||||
| Beutler E (1994). G-6-PD Deficiency; Review Article. Blood 84(11):2613-3636. | ||||
|
Beutler E, Yeh M, Faibanks VF (1962). The normal human female as a mosaic of X-chromosome activity; Studies using the gene for G-6-PD deficiency as a marker. Proc. Natl Acad Sci. USA 48:9. Crossref |
||||
|
Brewer GJ, Tarlov AR, Alving AS (1962). The methaemoglobin reduction test for primaquine type sensitivity of erythrocyte. JAMA 180(5):386-388 Crossref |
||||
| Carter SM, Gross SJ, Seiter K, McKenna R, Besa EC (2002). G6PD deficiency. E-Medicine 1:1-6. | ||||
|
Cappellini MD, Fiorelli G (2008) Glucose-6-phosphate dehydrogenase defciency. Lancet 371:64-74. Crossref |
||||
|
Elyassi AR, Rowshan HH (2009) Perioperative management of the glucose-6-phosphate dehydrogenase defcient patient: a review of literature. Anesth. Prog. 56:86-9. Crossref |
||||
| Glader BE (2008) Glucose-6-phosphate dehydrogenase defciency and related disorders of hexose monophosphate shunt and glutathione metabolism. In: The Wintrobe's Clinical Hematology. (10th Edition), Williams & Wilkins, Baltimore. | ||||
|
Howes RE, Dewi M, Piel FB, Monteiro WM, Battle KE, Messina JP, Sakuntabhai A, Satyagraha AW, Williams TN, Baird JK, Hay SI (2013). Spatial distribution of G6PD deficiency variants across malaria-endemic regions. Malar. J. 12:418. Crossref |
||||
|
Johnson MK, Clark TD, Njama-Meya D, Rosenthal PJ, Parikh S (2009) Impact of the method of G6PD defciency assessment on genetic association studies of malaria susceptibility. PLoS One 4:e7246. Crossref |
||||
| Luzzatto L, Mehta A, Vulliamy T (2001). "Glucose-6-Phosphate Dehydrogenase Definition." In: Scriver CR, Beaudet AL, Sly WS, Valle D (Eds.), The Metabolic and Molecular Basis of Inherited Disease, 8th edition Vol. 3. McGraw-Hill, New York, NY, USA. pp. 4517–4533. | ||||
| McCurdy PR, Scneir JH, Hansen TM (1972). Red Cell G6PD variants in Romania. Rev. Eur. Chin. Biol 17:66-9. | ||||
|
Nafa K, Roghis A, Usman N (1994). Atleast five polymorphic mutants account for the prevalence of G6PD deficiency in Algeria. Hum. Genet. 94:518. Crossref |
||||
|
Obasa TO, Mokuolu OA, Ojuawo A (2011). Glucose 6 phosphate dehydrogenase levels in babies delivered at the University of Ilorin Teaching Hospital. Niger. J. Paediatr. 38:165 -169. Crossref |
||||
| Owa JA, Osayintunji VO (1988). Screening For glucose-6-phosphate dehydrogenase deficiency by a simple method. Afr. Med. Med. Sci. 17(1):53-55. | ||||
|
Stamatoyannopoulos I, Viogtlander V., Kotsakis P, Akrivakis A (1971). Genetic diversity of the" Mediterranean" Glucose-6-Phosphate Dehydrogenase Phenotype J. Clin. Invest. 50:1253-61. Crossref |
||||
|
Sodeinde O, Chan MC, Maxwell SM, Familusi JB, Hendrickse RG (1995). Neonatal jaundice, aflatoxins and naphthols: report of a study in Ibadan, Nigeria. Ann. Trop. Paediatr. 15(2):107-113. PMid:7677410 |
||||
| Stephen K, Janney J, Heineich J, COY DF (1986). Excess release of Ferriheme in G-6 PD deficient erythrocytes: Possible cause of hemolysis and resistance to malaria. Blood 67(2):331-333. | ||||
|
Stocker R, Hunt NH, Buffinton GD, Weidenman MJ, Lewis-Hughes PH, Clark IA (1985). Oxidative stress and protective mechanisms in erythrocytes in relation to Plasmodium vinckel load. Proc. Natl. Acad. Sci. USA. 82:548. Crossref |
||||
|
Stoltzfus RJ (2001). Defining Iron-Deficiency Anemia in Public Health Terms: A Time for Reflection. J. Nutr. 131:565S–567S. Pubmed |
||||
| Valaes E, Drummond GS, Kappas A (1998). A control of hyperbilirubinaemia in malaria. Reforms Med 62:325. | ||||
|
Williams O, Gbadero D, Edowhorhu G, Brearley A, Slusher T, Slusher T, Lund TC (2013). Glucose-6-Phosphate Dehydrogenase Deficiency in Nigerian Children. PLoS ONE 8(7):e68800. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


